week 37 - non acute abdominal and urological problems in children
0.0(0)
Studied by 2 peopleCard Sorting
1/22
There's no tags or description
Looks like no tags are added yet.
Last updated 4:05 PM on 7/8/26
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
1
New cards
embryology
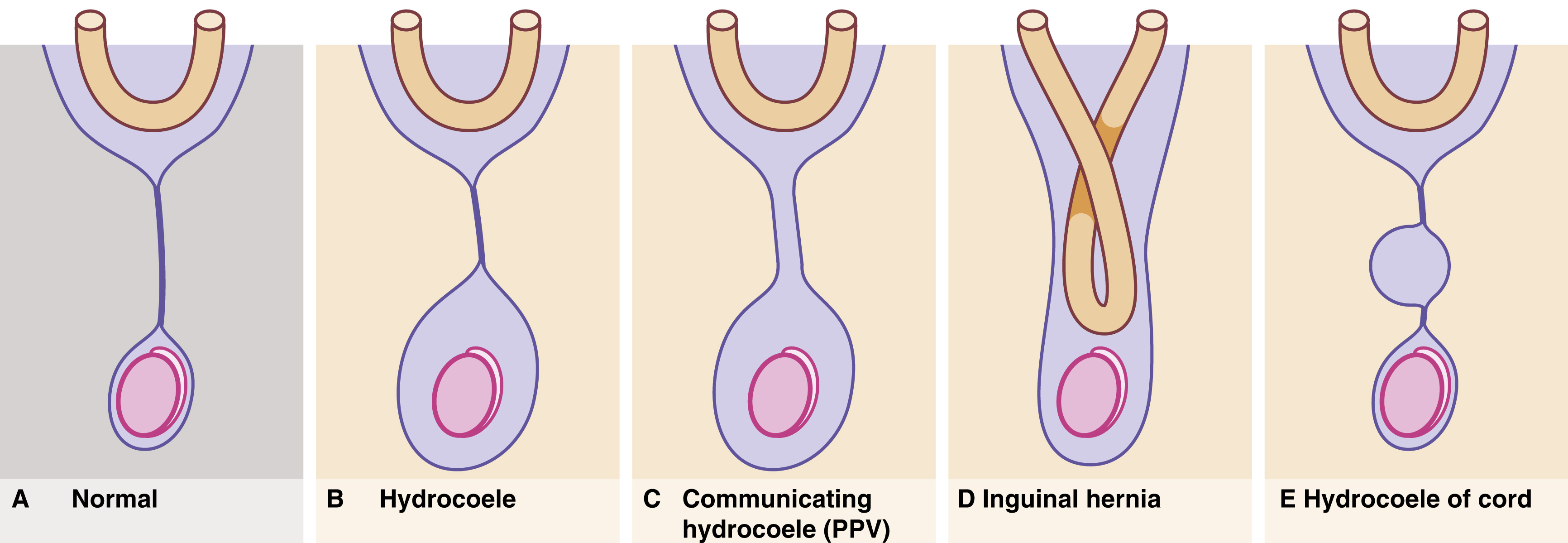
The indifferent gonad (i.e., ovary or testis) begins to develop at the fifth week in the gonadal ridge , part of the mesodermal urogenital ridge that will also form the kidney, ureter and genital ducts, in the male, or uterus and uterine tubes, in the female. At the lower pole of the developing testis, a strand of mesenchyme becomes the cord-like gubernaculum . In the eighth week, a prolongation of peritoneum, the processus vaginalis , appears beside the gubernaculum (or round ligament), and extends into the labioscrotal fold. The testis then migrates distally along the peritoneal canal
2
New cards
Patent processus vaginalis
They say that this term should only be reserved fro hydrogels communicating with the peritoneal cavity via a remnant too narrow to admit bowel but…
ISNT PPV also in hernias and stuff? Like isnt that the predisposition?
\
Anyways
\
Children with communicating hydrofiele present with sporthal swelling that increases during the day since peritoneal fluid accumulates and subsides at night
Seen up to the age of 3 y/o
Before the age of 2 they mostly go away spontaneously, otherwise → excision of the remnant
ISNT PPV also in hernias and stuff? Like isnt that the predisposition?
\
Anyways
\
Children with communicating hydrofiele present with sporthal swelling that increases during the day since peritoneal fluid accumulates and subsides at night
Seen up to the age of 3 y/o
Before the age of 2 they mostly go away spontaneously, otherwise → excision of the remnant
3
New cards
Hydrocele
* non communicating hydroceles are mostly seen in neonates and young babies
* The usual type is a scrotal swelling due to incomplete reabsorption of fluid within the tunica vaginalis after closure of the processus vaginalis = primary hydrocele (may appear after a viral illness)
* Secondary hydrocele (rare) = due to testicular trauma or torsion, epididymitis or a testicular tumour
* Transilluminate, testis can be felt posteriorly
In inguinal hernia, the examiner cannot get ‘above the swelling’ this is a cardinal feature, it means that the swelling originates in the groin (==__???__==)
* May also occur in the spermatic cord or in the round ligament in girls = hydroceles of the canal of Nick
* Most hydroceles resolve between 18 and 24 months of age
A hydrocele persisting or appearing after 2 y/o may require surgery
* The usual type is a scrotal swelling due to incomplete reabsorption of fluid within the tunica vaginalis after closure of the processus vaginalis = primary hydrocele (may appear after a viral illness)
* Secondary hydrocele (rare) = due to testicular trauma or torsion, epididymitis or a testicular tumour
* Transilluminate, testis can be felt posteriorly
In inguinal hernia, the examiner cannot get ‘above the swelling’ this is a cardinal feature, it means that the swelling originates in the groin (==__???__==)
* May also occur in the spermatic cord or in the round ligament in girls = hydroceles of the canal of Nick
* Most hydroceles resolve between 18 and 24 months of age
A hydrocele persisting or appearing after 2 y/o may require surgery
4
New cards
abnormalities associated with the processus vaginalis
5
New cards
Inguinal hernia
* due to PPV
* Anatomically the same as indirect inguinal hernias in adults but without a substantial abdominal wall defect
* 1-4.4% incidence but 30% in premature neonates
4:1 male predominance
98% are indirect
* Usually reduces spontaneously (if small, larger lumps typically persist and even expand during crying, a small one stays the same during crying or straining but then reduces) unless incarcerated
* The older the child, the less likely it will become incarcerated so the younger the faster it should be fixed
* Irreducible may eventually present with symptoms of obstruction
In this case there is a real risk of testicular necrosis and or strangulation of the hernia contents
Must be brought for emergency in these cases
* Standard operation = inguinal herniotomy, there is rarely a need to perform a repair
* Anatomically the same as indirect inguinal hernias in adults but without a substantial abdominal wall defect
* 1-4.4% incidence but 30% in premature neonates
4:1 male predominance
98% are indirect
* Usually reduces spontaneously (if small, larger lumps typically persist and even expand during crying, a small one stays the same during crying or straining but then reduces) unless incarcerated
* The older the child, the less likely it will become incarcerated so the younger the faster it should be fixed
* Irreducible may eventually present with symptoms of obstruction
In this case there is a real risk of testicular necrosis and or strangulation of the hernia contents
Must be brought for emergency in these cases
* Standard operation = inguinal herniotomy, there is rarely a need to perform a repair
6
New cards
Umbilical hernia
* many newborns have this, especially if premature
* Usually resolves during the first 2 years
* Common in Afro Caribbean children and can run strongly in families
* Indications for repair are symptoms, persistence beyond 5 years and perhaps social pressure to prevent teasing
* The size of the abdominal wall defect should be determined, large defects (> 2 cm) are less likely to close on their own although very large swellings may actually have small abdominal wall defects that are likely to close spontaneously
* !! It is important to differentiate them from epigastric hernias which do ==__not__== close spontaneously
* Usually resolves during the first 2 years
* Common in Afro Caribbean children and can run strongly in families
* Indications for repair are symptoms, persistence beyond 5 years and perhaps social pressure to prevent teasing
* The size of the abdominal wall defect should be determined, large defects (> 2 cm) are less likely to close on their own although very large swellings may actually have small abdominal wall defects that are likely to close spontaneously
* !! It is important to differentiate them from epigastric hernias which do ==__not__== close spontaneously
7
New cards
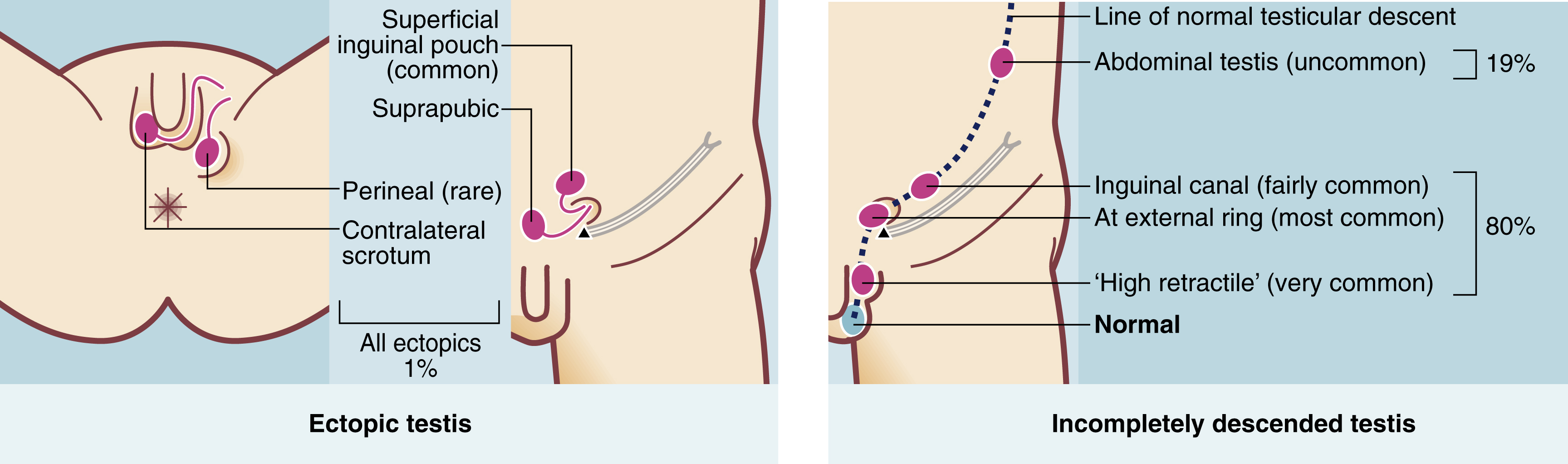
Testicular maldescent
* occurs in 3% of full term boys (higher in premature)
Full descent usually then occurs by 3-6 months (so when should it usually start by???) leaving 1.6% with maldescended testes and these ==__rarely descend later because androgen levels are highest in the first few months and then fall to very low levels until puberty__==
* 2 phases of descend:
1. Migration from the gonadal ridge to the internal inguinal ring:
* Depends on shortening of the gubernaculum, this is driven by mullerian inhibiting substance (not AMH?)
* This phase is not androgen dependent
2. Descent from the internal ring to the scrotum:
* androgen dependent
* 2nd phase maldescent can result from the testis being structurally abnormal rather than any abnormality caused by maldescent
* A maldescended testis may arrest anywhere on its path of descent. About 20% lie within the abdomen, but 80% lie in the groin area, in the inguinal canal or usually outside the external ring in the superficial inguinal pouch or upper scrotum. In addition, 1% of maldescended testes are deflected and lie ectopically
* Risk of malignancy, sub fertility and torsion or trauma
\+ cosmetic appearance and psychological impact of cryptorchidism
* neoplasia:
* carcinoma in situ is present in 2% of undescended testis → increases the risk by 10x compared to normal
* If surgical correction is done early it may reduce the risk
* Long term follow up after orchidopexy is good
* Subfertility:
* maldescended testis exhibit incomplete maturation of seminiferous tubules → abnormal sperm quantity, form or motility
This may be due to them being in the normal body temperature rather than the cooler (by 1 degree) temperature of the scrotum (recall that this is potentially important)
* Earl orchidopexy helps maturation of the tubules and spermatogenesis, ideally between 6 and 12 months
* Weirdly enough, those with ==__UNIlateral__== maldescent have more subfertility
* Torsion:
* maldescended testis are abnormally mobile
* Can occur at any age
* Intrauterine or neonatal torsion occurs proximal to the reflection of the tunica vaginalis = extravaginal
* Boys should be examined regularly from birth till school age for this to allow timely surgery
* *There may be a fibrous band within the processus vaginalis preventing elongation of testicular vessels as the boy grows. The resulting ‘stationary’ testis appears to ascend, and can no longer be drawn comfortably into the scrotum.*
* *With a history of a missing testis, the chief point is whether the testis is palpable. If palpable at the scrotal neck, it should be gently manipulated into its correct position. If it then stays put, it is retractile and needs no treatment, provided it becomes less retractile, as the boy grows. If the testis immediately retracts, it is maldescended and needs treatment*
* Optimum age for surgery is 6-12 months so fertility is not compromised
* Do we need to know how the surgery is actually done???
Full descent usually then occurs by 3-6 months (so when should it usually start by???) leaving 1.6% with maldescended testes and these ==__rarely descend later because androgen levels are highest in the first few months and then fall to very low levels until puberty__==
* 2 phases of descend:
1. Migration from the gonadal ridge to the internal inguinal ring:
* Depends on shortening of the gubernaculum, this is driven by mullerian inhibiting substance (not AMH?)
* This phase is not androgen dependent
2. Descent from the internal ring to the scrotum:
* androgen dependent
* 2nd phase maldescent can result from the testis being structurally abnormal rather than any abnormality caused by maldescent
* A maldescended testis may arrest anywhere on its path of descent. About 20% lie within the abdomen, but 80% lie in the groin area, in the inguinal canal or usually outside the external ring in the superficial inguinal pouch or upper scrotum. In addition, 1% of maldescended testes are deflected and lie ectopically
* Risk of malignancy, sub fertility and torsion or trauma
\+ cosmetic appearance and psychological impact of cryptorchidism
* neoplasia:
* carcinoma in situ is present in 2% of undescended testis → increases the risk by 10x compared to normal
* If surgical correction is done early it may reduce the risk
* Long term follow up after orchidopexy is good
* Subfertility:
* maldescended testis exhibit incomplete maturation of seminiferous tubules → abnormal sperm quantity, form or motility
This may be due to them being in the normal body temperature rather than the cooler (by 1 degree) temperature of the scrotum (recall that this is potentially important)
* Earl orchidopexy helps maturation of the tubules and spermatogenesis, ideally between 6 and 12 months
* Weirdly enough, those with ==__UNIlateral__== maldescent have more subfertility
* Torsion:
* maldescended testis are abnormally mobile
* Can occur at any age
* Intrauterine or neonatal torsion occurs proximal to the reflection of the tunica vaginalis = extravaginal
* Boys should be examined regularly from birth till school age for this to allow timely surgery
* *There may be a fibrous band within the processus vaginalis preventing elongation of testicular vessels as the boy grows. The resulting ‘stationary’ testis appears to ascend, and can no longer be drawn comfortably into the scrotum.*
* *With a history of a missing testis, the chief point is whether the testis is palpable. If palpable at the scrotal neck, it should be gently manipulated into its correct position. If it then stays put, it is retractile and needs no treatment, provided it becomes less retractile, as the boy grows. If the testis immediately retracts, it is maldescended and needs treatment*
* Optimum age for surgery is 6-12 months so fertility is not compromised
* Do we need to know how the surgery is actually done???
8
New cards
Foreskin problems
1. Phimosis:
* = a tight fibrotic ring develops at the end of the foreskin → retraction is not possible (95% of boys have a retractile foreskin by the time continence is achieved)
* Primary phimosis → chronic foreskin irritation, spraying on micturition
* Ballooning on micturition is just a sign of a non retractile foreskin and is not necessarily pathological
* Often a history or recent or recurrent balano-posthitis
* Most do not require circumcision
* may be indicated in cases of recurrent infections especially in boys with upper renal tract abnormalities or other congenital problems
* Prepuctioplasty may be enough instead of circumcision in young men
* careful attention to hygiene allows the prepuce to retract normally in time
* Attempts to dilate the phimosis under anaesthesia are unsuccessful as this causes further scarring and rapid relapse
* Secondary phimosis is usually due to balanitis xerotica obliterans
* characterised by a thickened whitish fibrotic non retractile foreskin
* ==__Plaques are formed on the deep surface which adhere to the glans and may cause meatal stenosis__==
* Peak incidence is around 8 y/o
* ==__Definite indication for circumcision__==
9
New cards
Paraphimosis
Paraphimosis sometimes occurs in children, especially if there is an underlying phimosis. The tip of the foreskin forms a tight band and when retracted, becomes trapped in the coronal sulcus behind the glans. The band inhibits venous return and causes swelling of the glans, making return of the prepuce even more difficult. Paraphimosis is painful and requires urgent reduction. This can sometimes be achieved using EMLA cream (local anaesthetic) or a penile block (if tolerated). Manual compression of the glans often allows reduction, but if this fails, general anaesthesia is needed. Sometimes the band needs dividing with a dorsal slit . Circumcision is usually performed later, once oedema has settled.
10
New cards
About 1/3 of all congenital anomalies affect the…
Genitourinary tract
11
New cards
Renal, vesicular and urethral abnormalities
* 90% of renal tract abnormalities can be detected at the 12 or 20 week scans
* Most common = hypospadias, pelviureteric junction obstruction and vesicoureteric reflux
\
1. Renal dysplasia:
* = incomplete or abnormal differentiation of the kidneys during development
* Dysplasia is classified into agenesis, hypoplastic (underdeveloped) and multi cystic dysplasia
* Bilateral agenesis is incompatible with life
* Unilateral agenesis has an incidence of 1 in 1000 with a male predominance
The contralateral kidney is usually normal and the disorder is usually not diagnosed until adulthood
* In multi cystic dysplasia → many cysts, the kidney is non function and there is ureteric atresia
→ most multi cystic kidneys spontaneously involute (atrophy) without complication but nephrectomy is sometimes needed
* Renal ectopic can be discovered incidentally or be associated with other anomalies such as anorectal malformations
* Horseshoe kidney = abnormal fusion of the developing metanephric masses during the first 2 months of foetal life
→ may cause hydronephresis by PUJ obstruction or be discovered incidentally
→ skeletal and cardiovascular abnormalities occur in atleast 1/3
→ girls with Turner syndrome often have this
2. Neonatal hydronephrosis:
* foetal urinary tract abnormalities occur in 1% of pregnancies and hydronephrosis accounts for half
* Management depends on severity and whether it is uni or bilateral
* May be caused by PUJ obstruction, vesicoureteric obstruction or reflux, multicystic kidney, primary obstructive megaureter or posterior urethral valves (???)
* Small unilateral hydronephrosis requires no action whereas larger lesions require US, micturating cystography and perhaps isotope renal scans repeated at intervals, to decide if surgery is needed
* *Early investigation is essential in bilateral severe hydronephrosis, particularly in boys, to exclude bladder outlet obstruction, secondary to posterior urethral valves*
3. Vesicoureteric reflux:
* Most common predisposing anatomical/functional abnormality in children to UTIs
* = retrograde flow of urine from bladder to kidneys → exposes the upper tracts to the greater range of pressure variation of the lower tract and to ascending infections
* Several causes but all lead to a faulty mechanism at the junction of the uterus and bladder (vesicoureteric junction)
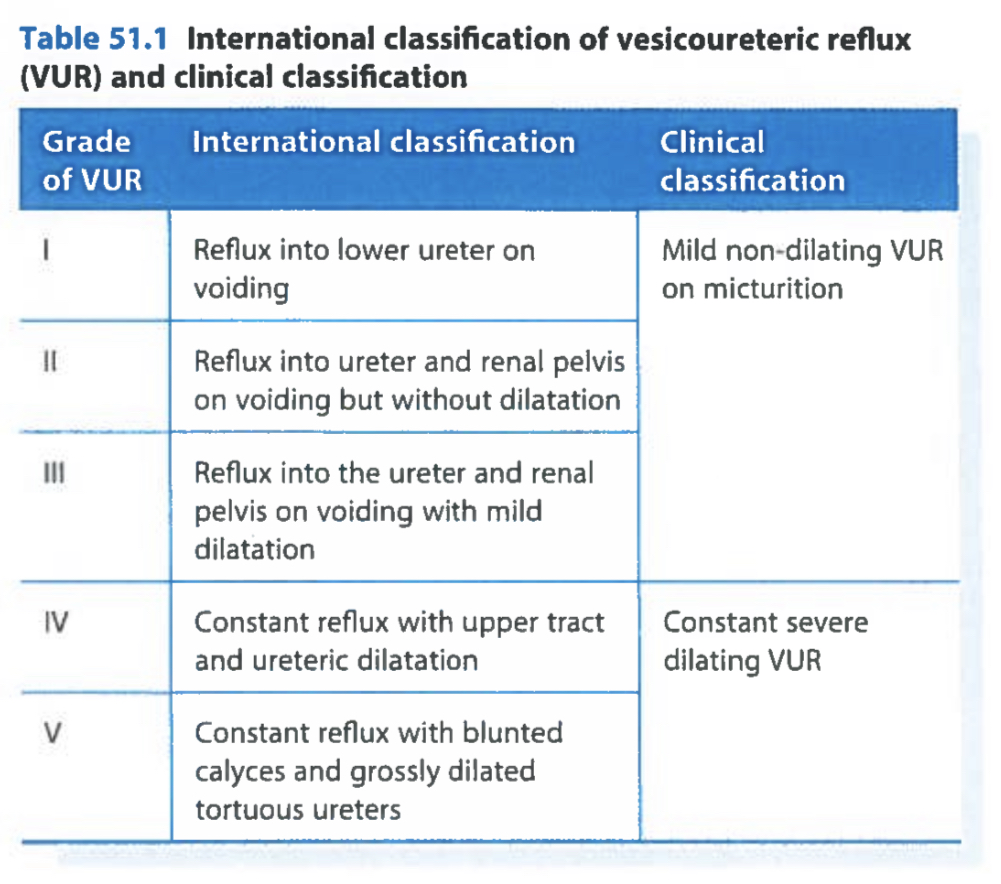
* Severity is ranged I to V
* Neonatal VUR is caused by anatomical abnormalities where female = male
But later in life there is a predisposition to girls
* Dysfunctional voiding = abnormal storage of urine or an abnormal emptying phase of micturition → urgency, frequency, incontinence and UTIs
→ vicious cycle may develop with reflux leading to infection, then bladder instability and further dysfunctional voiding
* Pathophysiology:
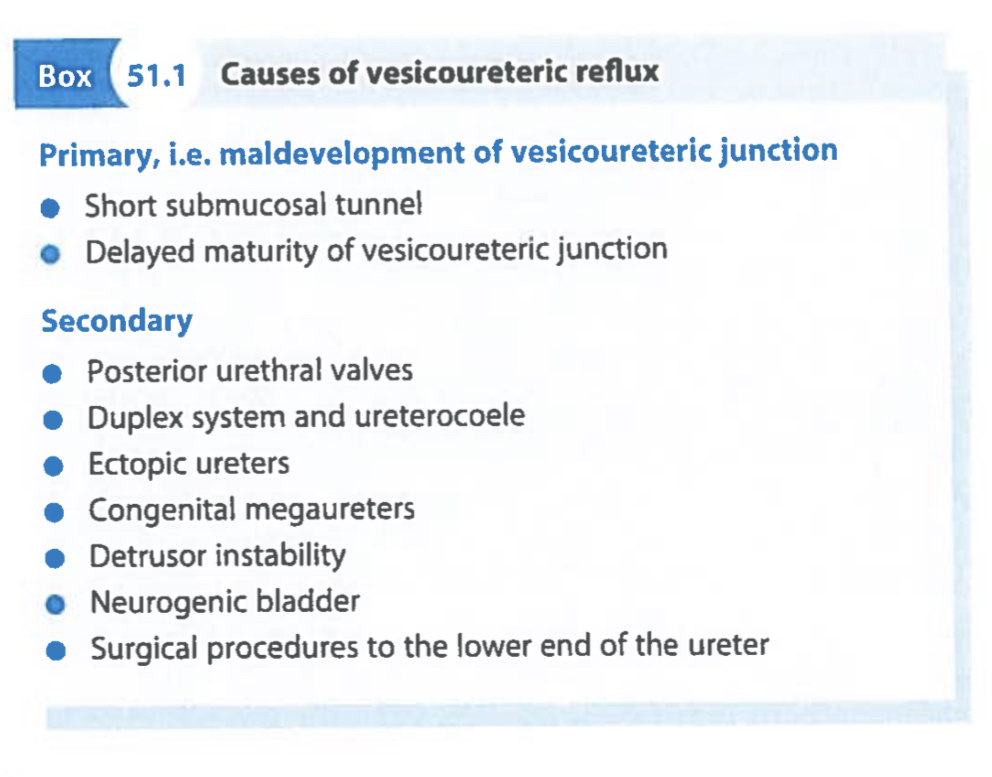
* primary VUR is the most common and it is usually due to a minor (often familial) abnormality of ureteric insertion or from ectopic or duplex ureters or congenital megaureter
* Secondary VUR may be caused by bladder outlet obstruction, neuropathic bladder (???) or surgical procedures to the lower end of the ureter
* Infection in lower tracts → ascends → reaches the bladder via the urethra and colonises it → cannot be cleared away effectively from the upper tract
Infections may also cause inflammation at the VUJ → prevents it from closing → aggravates the reflux
* Reflux of even sterile urine into the pelvicalyceal system during early childhood probably causes impaired renal development and function (why??? If its sterile???)
* Mild non dilating VUR (grades I-III) cause little damage but severe (dilating) VUR may cause renal scarring and reflux nephropathy which may progress to irreversible renal damage if untreated
* ==__May eventually lead to renal insufficiency and hypertension if both kidneys are involved in dilating VUR__==
* Loss of the normal conical shape of the papillae allows intrarenal reflux, which in the presence of infection results in pyelonephritis and renal scarring
* Clinical presentation and investigation:
* Can be detected as urinary tract dilation during antenatal screening
* May also present as one or more UTIs at any age (but recall that infants or young children do not present with the same UTI symptoms as adults and older children, may be seen instead as vomiting, fever or failure to thrive)
* In symptomatic UTIs, the prevalence of you are as 50% in neonates and 30% in those aged 2-18 years
* Demonstrating reflux US, micturating cystographic (only used in select cases despite being the golden standard as there is a 1% risk of pyelonephritis and the test is stressful) and isotope scans (??? Used for severe dilating VUR) using DMSA (bound to renal tubules, shows renal function and scarring) and MAG3 (for older children) coupled with indirect radionuclide cystography (also for older children)
* Management:
* 85% resolve as the child grows if there are no other anatomical abnormalities and it is undilated
* but the risk of UTIs should be minimised by encouraging high fluid intake, avoiding constipation and maintaining perineal hygiene plus medical management of bladder dysfunction (such as???)
* Child is maintained on continuous anti-bacterial chemotherapy (CHEMO???) and followed up regularly with US, charting growth and development, BP and plasma creatinine
* Surgical correction is indicated when there are recurrent infections, deterioration of a protract function or non-compliance with medical management
* Otherwise surgery is reserved for severe dilated VUR with complications and for other obvious anatomical abnormalities
* Newer treatments include injection of Deflux into the submucosa of the VUJ
* With ==__unilateral__== scarring, BP should be monitored lifelong for ==__hypertension__== and if ==__bilateral__== than ==__renal function__== must also be monitored
no scarring? Discharged from follow up operation
4. Pelviureteric junction dysfunction:
* Pelviureteric junction obstruction can be uni or bilateral and present between birth and 50 y/o, F = M
==__so this can be a part of PUJ dysfunction or something else???__==
* PUJ dysfunction is a congenital condition → dilatation of the renal pelvis and calyces (hydronephrosis) and incomplete or intermittent PUJ obstruction
* A normal PUJ prevents urinary reflux into the kidney when the ureter contracts but here urine accumulates and dilates the pelvicalyceal system
* Increase of pressure in renal collecting system → deterioration of renal function
* stasis may also predispose to infections and stone formation
* Most often diagnosed antenatally managed with regular postnatal follow-up with US
* Those with persistent or progressive hydronephrosis are investigated for VUR, renal function and renal drainage effectiveness and treated appropriately
* Many go undetected
* Initial diagnosis → US → dilated renal pelvis
Next step is to distinguish between static non-obstructive dilatation with preserved renal function, and genuine PUJ obstruction causing statis, dilatation and deteriorating function (==__how does the first one occur???__==) here, radionuclide diuretic renography is used
* Indications for operation → loss of differential renal function >10% or an increase in the anterior posterior diameter of the renal pelvis >35 mm
* *PUJ dysfunction with obstructive symptoms, stone formation, recurrent infections or progressive renal impairment, together with an obstructed isotope excretion curve, are indications for intervention. Pyeloplasty is indicated unless the kidney has less than 10% of total renal function, in which case nephrectomy may be indicated. Minimal invasive techniques include percutaneous antegrade endopyelotomy and laparoscopic pyeloplasty. Standard operations have a high technical success rate and usually prevent deterioration of renal function*
* Most common = hypospadias, pelviureteric junction obstruction and vesicoureteric reflux
\
1. Renal dysplasia:
* = incomplete or abnormal differentiation of the kidneys during development
* Dysplasia is classified into agenesis, hypoplastic (underdeveloped) and multi cystic dysplasia
* Bilateral agenesis is incompatible with life
* Unilateral agenesis has an incidence of 1 in 1000 with a male predominance
The contralateral kidney is usually normal and the disorder is usually not diagnosed until adulthood
* In multi cystic dysplasia → many cysts, the kidney is non function and there is ureteric atresia
→ most multi cystic kidneys spontaneously involute (atrophy) without complication but nephrectomy is sometimes needed
* Renal ectopic can be discovered incidentally or be associated with other anomalies such as anorectal malformations
* Horseshoe kidney = abnormal fusion of the developing metanephric masses during the first 2 months of foetal life
→ may cause hydronephresis by PUJ obstruction or be discovered incidentally
→ skeletal and cardiovascular abnormalities occur in atleast 1/3
→ girls with Turner syndrome often have this
2. Neonatal hydronephrosis:
* foetal urinary tract abnormalities occur in 1% of pregnancies and hydronephrosis accounts for half
* Management depends on severity and whether it is uni or bilateral
* May be caused by PUJ obstruction, vesicoureteric obstruction or reflux, multicystic kidney, primary obstructive megaureter or posterior urethral valves (???)
* Small unilateral hydronephrosis requires no action whereas larger lesions require US, micturating cystography and perhaps isotope renal scans repeated at intervals, to decide if surgery is needed
* *Early investigation is essential in bilateral severe hydronephrosis, particularly in boys, to exclude bladder outlet obstruction, secondary to posterior urethral valves*
3. Vesicoureteric reflux:
* Most common predisposing anatomical/functional abnormality in children to UTIs
* = retrograde flow of urine from bladder to kidneys → exposes the upper tracts to the greater range of pressure variation of the lower tract and to ascending infections
* Several causes but all lead to a faulty mechanism at the junction of the uterus and bladder (vesicoureteric junction)
* Severity is ranged I to V
* Neonatal VUR is caused by anatomical abnormalities where female = male
But later in life there is a predisposition to girls
* Dysfunctional voiding = abnormal storage of urine or an abnormal emptying phase of micturition → urgency, frequency, incontinence and UTIs
→ vicious cycle may develop with reflux leading to infection, then bladder instability and further dysfunctional voiding
* Pathophysiology:
* primary VUR is the most common and it is usually due to a minor (often familial) abnormality of ureteric insertion or from ectopic or duplex ureters or congenital megaureter
* Secondary VUR may be caused by bladder outlet obstruction, neuropathic bladder (???) or surgical procedures to the lower end of the ureter
* Infection in lower tracts → ascends → reaches the bladder via the urethra and colonises it → cannot be cleared away effectively from the upper tract
Infections may also cause inflammation at the VUJ → prevents it from closing → aggravates the reflux
* Reflux of even sterile urine into the pelvicalyceal system during early childhood probably causes impaired renal development and function (why??? If its sterile???)
* Mild non dilating VUR (grades I-III) cause little damage but severe (dilating) VUR may cause renal scarring and reflux nephropathy which may progress to irreversible renal damage if untreated
* ==__May eventually lead to renal insufficiency and hypertension if both kidneys are involved in dilating VUR__==
* Loss of the normal conical shape of the papillae allows intrarenal reflux, which in the presence of infection results in pyelonephritis and renal scarring
* Clinical presentation and investigation:
* Can be detected as urinary tract dilation during antenatal screening
* May also present as one or more UTIs at any age (but recall that infants or young children do not present with the same UTI symptoms as adults and older children, may be seen instead as vomiting, fever or failure to thrive)
* In symptomatic UTIs, the prevalence of you are as 50% in neonates and 30% in those aged 2-18 years
* Demonstrating reflux US, micturating cystographic (only used in select cases despite being the golden standard as there is a 1% risk of pyelonephritis and the test is stressful) and isotope scans (??? Used for severe dilating VUR) using DMSA (bound to renal tubules, shows renal function and scarring) and MAG3 (for older children) coupled with indirect radionuclide cystography (also for older children)
* Management:
* 85% resolve as the child grows if there are no other anatomical abnormalities and it is undilated
* but the risk of UTIs should be minimised by encouraging high fluid intake, avoiding constipation and maintaining perineal hygiene plus medical management of bladder dysfunction (such as???)
* Child is maintained on continuous anti-bacterial chemotherapy (CHEMO???) and followed up regularly with US, charting growth and development, BP and plasma creatinine
* Surgical correction is indicated when there are recurrent infections, deterioration of a protract function or non-compliance with medical management
* Otherwise surgery is reserved for severe dilated VUR with complications and for other obvious anatomical abnormalities
* Newer treatments include injection of Deflux into the submucosa of the VUJ
* With ==__unilateral__== scarring, BP should be monitored lifelong for ==__hypertension__== and if ==__bilateral__== than ==__renal function__== must also be monitored
no scarring? Discharged from follow up operation
4. Pelviureteric junction dysfunction:
* Pelviureteric junction obstruction can be uni or bilateral and present between birth and 50 y/o, F = M
==__so this can be a part of PUJ dysfunction or something else???__==
* PUJ dysfunction is a congenital condition → dilatation of the renal pelvis and calyces (hydronephrosis) and incomplete or intermittent PUJ obstruction
* A normal PUJ prevents urinary reflux into the kidney when the ureter contracts but here urine accumulates and dilates the pelvicalyceal system
* Increase of pressure in renal collecting system → deterioration of renal function
* stasis may also predispose to infections and stone formation
* Most often diagnosed antenatally managed with regular postnatal follow-up with US
* Those with persistent or progressive hydronephrosis are investigated for VUR, renal function and renal drainage effectiveness and treated appropriately
* Many go undetected
* Initial diagnosis → US → dilated renal pelvis
Next step is to distinguish between static non-obstructive dilatation with preserved renal function, and genuine PUJ obstruction causing statis, dilatation and deteriorating function (==__how does the first one occur???__==) here, radionuclide diuretic renography is used
* Indications for operation → loss of differential renal function >10% or an increase in the anterior posterior diameter of the renal pelvis >35 mm
* *PUJ dysfunction with obstructive symptoms, stone formation, recurrent infections or progressive renal impairment, together with an obstructed isotope excretion curve, are indications for intervention. Pyeloplasty is indicated unless the kidney has less than 10% of total renal function, in which case nephrectomy may be indicated. Minimal invasive techniques include percutaneous antegrade endopyelotomy and laparoscopic pyeloplasty. Standard operations have a high technical success rate and usually prevent deterioration of renal function*
12
New cards
Causes of VU reflux
13
New cards
International classification of VUR and clinical classification
14
New cards
Compared to VUR, what is the normal anatomy
In the normal individual, the distal ureter passes obliquely through the bladder wall so as bladder pressure rises, the ureter is flattened, acting as a sphincter preventing urine from refluxing ('flap-valve' anti-reflux mechanism). This prevents transmission of intermittent high bladder pressures.
15
New cards
Hypospadias
distal urethra fails to develop normally → urethral meatus is on the ventral surface of the penis between glans and perineum
The urethral remnant distal to the meatus is fibrotic → penis bends downwards or sideways on erection (= chordee), the more proximal the meatus, the worse the chordee
\+ ventral part of the foreskin is absent → hooded appearance
Distal hypospodias is more common (85%) = urethral opening between glans and the mid shaft with minimal chordee
Surgical repair, ideally at 6-12 months old
\
Epispadias → rare, urethral meats is dorsal, may be associated with other genitourinary abnormalities
The urethral remnant distal to the meatus is fibrotic → penis bends downwards or sideways on erection (= chordee), the more proximal the meatus, the worse the chordee
\+ ventral part of the foreskin is absent → hooded appearance
Distal hypospodias is more common (85%) = urethral opening between glans and the mid shaft with minimal chordee
Surgical repair, ideally at 6-12 months old
\
Epispadias → rare, urethral meats is dorsal, may be associated with other genitourinary abnormalities
16
New cards
Posterior urethral valves\*\*\*
*Urethral valves are congenital mucosal folds in the posterior urethra of a boy that impede or occlude urinary flow. Antenatal ultrasound screening usually detects the char- acteristic signs of oligohydramnios, a small thick-walled bladder and bilateral hydronephrosis and hydroureter. If not diagnosed antenatally, complete obstruction becomes apparent soon after birth, but partial obstruction may be overlooked*
*Severe oligohydramnios caused by this can be associated with pulmonary hypoplasia, which is incompatible with life. Neonates born with bladder outlet obstruction require urgent assessment. Urethral catheterisation facilitates accurate fluid management in the immediate postnatal period but management of post-obstructive diuresis and electrolyte abnormalities can be difficult and is best done in a specialist unit. Ultrasound scan and micturating cystography confirm the diagnosis*
*Definitive treatment involves ablating the valves by dia- thermy or cold-knife using a pediatric resecting cystoscope. Long-term follow-up is imperative, as renal function may deteriorate to the point of renal replacement therapy or trans- plantation in about 50%. Sometimes a low-capacity, high- pressure bladder persists, requiring drainage or a bladder augmentation procedure.*
*Severe oligohydramnios caused by this can be associated with pulmonary hypoplasia, which is incompatible with life. Neonates born with bladder outlet obstruction require urgent assessment. Urethral catheterisation facilitates accurate fluid management in the immediate postnatal period but management of post-obstructive diuresis and electrolyte abnormalities can be difficult and is best done in a specialist unit. Ultrasound scan and micturating cystography confirm the diagnosis*
*Definitive treatment involves ablating the valves by dia- thermy or cold-knife using a pediatric resecting cystoscope. Long-term follow-up is imperative, as renal function may deteriorate to the point of renal replacement therapy or trans- plantation in about 50%. Sometimes a low-capacity, high- pressure bladder persists, requiring drainage or a bladder augmentation procedure.*
17
New cards
Chronic constipation
* very common problem in children
* May present as faecal soiling = faecal overflow incontinence
* Early constipation usually respond to simple measures such as a high fibre diet, increased fluid intake, regular attempt at the defacation and combinations of osmotic and stimulant laxatives
* Check for CF, hypothyroidism and Hirschsprung’s disease if severe constipation
* May present as faecal soiling = faecal overflow incontinence
* Early constipation usually respond to simple measures such as a high fibre diet, increased fluid intake, regular attempt at the defacation and combinations of osmotic and stimulant laxatives
* Check for CF, hypothyroidism and Hirschsprung’s disease if severe constipation
18
New cards
rectal bleeding in neonates is most often due to…
Anal fissures, NEC or malrotation with volvulus
19
New cards
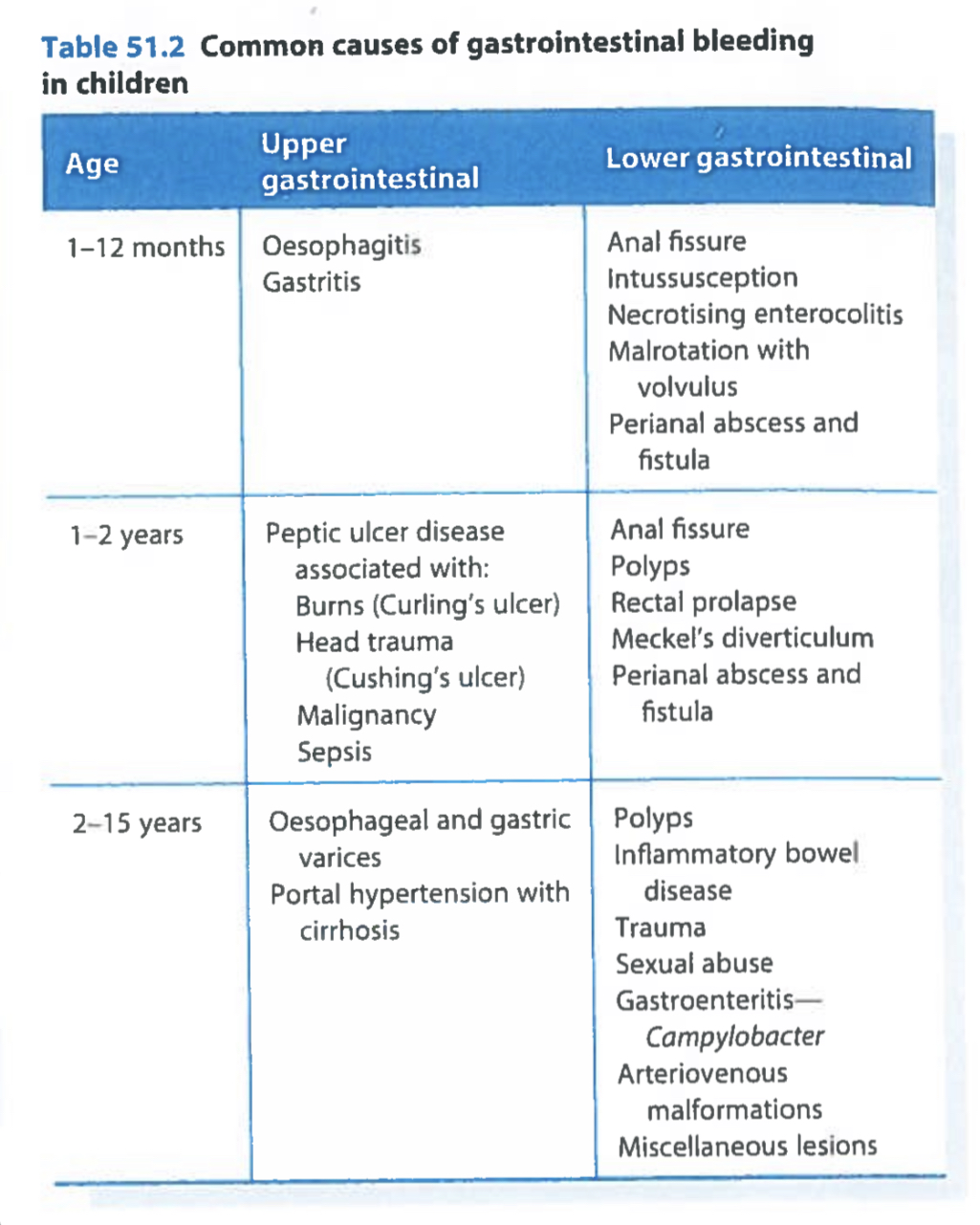
Common causes of GI bleeding in children
20
New cards
Upper GI bleeding
In neonates, apparent vomiting of blood may result from swallowed maternal blood. In older infants, gastritis may be the cause. Less common causes are bleeding disorders and coagulopathy
21
New cards
Lower GI bleeding
Neonates, think of → anal fissures, NEC or malrotation with volvulus
Older infants and children, think of → perianal abscess and fistula, anal fissure, large bowel polyps, rectal prolapse and meckels diverticulum
Where are IBD, coeliac all those???
\
1. Anal fissure:
* usually initiated by straining but may also develop after severe diarrhoea
* Main symptoms → pain at defacation, small amount of bright red blood on the stool or leaking out immediately after defacation
* readily diagnosed when digital rectal examination is found to be impossible because of extreme tenderness
* Treatment is conservative (only in children or???)
* anal skin tags often develop following healing of an anal fissure
2. Polyps:
* A juvenile hamartomatous polyp is a common cause of rectal bleeding and it almost always occur alone and in the rectum or sigmoid colon
* May present as → intermittent rectal bleeding in a child without constipation OR pain on the defacatkon without an anal fissure OR by prolapsing through the anus
* Maybe palpable on digital examination, confirmed on proctoscopy → Suture ligated and resected
if no polyp is visible → colonoscopy → remove polyp by snare
* Almost never malignant and almost never recur
* May cause rectal prolapse
* Familial adenomatous polyposis may present in childhood with rectal bleeding which may turn malignant from about the age of 16
3. Rectal prolapse:
* transient rectal prolapse is a common an alarming childhood problem usually during the first 2 years
* typically due to straining
* Maybe a presenting feature of CF
* Most can be gently manipulated back without pain although they frequently recur unless the stool is kept soft and the child can open the bowels without straining
* Persistent or recurrent? → proctoscopy and sigmoidoscopy → a rectal polyp may be the problem (occasionally)
* If simple stool softening measures fail to prevent recurrence, submucosal injections of hypertonic saline or phenol in oil may work by inducing fibrosis
4. Perianal abscess:
* common in infants
* Results from infection of an anal gland (same as in adult)
* drainage cannot be performed alone because this would turn it into a fistula so the the tract needs to be opened (same as in adults)
5. Meckels diverticulum:
* represent the embryological remnant of the vitello-intestinal duct which joined the fetal midgut and yolk sac → situated on the antimesenteric border of the distal ileum
* Typically a symptomatic
* Meckel’s diverticula often contain a variety of gut related tissues such as ==__ectopic acid secreting gastric mucosa__== which may cause inflammation and peptic ulceration
* Important cause of rectal bleeding in children below 2 y/o
* may require transfusion
* In older children the gastric mucosa more often causes chronic occult bleeding leading to iron deficiency anaemia rather than frank rectal bleeding
* Rare but peptic ulceration may cause perforation and present with signs of peritonitis
* If a Meckel's diverticulum is suspected in rectal bleeding, a radionuclide Meckel's scan may be positive but the test has a low negative predictive value and a laparoscopy or laparotomy often has to be performed to examine the bowel directly
* A Meckel's diverticulum with a narrow neck may become inflamed like appendicitis and cause similar symptoms and signs; the diagnosis is only made at operation. As with appendicitis, the complications are perforation and peritonitis. Meckel's diverticulitis is uncommon in children under 10 y/o
* Respect the diverticulum together with 2 cm of normal ileum in each side because an ectopic gastric mucosa can extend beyond it
Older infants and children, think of → perianal abscess and fistula, anal fissure, large bowel polyps, rectal prolapse and meckels diverticulum
Where are IBD, coeliac all those???
\
1. Anal fissure:
* usually initiated by straining but may also develop after severe diarrhoea
* Main symptoms → pain at defacation, small amount of bright red blood on the stool or leaking out immediately after defacation
* readily diagnosed when digital rectal examination is found to be impossible because of extreme tenderness
* Treatment is conservative (only in children or???)
* anal skin tags often develop following healing of an anal fissure
2. Polyps:
* A juvenile hamartomatous polyp is a common cause of rectal bleeding and it almost always occur alone and in the rectum or sigmoid colon
* May present as → intermittent rectal bleeding in a child without constipation OR pain on the defacatkon without an anal fissure OR by prolapsing through the anus
* Maybe palpable on digital examination, confirmed on proctoscopy → Suture ligated and resected
if no polyp is visible → colonoscopy → remove polyp by snare
* Almost never malignant and almost never recur
* May cause rectal prolapse
* Familial adenomatous polyposis may present in childhood with rectal bleeding which may turn malignant from about the age of 16
3. Rectal prolapse:
* transient rectal prolapse is a common an alarming childhood problem usually during the first 2 years
* typically due to straining
* Maybe a presenting feature of CF
* Most can be gently manipulated back without pain although they frequently recur unless the stool is kept soft and the child can open the bowels without straining
* Persistent or recurrent? → proctoscopy and sigmoidoscopy → a rectal polyp may be the problem (occasionally)
* If simple stool softening measures fail to prevent recurrence, submucosal injections of hypertonic saline or phenol in oil may work by inducing fibrosis
4. Perianal abscess:
* common in infants
* Results from infection of an anal gland (same as in adult)
* drainage cannot be performed alone because this would turn it into a fistula so the the tract needs to be opened (same as in adults)
5. Meckels diverticulum:
* represent the embryological remnant of the vitello-intestinal duct which joined the fetal midgut and yolk sac → situated on the antimesenteric border of the distal ileum
* Typically a symptomatic
* Meckel’s diverticula often contain a variety of gut related tissues such as ==__ectopic acid secreting gastric mucosa__== which may cause inflammation and peptic ulceration
* Important cause of rectal bleeding in children below 2 y/o
* may require transfusion
* In older children the gastric mucosa more often causes chronic occult bleeding leading to iron deficiency anaemia rather than frank rectal bleeding
* Rare but peptic ulceration may cause perforation and present with signs of peritonitis
* If a Meckel's diverticulum is suspected in rectal bleeding, a radionuclide Meckel's scan may be positive but the test has a low negative predictive value and a laparoscopy or laparotomy often has to be performed to examine the bowel directly
* A Meckel's diverticulum with a narrow neck may become inflamed like appendicitis and cause similar symptoms and signs; the diagnosis is only made at operation. As with appendicitis, the complications are perforation and peritonitis. Meckel's diverticulitis is uncommon in children under 10 y/o
* Respect the diverticulum together with 2 cm of normal ileum in each side because an ectopic gastric mucosa can extend beyond it
22
New cards
Go over IBD
23
New cards
Abdominal mass
* uncommon reason for a surgical referral in children
* May be caused by a malignant embryonal tumour, most often a nephroblastoma (wilms disease)
* Other causes → hydronephrosis and post traumatic pancreatic pseudocyst
\
1. Nephroblastoma:
* present in early childhood 80% before 5 y/o
* Tumour arises from embryonal renal tissue in the kidney
* Tumours are locally invasive and metastasise to regional nodes, liver, lungs and bone
* Most common presenting features → haematuria, classically after trivial trauma, anorexia, weight loss, pyrexia and hypertension
* Diagnosis is by clinical examination but confirmed by Trucut biopsy
* Tumour size and characteristics are shown by US or CT
* treatment → Neoadjuvant CT via Hickman line followed by surgery
2. Neuroblastoma:
* also an embryonal tumour, occurs in early childhood
* Highly malignant and arises from embryonal sympathetic nervous tissue in the adrenal gland or sympathetic chain
* Standard treatment is surgical resection + CT + RT, but the prognosis is poor
* Neuroganglioblastoma is a less aggressive variant
sometimes present as an abdominal mass but usually presents with FTT
* May be caused by a malignant embryonal tumour, most often a nephroblastoma (wilms disease)
* Other causes → hydronephrosis and post traumatic pancreatic pseudocyst
\
1. Nephroblastoma:
* present in early childhood 80% before 5 y/o
* Tumour arises from embryonal renal tissue in the kidney
* Tumours are locally invasive and metastasise to regional nodes, liver, lungs and bone
* Most common presenting features → haematuria, classically after trivial trauma, anorexia, weight loss, pyrexia and hypertension
* Diagnosis is by clinical examination but confirmed by Trucut biopsy
* Tumour size and characteristics are shown by US or CT
* treatment → Neoadjuvant CT via Hickman line followed by surgery
2. Neuroblastoma:
* also an embryonal tumour, occurs in early childhood
* Highly malignant and arises from embryonal sympathetic nervous tissue in the adrenal gland or sympathetic chain
* Standard treatment is surgical resection + CT + RT, but the prognosis is poor
* Neuroganglioblastoma is a less aggressive variant
sometimes present as an abdominal mass but usually presents with FTT