Lecture 17 & 18 Noncompartmental analysis and Nonlinear (Dose Dependent) PK
1/38
Earn XP
Description and Tags
1. Compare and contrast compartmental vs. noncompartmental analyses and understand the bene=ts of using noncompartmental analysis. 2. Understand de=ni>ons of pharmacokine>c parameters from noncompartmental analysis: AUC[Area Under the Curve, conc./mL x t], AUMC[Area Under the Moment Curve, conc./mLx t x t], MRT[Mean Residence Time, min. or hr], CL[Clearance, mL/min.], and Vdss [ Volume of distribu>on @ steady state, mL or L]. 3. Learn how to es>mate the following parameters: AUC, AUMC, MRT, CL, and Vdss 4. Understand various proper>es (usefulness) of AUC in linear kine>cs: Major phase concept and superposition principle. Describe linear and nonlinear pharmacokinetics and their differences • When presented with the mechanism of a nonlinear drug, be able to describe the kinetics parameter affected • Recommend appropriate phenytoin dosing or adjust phenytoin dosing regimen based on information provided (including the graphing methods)
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
39 Terms
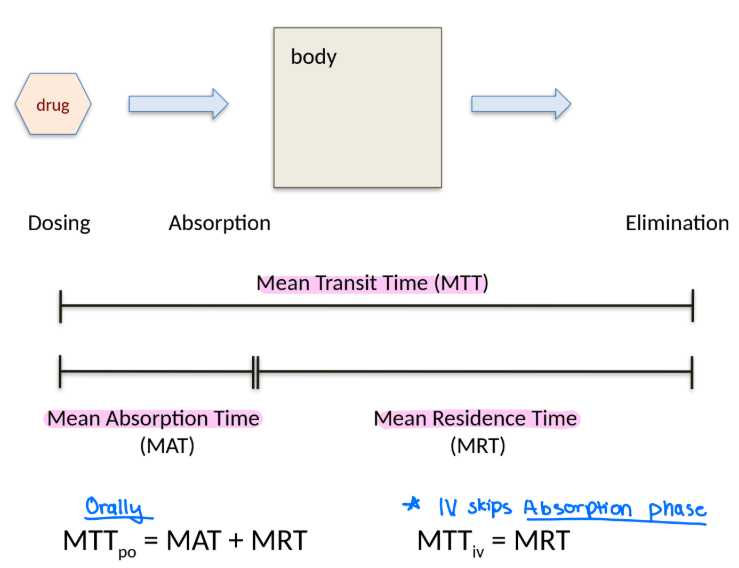
What is Mean Transit Time/Mean Residence Time (MTT)?
It is the average time one drug molecule spends in the body from dosing to elimination.

How do you calculate Mean Transit Time (MTT)?
MTT = AUMC/AUC
AUMC = area under the moment curve
calculated by t * C
AUC = area under the curve
trapezoidal rule
How do you calculate MTTpo?
a. Mean Absorption Time (MAT) + Mean Residence Time (MRT)
b. Mean Residence Time (MRT)
a. Mean Absorption Time (MAT) + Mean Residence Time (MRT)
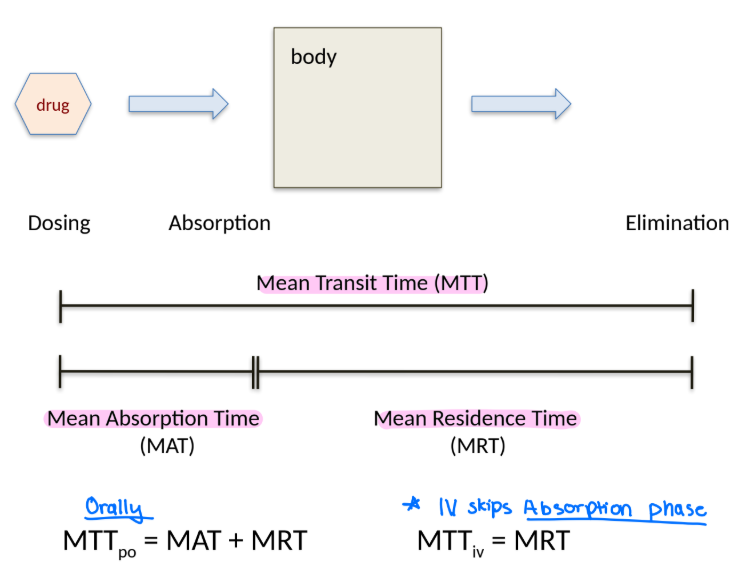
How do you calculate MTTiv?
a. Mean Absorption Time (MAT) + Mean Residence Time (MRT)
b. Mean Residence Time (MRT)
b. Mean Residence Time (MRT)
absorption does not take place during IV
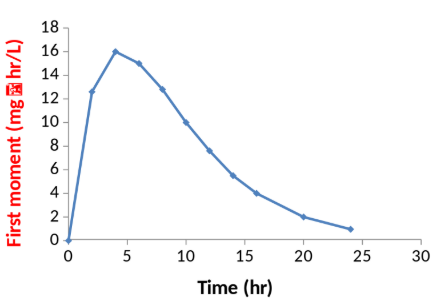
Identify the curve.
a. Linear curve (AUC)
b. First moment curve (AUMC)
b. First moment curve (AUMC)
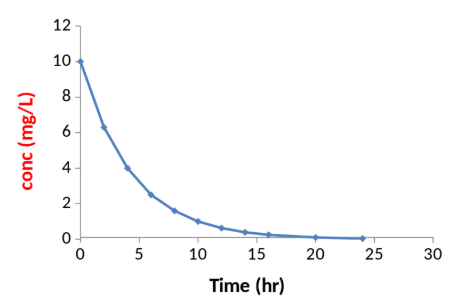
Identify the curve.
a. Linear curve (AUC)
b. First moment curve (AUMC)
a. Linear curve (AUC)
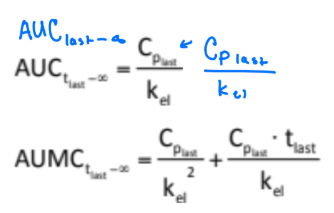
What is used to estimate AUClast-inf and AUMClast-inf?

kel is used (terminal phase elimination rate constant)
True or false: AUC, AUMC, MRT, and CL can be estimated regardless of peak shapes.
True!
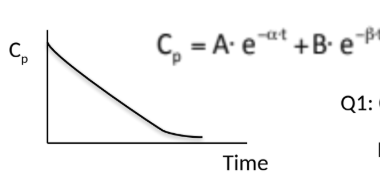
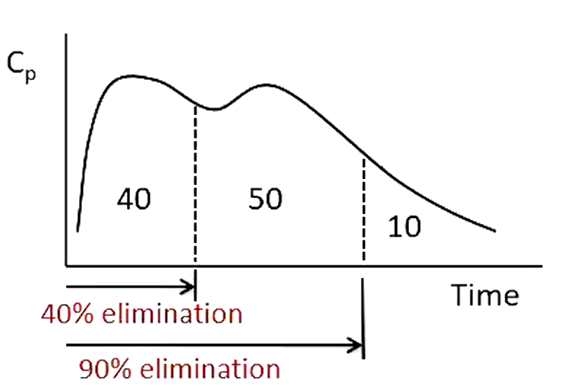
What is the “Major Phase Concept” in pharmacokinetics?
The idea that the phase of the concentration–time curve contributing the most to total AUC is the “major phase,” usually the elimination phase.
When can a multi-compartment PK model be approximated as a one-compartment model?
When the elimination phase contributes the majority of the AUC, and the distribution phase is short and contributes little to total exposure.
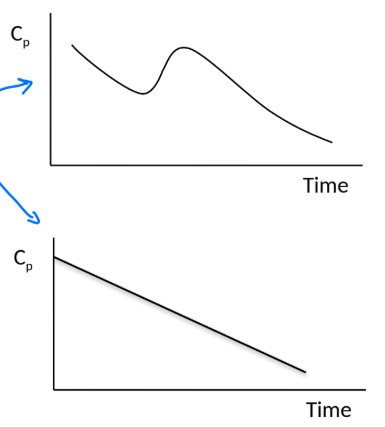
Can you explain the little bump in this curve?
It is called dose dumping —> when you dump a dose too fast after initially dumping a previous dose. This occurs often with fatty tissue or when drug is controlled release.
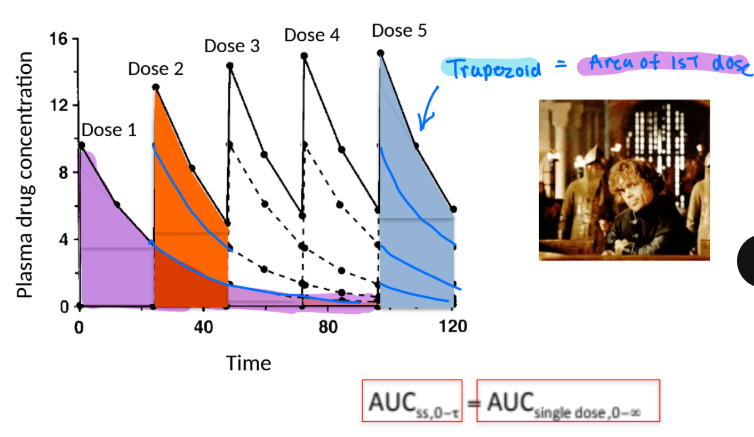
What does the superposition principle mean?
It states that the concentration–time profile after multiple doses is the sum of the profiles from each individual dose, assuming linear kinetics.
(At steady state, AUCₛₛ over one dosing interval = AUC after a single dose.)
In a 1 compartment model, is it possible to estimate the MRT and MAT?
Yes, MRT = 1/kel while MAT = 1/ka
After IV administration, Drug A and Drug B show MRT values of 1 and 5 hr, respectively. Which drug is eliminated faster?
a. Drug A
b. Drug B
c. Not enough info is given
a. Drug A
What is Vdss?
It is the steady-state volume of distribution of a drug.
Vdss = MRT x CL = amnt of drug in body at ss/steady state Cp
Does the volume of distribition observed before or after the drug has distributed into the tissues?
After
True or False:
MTT, AUMC, AUC, Cl, and Vdss are compartmental PK parameters
False. They are noncompartmental
Which of the following are benefits for noncompartmental analysis?
a. better accounts for biological processes
b. no assumptions about distribution into the body (holistic) which minimizes bias
c. poor relating to specific organ function
d. provides better insight into “Fate of drug”
b. no assumptions about distribution into the body (holistic) which minimizes bias
c. poor relating to specific organ function
Which of the following are benefits for compartmental analysis?
a. capability to predict concentrations for certain time point
b. no assumptions about distribution into the body (holistic) which minimizes bias
c. poor relating to specific organ function
d. provides better insight into “Fate of drug”
a. capability to predict concentrations for certain time point
d. provides better insight into “Fate of drug”
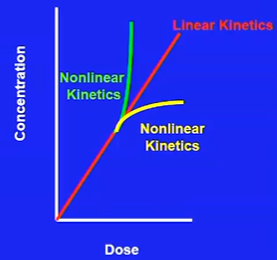
Which of the following are characteristics of linear (first-order) PK?
a. F, fu, V, CL are constant and does not change with changing dose.
b. Dose and concentration are not directly proportional
c. PK is predictable after different and repeated doses
d. considered “dose-dependent”
e. One of them: F, fu, V, Cl, changes with changing dose
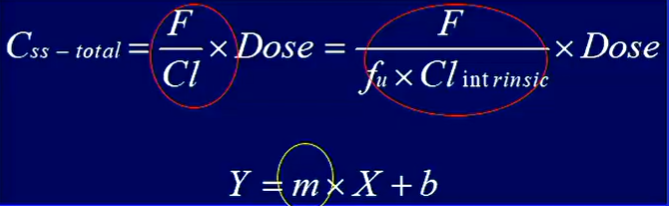
a. F, fu, V, CL are constant and does not change with changing dose. These variables are the slope.
c. PK is predictable after different and repeated doses
Which of the following are characteristics of non-linear PK?
a. F, fu, V, CL are constant and does not change with changing dose.
b. Dose and concentration are not directly proportional
c. PK is predictable after different and repeated doses
d. considered “dose-dependent”
e. One of them: F, fu, V, Cl, changes with changing dose
b. Dose and concentration are not directly proportional
d. considered “dose-dependent”
e. One of them: F, fu, V, Cl, changes with changing dose
True or False: Phenytoin is a dose-dependent (non linear) drug, part of the reason why is due to its decreasing oral absorption when the dose is increased.
True! greater dose = lower F, higher Cmax, higher Tmax
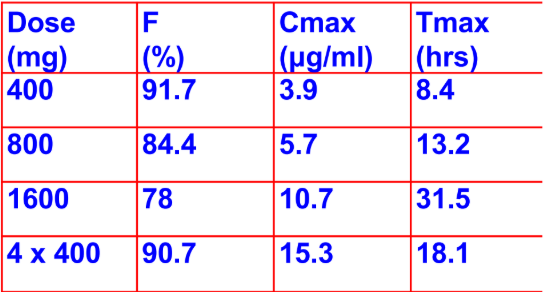
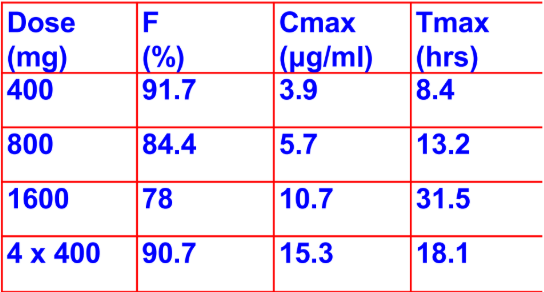
Based on this graph of the different Phenytoin doses, what do you think is the most suitable dose?
a. 400 mg
b. 800 mg
c. 1600 mg
d. 4 × 400 mg
a. 400 mg
going past 400 mg decreases rate and extent of oral absorption
True or False: Phenytoin can be administered in other ways other than in loading dose situations.
False. Phenytoin is administered in loading dose situations only (IV, IM, PO: 300-400mg increments 2-4 hrs apart)increments
Name the factors of the equation shown as a guideline for administering Phenytoin Loading Doses:

What should be noted when calculating for oral administration?
V = volume of distribution
Cinitial = initial conc.
Cdesired = desired conc.
F = bioavailiability
S = salt formulation of Phenytoin
Note: for oral administration, divide the dose into 300 to 400 mg increments and give 2-4 hrs apart
True or False: Gabapentin is another dose-dependent drug that has a decrease in oral absorption with an increasing dose.
True!
Bioavailability is 60% at 400 mg to 30% at 1600 mg
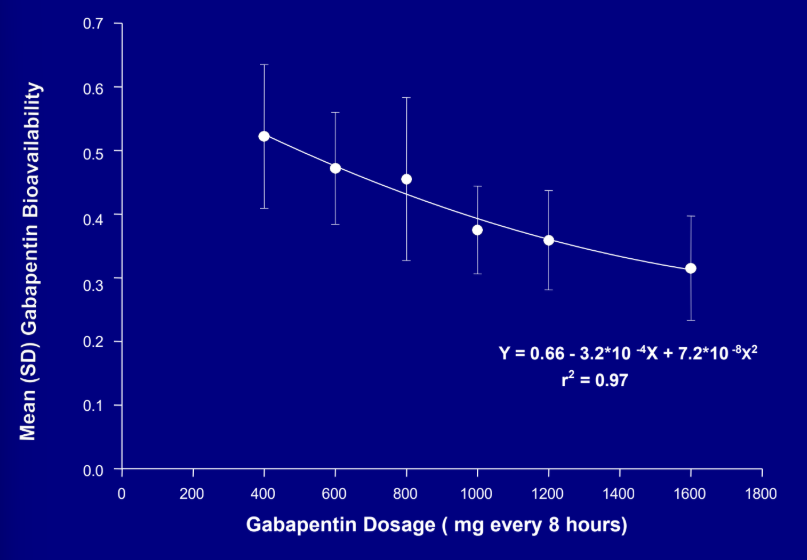
True or False: There is a therapeutic benefit at doses above 3600 to 4800 mg/d for Gapapentin.
False: clinically, there is unlikely any therapeutic benefit and usually dose is increased until seizures are controlled or reach to max 4800mg/d
What is interesting about Carbamazepine?
It induces its own metabolism —> signals the liver to metabolize after a single dose and continues after 3-4 weeks of therapy —> stops inducing metabolism after a month.
46 y/o female admitted to the hospital with
uncontrolled seizures. There is a
discussion about starting her on
Carbamazepine to control her seizures.
Do you agree?
No, because Carbamazepine’s pharmacokinetics change over the first month.
You cannot assume that a dose that works in week 1 will still be therapeutic in week 4.
You cannot quickly determine or maintain a therapeutic concentration (must wait after 4 weeks, send patient to lab to see their levels to determine a change of dosing to therapeutic level)
Why is Phenytoin also a problem in hepatic metabolism?
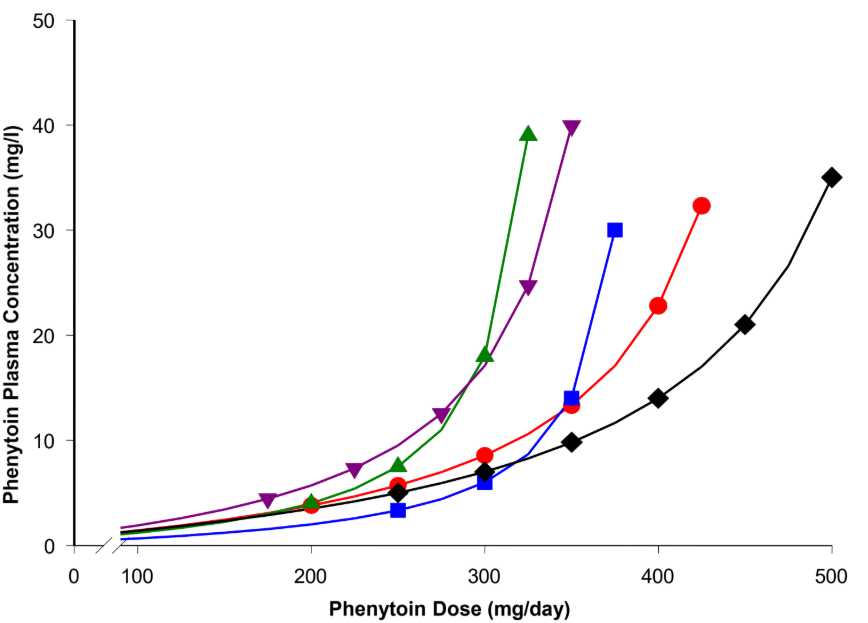
Increasing the dose of phenytoin —> CYP2C9 enzyme cannot metabolize the extra drug because it is already working at full capacity.
The graph shows 5 different patients with different Cp (challenging to manage Phenytoin)
With an increased dose of Phenytoin, CLintrinsic ____ and half-life ____.
decreases, increases
What is Km?
Affinity of the drug to the metabolizing enzyme
What occurs when Phenytoin interacts with Enzyme inducers?
a. increase in Km
b. decrease in Km
c. increase in Vmax
d. decrease in Vmax
c. increase in Vmax
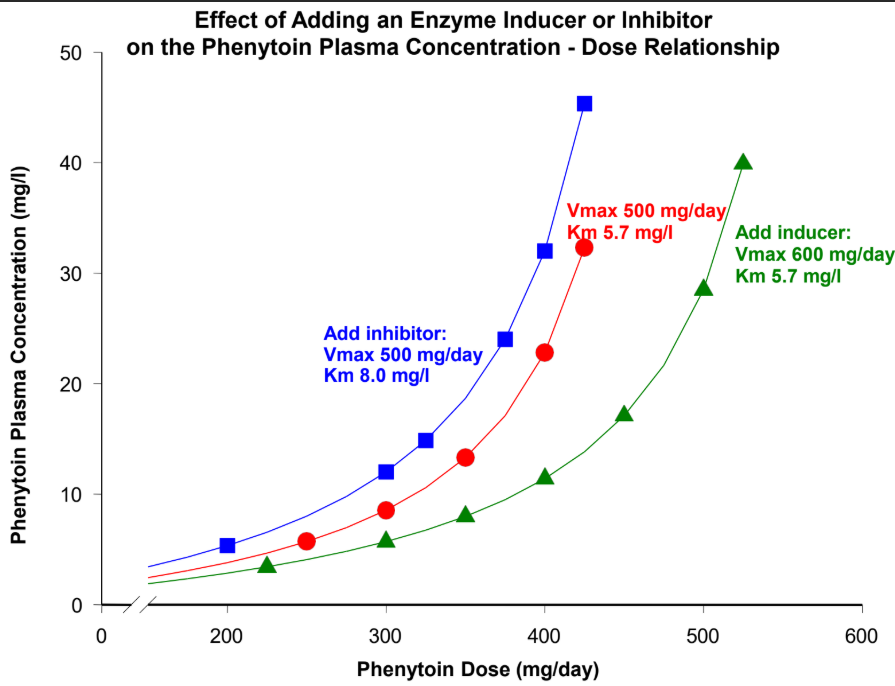
needs less drug to reach regular Phenytoin concentration
What occurs when Phenytoin interacts with Enzyme inhibitors (inhibits metabolism)?
a. increase in Km
b. decrease in Km
c. increase in Vmax
d. decrease in Vmax
a. increase in Km
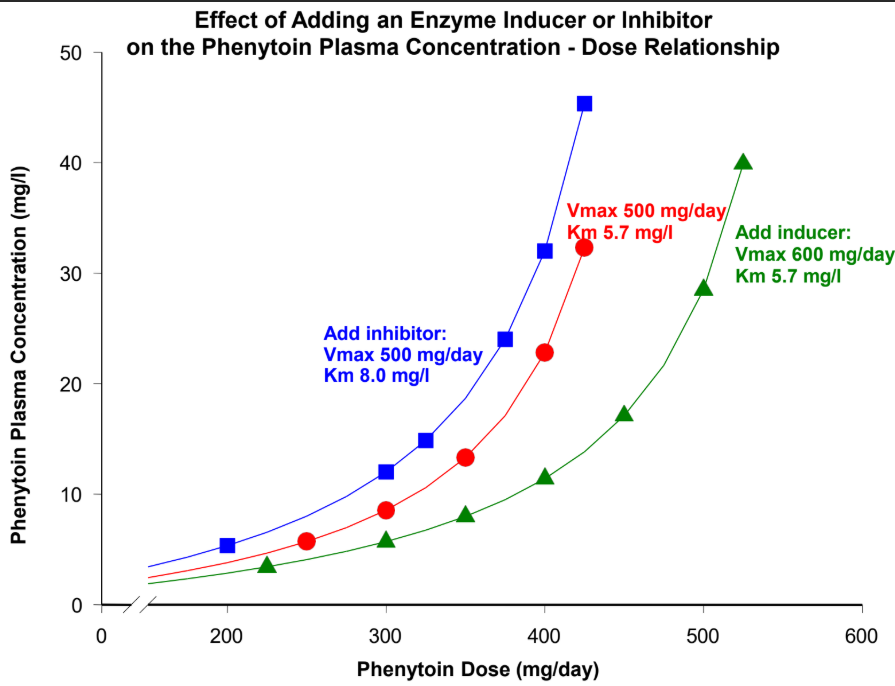
need less drug to get to regular Phenytoin concentration
If an older person takes Phenytoin, what will happen to their Vmax and Km in comparison to a younger child taking the medication?
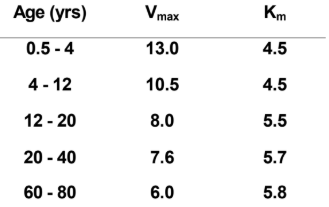
The Vmax of an older person decreases since metabolism slows down as you age, the affinity (Km) increases just a bit.
When is the Empiric Dosing Method used?
It is used when 1 Css is present. You use the average Vmax and Km from the general population.
Vmax: 7.6 mg/kg/day (2-13 mg/kg/day)
Km: 5.7 ug/ml (1-15 ug/ml)
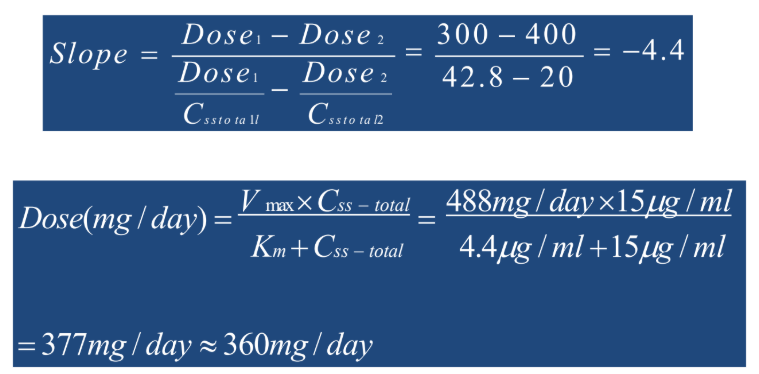
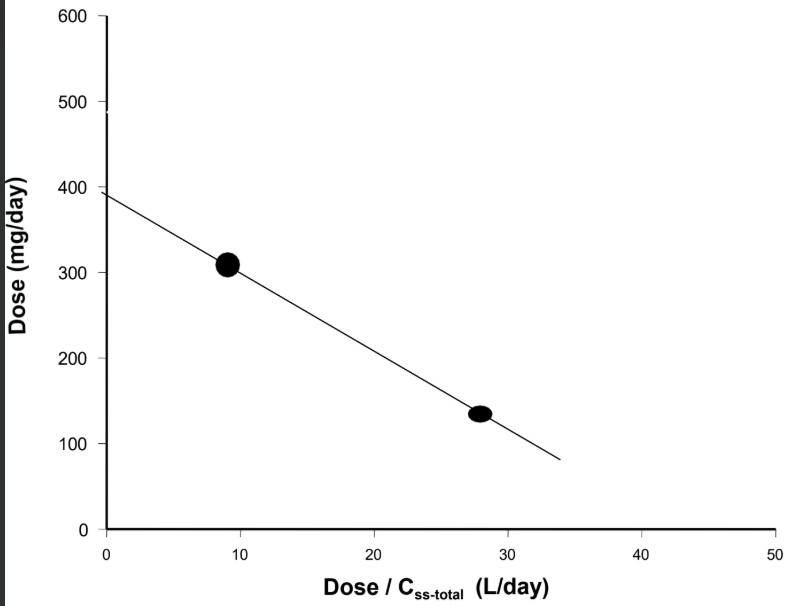
When is the Linear Graphing (Ludden) Method used?
It is used when there is more than 1 Css that needs dose adjustment. Calculate the patient’s own Vmax and Km (doesn’t need to use population reference).
Graph is linear: Dose vs Dose/Css-total
CD is a 43 y/o male with h/o seizures.
He is currently taking phenytoin sodium
capsules 300 mg/day. He is seen today
in neurology clinic and his seizures are
not controlled experiencing 2-3 seizures
per month. He states he has been
compliant. What would you recommend
to be done at this point in order to
evaluate his current management?
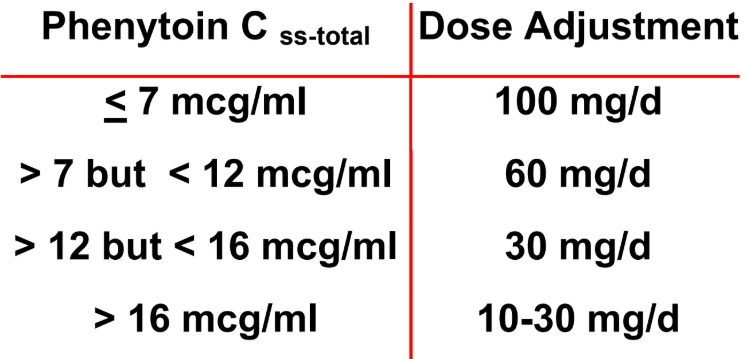
CD has a steady state phenytoin plasma
concentration of 7 mcg/ml.
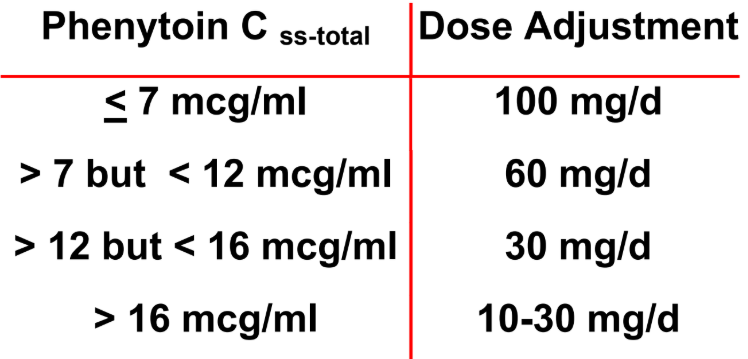
Adjust the dose by 100mg/d
So his new dose: 300 + 100 = 400 mg/d
When re-evaluated 2 months after the dose
increase, CD’s seizure control was markedly
improved but he now has signs and
symptoms of phenytoin toxicity. The steady-
state phenytoin plasma concentration on the
dose of 400 mg/day is 20 mcg/ml.
Recommend a phenytoin dose for CD to
achieve a steady-state phenytoin plasma
concentration of 15 mcg/ml.
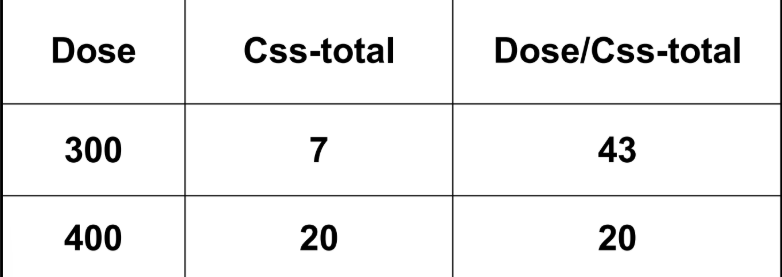
There are 2 Css values now (7mcg/ml) and (15 mcg/ml)
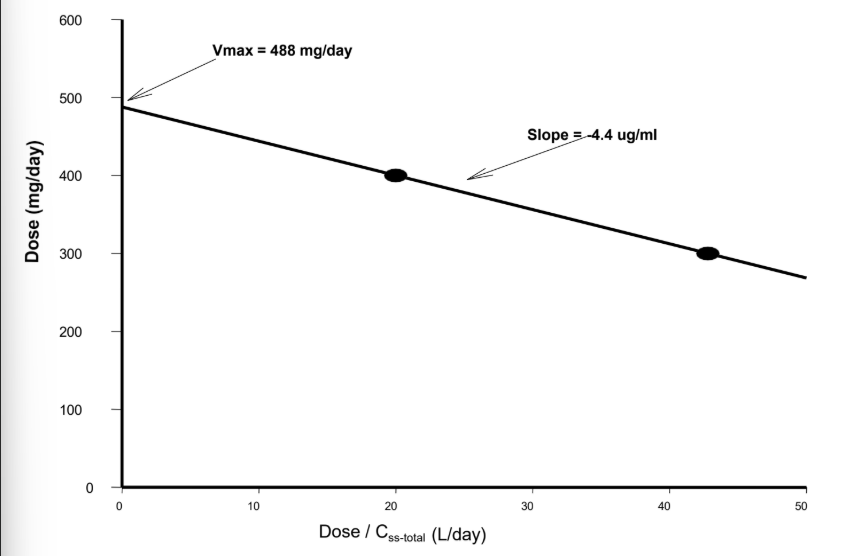
Km= Slope
(Dose1 - Dose2) / (Dose1/Css — Dose2/Css)
Vmax = y intercept