Hormone therapy in breast cancer treatment
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
What are hormones?
Substances that function as chemical messengers in the body.
They affect the actions of cells and tissues at various locations in the body, often reaching their targets through the bloodstream.
Oestrogen and Progesterone
produced by the ovaries in premenopausal women and by some tissues in pre and post menopausal women and men
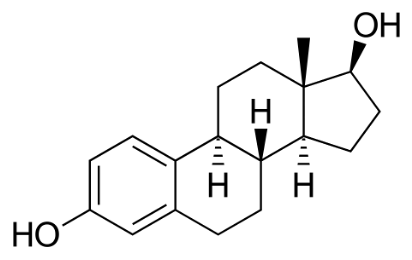
Oestrogen
promotes the development and maintenance of female sex characteristics and the growth of long bone
produced by the ovaries in premenopausal women and by some tissues in pre and post menopausal women and men
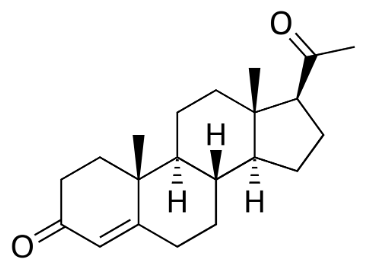
Progesterone
plays a role in the menstrual cycle and pregnancy.
produced by the ovaries in premenopausal women and by some tissues in pre and post menopausal women and men
Issues with oestrogen and progesterone
promote growth of some breast cancers that are hormone dependent/hormone sensitive and contain receptors that become activated when hormones bind to them and change expression of genes leading to stimulation of tumour growth
Structure of Oestrogen
Structure of Progesterone
Hormone therapy
slows or stops the growth of hormone-sensitive tumours by blocking the body’s ability to produce hormones or by interfering with effects of hormones on breast cancer cells
ER+ and ER-
oestrogen receptor positive (ER positive), oestrogen sensitive, or oestrogen responsive
oestrogen receptor negative (ER positive), oestrogen insensitive, or oestrogen unresponsive aka they do not use oestrogen to grow → do not respond to hormone therapy
HR+ and HR-
HR+ = tumours that contain oestrogen and/or progesterone receptors
HR- = tumours that lack BOTH oestrogen and progesterone receptor
HRT in HR+ cancer
can promote the growth of the tumour
usually patients asked to stop this therapy or any OC if they are taking it (but EHC can be taken as it is single dose in case of emergency)
HER2
Human Epidermal Growth Factor 2
Triple negative cancer
the cancer does not have receptors for either HER2 or the hormones oestrogen and progesterone
HER2 +ve cancer treatment
herceptin - trastuzumab
What are the main strategies used to treat hormone-sensitive breast cancer?
blocking ovarian function
blocking oestrogen production
blocking oestrogen effects
Blocking ovarian function as a treatment for breast cancer
Known as ovarian ablation
surgically removing the ovaries in a oophorectomy OR treat with radiation
usually permanent
Drugs that block ovarian function
Goserelin - LH-R
ovarian function can be suppressed temporarily by treatment with drugs called gonadotropin-releasing hormone (GnRH) agonists, which are also known as luteinizing hormone-releasing hormone (LH-RH) agonists
Blocking oestrogen production to treat breast cancer
Aromatase inhibitors
block the activity of aromatase which is used in the body to make oestrogen in the ovaries and other tissue
primarily used in post-menopausal women cause in pre-menopausal too much aromatase is made for the inhibitor to be effective
Anastrozole/Letrozole
aromatase inhibitor - temporary
Exemestane
aromatase inhibitor - permanent
Role of aromatase
converts androstenedione to oestrogen/testosterone to oestradiol
makes the hexene ring + carboxyl on the LHS of andro → aromatic ring + OH
Blocking oestrogen effects to treat breast cancer
use SERM - selective oestrogen receptor modulators
bind to oestrogen receptors and prevent oestrogen from binding
e.g. tamoxifen and toremifene
Potential issue with SERM
Potentially not only block estrogen activity (i.e., act as oestrogen antagonists) but also mimic oestrogen effects (i.e., serve as oestrogen agonists).
SERMs can behave as oestrogen antagonists in some tissues and as oestrogen agonists in other tissues.
For example, tamoxifen blocks the effects of oestrogen in breast tissue but acts like oestrogen in the uterus and bone.
Tamoxifen
SERMs
to treat HR+ hormone receptor–positive breast cancer.
Fulvestrant
Also blocks oestrogen effects
oestrogen antagonist like SERM BUT no agonist effects
pure antioestrogen
when it binds to ER, it targets the receptor for destruction
Three main ways that hormone therapy is used to treat hormone-sensitive breast cancer
Adjuvant therapy for early-stage breast cancer
Treatment of advanced or metastatic breast cancer
Neoadjuvant treatment of breast cancer
Adjuvant therapy for early-stage breast cancer (tamoxifen)
Women who receive at least 5 years of adjuvant therapy with tamoxifen (after having surgery for early-stage ER-positive breast cancer) have reduced risks of breast cancer recurrence, including a new breast cancer in the other breast, and death (at 15 years).
Tamoxifen is approved for adjuvant hormone treatment of premenopausal and postmenopausal women with ER-positive early-stage breast cancer, and the aromatase inhibitors anastrozole and letrozole are approved for this use in postmenopausal women.
Exemestane
Aromatase inhibitor approved for adjuvant treatment of early-stage breast cancer in postmenopausal women who have received tamoxifen previously.
Treatment of advanced or metastatic breast cancer using hormone therap
Many types of HT are approved for treatment of metastatic/recurrent hormone-sensitive breast cancer including:
tamoxifen/toremifene to treat metastatic breast cancer
fulvestrant for postmenopausal women with metastatic ER-positive breast cancer that has spread after treatment with antioestrogen (could also be used in premenopausal women who have had an ovarian ablation)
aromatase inhibitors for post menopausal women with metastatic/locally advanced hormone-sensitive breast cancer but only as INITIAL therapy
Aromatase inhibitors (including Exemestane) may also be used to treat postmenopausal women who’s disease has advanced after treatment with tamoxifen
Lapatinib
tyrosine kinase inhibitor
targeted therapy drug used in combination with aromatase inhibitor to treat HER-positive metasatic breast cancer in postmenopausal women
Locoregional recurrence
ER-positive breast cancer that has come back in the breast, chest wall, or nearby lymph nodes after treatment
Palbociclib use
targeted therapy used in combination with letrozole as initial therapy for the treatment of hormone receptor–positive, HER2-negative advanced breast cancer in postmenopausal women.
also approved to be used in combination with fulvestrant for the treatment of women with hormone receptor–positive, HER2-negative advanced or metastatic breast cancer whose cancer has gotten worse after treatment with another hormone therapy
CDK 4/6
Cyclin dependent kinase that promote the growth of hormone receptor positive cancer cells
Palbociclib
CDK4/6 inhibitor
Neoadjuvant treatment of breast cancer using hormone therapy
The goal of neoadjuvant (before surgery) therapy is to reduce the size of a breast tumour to allow breast-conserving surgery.
Neoadjuvant hormone therapy (in particular, with aromatase inhibitors) can be effective in reducing the size of breast tumours in postmenopausal women.
The results in premenopausal women are less clear because only a few small trials involving relatively few premenopausal women have been conducted thus far.
How can Tamoxifen reduce the risk of developing breast cancer?
Tamoxifen if taken for 5 years can reduce the risk of developing invasive breast cancer by about 50% in post menopausal women who were at increased risk and long term it reduces the incidence of breast cancer for at least 20 years
Raloxifene if taken for 5 years reduces breast cancer risk in such women by about 38%
How can Raloxifene reduce the risk of developing breast cancer?
Raloxifene if taken for 5 years reduces breast cancer risk in such women by about 38% in post menopausal women who were at increased risk and long term it reduces the incidence of breast cancer for at least 20 years
Can aromatase inhibitors reduce risk of breast cancer?
Yes, it has been found to reduce the risk of breast cancer in postmenopausal women at increased risk of the disease.
Women who took exemestane were 65% less likely than those who took a placebo to develop breast cancer after three years.
After 7 years of follow-up women who took anastrozole were 50% less likely than those who took placebo to develop breast cancer.
Common side effects of hormone therapy
hot flashes
night sweats
vaginal dryness
disruption of menstrual cycle
Side effects of Tamoxifen
Risk of blood clots, especially in the lungs and legs
Stroke
Cataracts
Endometrial and uterine cancers
Bone loss in premenopausal women
Mood swings, depression, and loss of libido
Side effects of Raloxifene
Risk of blood clots, especially in the lungs and legs
Stroke in certain subgroups
Side effects of Aromatase inhibitors
Risk of heart attack, angina, heart failure, and hypercholesterolemia
Bone loss
Joint pain
Mood swings and depression
Side effects of Ovarian suppression drugs
Bone loss
Mood swings, depression, and loss of libido
Side effects of Fulvestrant
Gastrointestinal symptoms
Loss of strength
Pain
Antidepressants + Tamoxifen
SSRIs can inhibit CYP2D6 which is responsible for metabolising the Tamoxifen into it’s more active metbaolite
inhibiting the CYP2D6 enzyme can slow the metabolism of tamoxifen and reduce it’s effectiveness → need patients to consider switch to a weaker inhibitor (e.g. sertraline) or one that isn’t an inhibitor at all (e.g. citalopram/venlafaxine
if postmenopausal then suggest aromatase inhibitor instead?