Congenital and Structural Renal Disorders
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
What is Autosomal Dominant Polycystic Kidney Disease (ADPKD)?
PKD1 > PKD2 gene causing fibrocystic changes in the kidney often between 25-45 years old
What family history risk factors are related to ADPKD?
Renal disease, dialysis, renal transplant, cerebral aneurysms, sudden unexplained death
What symptoms are seen with ADPKD?
HTN, Abdominal/Flank pain, palpable flank mass, hematuria, recurrent UTI, nephrolithiasis
What extrarenal manifestations are associated with ADPKD?
Liver cysts, cerebral aneurysms, and mitral valve prolapse
What is seen on renal ultrasound and CT/MRI with ADPKD?
Multiple renal cysts, varying sizes that are often bilateral

What is the management of ADPKD?
Aggressive BP control (ACE/ARB), sodium/protein restriction, increase fluids, manage complications
What is Autosomal Recessive Polycystic Kidney Disease (ARPKD)?
PHKD1 gene leading to congenital hepatic fibrosis that presents perinatally or during infancy
What is the clinical presentation of ARPKD?
may be detected on routine prenatal ultrasound or present with respiratory distress
What are some long term complications of ARPKD?
End stage renal and liver disease (ESRD and ESLD)
How does ARPKD appear on ultrasound and CT/MRI?
US: Numerous tiny cysts (microcysts), uniform in size, Bilateral renal enlargement, echogenic kidneys
CT/MRI: hepatic fibrosis

What is the management of ARPKD?
respiratory support, BP control, portal HTN and ESRD management, +/- nephrectomy or transplant
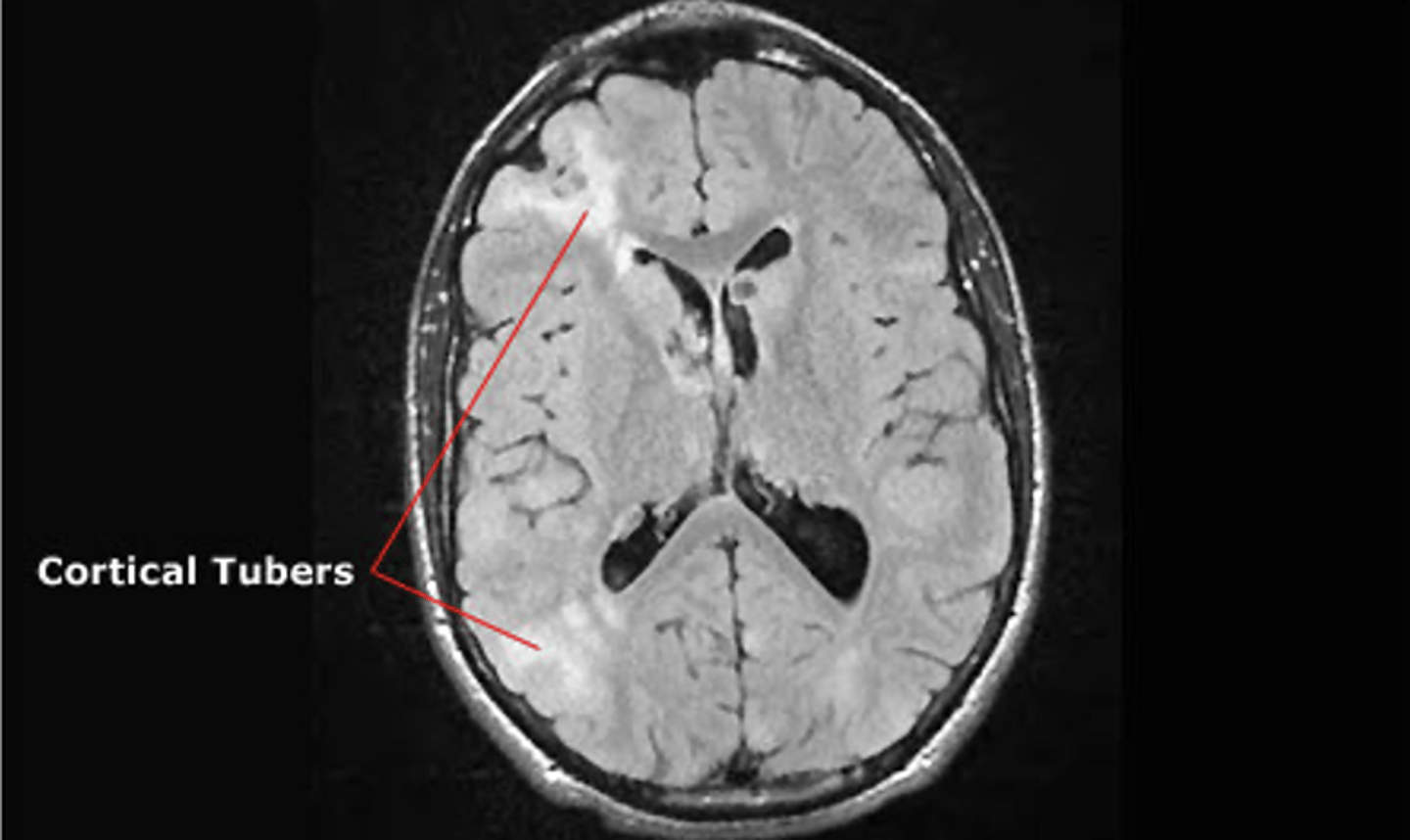
What is Tuberous Sclerosis (TSC)?
Autosomal dominant, multisystem disorder from variants in TSC1/TSC2 genes causing dysplastic lesion in multiple organs
When does TSC most often present?
infancy or within 1st year of life
What are the dermatologic presentations of TSC?
Hypomelanotic macules, Facial Angiofibromas, Fibrous plaques

What are the neurologic presentations of TSC?
epilepsy, cortical tubers, subependymal nodules, astrocytomas, TAND, cognitive deficits
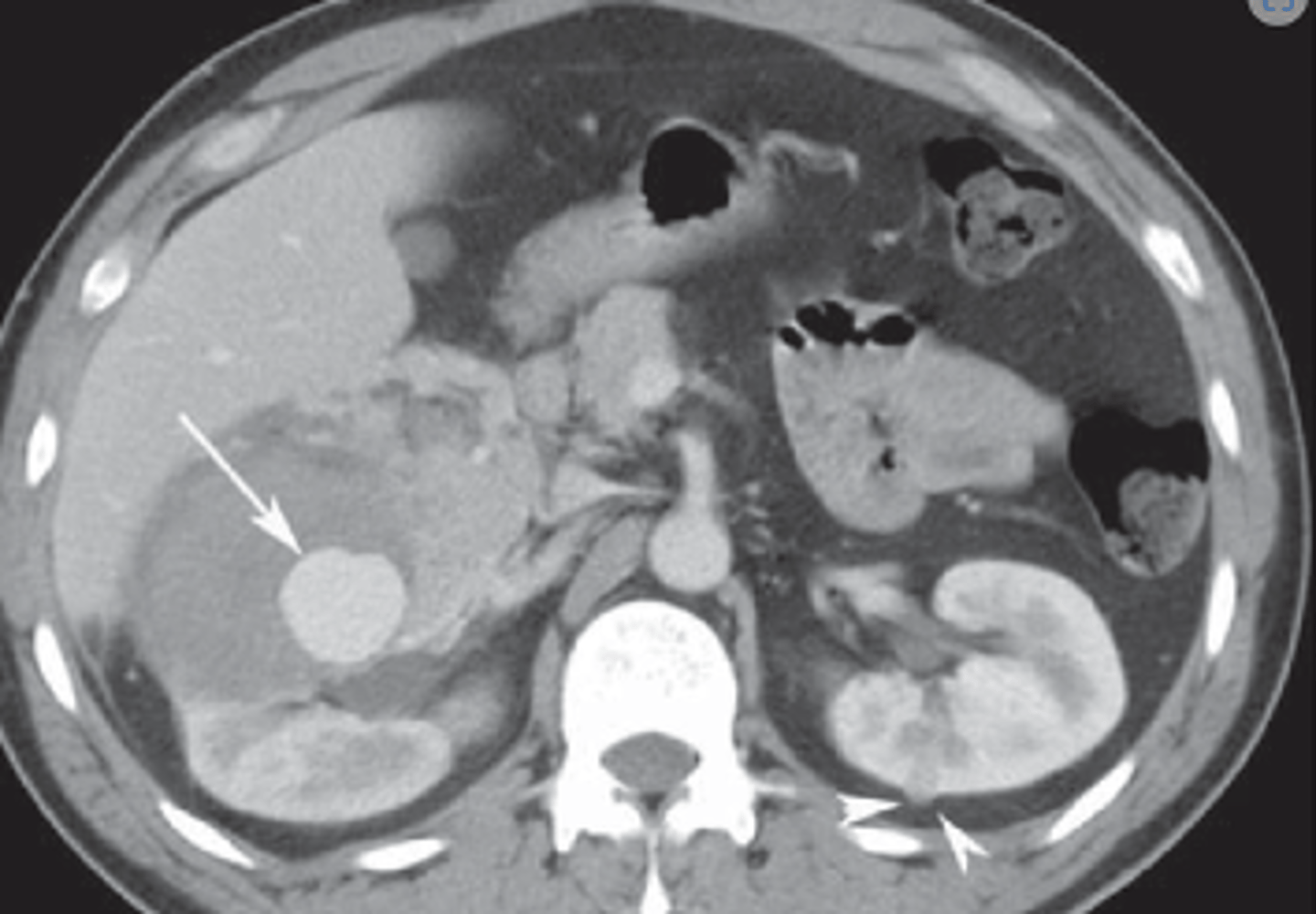
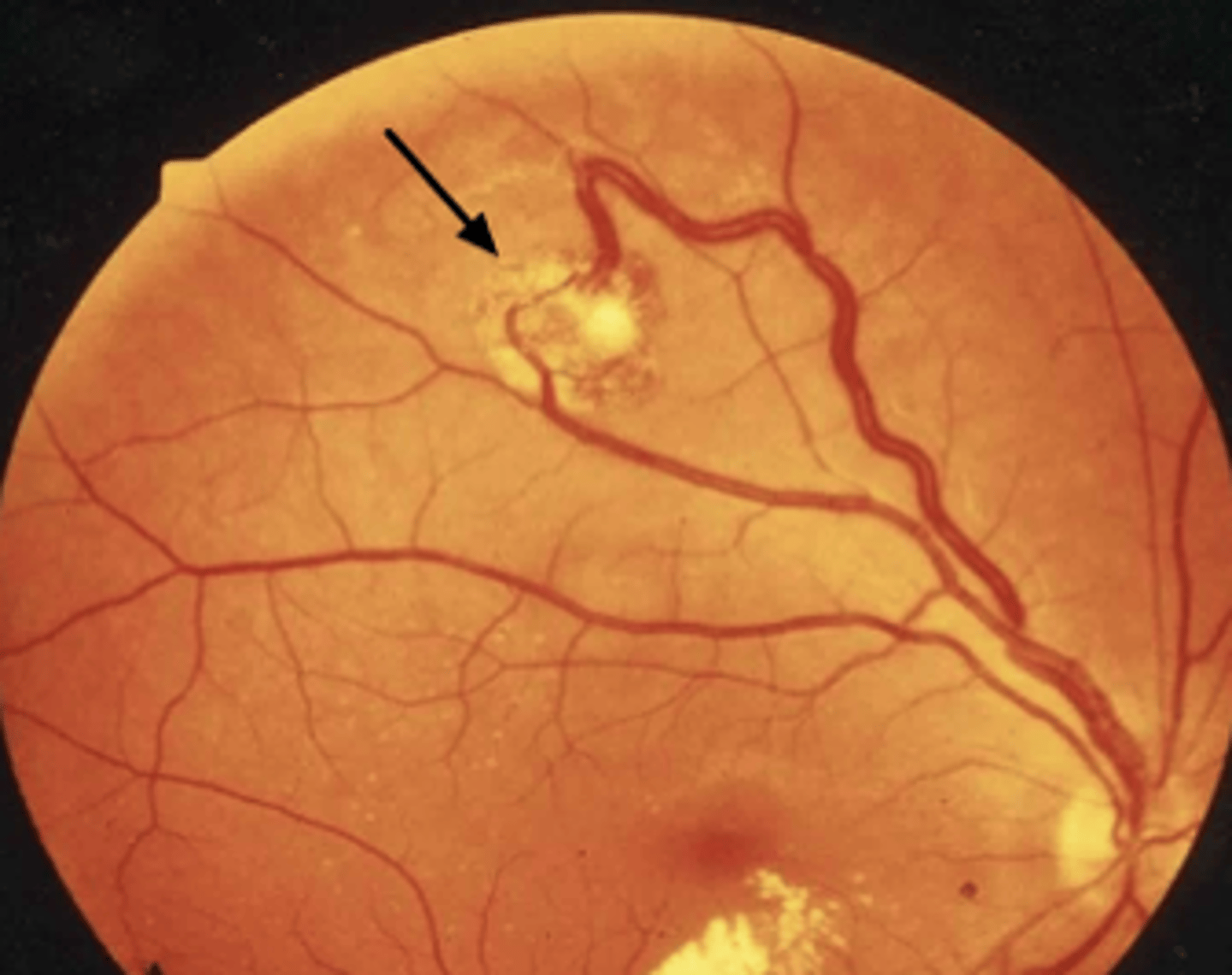
What are the other systemic manifestations of TSC?
- Renal angiomyolipomas
- Cardiac rhabdomyomas
- Retinal hamartomas
- Dental enamel pits
How does TSC appear on US or CT/MRI?
Angiomyolipomas (fat containing lesions) are characteristic
How is TSC managed?
mTOR inhibition (everolimus, sirolimus), seizure management (vigabatrin), complication prevention
What monitoring/screening is required for TSC?
- annual skin evaluation
- Brain MRI every 1-3 years until 25
- EEG as frequently as needed
- Annual TAND screening
- Echo/ECG every 1-3 years
- Regular dental/oral exams
What is Von Hippel-Lindau Syndrome (VHL)?
Autosomal dominant disorder with pathogenic variant in the VHL gene on the 3p25-26 chromosome
When does VHL most often present?
Renal and extra-renal involvement between 12-26 years old
What is the clinical presentation of VHL?
CNS hemangioblastomas: HA, ataxia, focal neuro deficits
Retinal hemangioblastomas: vision loss
Renal cell carcinoma
What imaging is preferred for renal abnormalities in VHL?
MRI preferred to evaluate for smaller lesions and for solid components

What is the management of VHL?
Surgical removal or Belzutifan (if not amendable)
What screening/monitoring is required for VHL?
- repeat imaging every 6mo-1yr
- MRI of brain and spine every 2 years starting at age 11
- eye exam annually starting at age 1
- MRI of abd/pelvis every 2 years starting at age 15
- pheochromocytoma annual screen starting at age 5
- auditory evaluation every 2-3 years starting at age 11
What is a Wilm's Tumor (nephroblastoma)?
Most common malignancy of the GU tract in children often presenting at age 3
What is the most common metastatic site of a Wilm's Tumor?
Lung (#1) then Liver
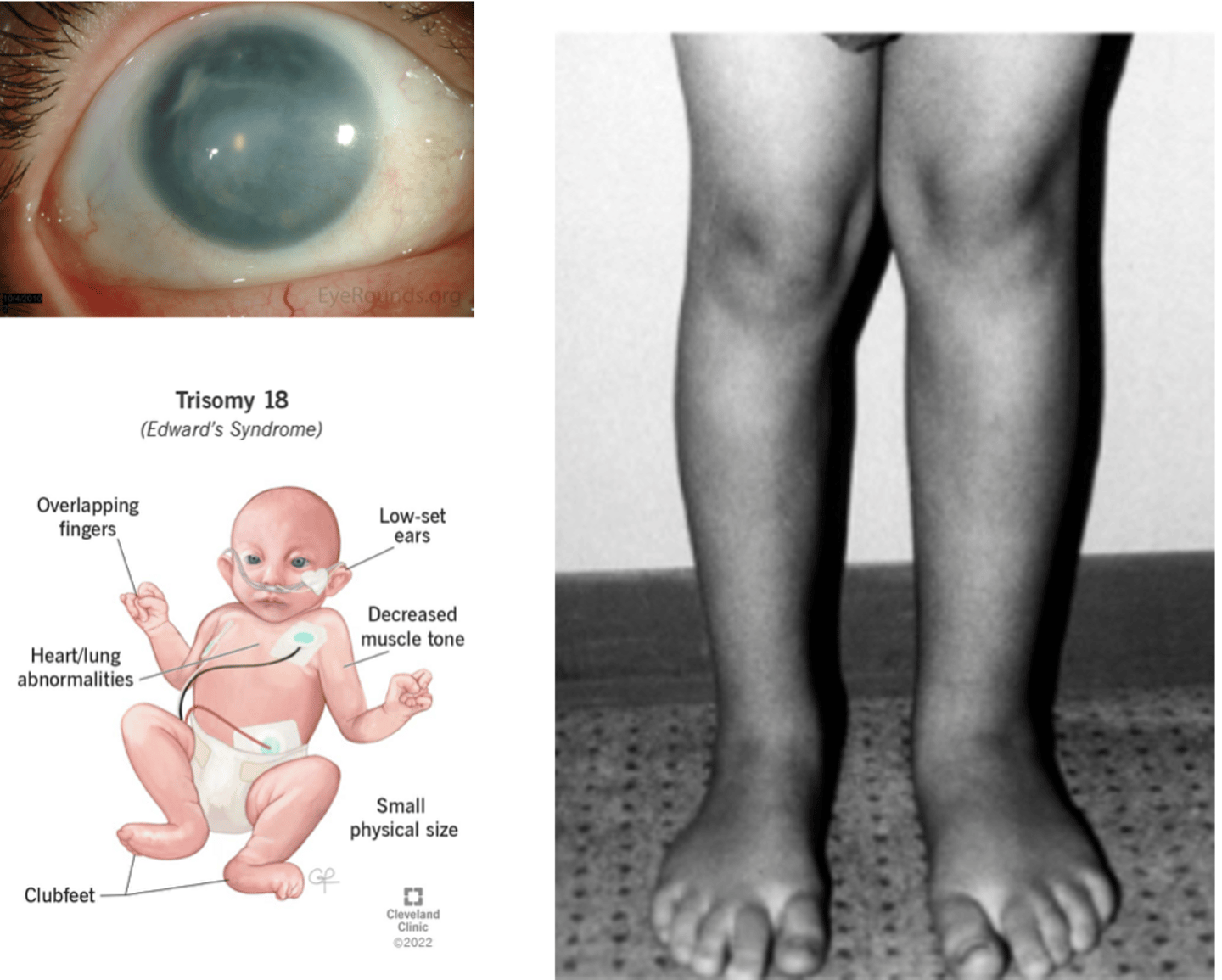
What are the associated anomalies/syndrome with a Wilm's tumor?
Aniridia (absence of iris), hypospadias, cryptorchidism, hemihypertrophy, trisomy 18
What is the clinical presentation of a Wilm's Tumor?
Unilateral abdominal mass, abd/flank pain +/- hematuria, HTN, fever
What imaging is obtained in Wilm's Tumor?
Abdominal US: vascular infiltration
MRI/CT: Large, heterogeneous, mixed components
+/- metastasis

How are Wilm's Tumor staged?
I: limited to the kidney
II: local spread/renal vein
III: lymph node spread
IV: hematogenous spread
V: bilateral renal involvement
What is the management of Wilm's tumor?
Surgical resection is standard of care
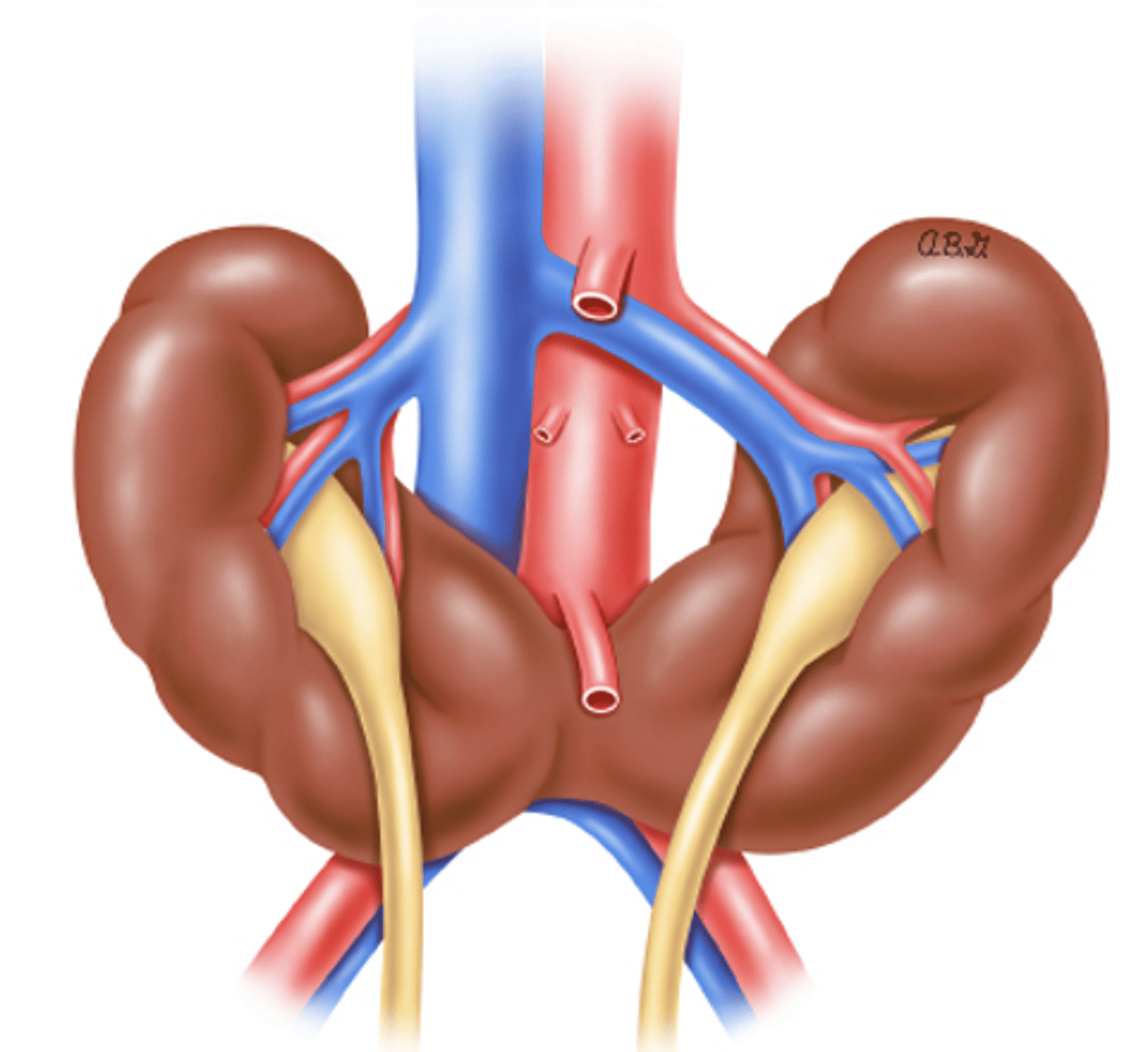
What is a Horseshoe kidney?
MC renal fusion anomaly that occurs at lower poles and disrupts normal rotation and ascent
What are some risk factors for a horshoe kidney?
M > F, 2-4 years old, Turner syndrome, Trisomy 18, Wilm's tumor
What is the clinical presentaiton of a horseshoe kidney?
asymptomatic, palpable abd mass, abdominal/flank pain, UTI, hematuria, nephrolithiasis
What extra renal anomalies may be present with horseshoe kidney?
Hypospadias (abnormal urethra), cryptorchidism, anorectal/vertebral malformation, genetic syndromes (Tuner and Trisomy 18)
What are the most common complications with horseshoe kidney?
- Vesicoureteral reflux (VUR)*
- Ureteropelvic junction obstruction (UPJO)*
- Hydronephrosis*
What is seen on prenatal US for horseshoe kidney?
Fusion of the lower poles of the kidneys, Low position of the renal units, and Malrotation

What labs are obtained for horseshoe kidney?
BMP, UA (infection, proteinuria) +/- Voiding cystourethrogram (VCUG)

What is the management for a horseshoe kidney?
close routine monitoring (BMP, UA) and managed complications
What is cystitis?
Infection within the bladder
What is pylenonephritis?
•infection within the kidney
How do urinary tract infection presentations change with age?
Infants: fever, irritability, poor feeding vomiting
Older children: dysuria, frequency, urgency, abd/flank pain, fever
What is included in the workup for a pediatric UTI?
UA, Urine culture, and Renal and bladder ultrasound (RBUS)
What is vesicoureteral reflex (VUR)?
Retrograde regurgitation of urine from the bladder into the ureters/kidneys
What are the risk factors for VUR?
Congenital anomalies, UTI (recurrent, febrile), and positive family history
What is the primary classification of VUR?
Abnormally short ureter + ineffective valve with limited peristalsis or abnormal insertion of ureter
What is the secondary classification of VUR?
Bladder outlet obstruction that can be functional or structural
What is the clnical presentation of VUR?
UTIs, pyelonephritis, bowel and bladder dysfunction (BBD), incontinence, enuresis, constipation
What imaging is obtained for VUR?
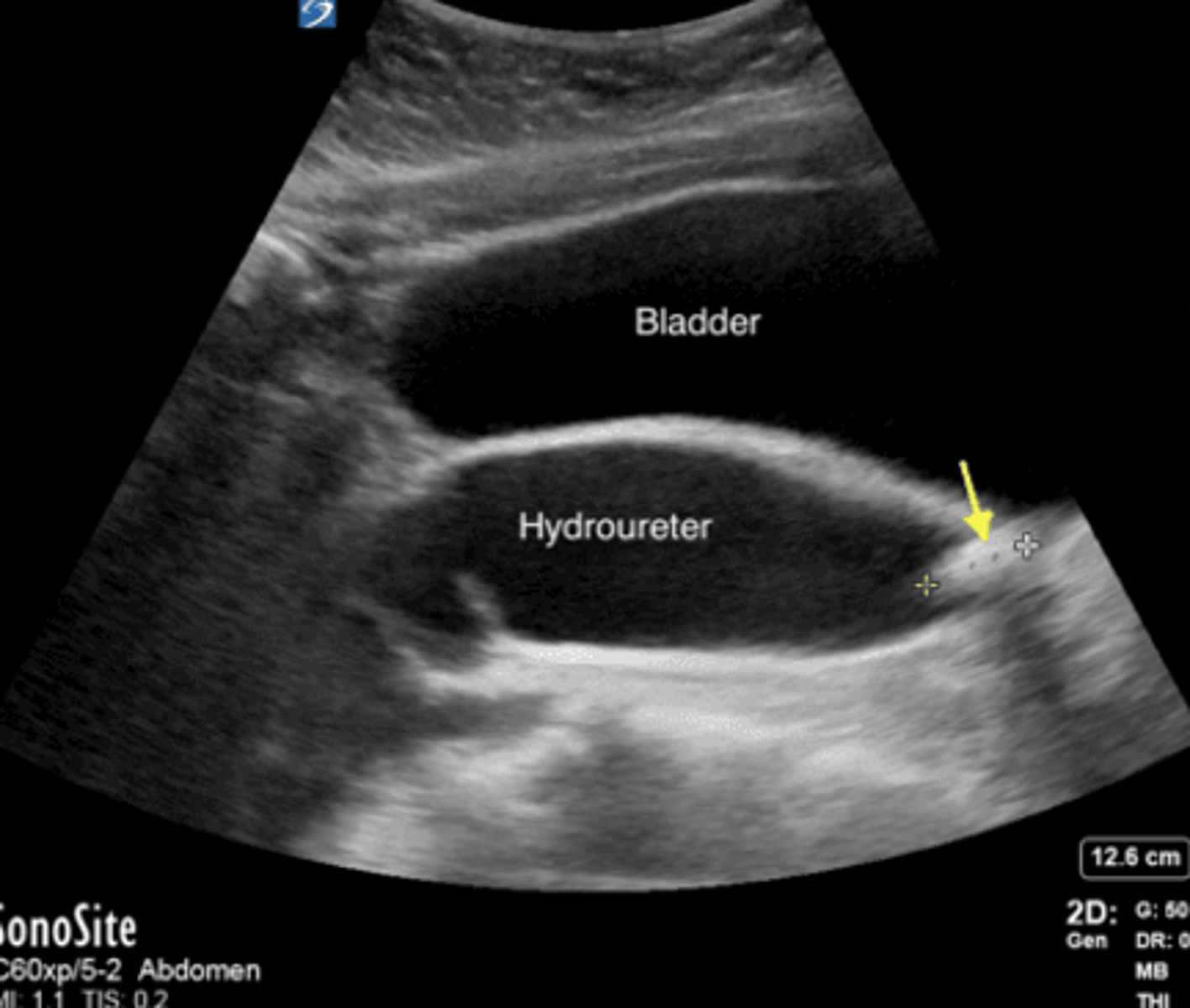
Renal bladder ultrasound (RBUS): often initial diagnostic and may show hydronephrosis and hydroureter
Voiding cystourethrography (VCUG): gold standard for diagnostic and grading of retrograde flow

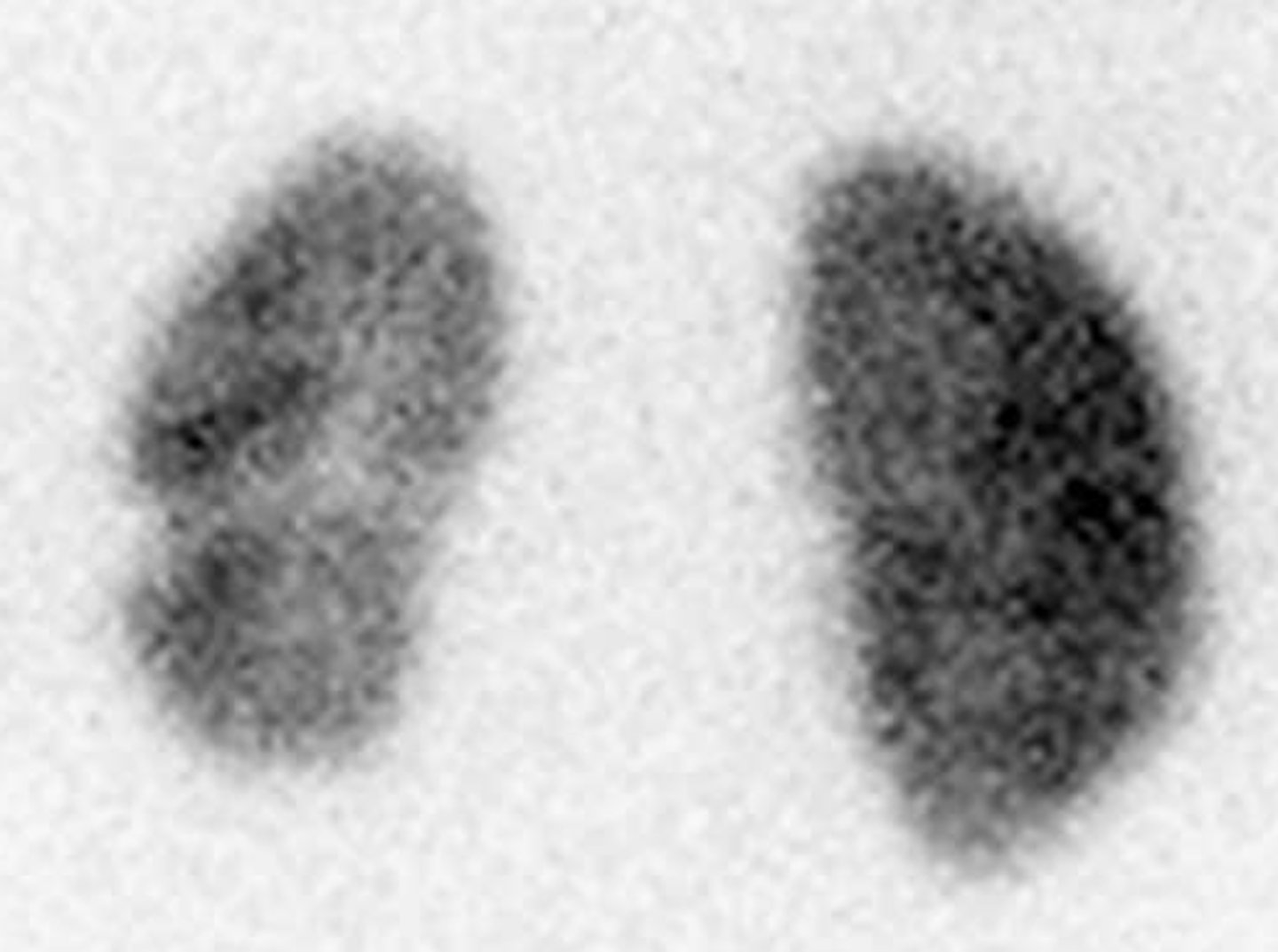
What are Dimercaptosuccinic acid (DMSA) scans used for in VUR?
asses for renal scarring in high-risk cases
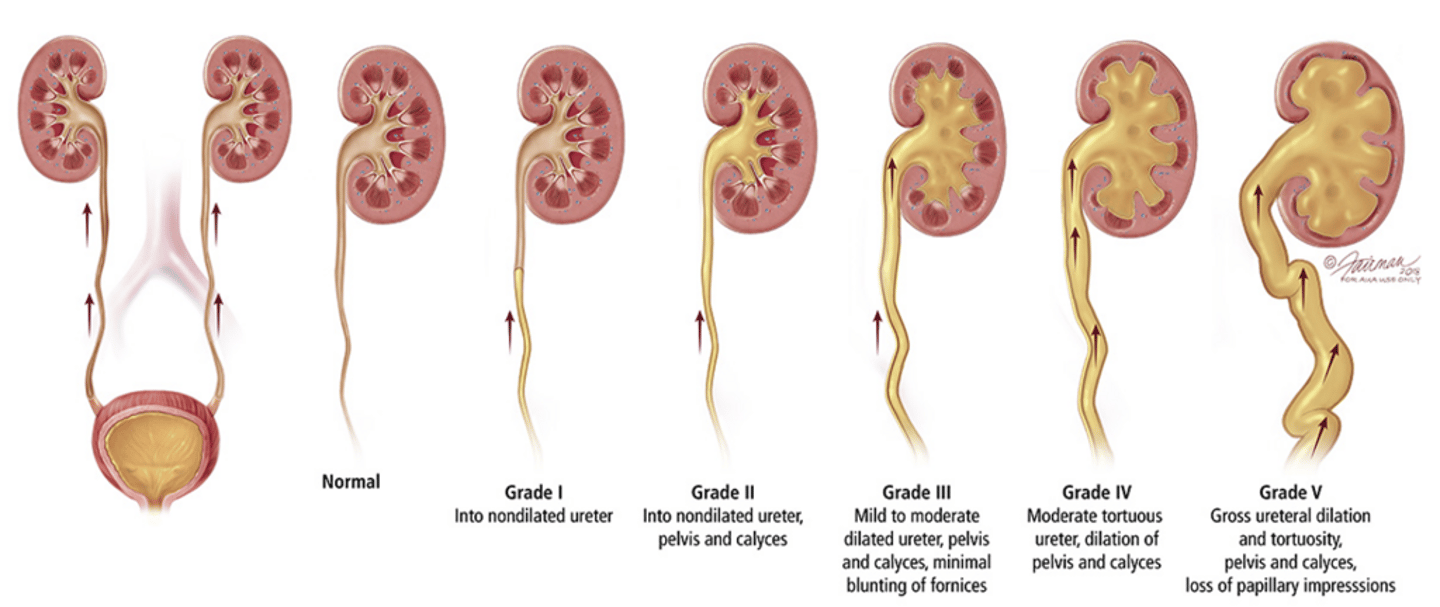
What is the expected course of VUR?
Grades I & II: resolves spontaneously
Grades IV & V: decreased resolution complicated with bilateral presentaiton or older age
When can watchful waiting be used to manage VUR?
- Very low risk patients
- Low grade
- >1yo or toilet trained
- No recurrent febrile UTIs
- No renal imaging abnormalities
When should continuous antibiotic prophylaxis used to manage VUR?
Low grade VUR that is symptomatic or has abnormal imaging; given once daily preferably at night
When is surgical intervention + CAP used for VUR managment?
- High grade VUR (III-IV) + renal scarring
- Any grade AND Recurrent UTIs despite CAP
What is hydronephrosis?
Dilation of the kidney due to accumulation or urine
What is hydroureter?
Dilation of the ureter due to accumulation or urine
What are the common causes of hydronephrosis/hydroureter?
Congenital anomalies, urinary stones (nephrolithiasis), and vesicoureteral reflux
What is Ureteropelvic Junction Obstruction (UPJO)?
Congenital anomaly causing impairment of urine flow between the renal pelvis and the proximal ureter
What is intrinsic UPJO?
Congenital narrowing at peristaltic segments of proximal ureter
What is extrinsic UPJO?
- Crossing vessels
- High insertion of ureter
- Polyps, cysts, masses
What is the clinical presentation of UPJO?
abd/flank pain, infection, oliguria, edema
What is a dietl crisis of UPJO?
Intermittent/episodic severe abdominal/flank pain and N/V precipitated by increased fluid intake or diuresis
How does UPJO and VUR differ on RBUS?
VUR: hydronephrosis and hydroureter
UPJO: hydronephrosis without hydroureter
What additional imaging is needed is any evidence of hydronephrosis is seen on prenatal US?
postnatal US within 48 hours of birth
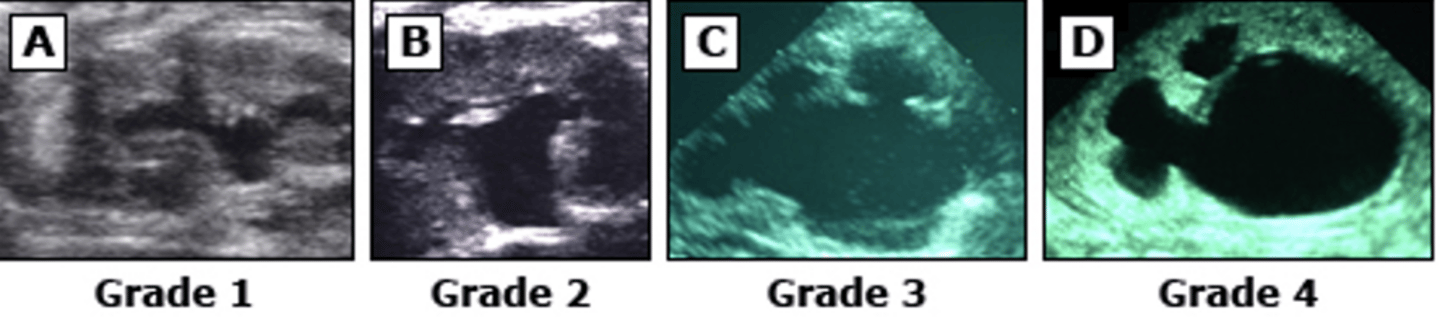
What is the grading of UPJO?
0: No dilation
1: renal pelvis only visualized
2: renal pelvis and few calyces
3: all calyces are visualized
4: parenchymal thinning
What follow up is indicated based on the grade of Hydronephrosis/Hydroureter on postnatal US?
Grades 1-2: repeat imaging in 1-6 months
Grades 3-4: additional testing required
What is the treatment for UPJO?
Primarily surgical, pyeloplasty and reconstruction of the ureteropelvic junction