Management of Primary Angle Closure Glaucoma
1/50
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
51 Terms
Angle closure
iris obstruction of the anterior chamber angle resulting in an elevation of IOP. Can be primary (anatomical predisposition) or secondary (pathological process with or without pupillary block).
40
IOP in an acute angle closure attack is usually >____ mmHg
rapid and permanent blindness
ACUTE ANGLE CLOSURE IS AN OCULAR EMERGENCY as it can cause _____ if not properly treated. The longer the duration of the attack, the greater than damage to ocular structures
medical therapy, laser or incisional surgery
Treatment of acute angle closure is immediately initiated with _____ and then definitely treated with ____
reactive
Pupil response can provide indication to the response to medical therapy in acute angle closure. A pupil that is (reactive or non-reactive) has a higher likelihood of having a quick response to medical therapy.
reducing aqueous production, prostaglandin analogues, increasing TM outflow
All IOP lowering medications used in the initial treatment of acute angle closure function to lower IOP by ____. IOP lowering medications such as _____ which decrease IOP by ______ will not be effective due to blockage of the angle
Acetazolamide
the most widely used systemic carbonic anhydrase inhibitor in the treatment of acute angle closure. 2x250 mg oral tablet or 500 mg bolus initially. Additional full doses are given 4-6 hours later.
two 250 mg tablet
dosage of oral acetazolamide in acute angle closure
500 mg bolus
dosage of intravenous acetazolamide in acute angle closure
dorzolamide (trusopt 2%), corneal edema
Topical carbonic anhydrase inhibitors such as ____ should not be used in acute angle closure as they may aggravate ____ due to their topical toxicity. Additionally, they are not as effective as systemic carbonic anhydrase inhibitors
Timolol 0.5%
nonselective beta blocker used in the treatment of acute angle closure. Is initially administered at 30 minute intervals to reduce IOP 20-30% within an hour. It can then be repeated 4, 8, and 12 hours later.
Apraclonidine 1%
alpha agonist used in the treatment of acute angle closure. Reduces IOP by about 26% within 2 hours.
Pilocarpine 2%
miotic used in the treatment of acute angle closure. Is administered every 15 minutes for 4 doses then every 30 minutes.
(4% is no more effective but can still be used, may just have more side effects)
40
Miotics such as pilocarpine will not be effective initially in acute angle closures when pressures are >_____ mmHg. Should be used after IOP is already managed below this level
1-2 hours, iris sphincter infarct
Pilocarpine may be ineffective and may even exacerbate an acute angle closure attack lasting longer than ____ due to ____
Lens induced angle closure, malignant glaucoma (aqueous misdirection)
two contraindications of pilocarpine
Glycerin
hyperosmotic agent used in the treatment of acute angle closure. Is administered 1-1.5 g/kg to reduce IOP in 30-90 minutes lasting for about 5-6 hours.
Hyperglycemia, dehydration
two side effects of oral glycerin making it contraindicated in diabetics or elderly patients with renal failure or cardiovascular disease
Mannitol/Isosorbide
oral hyperosmotic agent used in the treatment of acute angle closure. Is administered 1-2 g/kg to reduce IOP in 1-3 hours for about 3-5 hours. Is generally less effective than oral glycerin, but is safer in diabetics as it is not metabolized.
Metabolic acidosis, electrolyte disturbance
two side effects of systemic hyperosmotic agents
Indentation
____ on gonioscopy may be tried as a therapeutic means to break an angle closure attack, but peripheral iridotomy is still indicated even when the attack is broken
Prednisolone acetate 1%
topical steroid dosed as 1 gtt every 15 to 30 minutes four times then q1h in order to address inflammation following IOP control of an acute angle closure attack.
Anterior chamber paracentesis
procedure where a small perforation of the anterior chamber is made in order to relieve pressure during an acute angle closure. Is not commonly performed as many consider this an aggressive and too invasive initial treatment.
Laser peripheral iridotomy (LPI)
the definitive treatment of acute primary angle closure WITH PUPIL BLOCK. Works best for patient with early synechiae development. Patient having chronic PAS or glaucoma optic neuropathy respond poorly and may need further treatment.
temporal or nasal
Currently laser LPI procedures are performed _____ in order to reduce optical aberrations induced by the procedure
peripheral third, anterior, crypt
Laser peripheral iridotomy should be placed in the ____ of the iris _____ to any arcus preferably within a ____ where the iris is thinner
Cataracts, corneal or lenticular burns, corneal edema
three complications associated with laser peripheral iridotomy
Iridectomy
surgical removal of a portion of the iris at its root leaving the pupillary margin and sphincter muscle intact. Is indicated when laser treatment cannot be accomplished or is no effective.

suprachoroidal hemorrhage
Iridectomy is much more invasive than LPI and poses an increased risk of ____ in patients having high IOP
Laser peripheral iridoplasty (gonioplasty)
procedure involving applying a series of laser burns of low power, long duration, and large size to the extreme peripheral iris. Scarring following laser treatment causes compaction of the iris stroma increasing the space between the anterior iris surface and the TM. Is typically used for PLATEAU IRIS, but can also be used to generally break an acute angle attack. LPI should still be performed in patients having pupil block.

Laser peripheral iridotomy
the most appropriate long lasting therapy for subacute angle closure glaucoma
Laser peripheral iridoplasty (gonioplasty)
procedure that may be used in an attempt to break recently formed synechiae in patients having subacute angle closure glaucoma
Trabeculectomy
filtration surgery that can be used in patients having extensive synechiae caused by subacute closure glaucoma.
270
Trabeculectomy filtering procedure is performed with >____ degrees of the angle is closed by synechiae
Endophthalmitis, bleb leaks
two sight threatening complications that may occur following trabeculectomy
Chronic angle closure
angle closure caused by coexistence of peripheral anterior synechiae and appositional angle closure.
Laser peripheral iridotomy
treatment for chronic angle closure without PAS
Laser peripheral iridoplasty (gonioplasty)
treatment for chronic angle closure with PAS
Trabeculectomy
treatment for chronic angle closure to which laser iridotomy or LPI is ineffective
40-80, 5-10
The fellow eye has a ____% chance of developing an acute angle closure attack within ____ years and therefore prophylactic LPI should be performed in the fellow eye
3-6%
risk of acute angle closure in angle closure suspects
13%
risk of chronic angle closure in angle closure suspect
lens thickness, anterior position of the lens
The anterior chamber depth is primarily determined by the _____ and _____.
Lens extraction
the definitive treatment for phacomorphic glaucoma
greater
The narrower the preoperative angle, the (lesser or greater) the postoperative widening of the angle following lens extraction
EAGLE, 1.8
The ____ study showed a mean IOP that was ___ mmHg lower in patients having lens extraction versus LPI
Goniosynechialysis
procedure that removes peripheral anterior synechiae from the angle wall in order to restore trabecular outflow.
60%
percentage of patients with acute primary angle closure that have persistent IOP elevation requiring glaucoma medications following laser iridotomy. Post operative IOP control in these patients depends on amount of TM damage and extent of PAS
80%
effectiveness (percent) of goniosynechialysis in eyes with PAS for the first year
cataract removal, lens
Goniosynechialysis is more effective when performed after _____ as the ____ is a significant contributor to PAS formation
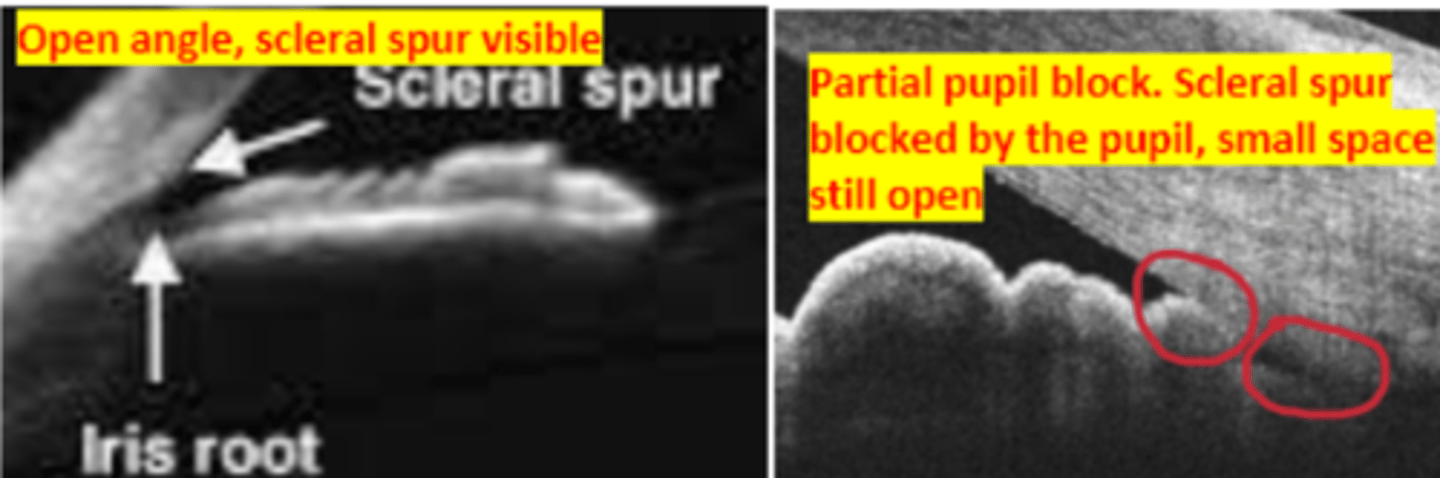
250-500
Anterior segment imaging measures the anterior chamber depth by locating the trabecular meshwork as being _____ microns anterior to the scleral spur demarcated by the person performing the test