PT 515 Midterm 1 (Examination, ROM and Joint play)
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
Philosophy of BU DPT
Empathetic Patient Centered Care
Critical Thinking/Clinical Reasoning
Evidence Informed Practice
Experts at examination and integration of human
movement
What is Empathetic Patient Centered Care
Respecting person’s experience and listening to their POV, desires and goals
NOT top-down
NO judgment
Relation w/ you + pt (it is unity in decisions and goals
Critical Thinking/Clinical Reasoning
Acting upon the missing details
knowledge + skills + character
being curious
Experts in Examining Movement
Evidence Informed Practice
Engage with/interpret/implement research to advance the profession
integrating the best research + clinical experience + pt opinions & expectations
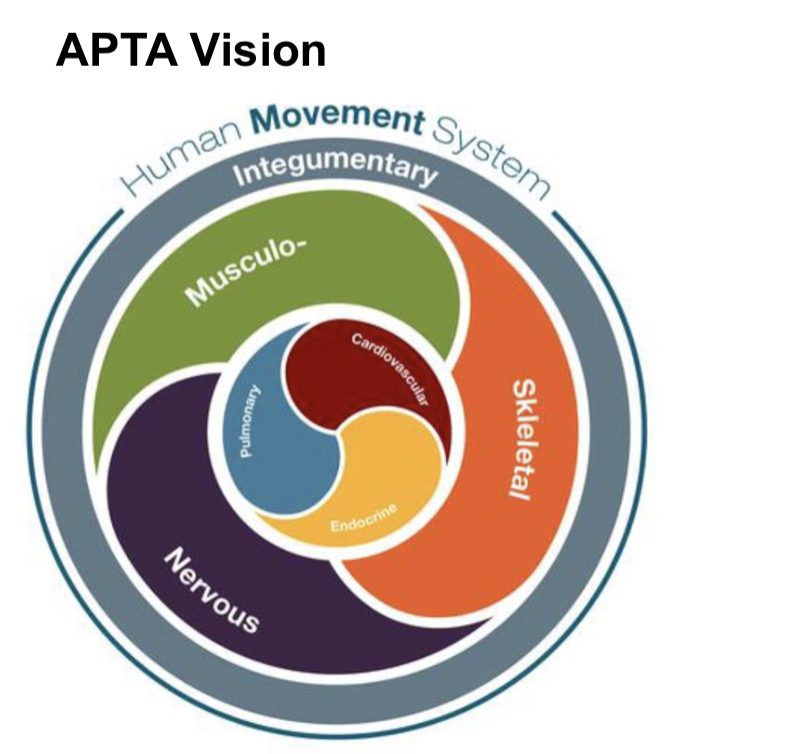
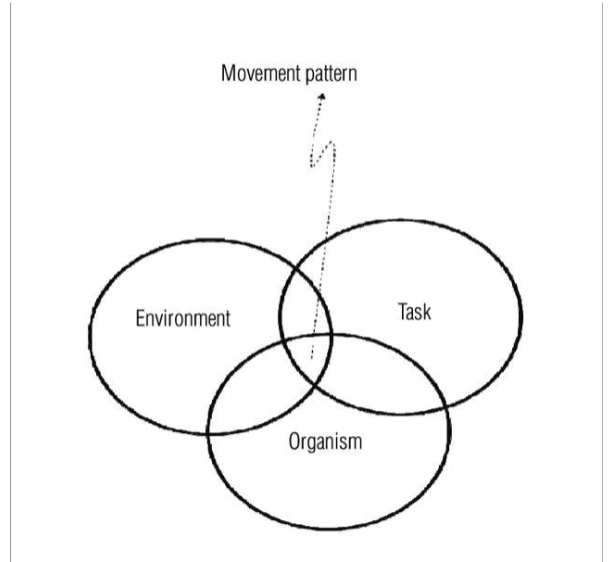
Human Movement System
Movement to guides our clinical reasoning
▪ Task: what is the goal of the movement (stand up)
▪ Environment: conditions of the task
▪ Organism: the human condition
Movement Assessment
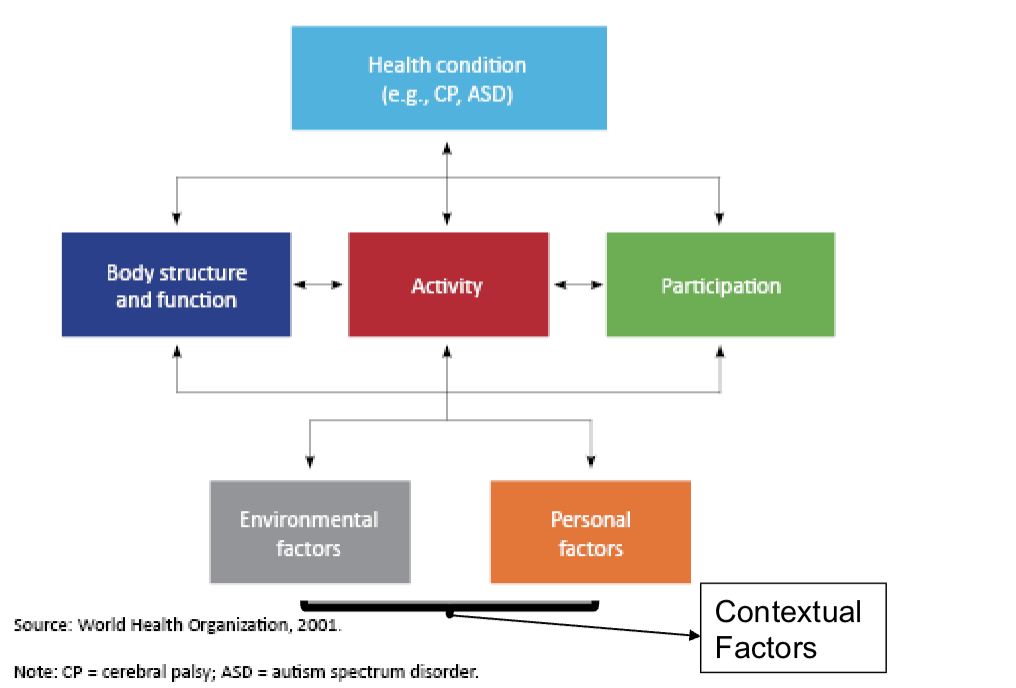
International Classification of Functioning, Disability and Health (ICF)
Body structure + fxns:
physiological + psych functions of body systems
Impairments:
problems in body fxn or structure that creates major deviation or loss
Activity limitations:
difficulties of an individual in execution of a task or action by an individual
(Restriction in Activities of Daily Living)
Participation restrictions:
problems an individual experience in involvement in life situation
Environmental factors:
phys, social, and attitudinal environment in which people live and conduct their lives
Step 1 of PT exam
Patient Interview
Gather information about current condition
Identify patient's beliefs and expectations about current health condition
Identify patient's goals for physical therapy
Establish therapeutic relationship with patient
This is where we initiate our collaboration

Basic Structure of PT exam
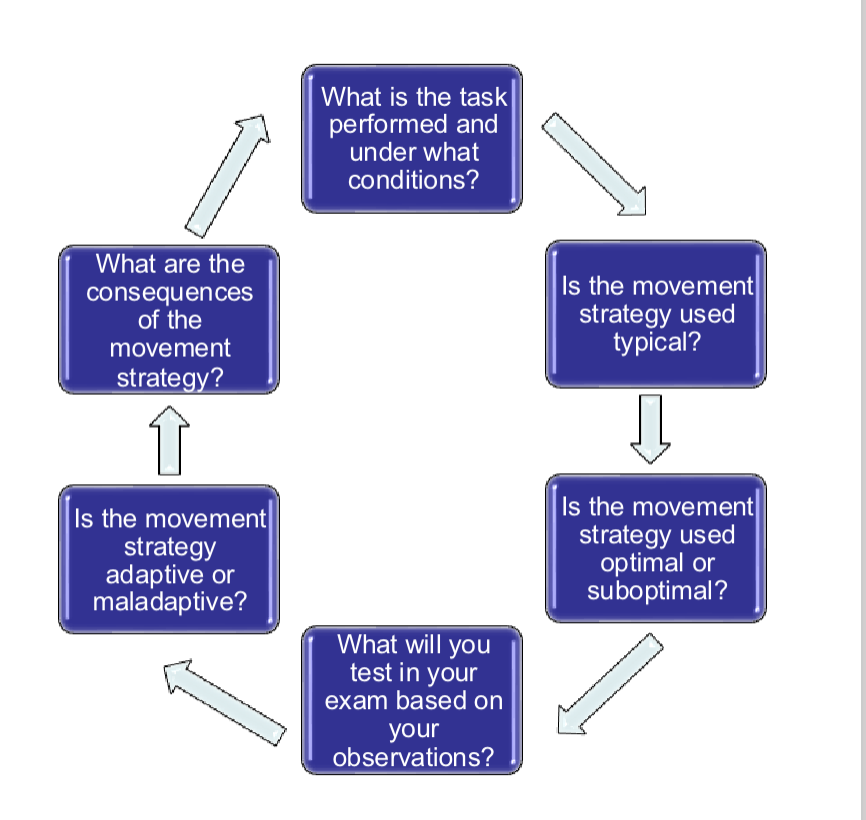
Step 2 of PT Therapy Exam: Movement Assessment
Observation of mobility or patient engagement in environment/tasks:
(MOVEMENT ASSESSMENT)Appraise movement quality and compare to expectations or
knowledge of functional anatomy (Critical Thinking/Clinical
Reasoning)
2 ways of assessing Joint mobility
ROM
physiological joint (ostekinematic) motion
examined when NO visible sufficient movement in function and suspect limited mobility
Joint play
accessory movement (arthrokinematic) motion
examined when there is abnormal ROM (too little or too much)
Range of Motion
measure of bone motion/rotation (osteokinematics) in cardinal plane
parallel to plane around axis
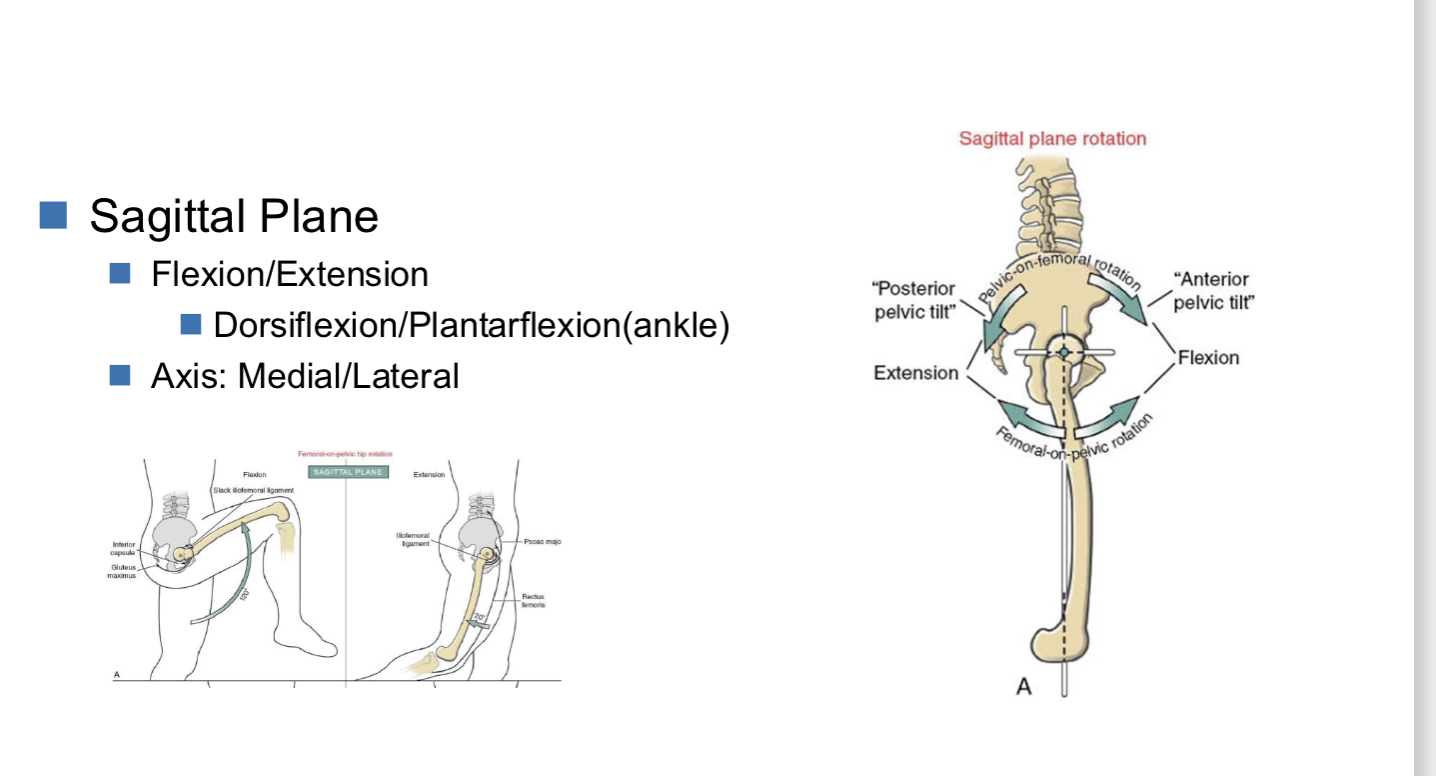
Sagittal plane
Sagittal plane of ROM
Flexion/Extension
dorsiflexion/plantarflexion (ankle)
Axis: Medial/lateral aka horizontal
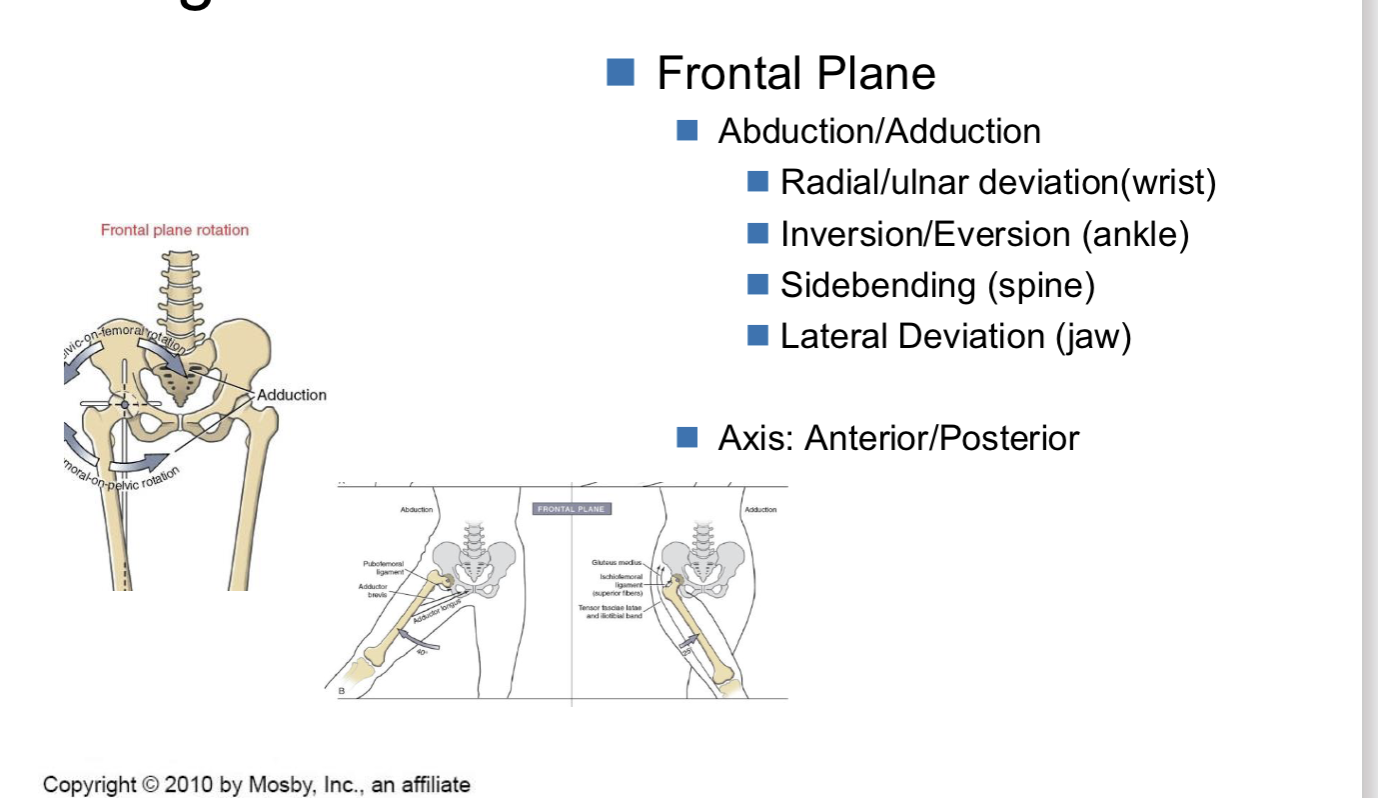
Frontal plane of ROM
Abduction/Adduction
Radial/ulnar deviation(wrist)
Inversion/Eversion (ankle)
Sidebending (spine)
Lateral Deviation (jaw)
Axis: Anterior/Posterior aka Anteroposterior
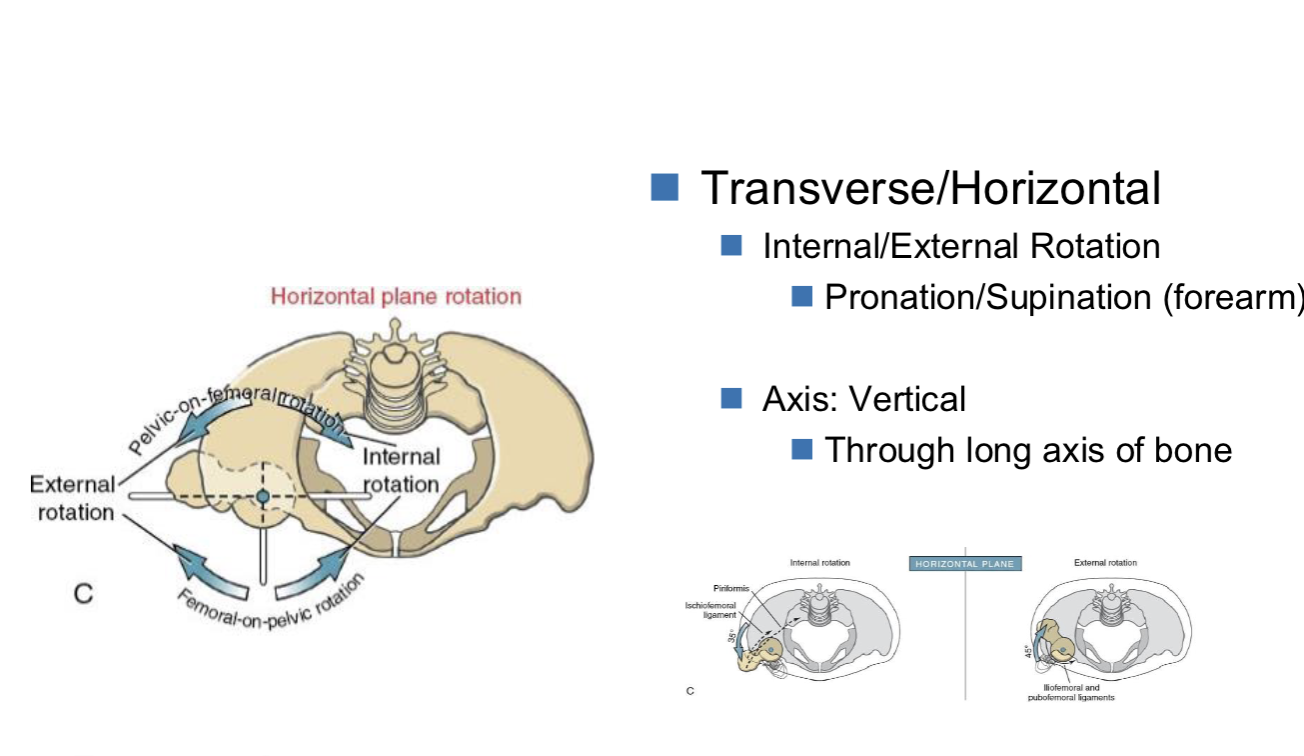
Transverse/Horizontal plane of ROM
Internal/External Rotation
Pronation/Supination (forearm)
Axis: Vertical
Through long axis of bone
Types of ROM
Passive (PROM aka ROM): measures total amount of available motion at the joint
Physical therapist does movement
Standard measurement of joint mobility
Active (AROM): measures how willing the individual is to move, some degree of strength
neurological integration + individual
NOT info on joint capacity, but tells us if pt can move
Indications (GO) and Contraindications/Precautions of examination ROM
Indications (GO)
when joint mobility may contribute to individual’s activity or participation restriction
for determining health well being of joint
before measuring strength of muscle
Contraindications/Precautions (STOP)
passive movement of joint will cause injury
if limited by health condition (ex. Surgery, fracture)
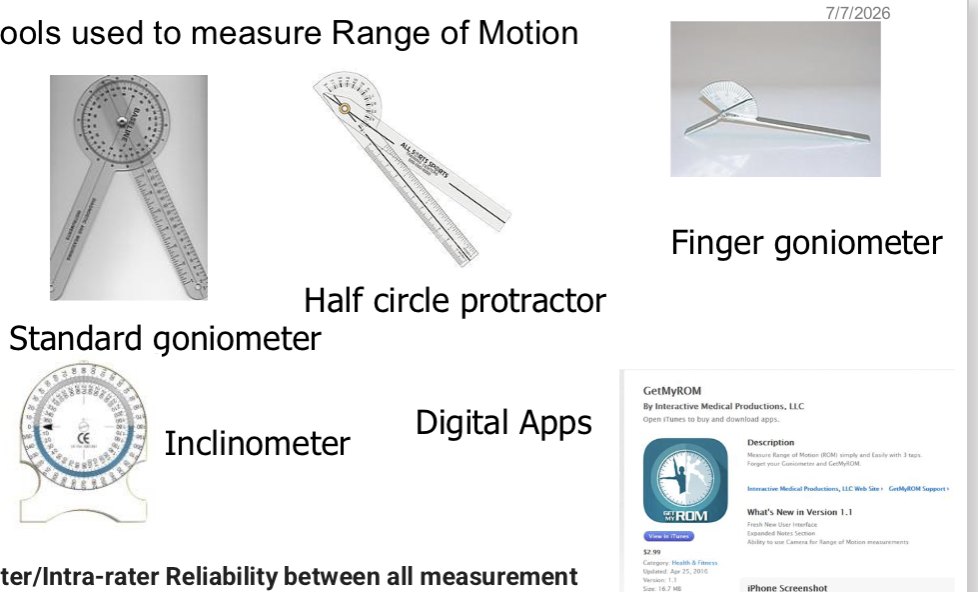
Tools to measure ROM
goniometer
inclinometer (incline amt - used for spine + limb displacement)
Accelerator
***they have Inter/Intra-rater reliability***
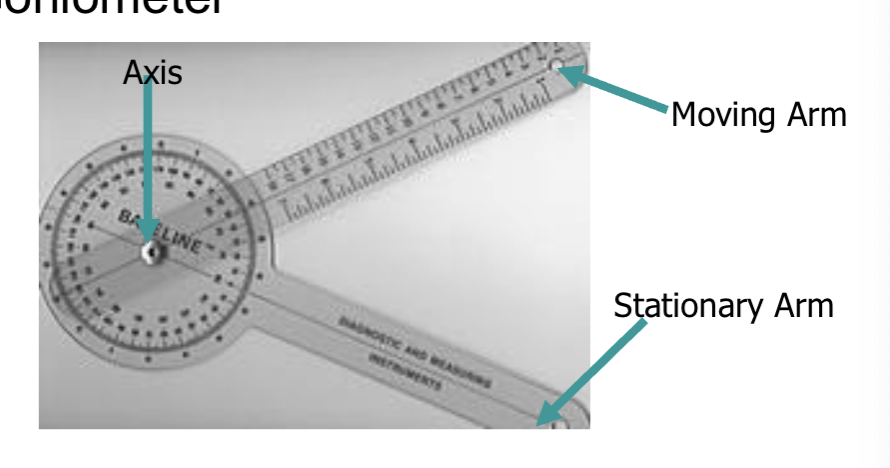
Goniometer
moving arm - is for mobile segment
stationary - non mobile segment
axis - joint bony part
Standardization of Practice
Standard Testing Position
Maintain Moving Limb in the cardinal plane
Stabilization of proximal segment
Size and Type of Goniometer
Boney Landmarks
Record Results:
Include both a quantitative and qualitative component
ROM - Quantitative
Measurement in degrees
2 numbers always: Start and End position
Normal ROM always starts at 0
Reliability
+/- 5⁰ Standard Error of Measurement (SEM)
Validity
Range of Motion-Qualitative (NORMAL/TYPICAL)
Hard
Think Bone…elbow extension
Soft
Think soft tissue (adipose, muscle approx)…elbow/knee flexion, hip flexion
Firm
Think Capsule….try MCP joint extension
also ligament, muscle length, tendon
Range of Motion-Qualitative (ABNORMAL/ATYPICAL)
Empty (NOT safe)
NOT getting to end feel,
dislocation of joint or pt not wanting to go further
Boggy(“squishy”)
inflammed joint
Crepitant
crack feel
Springy
muscle guarding or ligament abnormality
also ***any one of the normal end feels that is not supposed to be felt at that joint***
ROM - Standard Procedure
Explain the test to the patient-using non-threatening language
Position the patient in the starting position(Standard Test)
Stabilize the proximal joint segment
Passively move the joint through the ROM and determine the end-feel
Eyeball the degrees of motion-vocalize your estimate
Return the limb to the starting position
Palpate the bony landmarks, align the goniometer and record starting position
Move the limb passively through the ROM
Re-palpate and align the goniometer
Read the value on the limb and record the reading
Examination of Joint play
motions of bones relative to other bones aka joint surfaces (Arthrokinematics)
it is passive
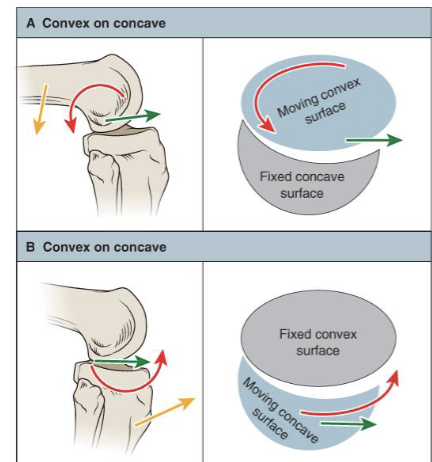
Arthrokinematics
Requires forces either passive (external) or muscle (internal)
Constrained by anatomy and joint structure
Axis of rotation of any joint partner is always within the center of the convex bone surface
Arthrokinematics (Treatment plane)
Treatment plane
is parallel to the deepest part of concavity
is perpendicular to the line running from the axis of rotation in the convex joint partner
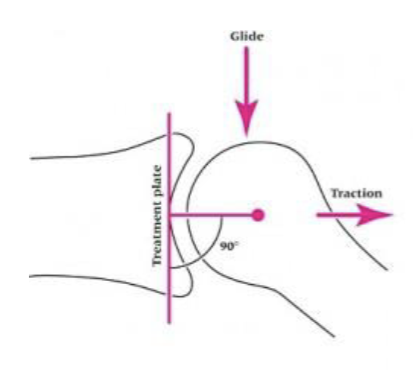
Glide in athrokinematics
is always parallel to treatment plane
Arthrokinematics (Traction)
applied perpendicular and away from treatment plane
entire bone is moved for joint surfaces to be separated

When do we assess joint play
when there is abnormal ROM
it’ll assess capsular mobility, sensitivity to shear, load, and distraction
Indications (GO) and Contraindications (STOP) for Joint play assessment
Indications (GO):
Make inference about joint function
Determine the type of resistance between joint surfaces
Determine any tissue injury or inflammatory process
Determine level of patients pain/ tolerance to movement (doing movements to see if it provides relief or pain)
Contraindications (STOP):
Fear on the part of the patient or therapist
Red Flags including signs of neoplasm, fracture, or systemic disturbance (that prevents passive movement)
Rheumatoid collagen disease (if untreated)
There are more… you will learn as we get more into pathologies
What do we assess for in Joint play
Available mobility of the capsule and supporting
ligaments(glides, traction)Pain provocation
Pain Alleviation
muscle tension
Loose packed position v Closed packed position
Loose pack (RESTING):
point in joint’s range where capsule + ligaments have least restraint to passive sliding
least bony congruency + most lax
Closed pack:
where the ligaments and capsule are maximally taut.
usually (but not always) at the end of a joint’s ROM
greatest joint stability, and most resistant to distraction forces that cause separation of the joint surfaces
little or no joint play is possible
Joint Play Standard procedure
Explain the test to the patient
Position the patient comfortably to minimize muscle tension
Stabilize the proximal joint segment with your stabilizing hand
Grip the moving segment as close to the joint line as possible
Position the patient in the resting position (loose pack) for the joint
Perform the joint play assessment by moving the moving segment either parallel or perpendicular to the treatment plane and determine the end-feel
Compare to the opposite side and determine normal, hypomobility, or hypermobility
compare to other limb
compare to historical normal if person has NO other limb
Joint play measurement
Qualitative:
Normal-Motion: feels the same as the other side
Hypomobile: Motion is limited compared to other side
Hypermobile: Motion is excessive compared to the other side
Joint Play-Measurement (Descriptor)
Normal End/Feel
firm
Abnormal End/Feel —> pain
soft, hard, empty, baggy (squishy), crepitant, springy
Loose pack position, Treatment Plan for Tibiofemoral joint
Loose Pack Position: 30 dg flexion
Treatment Plane: Concave surface of the tibia.
Loose pack position, Treatment Plan for Patellofemoral joint play
Loose Pack Position: 0° of tibiofemoral flexion / extension.
Treatment Plane: Underside of the patella.
Normative values for Tibiofemoral ROM (ext + flex)
Flexion: 0-135 dgs
Extension: 0-10 dgs
Normal end feels for Tibiofemoral ROM (ext + flex)
Flexion: Soft/ Firm
Extension: Firm
Normal end feels for Femoroacetabular joint ROM (ext + flex + IR + ER + ABD + ADD)
Flexion: Soft / Firm
Extension: Firm
Internal Rotation: Firm
External Rotation: Firm
Abduction: Firm
Adduction: Soft / Firm
Normative values for Femoroacetabular Joint ROM (ext + flex + IR + ER + ABD + ADD)
Flexion: 0-120 dg
Extension: 0-30 dg
Internal Rotation: 0-45 dg
External Rotation: 0-45 dg
Abduction: 0-45 dg
Adduction: 0-30 dg
loose pack and closed pack positions for femoroacetabular
loose pack:
30 dg flexion, slight ER, 30 dg abduction
closed pack:
full extension, slight IR, slight abduction
loose pack and closed pack positions for humeroulnar joint
loose pack: 70 dg flexion, 10 dg supination
closed pack: full extension, full supination
loose pack and closed pack positions for metacarpophalangeal joint
loose pack: slight flexion
closed pack: full extension