AKI - Zhang
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
10 Terms
Pathophysiology of pre-renal AKI
Renal blood hyperfusion → renal artery, segmental branches, interlobar vessels, arcuate arteries, interlobular arteries, afferent arterioles, efferent arterioles
Pathophysiology of intrinsic AKI
Ischemic or toxins → Glomerulus, tubules, interstitial tissue, peritubular vasculature
Pathophysiology of postrenal AKI
Obstruction in urine flow → collecting ducts, minor calices, rena pelvis, ureter, bladder, urethra!
Causes of prerenal AKI
NSAIDs, ACEI/ARBs, calcineurin inhibitors
Causes of intrinsic AKI
ATN nephrotoxins like contrast dye and endogenous toxin
Causes of postrenal AKI
Prostatic hypertrophy
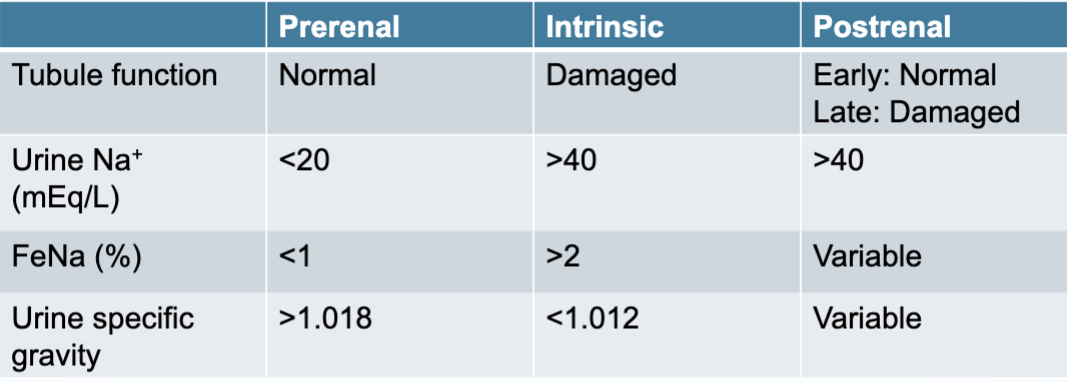
Diagnosis of prerenal, intrinsic, postrenal AKI
DOC for AKI treatment - Loop diuretics
MOA: inhibit NKCC2 in thick ascending limb of loop of henle
Side effects:
Electrolyte imbalance
Metabolic alkalosis
Hyperuricemia
Ototoxicity
Allergies/other reactions
Loop diuretic comparisons
Predictable oral bioavailability: torsemide and bumetanide > furosemide
Potency: bumetanide > torsemide > furosemide
Allergy to sulfa drugs: ethacrynic acid
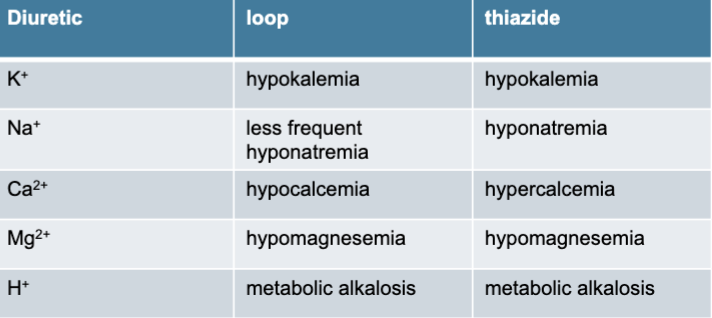
Loop vs thiazides