Looks like no one added any tags here yet for you.
what are the Pathoanatomical Diagnoses of Subacromial Pain Syndrome (SAPS)
Subacromial Impingement Syndrome, Rotator Cuff Tendinopathy/Dysfunction, Rotator Cuff Tears, Bicipital Tendinopathy, Superior Labrum Anterior to Posterior (SLAP) Tear
Subacromial Impingement Syndrome (SAIS) is compression of
RC Tendons &/or bursa under:
Acromion
Coracoacromial ligament
Coracoid
AC joint
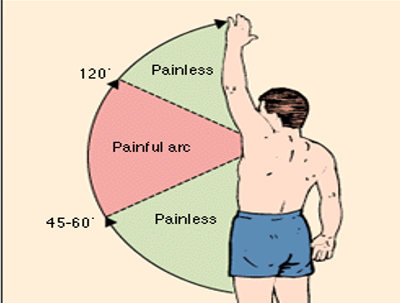
Subacromial Impingement Syndrome (SAIS) is typically seen to affect mid range shoulder elevation
80-130°, demonstrates painful arc
why is there a relief in SAIS after mid range?
scapular upward rotation & posterior tilting takes over in motion
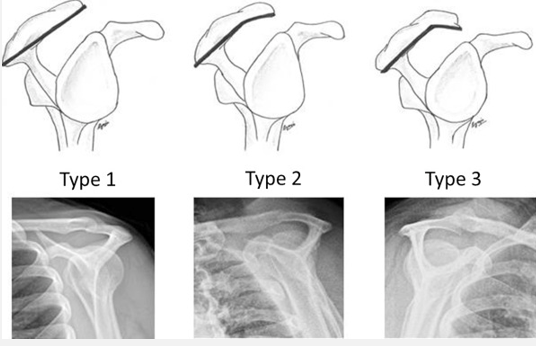
Shoulder Impingement has Anatomical Contributors such as changes in shape of
acromium, Type 1-3
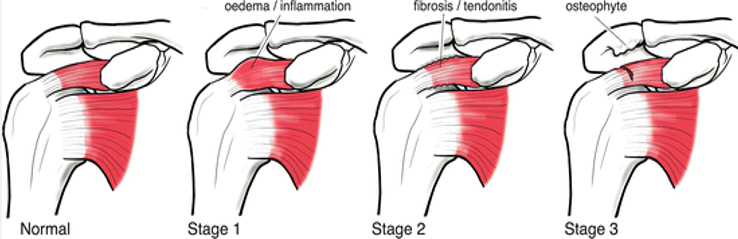
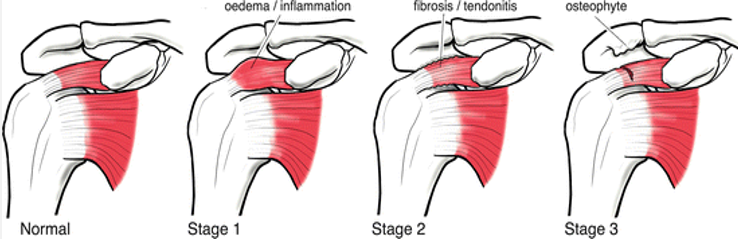
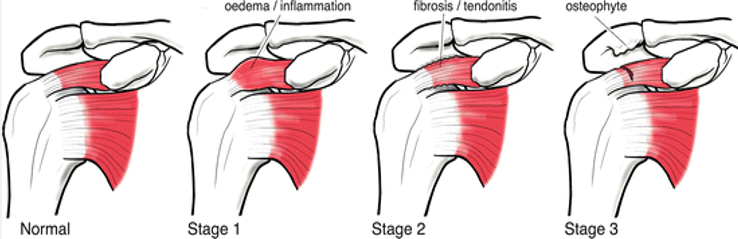
tendon overload inflammation can cause SAIS, what is the presentation of Neers Stage 1?
Inflammation
Pain and Weakness
Impingement signs
tendon overload inflammation can cause SAIS, what is the presentation of Neers Stage 2?
RC tendinosis
Bursa Fibrosis: Pain & Weakness, Impingement signs
tendon overload inflammation can cause SAIS, what is the presentation of Neers Stage 3?
Osteophyte formation in SA Space
RC tearing: Full Thickness vs Partial Tears, More pain & significant weakness
Signs and Symptoms of SAIS - subjective signs
Pain w/ active elevation
Difficulty sleeping on arm (compression)
Signs and Symptoms of SAIS - objective signs
AROM: painful arc
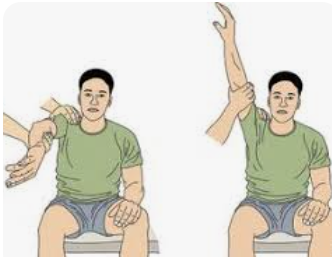
PROM: may be painless
resisted movements: weak & painful
Does acromial compression contribute to SAPS?
yes, but it is not the only structure involved
What is the source of the symptoms for SAPS?
Symptoms may come from compression, tension, or both
what is the most common mechanism of supraspinatus tears?
bottom up tear, humeral head being pulled into supraspinatus
RC Tendinopathy can occur from tensile overload (Eccentric activities related to throwing, Repetitive manual labor/overhead tasks), which tendon is most commonly involved?
supraspinatus (teres is least affected)
Intrinsic Mechanisms/causes/factors of RC Tendinopathy
Tendon health & quality
Aging, Genetics
Vascular changes: Comorbidities, Tissue Injury
Altered loading: ↑ humeral head migration, Tendon Swelling after acute overload
Extrinsic Mechanisms of RC Tendinopathy
Smoking, Diet
Occupational: Manual Labor, Prolonged Overhead Activity
Athletics: Overhead
Hobbies
Tendinopathy Contributors include
Scapular Dyskinesis: conflicting evidence
posture: flexed posture limits shoulder motion
hypermobility of GH jt: labral tearing, shoulder instability
hypomobility: posterior capsule tightness (anterior shoulder gliding can cause more compress/overload)
which shoulder special test cluster by Michener shows >3/5 (+) tests is clinically significant?
Hawkins-Kennedy, Neers, Painful arc, empty can, ER resistance
what special test involves IR, passive elevation, and scapular depression?
Neers Test (closes SA space)
what special test involves horizontal abduction, IR, 90° elevation?
(max compression of SA space) Hawkins-Kennedy
what special test involves over pressure in IR in scaption position (coils supraspinatus)
empty can special test
resisted ER stresses
supraspinatus & infraspinatus
Posterior Shoulder Impingement is usually seen in OH athletes at
90/90
Pain/pinching during cocking phase of throwing
in the 90/90 position, humerus (Anterior translation of humeral head during cocking phase) pinches posterior capsule between
humeral head & glenoid (Posterior Shoulder Impingement)
Calcific tendinopathy - Supraspinatus has a calcium deposit buildup in rotator cuff tendon, is a result of
chronic tendinopathy, May or may not be a source of pain in of itself (may not change on imaging, but can be pain free)
Management of Cuff Tendinopathy
NSAIDs: (long term tissue degradation, GI bleeding)
Corticosteroid Injection: Efficacy Mixed, Short Term improvements, Potential (-) effects
CSI vs Manual Therapy: Same at 1 yr
intervention focus for high irritability (7/10) pts: Minimize Physical Stress, Activity modification, Monitor impairments &
MT to Shoulder/Cervical Thoracic
Scapular Strengthening (it still works GH)
ROM: AAROM (pulleys)
intervention focus for mod irritability (4-6/10) pts Mild–Moderate Physical Stress: •Address impairments, •Basic-level functional activity restoration intervention focus w/
Tendon Loading of RC: Lower load seems = as effective as higher load (ER, IR)
Scapular Strengthening (rows)
ROM
intervention focus for low irritability (3/10) pts w/ Moderate–High Physical Stress: •Address impairments, •High-demand functional activity restoration w/
Tendon Loading of RC: Lower load seems = as effective as higher load
UE strengthening in most comfortable positions (start w/ dumbbells, OHP, bench) can progress
Scapular Strengthening (loaded Is, Ts, Ys, heavy rows)
ROM -PRN
Functional Training