Week 9: Transfer Techniques
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
55 Terms
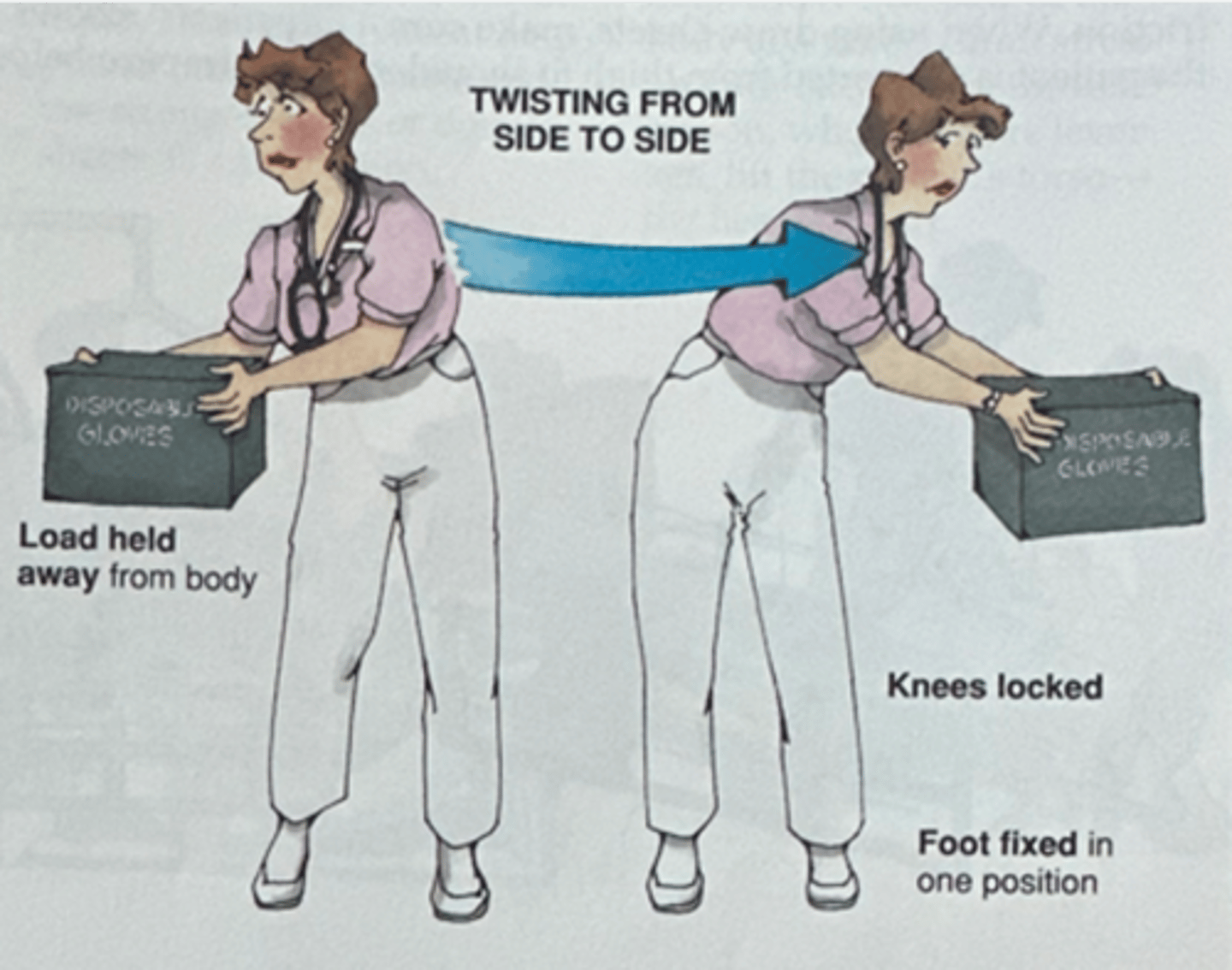
proper body mechanics: twisting (from side to side)
- Load held away from body
- Knees locked
- Foot fixed in one position
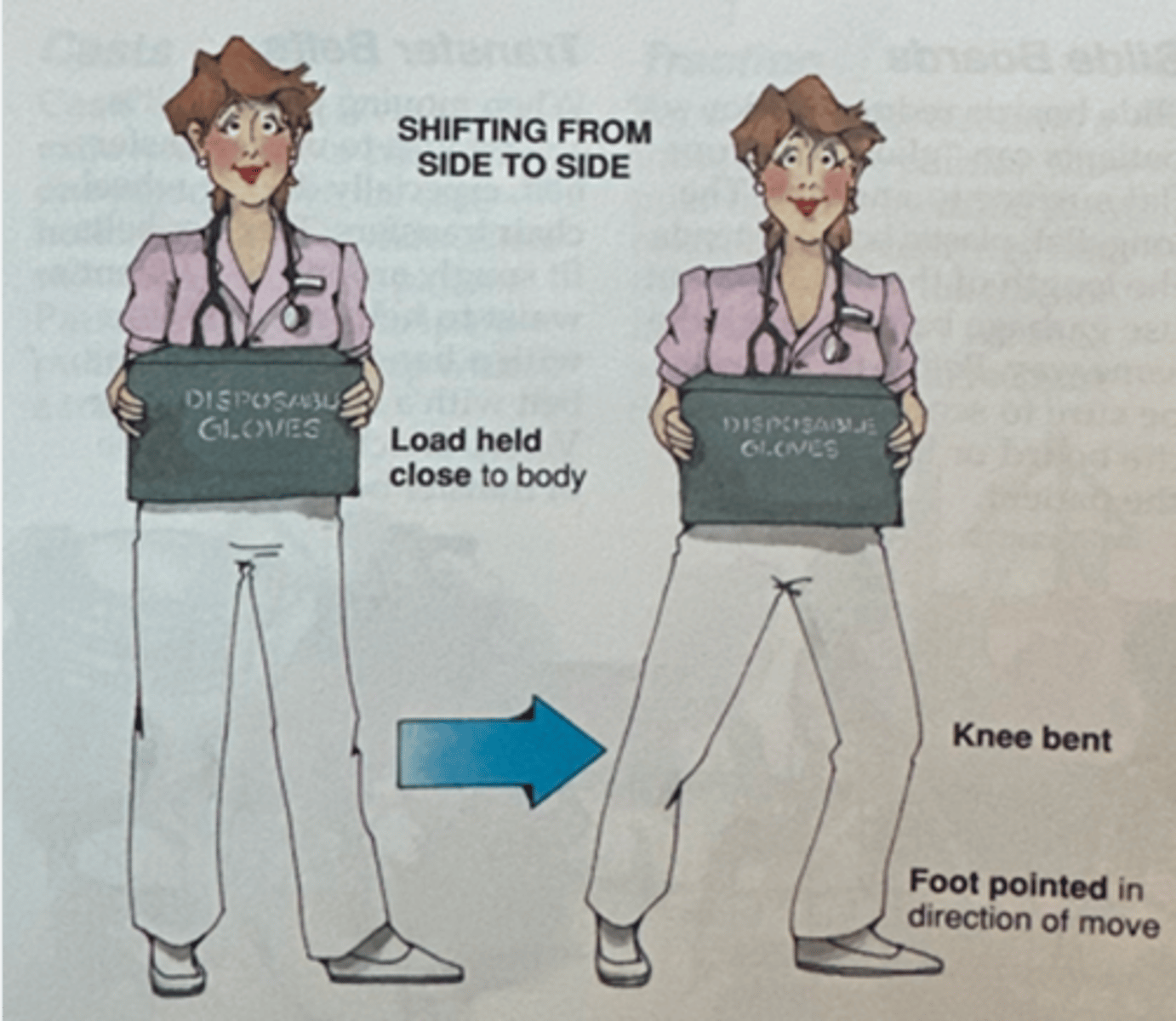
proper body mechanics: shifting (from side to side)
- Load held close to body
- Knees bent
- Foot pointed in direction of move
warm-up
should do this prior to lifting and transferring
gait belt; explain; equipment
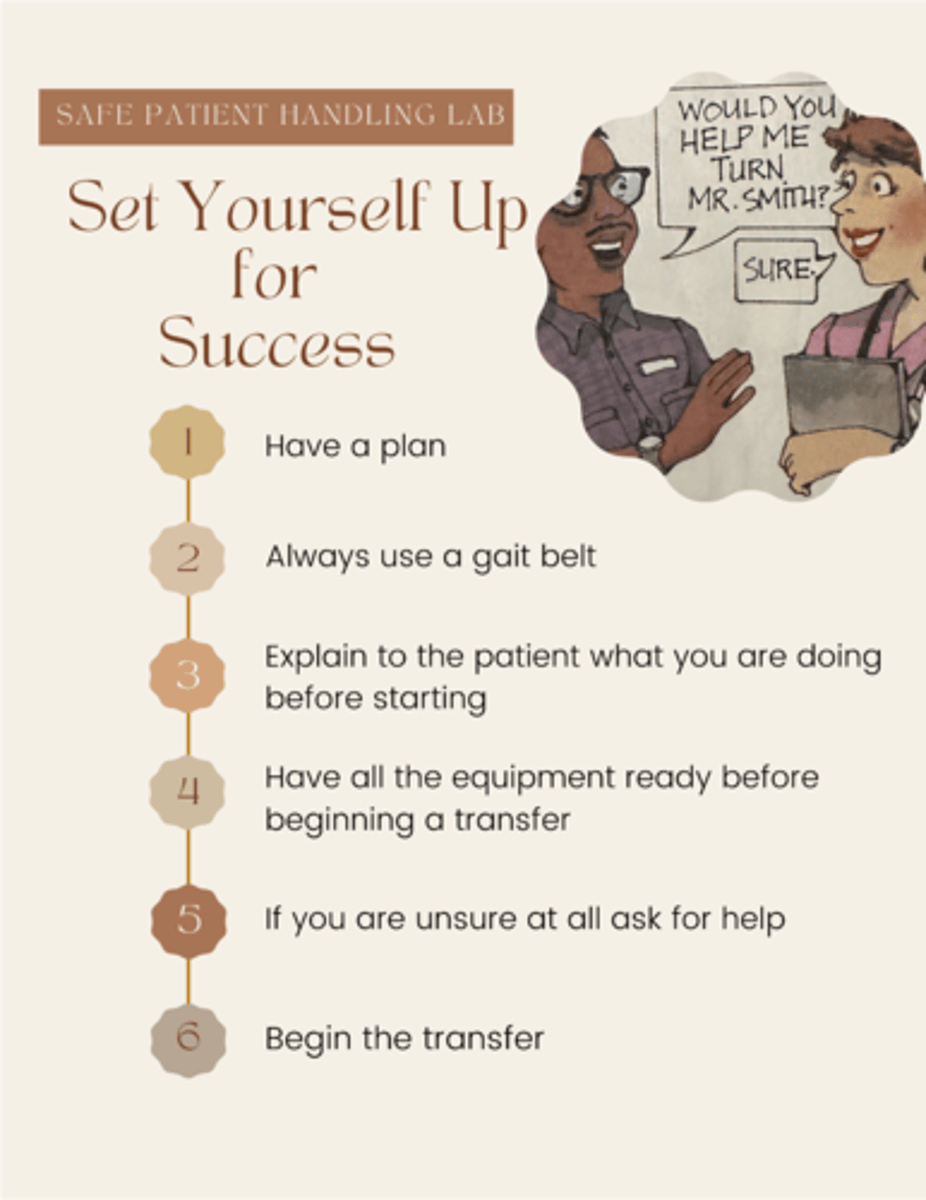
Safe patient handling:
- Have a plan
- Always use a (?)
- (?) to the patient what you are doing before you start
- Have all the (?) ready before beginning a transfer
- If you are unsure at all ask for help
- Begin the transfer
pre-transfer: bed mobility
the ability to move the body in bed to perform activities in the various positions of supine, prone, side lying, or sitting
functional; sensory; breakdown
Bed mobility:
- Promotes (?) positioning
- Optimizes (?) input
- Minimizes risk of skin (?) - shifts weight and reduces pressure on bony prominences
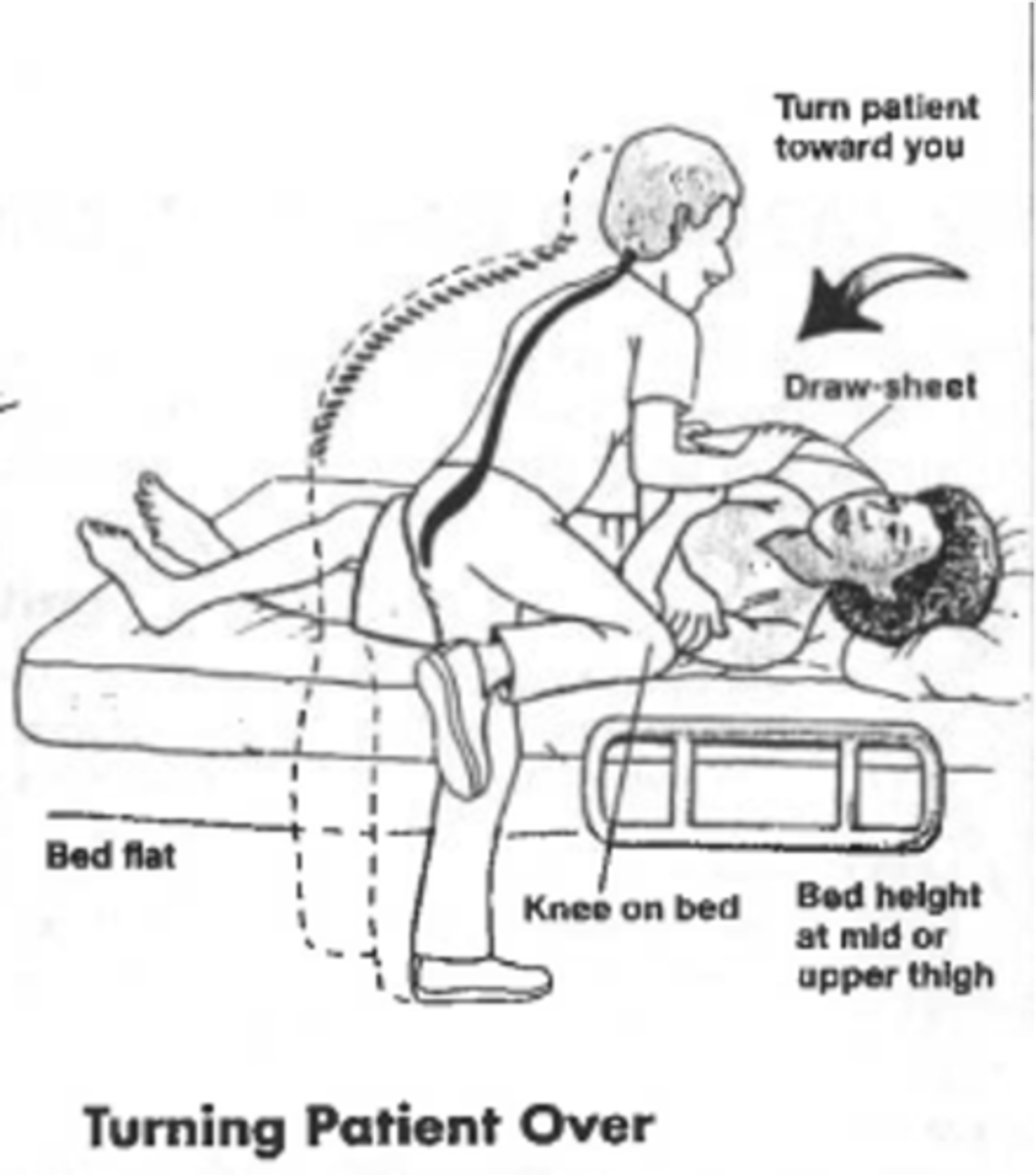
rolling side-to-side, supine to sit, side-lying to sit
basic bed mobility functional tasks
rolling; knees; arm
(?):
- Roll towards (?) side
- Bend (?) and reach for opposite bedrail
- DO NOT pull (?)
lying to sit
(?): move legs off edge of bed at the while pushing with the elbow
side-lying to sit; back
(?):
- Sit close to the head of bed
- Lay on side on bring legs up
- Roll onto (?)
mobility task components
- Bridging (bed pan, reduces pressure on buttocks, scooting in bed, donning pants)
- Long sitting
- Rolling
- Moving legs over side of bed
- Sitting edge of bed
bed --> long sitting --> edge of bed sitting --> out of bed
What is the activity progression of bed mobility?
back; neutral; combine
Proper body mechanics:
- Get close to the client or move them close to you
- Position your body to face the client (face head on)
- Bend the knees; use your legs, NOT your (?)
- Keep a (?) spine
- Keep your heels down
- Don't tackle more than you can handle
- Don't (?) movements
- Use the hospital bed to make transfer easier when needed
weight-bearing; stronger
Client safety practice: transfers
- Proper footwear
- Be aware of IV catheters, open wounds, pressure sores, postural limitations, (?) limitations
- Special patient precautions - pay attention to all limitations and include them in patient instructions
- Transfer toward (?) or less involved side initially
- Instruct patient and give time for them to respond
- Use positioning principles as needed after transfer
T
T/F: A transfer is not considered complete until the patient is safe in the new position.
pelvic tilt
Clients will assume a posterior (?) with prolonged periods of time in the hospital or with their illness. This moves the center of mass back toward the buttocks. You must verbally cue or manually assist client to assume a neutral to slightly anterior tilt to move the center of mass over the center of the body.
trunk alignment
check to see if client's trunk is shifted right or left because this might throw off balance
weight shifting
initiate transfer by shifting weight forward; must be performed no matter what type of transfer you are performing
LE positioning
Client's feet must be placed firmly on the floor with knees at 90 degrees flexion and over the feet. Make sure they have socks or shoes with slip-resistant material.
UE positioning
Either position arms in a safe position or in a position where client can assist with transfer.
stronger; 30-45 degree; brakes
General transfer set-up:
- Position W/C on (?) side
- W/C at a (?) angle
- Lock (?)
- Remove/swing away both leg rests
- Sit at the edge of bed or chair
- Rock them forward and use legs to lift
W/C positioning; armrest
(?):
- Place W/C at approximately a 30-45 degree angle to the surface to which the client is transferring
- Lock the brakes on W/C and bed
- Place both of the client's feet firmly on the ground, hip width apart, with the knees over the feet
- Remove the W/C (?) closest to the bed
- Remove the W/C pelvic seat belt
- Remove the W/C chest belt and trunk/lateral supports if present
bed mobility; W/C
Transfers: sequence of events:
- Pre-transfer: (?)
- During transfer: verbal and/or tactile cues may be given for safety and/or sequencing
- Post-transfer: (?) positioning
medical precautions, weight-bearing status, type of transfer, level of assistance, equipment needed
What are the five most important things to know before a transfer?
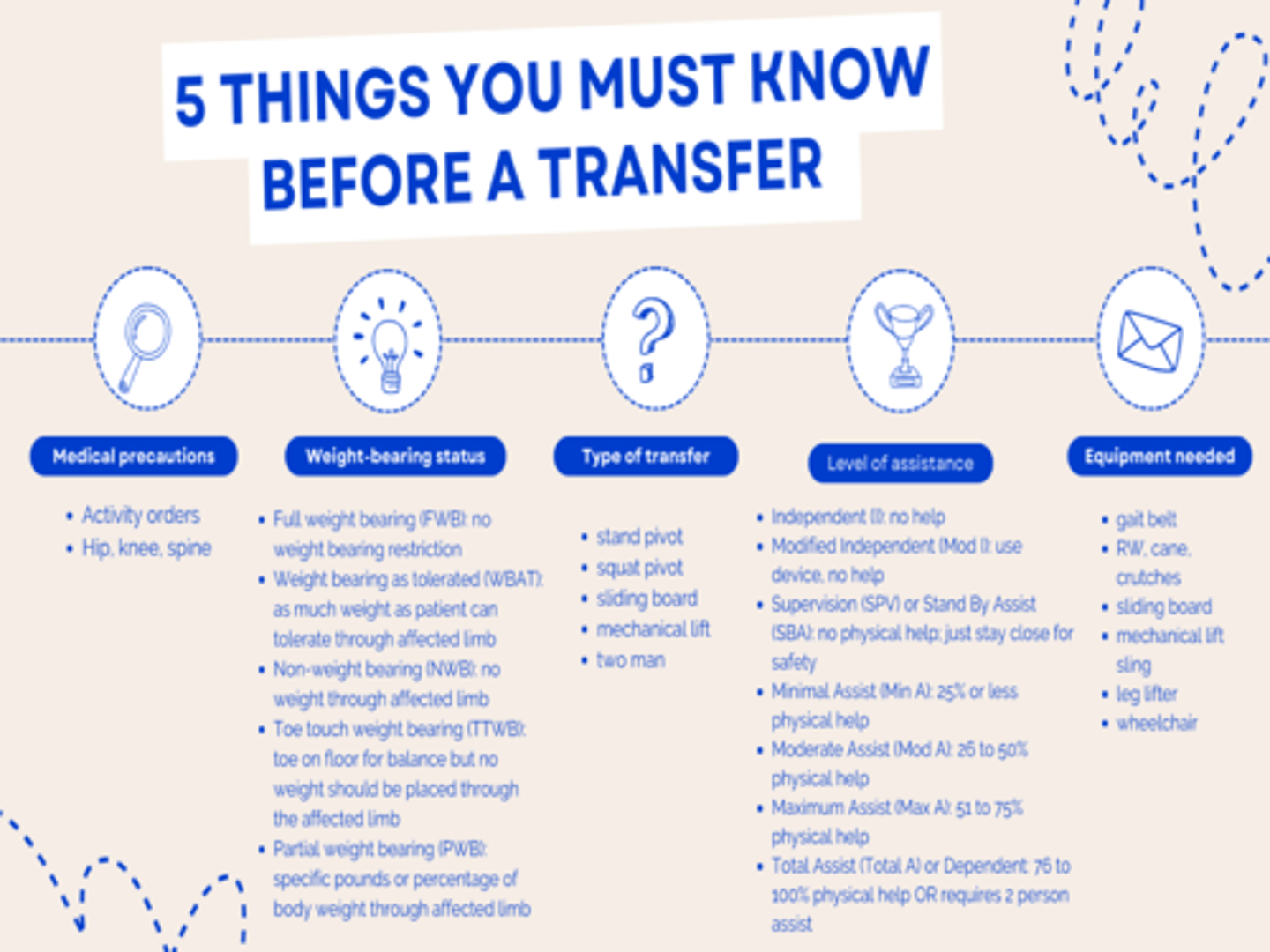
full weight bearing (FWB)
no weight bearing restrictions
weight bearing as tolerated (WBAT)
as much weight as the patient can tolerate through their affected limb
non-weight bearing (NWB)
no weight through affected limb
toe touch weight bearing (TTWB)
toe on floor for balance but no weight should be placed through the affected limb
partial weight bearing (PWB)
specific pounds or percentage of body weight through affected limb
activity orders
- Up ad lib (out of bed)
- Activity as tolerated
- Bedrest with bathroom privilege
- Out of bed
- Ambulate x times a day
- Ambulate with assist
- Weight-bearing status
anterior hip precautions
- No hip extension beyond neutral (ex: stepping backwards)
- No hip adduction (ex: crossing legs)
- No hip external rotation (ex: turning toes out)
posterior hip precautions
- No hip flexion past 90 degrees
- No hip adduction (ex: crossing legs)
- No hip internal rotation (ex: turning toes in)
spinal precautions
BLT:
- No bending
- No lifting heavier than 5 pounds
- No trunk rotation (ex: twisting)
cervical precautions
- No bending neck
- No lifting more than 5 pounds
- No turning head to the side
heterotopic ossification S/S
- Swelling
- Elevated temperature in the area that is swollen
- Decreased ROM of affected joint
DVT - in muscle belly; HO - on a joint
Although the signs and symptoms are similar, what differentiates a heterotopic ossification from a deep vein thrombosis?
T
T/F: For HO patients, you should stretch and/or exercise the affected joint.
sit to stand transfers
- Scoot forward
- Put fleet flat on the floor
- Push up from the surface they're sitting at
- Come to standing position
stand pivot transfers
- Requires client to come to standing position and pivot on both feet
- W/C to bed or mat transfer
- Usually done by patients who can walk
- Place assistive device in front of patient if appropriate
- Instruct patient to push up from the surface they are sitting on with at least one hand - do NOT let them pull on the walker
- Pivot or walk to chair/bed
- Back up to chair/bed so that they are squared up
- Instruct them to reach back for the chair/bed to help them sit slowly
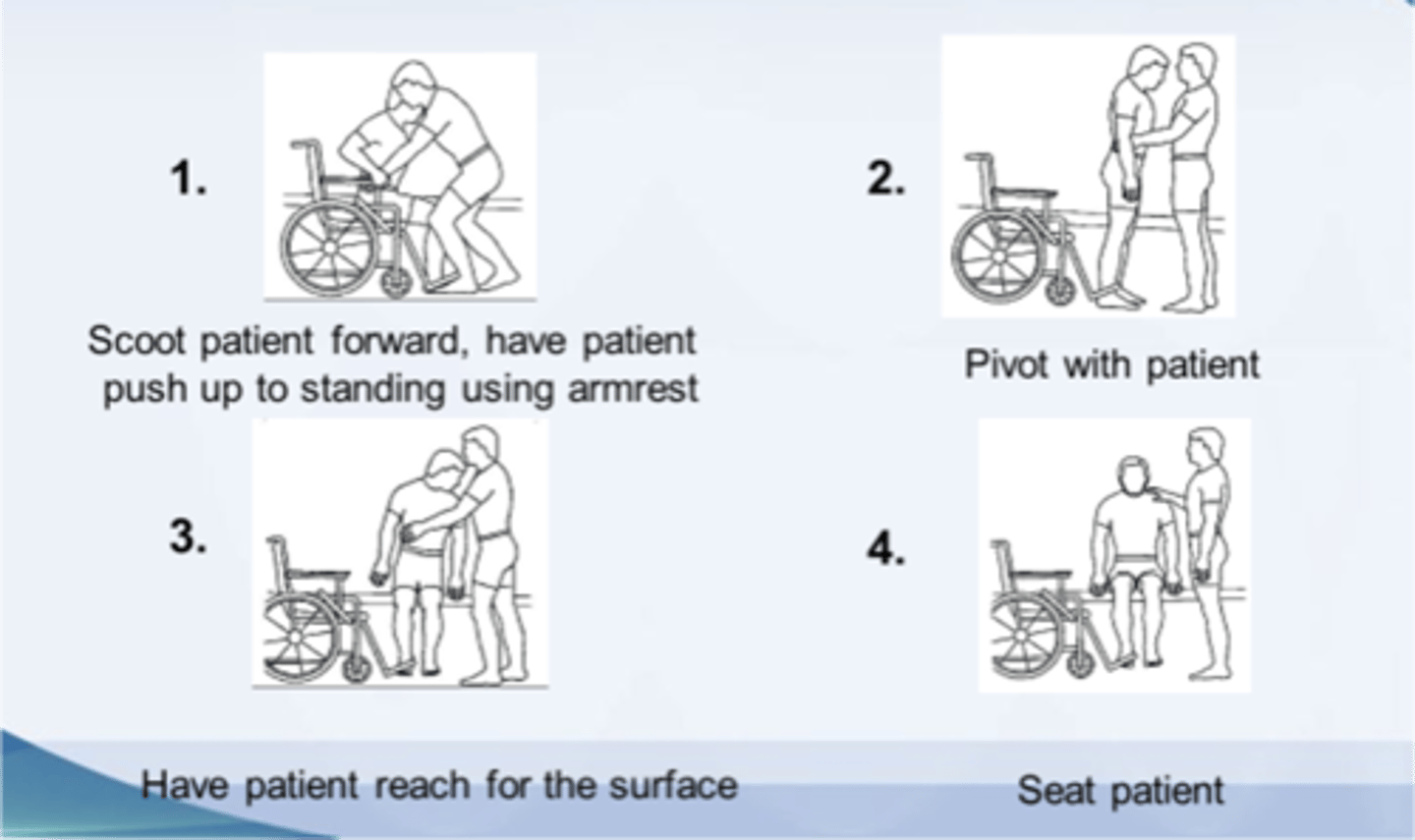
stand pivot transfers
Which type of transfer is used commonly with patients who have hemiplegia, hemiparesis, or general loss of strength/balance?
household transfers
- Sofa or chair
- Toilet and bedside commode
- Bathtub

sit/squat pivot transfers
- Block patient's knee(s) with your knee(s) to prevent buckling
- Have the patient reach for the transfer surface
- Have them help you in lifting their bottom and pivot patient
- Seat patient on transfer surface
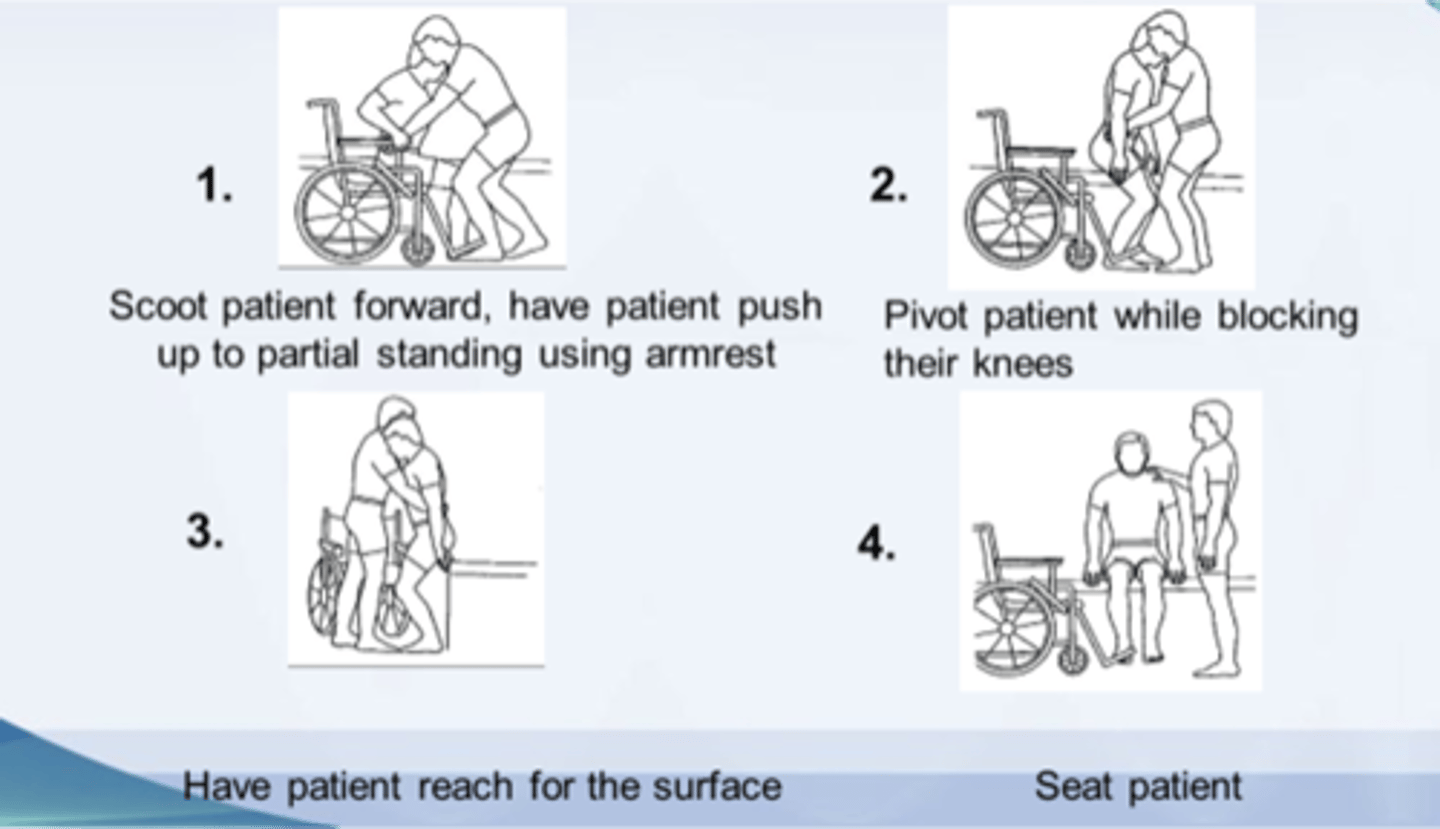
sit/squat pivot transfers
Which type of transfer is used commonly when client cannot initiate or maintain a standing position?
sliding board transfers
- Remove armrest between patient and transfer surface
- Angle bottom closer to transfer surface with knees facing in opposite direction
- Have patient lean to the side and place sliding board approximately halfway under upper thigh
- Squeeze patient's knees with your knees OR block both knees with your knees
- Make sure patient leans forward and uses head/hip relationship
- Have patient reach for opposite armrest or end of sliding board
- Slightly lift patient while you slide them along the board
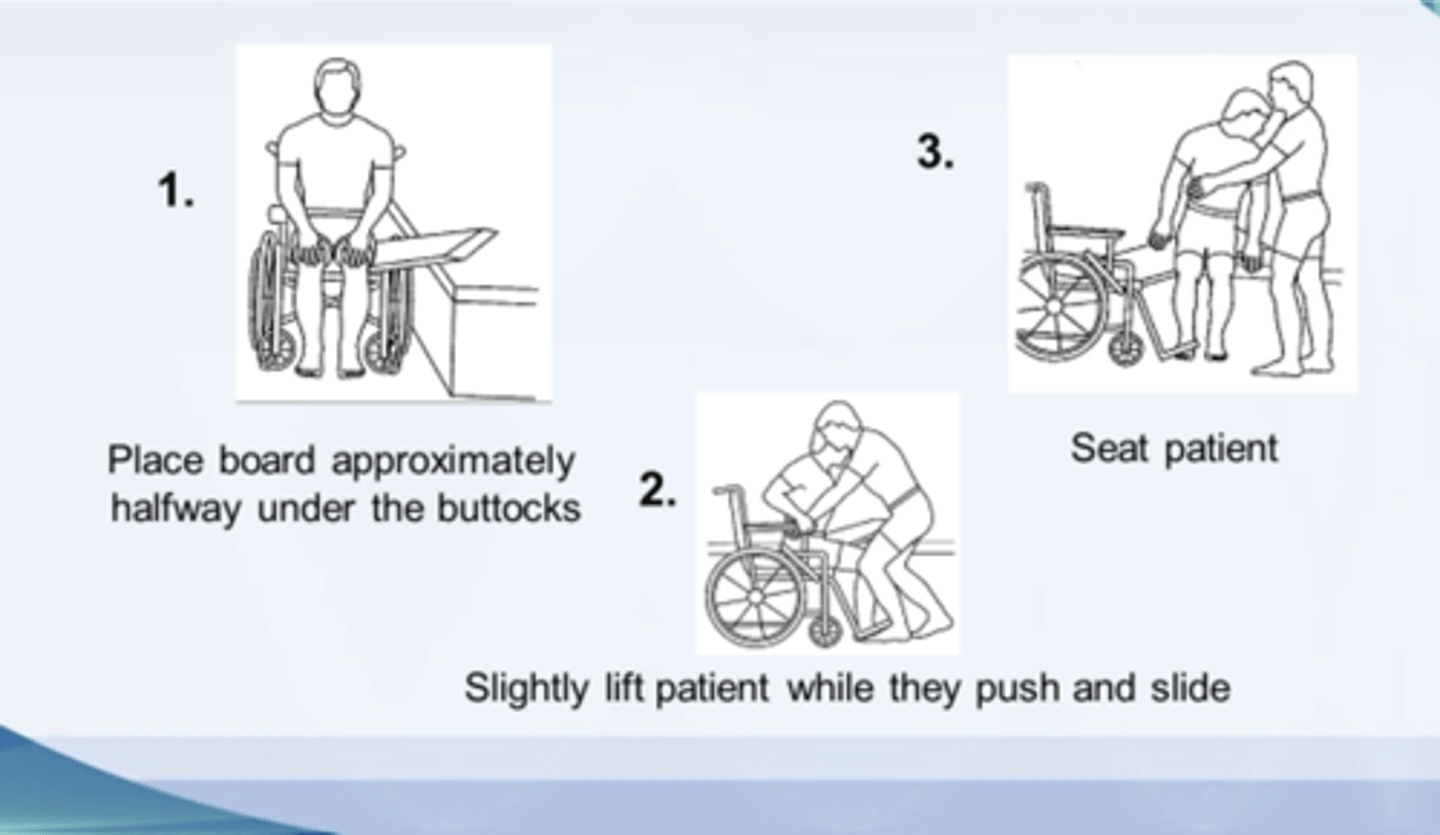
sliding board transfers
Which type of transfer is used best with those who cannot adequately bear weight on the LE and who have paralysis, weakness, or poor UE endurance (ex: LE amputations, SCIs, bariatric clients)?
car transfers
- Often most challenging transfer for therapists and clients - may involve trial-and-error method
- Extra long sliding board may be helpful
- Might be an uphill transfer
- Can practice in front and back seats to determine which car position is safest for the client
dependent transfers
- Designed for use with the client who has minimal to no functional ability
- Client must be cooperative and willing to follow instructions
- One-person dependent sliding board transfers, two-person dependent transfers (bent pivot - with or without sliding board to W/C), mechanical lift transfers
independent (I)
no help
modified independent (Mod I)
use device, no help
supervision (SPV) or stand by assist (SBA)
no physical help; just stay close for safety
minimal assist (Min A)
25% or less physical help (client does 75% or more)
moderate assist (Mod A)
26-50% physical help (client does 50-74%)
maximum assist (Max A)
51-75% physical help (client does 25-49%)
total assist (Total A) or dependent
76-100% physical help (client does 0-24%) OR requires 2 person assist
transfers with orthopedic conditions
- Bed to W/C
- W/C to toilet
- W/C to tub bench/shower