psych MT 3
1/151
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
152 Terms
Memory
recalling past events and past learning by means of encoding, storage, and retrieval
Memory overview (3 processes)
encoding: getting information into memory in the first place
Storage: retaining memories for future use
Retrieval: recapturing memories when we need them
2 theories of how many memory works
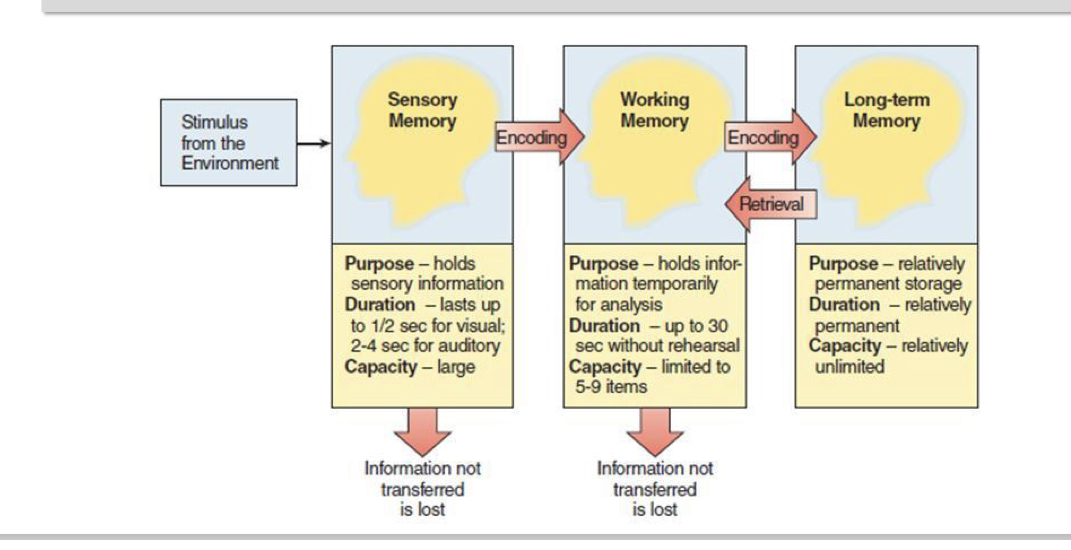
–Information-Processing Model – information passes through three memory stores during encoding, storage, and retrieval
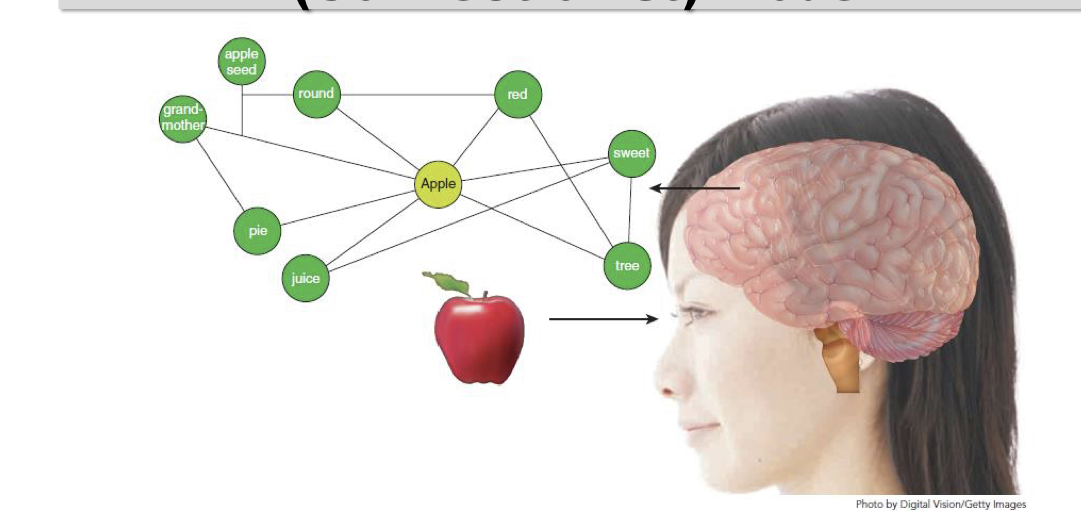
–Parallel Distributed-Processing Model – information is represented in the brain as a pattern of activation across entire neural networks
Information processing model (sensory memory)
• We are presented with a stimulus and our brain retains a sensory memory of it for less than a second
• Sensory memories include: –What we see (iconic memory) –What we hear (echoic memory)
Information processing model (working memory and long term memory)
If we pay attention, information enters our....
• Working (short-term) memory, which holds information for 30 seconds; capacity is 5-9 items
If we encode the information, it enters our...
• Long-term memory, which stores information forever
requires the person to pay attention to it and encode it
Information processing model (overview)
• Memory is similar to a computer – different storage locations for different kinds of information
– Sensory memory – desktop icons
– Working memory – open files that disappear unless saved
– Long-term memory – the hard drive
Parallel distributed processing (connectionist) model and contrast with IPM (Information processing model)
Memories are stored in a network of associations throughout our brains
– Contrast with the IPM (Information processing model) model of memory that says that material is processed and remembered in stages
– It’s a subtle difference but it has implications for understanding how memories are formed and later recalled
TLDR: the connectionist model suggests memories are interconnected, while the IPM emphasizes sequential stages.
2 ways to encode
Automatic processing: when you remember something without much conscious awareness or effort
Effortful processing: when you remember something with careful attention and conscious effort
Automatic processing
Often used for remembering matters of time, space, and frequency
– E.g. we can remember the path from our front door to our bedroom, we remember where things are in relation to us
Effortful processing
• Used for a lot of other stuff that we want to remember
– E.g. studying for class, remembering someone’s name or phone number, etc.
Attention vs awareness
• To encode anything into memory using either type of processing, we need to pay attention to it
• But we are only aware of it in effortful processing
sensory memory
memory involving detailed, brief sensory images or sounds retained for a brief period of time:
• a photograph viewed for a brief moment
• a brief glance at a passing car
• random letters examined for less than a second
Working memory and rehearsal
a short-term memory store for information you are thinking about right now, including:
• recalled memories, such as a phone number
• what you are reading
Rehearsal – consciously repeating information to ensure it is encoded
Long term memory
all of the information we have gathered that is available for use, such as acquired skills, people we know, and past feelings
Spaced practice effect
facilitates moving working memories into long-term memory by rehearsing over time
– Don’t cram! Studying a little bit over a long period of time is better for memory.
3 types of encoding
• Phonological – encoding based on sound
• Visual – encoding based on how the information looks
– People with amazing visual encoding skills have eidetic (photographic) memory
• Semantic – encoding based on the meaning of the information
understand and elaborate (methods of effortful encoding)
• Understand – we remember things better when we can understand what it means
• Elaborate – the more we can elaborate (or expand) on the meaning and make the information personally relevant, the better we remember it
Mnemonic devices (method for effortful encoding)
Use mnemonic devices – techniques used to increase meaningfulness of information to make it more memorable
– HOMES
– Every Good Boy Deserves Fudge
– 30 days hath September...
– "How I want a drink, alcoholic of course, after the heavy lectures involving quantum mechanics."
Chunking and schemas (methods for effortful encoding)
• Use chunking – group bits of information together – E.g. remembering phone numbers
• Use Schemas – organize new information according to the categories created by previous experience and learning
– If you’ve been in one university class, you have a decent schema that will guide how you behave in a new, different class
PQRST method (method of effortful encoding)
• Use the PQRST Method
– Preview: skim it first, identify key themes
– Question: turn each subsection into a question that
you’ll answer as you read
– Read: try to answer the questions you posed yourself
– Self-Recitation: ask and answer questions aloud to
yourself
– Test: practice recalling information from what you read
Storage limits of memory
• Once information enters working memory, it can be stored for only a limited period of time (about 30 sec). This kind of memory is either passed on to long-term memory or lost.
• Memory span = max. number of items that can be recalled in the correct order
Types of long term memories (2)
Explicit Memory – memory that a person can consciously bring to mind (e.g., home address or date of birth)
Implicit Memory – memory that a person is not consciously aware of, such as learned motor behaviours, skills, and habits (e.g., riding a bike)
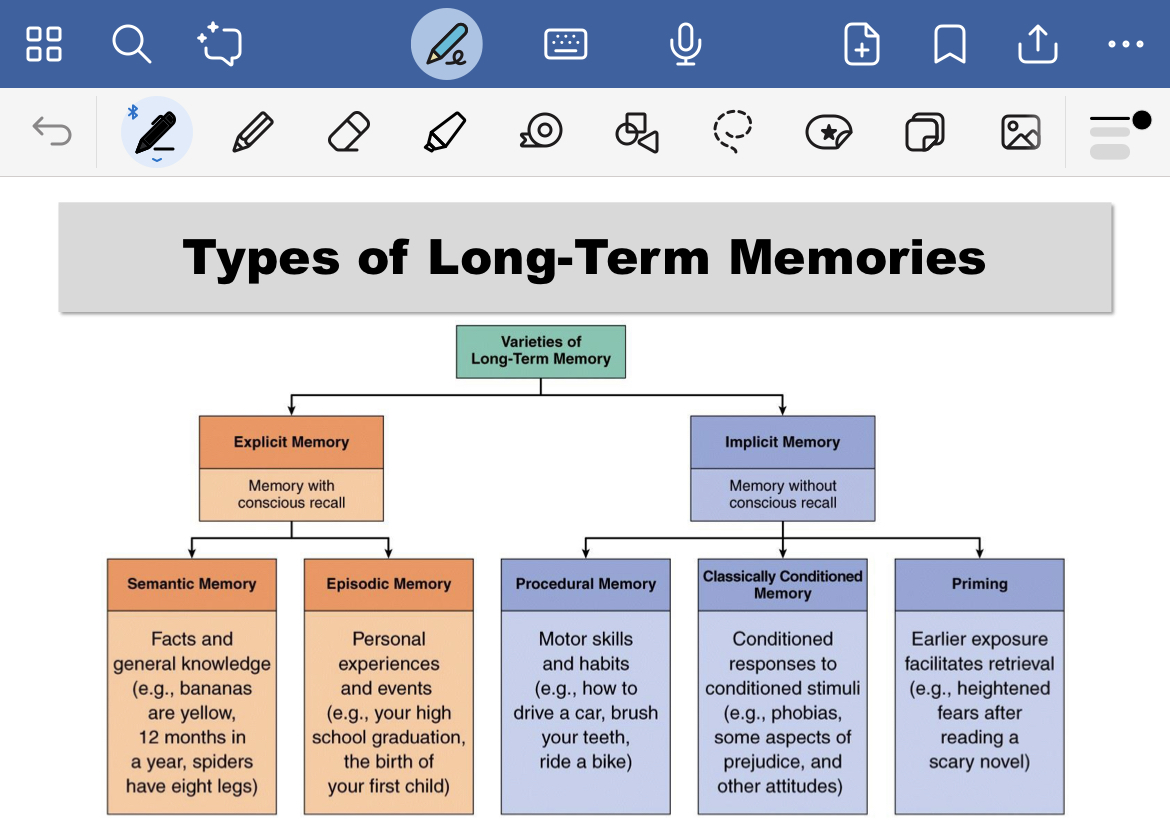
2 types of explicit memories
• Semantic
–Memory of general knowledge of the world
• Episodic
–Memory of personal events or episodes from one’s life
3 types of implicit memory
• Procedural memory – Motor skills and habits
• Classically conditioned memory
– Conditioned responses like fear, disgust, excitement, etc.
• Priming
– Exposure to something in your environment that makes a memory more accessible (e.g. seeing an ad reminding
How are long term memories organized
• This is still not fully understood
• Regardless of their precise organization, pieces of information stored in long-term memory are linked to each other, forming a vast network of interwoven associations
How are memories retrieved
• Mentally search brain for stored information
• If it is located, then it is brought back into working memory
• Activity: Write down the provincial capitals of Canada
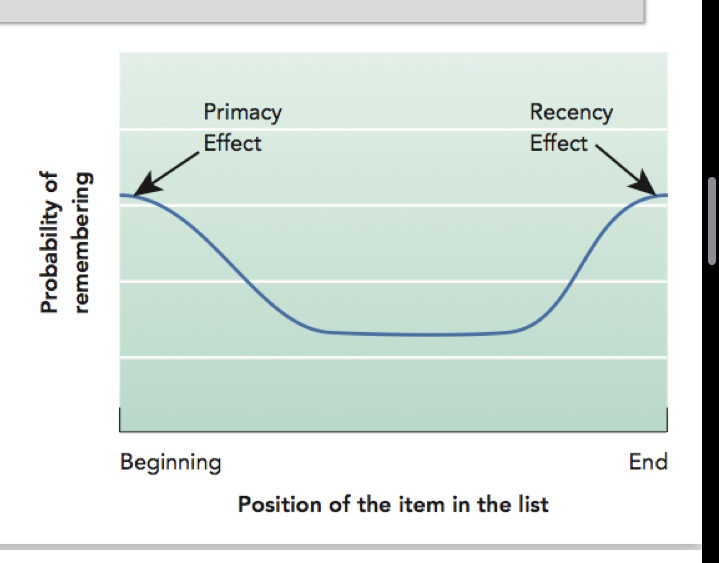
Serial position effect (2 effects)
• Primacy effect: more likely to remember things heard first
– Happens when asked after a delay
• Recency effect: more likely to remember things heard most recently
– Happens when asked soon after learning
Retrieval cues and context effects (helps with retrieval)
• Retrieval cues – words, sights, or other stimuli that remind us of the information we need to retrieve from our memory
• Context effects – we can remember things better where we first learned them
(How the environment or situation (context) influence the way we perceive, remember or interpret info)
Encoding specificity principle and priming (helps with retrieval)
• Encoding specificity principle – the original context (location or situation), mood, or state in which we learn material is loaded with retrieval cues, which leads to memories of the original event ie: going back to the area where the info was learnt can help retrieve the info
• Priming – one piece of information helps us retrieve other related memories
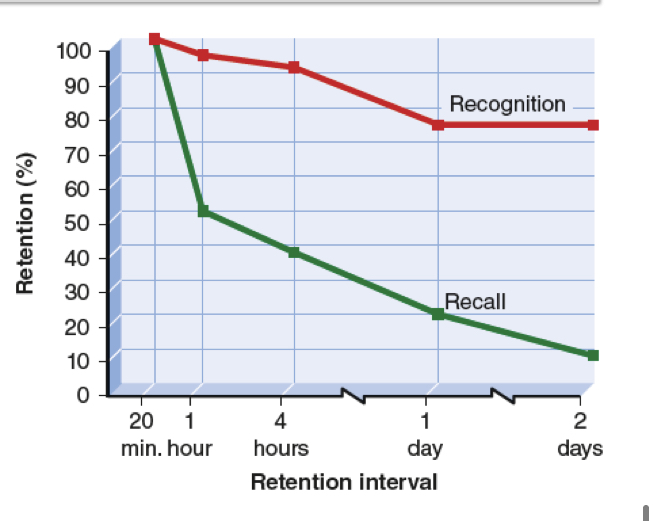
Recognition and recall
• Recognition tasks are easier than recall tasks because of priming.
State dependent memory
• You remember things better when you are in the same state of mind you were in when you first learned it.
– Similar to context dependent memory but different
Flashbulb memories
• Detailed memories of an emotionally significant event, or of the circumstances surrounding the moment we learned about the event
–E.g. for my generation: 9/11
–Not necessarily more accurate than any other memory
Forgetting
• The inability to recall information that was previously encoded into memory
• May be due to failure of attention or lack of retrieval cues
3 possible reasons for retrieval failure
• Decay theory
• Interference theory
• Motivated forgetting
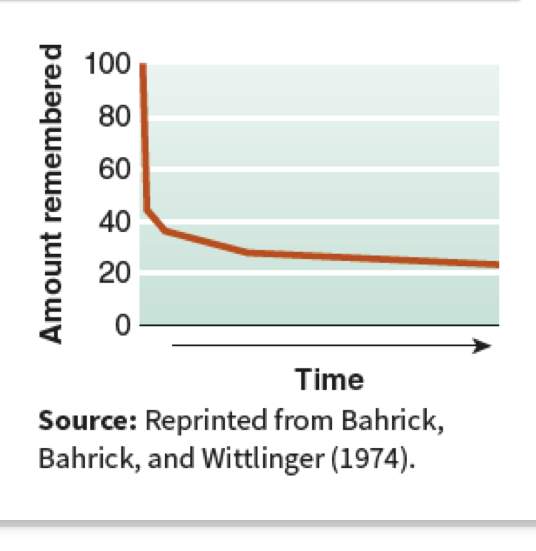
Decay theory
• Memory traces (physical traces in brain) fade over time if they are not used
• Forgetting curve – we forget a great deal very rapidly, but the forgetting levels off and the amount of information we retain stabilizes
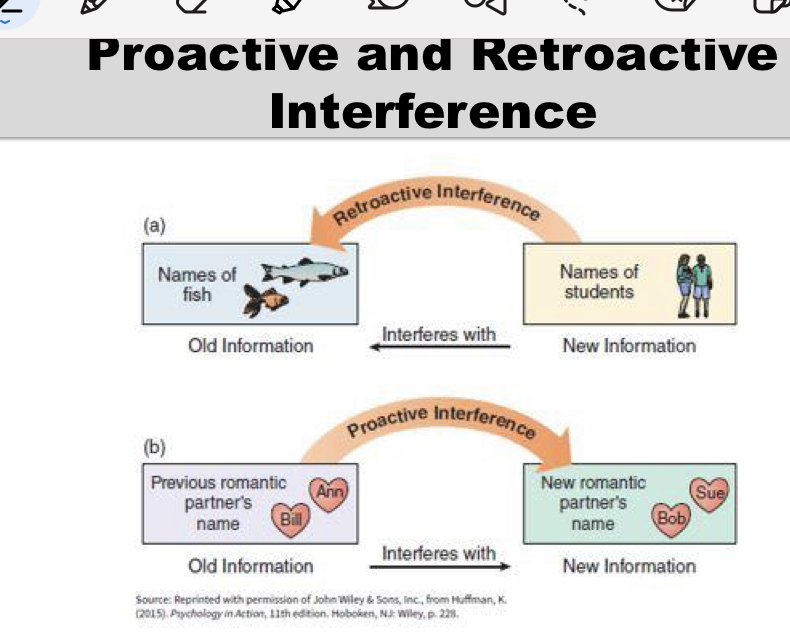
Interference theory
Forgetting is influenced by what happens to people before or after they take information in
• Proactive interference – competing information that is learned before the forgotten material, preventing its subsequent recall
• Old info interferes with new
• Retroactive interference – learning of new information
disrupts access to previously recalled information • New info interferes with old
Proactive and retroactive interference
Motivated forgetting and repression
We may forget information that is unpleasant, embarrassing, or painful
• Repression – process in which we unconsciously prevent some traumatic events from entering our awareness so that we do not have to experience the anxiety or blows to our self-concept that the memories would bring
3 factors that contribute to memory distortion (distracted or manufactured memories)
Memories are subject to distortions because we often have to reconstruct them.
Three factors that contribute to memory distortions are:
• Source misattributions – remembering information, but not its source, may lead to remembering information from unreliable sources as true
• Imagination – memories can be distorted by false information that comes from within, from our imaginations
• Misinformation – exposure to new information, particularly misinformation, can also lead to the distortion or the manufacture of false memories
Hypnosis (distorted or manufactured memories: misinformation)
• Hypnosis and memory
• Hypnosis in therapy, law enforcement, and other contexts has been shown to cause people to distort or manufacture memories, rather than rediscover them.
Memory in the brain (Memory consolidation, potentiation and Long term potentiation, prefrontal cortex’s importance in what?)
• There’s no specific “memory” region
• The prefrontal cortex is particularly important in
working memory
• The hippocampus is important for the transfer of memories into long-term memory
• Memory consolidation – process by which memories stabilize in the brain
• Potentiation – synchronous networks of cells firing together
• Remember the idea of neural circuits
• Long-term potentiation (LTP) – a phenomenon where repeated stimulation of certain nerve cells in the brain greatly increases the likelihood that the cells will respond strongly to future stimulation
• It’s like blazing a trail in the brain that makes subsequent travel easier
Infantile amnesia (memory and age)
Before four years of age, we have memories of faces, places, and skills, but not memories of life events
• The hippocampus develops slowly
• Most early episodic memories are emotional
• Some types of memory decline with age, starting in our 20s
• Prospective memory – ability to remember content in the future; i.e. remembering to do an action in the future
• Retrospective memory – ability to remember content from the past
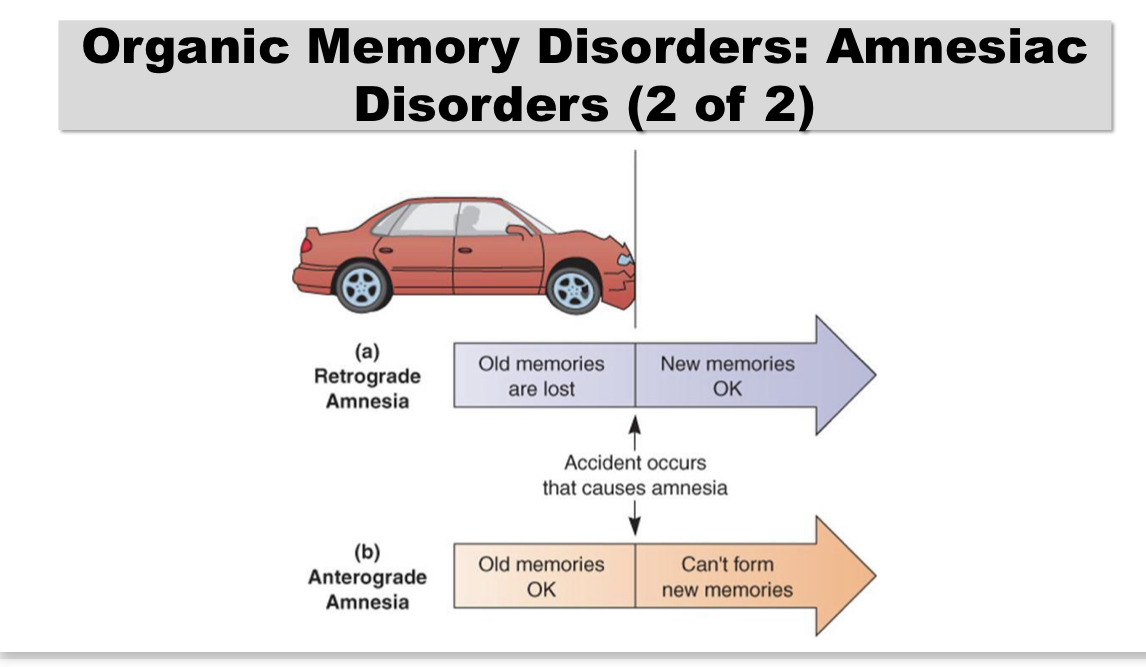
Amnestic disorders (2 of them) (organic memory disorders)
Amnestic disorders – organic disorders in which memory loss is the primary symptom
• Anterograde amnesia – can’t form new memories
– “Hi. I’m Tom....Hi. I’m Tom”
• Retrograde amnesia – can’t remember
things before amnesia-inducing event – “Who am I?”
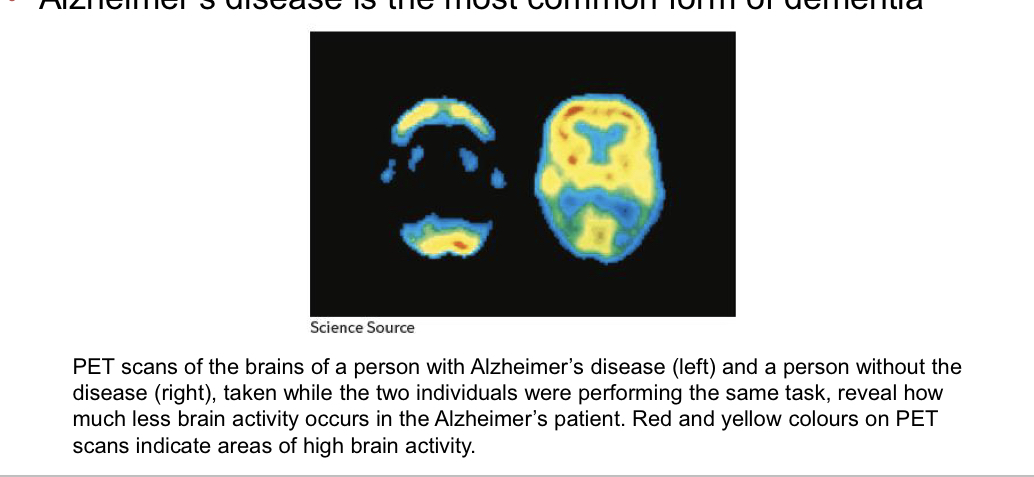
Dementia (organic memory disorder)
severe memory problems combined with losses in at least one other cognitive function, such as abstract thinking or language
• Alzheimer’s disease is the most common form of dementia
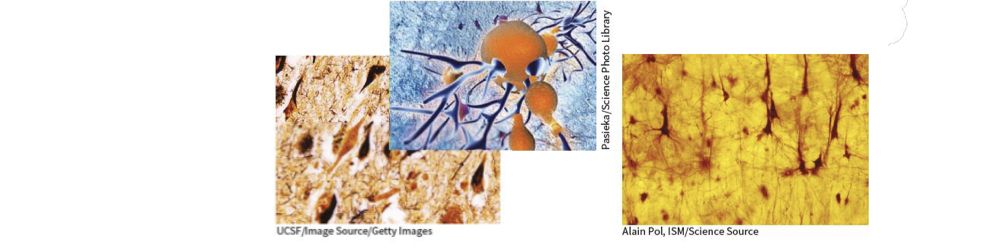
Plaques and tangles of Alzheimer’s disease
Both senile plaques (protein fragments that accumulate between neurons) and neurofibrillary tangles (insoluble fibres that twist together) are thought to damage neurons in the brains of Alzheimer’s patients (both shown on the left). Plaques and tangles are absent in the healthy brain (right).
Consciousness
immediate awareness of our internal and external states
• Everything you are thinking about right now!
• Your awareness of your surroundings and yourself
• Stream of consciousness—a continuing flow of changing thoughts (William James, 1890)
Different level of consciousness
• When we are awake
– Usually what we think of when we think of consciousness.
– We are awake and aware of what’s going on around us
– But our degree of awareness varies a lot
• Conscious awareness
• Preconsciousness
• Unsconscious state (not the same as being unconscious in the way someone is when they’re passed out)
• Most of our neurons are active.
• We don’t merely use 10% of our brains, we use it all.
• Brain activity = consciousness
When we are asleep
– We are “unconscious” in a meaningful way but still very much
alive and sensitive to external stimuli
• When we do other things that influence our level of awareness
Different altered states of consciousness
“A change in a person’s ability to be fully aware of their external surroundings and internal states.”
• Being asleep
• Hypnosis
• Meditation
• Drugs
2 components of consciousness whilst awake
•States of consciousness – level of awareness for our external surroundings and internal states
• Differentiated by the amount and type of attention we’re able to pay to stimuli
Contents of consciousness – specific thoughts we are aware of about our internal states or external surroundings
Inattention blindness
if you aren’t paying attention to something visual, you are unable to report on the details of what the visual stimuli contain
attention alone is not consciousness
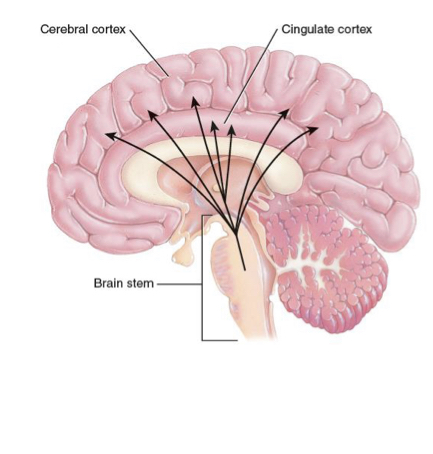
Reticular formation and conscious awareness
• Reticular formation
– Role in being awake and, therefore, consciousness
– Damage results in inability to stay awake; associated with comas
Thalamus, hypothalamus and consciousness
• Thalamus and hypothalamus
– An awake brain needs information processed
– Signals from reticular formation go to and through thalamus and hypothalamus
– Damage or dysfunction in these pathways can result in things like narcolepsy or comas
Cerebral cortex and conscious awareness
• Cerebral cortex
– Important for the “awareness” aspect of consciousness
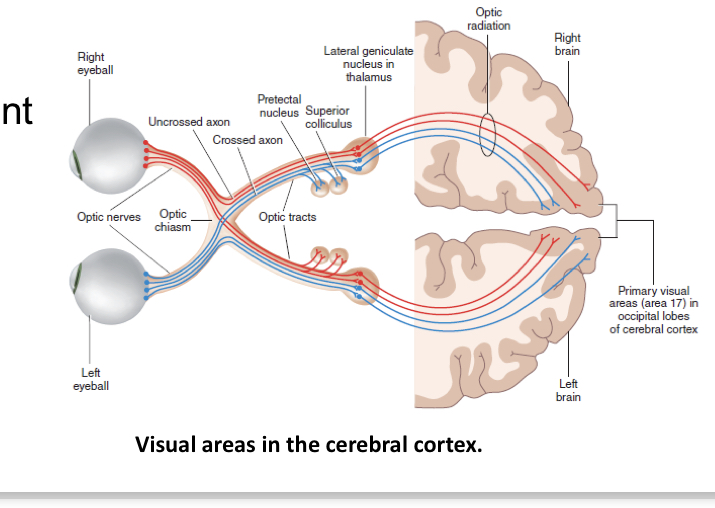
Case of blind sight and illustration of separate roles of diff parts of brain in sensing stimuli
• The case of “blindsight” helps illustrate the separate roles of different parts of the brain in ”sensing” stimuli and being “aware” of stimuli
– Primary visual cortex destroyed, leading to blindness
– But individuals could still point to a spot of light and dodge obstacles
– This suggests that parts of the brain are still registering external visual stimuli but the individual is not aware of it
Overall conscious awareness and the brain (reticular formation, hypothalamus and thalamus, cerebral cortex and blind sight)
• Reticular formation
– Role in being awake and, therefore, consciousness
– Damage results in inability to stay awake; associated with comas
• Thalamus and hypothalamus
– An awake brain needs information processed
– Signals from reticular formation go to and through thalamus and hypothalamus
– Damage or dysfunction in these pathways can result in things like narcolepsy or comas
• Cerebral cortex
– Important for the “awareness” aspect of consciousness
• The case of “blindsight” helps illustrate the separate roles of different parts of the brain in ”sensing” stimuli and being “aware” of stimuli
– Primary visual cortex destroyed, leading to blindness
– But individuals could still point to a spot of light and dodge obstacles
– This suggests that parts of the brain are still registering external visual stimuli but the individual is not aware of it
Conscious awareness and cerebral cortex within split brain patients
• Remember how information processed in different visual fields was accessible only to certain parts of the brain.
Development of consciousness
• Babies aren’t great at describing their feelings of consciousness to us
– But we can tell that they pay attention to things, hold concepts in mind (memory), engage in planned behaviour
• Conscious awareness of self (i.e. noticing that you are a unique being separate from others) seems to develop around 18 months
• Full conscious awareness develops at around 22 months
– This age is associated with more advanced language use, the ability to reason inductively, and categorize concepts
2 awake sates other than consciousness
• Preconsciousness and Unconsciousness
–The difference is about the level of awareness one has
Preconsciousness and automatic behaviours
level of awareness in which information can become readily available to consciousness if necessary
• It’s not currently in our awareness but it’s accessible
• Example: What did you do last weekend?
• Recall our discussion of working memory, implicit memory, and priming
Automatic Behaviours – a type of preconscious behaviour of which occur without conscious thought or intention
• Example: Do you remember every step each time you brushed your teeth last week?
Unconscious state
Unconscious state – state in which information is not easily accessible to conscious awareness
• Not the same as “being unconscious”
• Example: What did you eat last weekend?
• Analogous to information in long-term memory that we can’t retrieve
evidence for unconscious “awareness”
•Implicit memory – knowledge that we have stored in memory that we are not typically aware of or able to recall at will
• The contents of our implicit memory allow us to perform a variety of tasks/skills without thinking deeply about all the individual parts of the task/skill.
• E.g. riding a bike, “gut reaction” decisions in high- stakes scenarios
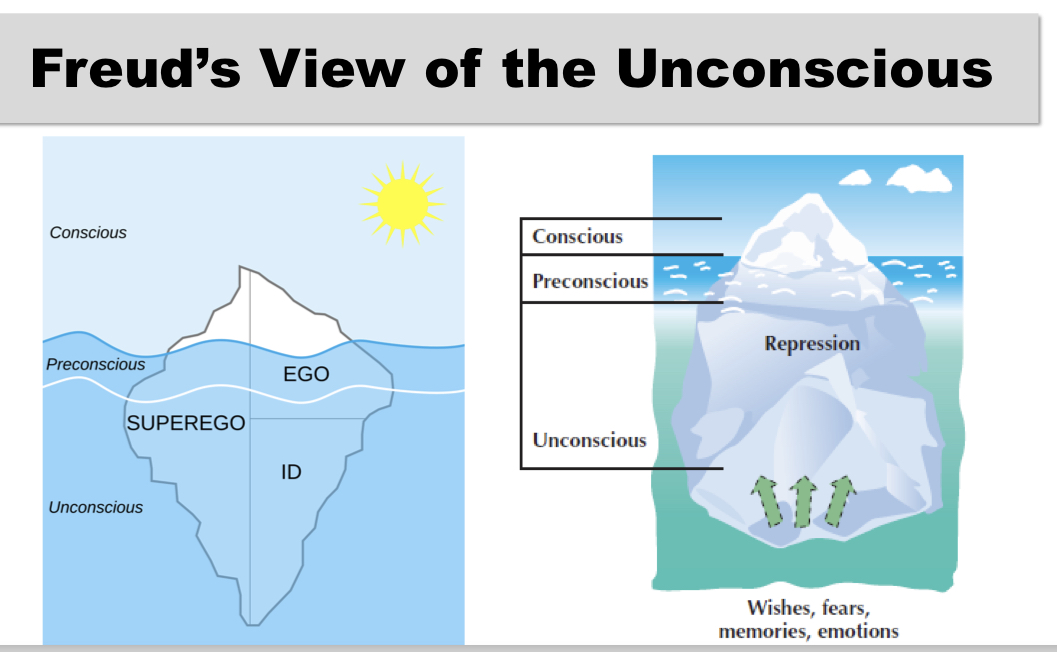
Freud’s view of unconsciousness
• Freud is a major reason we started thinking about the “unconscious” in the first place
• Freud imagined a very large role for the unconscious mind.
• Not only does the unconscious contain a lot of stuff but it also guides our behavior in a whole bunch of ways, according to Freud.
Adaptive theory of sleep
theory that organisms with bad night vision hide and sleep at night for the purpose of self-preservation, to keep away from predators
Restoration theory (theory of sleeping)
holds that sleep restores our brains and bodies; restores depleted resources, cleans up “waste” that has accumulated throughout the day
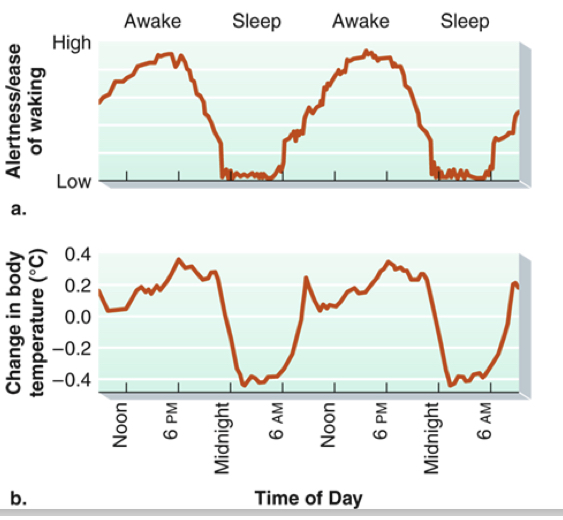
Circadian rhythm (biological clock)
– pattern of sleep-wake cycles that in human beings roughly corresponds to periods of daylight and night
• We experience changes in alertness and body temperature in predictable ways during sleep/waking.
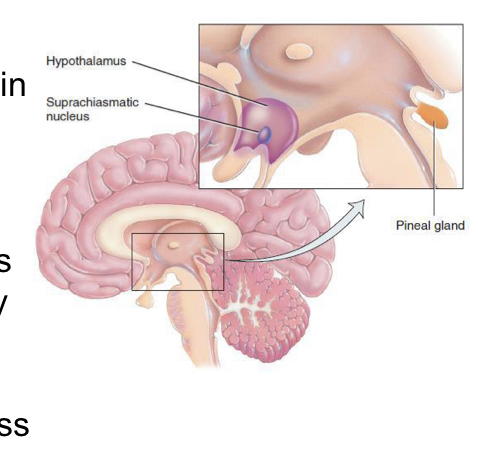
Role of the brain in sleeping and the suprachiasmatic nucleus
• Sensory signals about daytime/nighttime tell parts of our brain to prep for sleep/waking
• Suprachiasmatic nucleus: a small group of neurons in the hypothalamus responsible for coordinating the many rhythms of the body.
• Directs pineal gland to produce melatonin, which triggers sleepiness
Controlling of the internal biological clock
• During the day, photoreceptors in the retina of the eye, send signals to the SCN (Suprachiasmatic Nucleus) about daylight, which helps regulate dopamine and melatonin production
– This is why artificial lighting has an impact on our sleep quality
• In the total absence of natural light, our SCN may extend our body’s “day” and disrupt our circadian rhythm.
• We return to a natural rhythm quickly upon being exposed to natural light
Sleep cycles (how it can be measured and overall cycles within ppl)
• Using EEG we can measure patterns of brain activity while people sleep
• Different patterns of brain waves denote different stages of sleep
• We go through these stages in order and on repeat
Sleep cycle
• 90 to 100 minutes per sleep cycle
• One cycle consists of five stages
• Over the latter part of the night, we spend most time in stages 1 and 2 and REM sleep
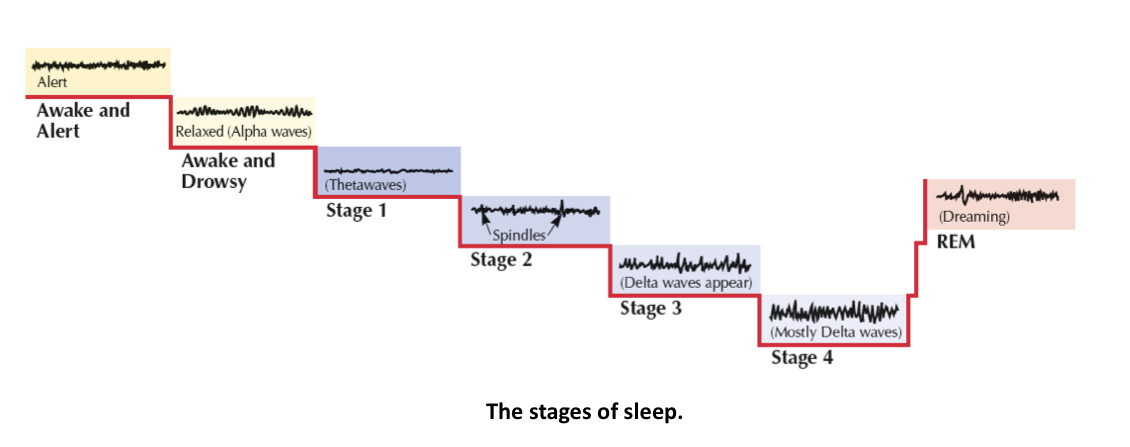
stages of sleep
Pre-sleep period (hypnagogic state)
• Alpha waves
• Hypnagogic hallucinations
– Vivid sensory hallucinations
– E.g. “Exploding head syndrome”
• Myoclonic jerk
– Muscle spasm that accompanies hypnagogic hallucination of falling
Stage 1 – a few minutes
• Bridge between wakefulness and sleep
• Alpha waves change to slower theta waves
Stage 2 – 15 to 20 minutes
• More relaxed
• Rhythmic breathing
• Sleep spindles (burst of rapid brain waves)
Stage 3
• Deep sleep
• 20%-50% delta waves
Stage 4
• Heart rate, blood pressure, breathing rates at lowest levels
• Muscles relax
• Sleepwalking more likely
Stage 5
• Rapid eye movement (REM) sleep
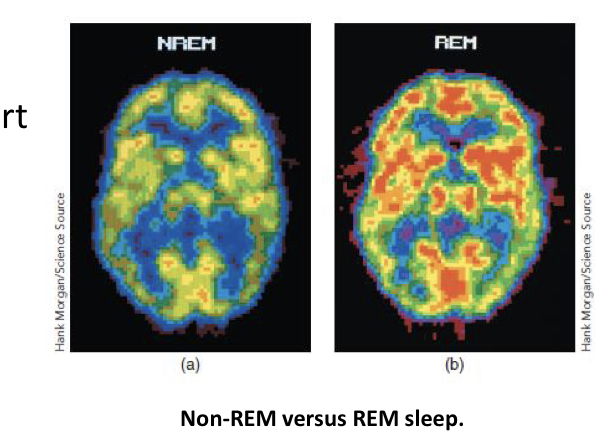
Rapid eye movement (rem) sleep
A stage of sleep is associated with rapid and jagged brain wave patterns, increased heart rate, rapid and irregular breathing, rapid eye movements, and dreaming
Dreams
• Extra brain activity while asleep
• Dreams involve processing information from the day (i.e., encoding memory and problem solving)
• Dreams could be a mental realm where we can solve problems and think creatively
Activation synthesis model of dreaming
• During sleep, the brain has a lot of random activity via brainstem activity that activates the sensory systems of the cortex
• Dreams reflect the brains efforts to make sense out of or find meaning in the neural activity that takes place during sleep
Freudian dream theory
• Dreams represent the expression of unconscious wishes or desires
• Not much evidence for this theory.
Notable types of dreams (3 types)
– Nightmares – dreams filled with intense anxiety
– Nightmare or dream disorder anxiety – frequent or distressing
nightmares
– Lucid Dreams – the sleeper fully recognizes that she is dreaming and occasionally actively guides the outcome of the dream
– Daydreams – fantasies that occur while one is awake and aware of external reality, but is not fully conscious
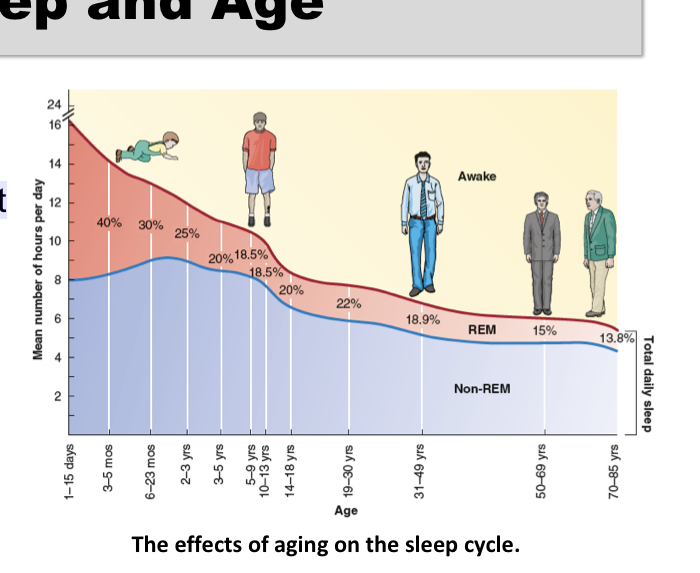
Sleep and age
• Babies spend more time in REM sleep
– Seen as evidence that this is part of how young brains develop
• Sleep requirements change as we age
Sleep deprivation
If we could sleep as long as we wanted, most people would sleep 9–10 hours. But we don’t always get this.
Chronic sleep loss results in:
• General depressed state
• Lower immune system
• Lower ability to concentrate
• Higher incidence of accidents
• Lower productivity and higher likelihood of making mistakes
Sleep hygiene
Practices and routines to help you sleep better
• Make your bedroom a place you associate most strongly with sleep
– Keep it dark, quiet, and cool
– Don’t have devices or screens in your room
• Limit eating/drinking within 3 hours of bedtime – Especially alcohol and caffeine
• Limit naps and physical activity late in the day if you’re having trouble sleeping
Insomnia (1 of 7 sleep disorder)
• Most common
• Difficulty going to sleep or staying asleep
• Caused by stress
• More common in older people due to medical conditions, pain, medications, and depression and anxiety
Sleep apnea(2 of 7)
• Second most common
• Repeatedly stops breathing during night leading to frequent
awakenings
• Possible to have hundreds of attacks per night
• Can lead to cardiac arrest
Excessive daytime sleepiness and narcolepsy (3 of 7)
Excessive daytime sleepiness
• Chronically tired, even if slept well
Narcolepsy
• Uncontrollable urge to fall asleep
• Suddenly fall into REM sleep during the day
• Can last up to 15 minutes
• Genetic factors involved
• No cure
Delayed, advanced sleep phase syndrome and restless leg syndrome and periodic limb movements of sleep(4 of 7)
Delayed sleep phase syndrome
• Long delay in ability to fall sleep Advanced sleep phase syndrome
• Fall asleep between 6 p.m. and 9 p.m. and wake between 2 a.m. and 5 a.m.
Restless leg syndrome
• Strong urge to move legs before sleep
Periodic limb movements of sleep
• Strong urge to move legs during sleep
Sleep walking (5 of 7)
• Mostly occurs during first three hours of sleep
• Eventually returns to bed • Inherited
Night terrors ( 6 of 7)
Night terrors
• Occurs in stages 3 and 4 of sleep
• Child screams in panic; goes back to sleep immediately and does
not remember the event in the morning
• Resolves by adolescence
• May be genetic
REM sleep behaviour disorder (7 of 7)
REM Sleep Behaviour Disorder
• Acting out the dream while in bed and sleeping
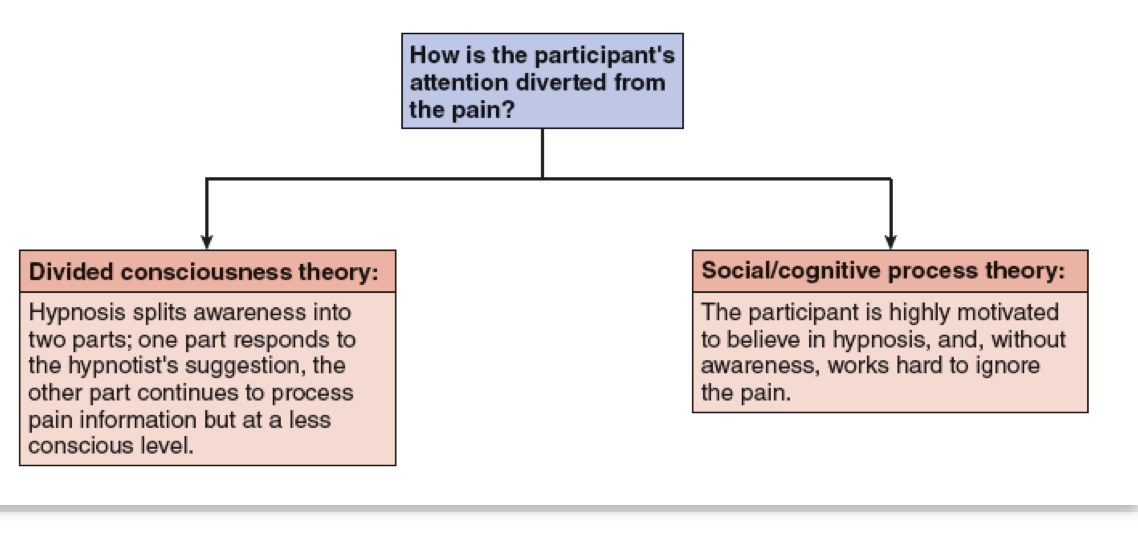
Hypnosis and use in pain relief (Divided consciousness theory and Social/cognitive process theory)
altered state of consciousness, with heightened suggestibility, deep relaxation, and intense focus
• Posthypnotic responses
• Posthypnotic amnesia
• Hypnotic hallucinations
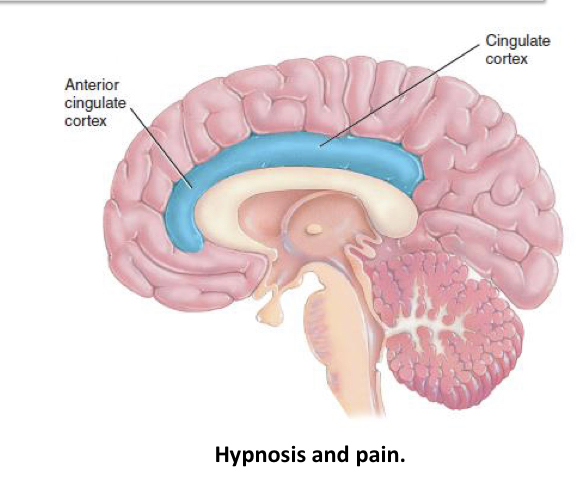
• Decreased activity in anterior cingulate cortex when used to reduce pain
Divided consciousness theory: The patient’s consciousness is divided into 2 parts. 1 part that listens to the hypnotist and other continuous to process pain but less consciously
Social/cognitive process theory: participant is highly motivated to believe the hypnosis, without awareness would work hard to ignore the pain.
Mechanism of hypnosis on the brain
• Neuroimaging research suggests that the brain’s anterior cingulate cortex may be particularly involved when hypnosis is used to anaesthetize or reduce pain
Psychoactive drugs and addiction
Psychoactive drugs – chemicals that affect awareness, behaviour, sensation, perception, or mood
Addiction – a psychological or physical compulsion to take a drug, resulting from regular ingestion and leading to maladaptive patterns of behaviour and changes in physical response
Tolerance for drugs and withdrawal symptoms
Tolerance – mark of physical dependence on a drug, in which the person is required to take incrementally larger doses of the drug to achieve the same effect
Withdrawal symptoms – unpleasant and sometimes dangerous side effects of reducing intake of a drug after a person has become addicted
Depressants and its consequences
– slow the activity of the central nervous system, reducing tension and inhibitions
• Include alcohol and sedative-hypnotic drugs
• Can interfere with judgment, motor activity, and concentration
Sedative-hypnotics (benzodiazepines)
– produces relaxation and drowsiness; relieves anxiety
• Examples include Xanax, Ativan, and Valium
Opioids
– derived from the sap of the opium poppy
• Include opium heroin, morphine, codeine, and OxyContin
• Activate the opioid receptors in the brain, providing their analgesic effect and their related high
• Reduce pain and emotional tension and produces pleasurable and calming feelings
Stimulants
– increases the activity of the central nervous system
• Include caffeine, nicotine, cocaine, and amphetamines
Cocaine’s effects
• Increases energy and alertness
• Produces euphoric feelings of well-being
• Negatively impacts memory, attention, and decision- making ability
Amphetamines effects
• Small doses increase energy and alertness and reduce appetite
• Large doses produces intoxication and psychosis
• Includes methamphetamine (crystal meth) and MDMA (ecstasy), Adderall, and others
Hallucinogens
– produce sensory or perceptual distortions called hallucinations
• LSD
• Magic mushrooms
• Mescaline (buttons, mesc)
• DMT
• Ketamine (special K, cat valium) • PCP
• Cannabis
LSD effects
• Dramatically strengthens visual perceptions (including illusions and hallucinations) along with profound psychological and physical changes
Cannabis effects
• Produces a mixture of hallucinogenic, depressant, and stimulant effects
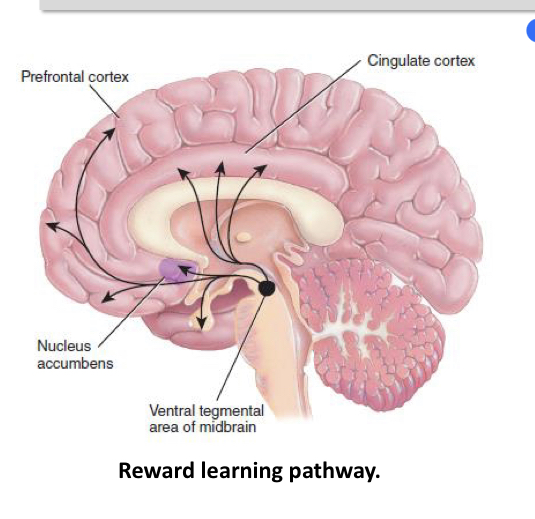
Psychoactive drugs and reward deficiency syndrome
• Psychoactive drugs activate a reward learning pathway, or “pleasure pathway,” in the brain.
Reward-deficiency syndrome – people might abuse drugs because their reward centre is not readily activated by usual life events.
Motivation
any internal process or condition that directs behaviour