Virtual reality & therapeutic applications in autism
1/20
Earn XP
Description and Tags
Dr David Simmons
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
21 Terms
therapeutic applications of VR in autisim
phobia
social skills
(autism controversial)
anxiety
specific phobia
extreme or irrational fear of an object or situation
common in autism
30-64% of autistic children
VR for specific phobia rationale
graded exposure combined w/CBT known to effective
usually progress from imaginal exposure to real-life
but some people struggle w/imaginal exposure & real life exposure is hard to control
why use VR for specific phobia
allows simulations of RW to be created
newly learned coping skills can be rehearsed & reinforced in safe & controlled way
facilitates a more gradual exposure
a good alternative
Maskey et al (2019) - blue room
Looking into specific phobias
single blind randomised controlled trial
VR treatment vs usual care
built on previous proof of concept
outcome measures of comparision of
initial vigette
produced by blind assessor
rated by expert panel
to see how p responds
Maskey et al (2019): Methods
Careful Onboarding procedures
bringing P into enviroment
Home visit with video of procedure
Relaxation before exposure
CAVE VR (No headset)
4 m3
Therapist sits next to child to deliver CBT
Broad range of measures
Children seemed to enjoy the procedure
Low dropout rates
Maskey et al (2019): results
gradation allowed P to experience levels of mastery in managing their anxiety and to repeatedly practice
most children’s rating of their confidence at tackling their goal situation increased
an increase reflected in parent ratings
Data completeness for the main outcome measure of target behaviour rating was excellent
a success rate of 38% with definite positive change on blinded, independent rating, with a large effect size, is at least comparable with other interventions for anxiety
evaluation of Maskey et al (2019)
Innovative use of VR in a very specific context
Cost of individual adaptation
Potential bias from non-blinded parents
Unclear why works well for some but not others
Comparison vs. “treatment as usual” but not “VR vs. non-VR”
Autism
common form of ND which directly effect 1-2% of pop
characterised as having difficulties w/social interactions
recasted as differences rather than deficits
social skills training used to be seen as useful but now seen as highly controversial
tend to have bias towards local processing due to weak central coherence
Autism & social skills rationale
If role-playing social situations is thought to be a good thing, alternatives are:
Reading and imagining
Watching videos
Live role play w/actors
VR offers another alternative which is
Safe
Reproducible
Customisable
Parsons et al (2004)
36 participants
12 Autistic, 12 controls matched on Verbal IQ, 12 on Non-verbal (”Performance”) IQ
“Desktop” VR (Cheap, Accessible
Less problems of “cybersickness”
PoV display, controlled by a joystick
“Training Environment”
“Virtual Café
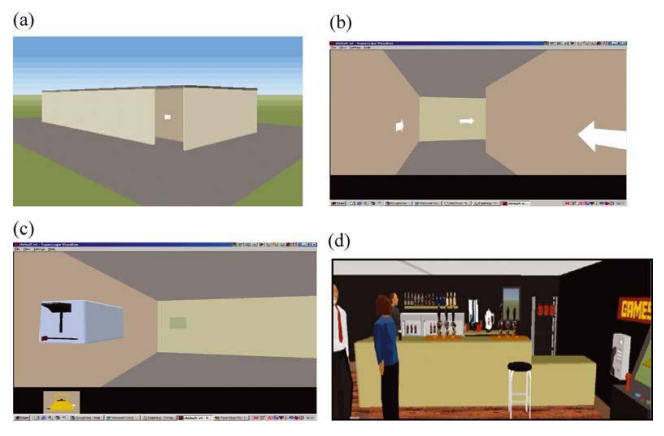
Parsons et al (2004) results
learned to use the equipment quickly
showed significant improvements in perfomance
VR technologies are potentially trasnformative for education
tendency to walk into objects/people could not be explained by executive dysfunction or a general motor difficulty → might be a sign that understanding personal space is impaired in autism
structuring of tasks within the environments provides extra support for people with weaker executive abilities
Parson et al (2004) evaluation
20 year old
outdated langauge to describe autism
outdated attitudes towards social skill training
early influential study
intresting that there wasnt a issue as it wasnt similar to the experience
anxiety
A mental state characterized by apprehension, avoidance, and cautiousness regarding potential threats, dangers and negative events
Psychobiologically distinct from fear
Response to imminent danger
Can be useful
Assisting w/uncertain threats
Mitigation/avoidance of future events
Can be maladaptive
Negative impact on mental well-being
Particular problem for autistic people (27-50%)
manipulating anxiety rationale
evidence that sensory features of autism vary w/anxitey
evidence is largely from questionnaires & self-reports
useful to manipulate anxiety in controlled, reproducible & safe environment
Millington (2023)
48 participants
Completed autism trait and anxiety questionnaires
State Anxiety manipulated using custom designed VEs
Performance in sensory task measured after each manipulation
HMD (HP Reverb Omni) with associated pupil & heart rate measures
performed at Glasgow ARC/XR lab and Engineering laboratories
Millington (2023) findings
state anxiety varied significantly between virtual environments
task did not reveal any significant effects of anxiety or autistic traits
Millington (2023) evaluation
Effects on perceptual task almost significant
Not many diagnosed autistic participants
Some technical issues
Face Makeup smudging sensors
Consistency in auditory stimuli
Pupil size varies with display brightness
Some participants found the forest environment scary!
Anxiety maybe increased with unfamiliar tech
Parson (2016) Authenticity in VR for assessment & learning
VR is a promising tool for learning & assessment, especially for individuals with autism.
Authenticity = key to ecological validity (VR behaviour reflects real life).
Designers must prioritise essential authenticity dimensions (visual, functional, contextual).
Functional fidelity often matters more than visual realism; test VR tasks against real-world performance.
authenticity (Parsons, 2016)
how closely the VR scenario maps into real-world tasks/contexts
more authentic a VR system the stronger its validity for assessment
issues of authenticity (Parsons, 2016)
more authentic --> more it costs, technical complexity & usability constraints
over-realistic can overwhelm users or reduce usabilityOver-realistic