Lecture 1: Neuroanatomy of CNS & PNS
1/94
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
95 Terms
Neuron contains
-Functional unit of the nervous system
-contains soma, dendrites, axon, axon terminal, and synapse
Soma (cell body)
-Part of the neuron
-Contains the nucleus and does most of the cell's processing and maintenance
Dendrites
-Branch like structures coming off the soma
-Receive input (signals) from other neurons
Axon
-Long extension from the cell body
-Carries the output to the axon terminal (away from soma)
Axon Terminal
-Very end of the axon where the neuron passes the signal onto the next cell
Synpase
-The junction (tiny gap) between one neuron's axon terminal and another neuron's dendrite
-Where communication occurs
Myelin Sheath
-Protective layer on the axon which insulates the axon and allows for fast impulses of the signal
Central Nervous System (CNS)
-Brain & spinal cord
Peripheral Nervous System (PNS)
-Spinal & cranial nerves
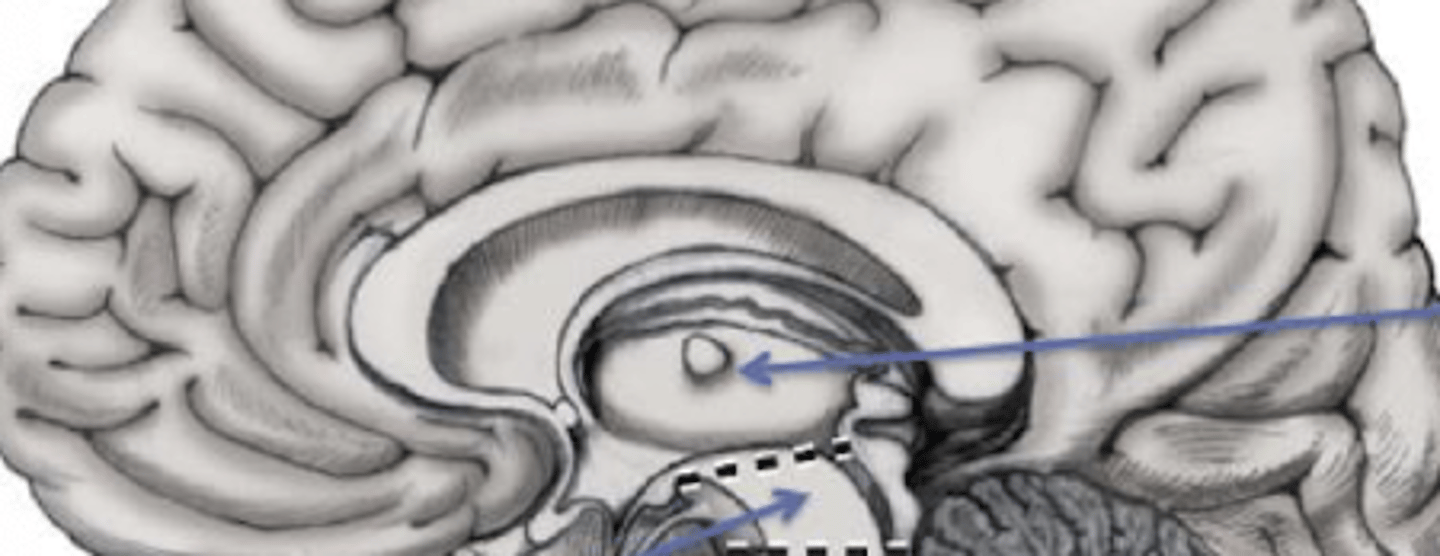
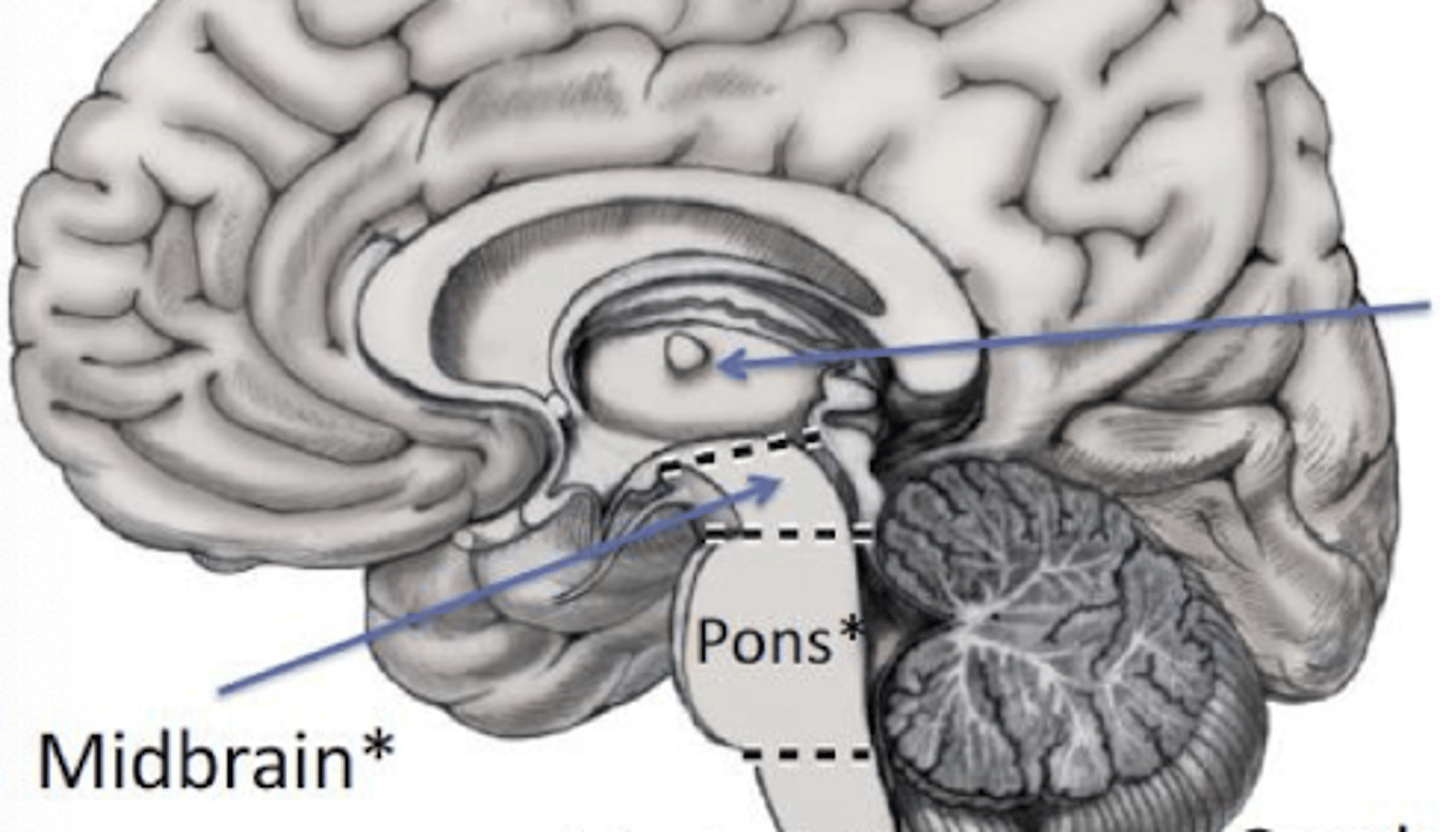
Brainstem
-Consists of midbrain, medulla and pons
Diencephalon (thalamus, hypothalamus)
Cerebellum
White Matter
-regions containing myelinated axons
Grey Matter
-Regions containing cell bodies of neurons
Medial Longitudinal Fissure
-Separates the two cerebral hemispheres: right and left
-A really big sulcus
Corpus Callosum
-2 cerebral hemispheres (left & right) are connected by this
-It is white matter
-Allows for communication b/w 2 hemispheres
Gyri
-Ridges or bumps on the surface of the brain
Sulci
-Grooves or valley's between the gyri
6 Lobes of the Cerebrum
-Parietal
-Frontal
-Temporal
-Occipital
-Limbic
-Insula
Central Sulcus
-Divides the parietal and frontal lobes
Lateral Sulcus
-Frontal/parietal lobes are separated from temporal lobe by this
Frontal Lobe
-Voluntary movement
-Short term memory
-Motivation
-Planning
-Speech
Temporal Lobe
-Auditory processing
Parietal Lobe
-Integrates sensory stimuli
-Language
Occipital Lobe
-Center for visual processing
Limbic Lobe
-Next to the corpus callosum and extends onto the medial surface of the temporal lobe
-Modulation of emotions
Insula
-Located deep within the lateral sulcus
-Taste, vestibular function
Upper Motor Neuron (UMN)
-Located fully in CNS
-Neurons of the cerebral cortex & brainstem that govern the activity of LMNs in the brainstem & spinal cord
-Start in motor cortex (in the brain) and travel down through the brainstem and spinal cord
-Send signals down to anterior horn to synapse with lower motor neurons
Lower Motor Neuron (LMN)
-Cell body is located in the CNS (anterior horn OR cranial nerve motor nuclei in brainstem) but axon is in the PNS
-Innervates the skeletal muscle (or target)
-synapses with UMN at anterior horn
Enlargements
there are two well defined __________________ to accommodate for innervation of the upper and lower limbs (house motor neurons)
-Cervical & lumbosacral
Conus medullaris
-Term used to describe the vertebral level at which the spinal cord ends L1/L2
Cauda Equina
-Collection of nerve roots below the conus medullaris
-Horse's tail
Spinal Nerve
-Contain an anterior/sensory (ventral) and dorsal/motor (posterior) root which combine to form a mixed ______
-Exit the intervertebral foramen
Efferent Nerve
-Exiting the CNS
-Motor
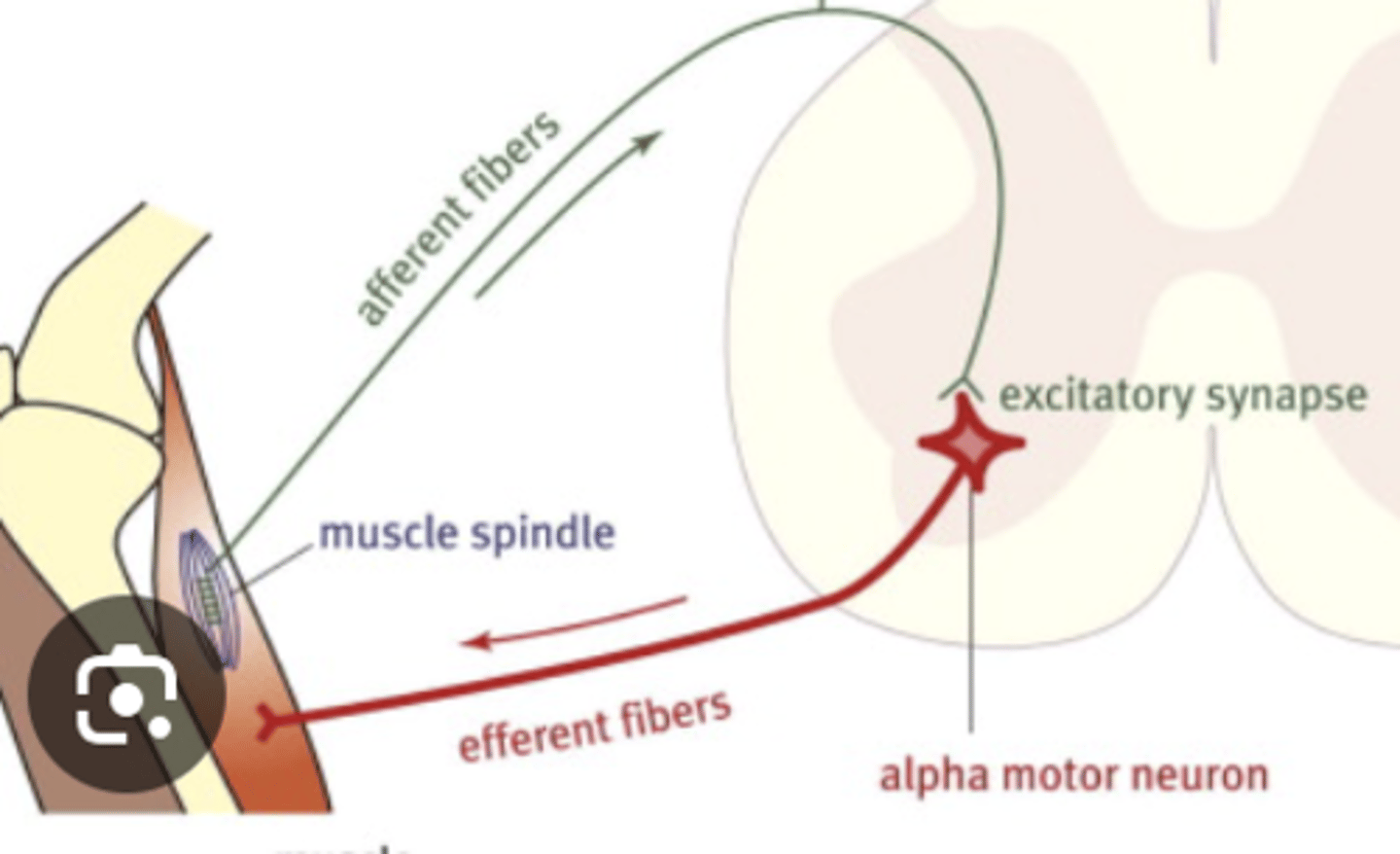
Afferent Nerve
-Sensory
-Going towards the CNS
Dermatome
-Area of skin that is mainly supplied by afferent nerve fibres (posterior) root of a spinal nerve
-Changes in sensation are detected by posterior root and are carried towards the CNS
Peripheral nerves
-Refer to both spinal nerves/nerve roots, cranial nerves & terminal branches (i.e., median nerve)
-Collection of axons
-Most are mixed (motor & sensory)
Terminal branches
-Collection of spinal nerves at the end of the plexi
Types of Lower Motor Neurons
1. Alpha Motor Neurons
2. Gamma Motor Neurons
3. Cranial nerve LMNs
Alpha Motor Neurons
-LMNs that innervate extrafusal muscle fibers (regular skeletal muscle fibers)
-These directly cause muscle contraction (movement & posture)
Gamma Motor Neurons
-LMNs that innervate infrafusal muscle fibers (muscle spindles)
-keep the spindle sensitive to changes in length (keep the spindles taut so stretch can always be detected)
-Sudden lengthening will be detected
-Active during voluntary movement (alpha-gamma co-activation & passive stretch)
Cranial Nerve LMNs
-Originate in the brainstem
Motor Unit
-One alpha motor neuron and the skeletal muscle fibers it innervates (one muscle)
-All fibers in this _____ contract together when the neuron fires
-There can be small and large of these...small = few fibers, precise control while large = many fibers, strong
UMN Lesions
-Damage to the descending tract before the anterior horn of the spinal cord
Lower Motor Neuron Lesion
-Damage to the alpha motor neuron at or distal to the anterior horn
i.e., Damage to cell body in the anterior horn (CNS), ventral root before joining spinal nerve or even after their axons continue in spinal/peripheral nerves (PNS)
Signs of UMN Lesion
-Weakness/paralysis/paresis (possibly)
-Hypotonia (possibly)
-Hypertonia (Yes)
-Hyporeflexia (Possibly)
-Hyperreflexia (Yes)
-Babinski/Hoffman's (Yes)
-Atrophy (Minimal)
-Nerve conduction tests (normal)
-EMG (normal)
-Fasiculations (no)
Why do UMN lesions cause hypertonia?
-When passively stretching a limb they muscle spindles are stretched - the spindle sends sensory input --> alpha motor neuron --> slight reflex contraction (i.e., normal resistance) which is fine tuned by UMNs
-With no control from UMN, the alpha motor neurons are more excitable, the sensory input excites the alpha MNs with no fine tuning and the muscle resists more against stretch
Signs of LMN Lesion
-Weakness/Paralysis/Paresis (YES)
-Hypotonia (YES)
-Hypertonia (NO)
-Hyperreflexia (NO)
-Hyporeflexia (YES)
-Babinski & Hoffman's (NO)
-Atrophy (YES, LOTS)
-Nerve conduction tests (Abnormal)
-EMG (Fibrillation potentials)
-Fasciculations (YES)
How does the tract run from UMN to LMN?
-Moves from right side (cerebral cortex & brain stem) to left side (spinal cord)
If a lesion is present in cerebral cortex or brain stem (UMN) on right side of LATERAL CORTICOSPINAL TRACT where would deficits be seen?
-On left side and below the lesion
**Spastic paresis, hyperreflexia, hypotonia
If a lesion is present in the spinal cord (UMN) on the left side of LATERAL CORTICOSPINAL TRACT, where would deficits be seen?
-Ipsilateral (same side)
**Spastic weakness below the level of the lesion
If a lesion is present at the LMN (anterior horn) on the left side of LATERAL CORTICOSPINAL TRACT, where would deficits be seen?
-Ipsilateral on same side
**Flaccid paralysis at level of lesion, hypotonia, hyporeflexia
UMN Injuries
-Stroke
-Spinal Cord Injury *Could also be LMN
Stroke Signs
-UMN injury
*UMN lesion
*Paresis
*+ Babinski & Hoffman's
*Hyperreflexia
*Hypertonia
Paresis
Partial loss of voluntary movement (weakness)
*this is usually present after UMN lesions because the voluntary command signal leading to weakness; however, LMNs are still active so there is not full paralysis
Spinal Cord Injury
-Primarily UMNs affected
*CAN ALSO BE LMN impact or MIXED
-If injured at C-spine (more likely UMN presentation)
-If injured at L-spine (more likley LMN presentation)
-Weakness below the level of the lesion (most likely bilateral)
-Hypertonia/Hyperreflexia
-Bladder/Bowel involvement
-Sensory loss below lesion (sensory tract may also be impacted)
Why is is more likely that UMN are impacted in spinal cord injury at C-spine?
-More white matter
Why is is more likely that LMN are impacted in spinal cord injury at L-spine?
-Larger proportion of grey matter
ALS Presentation
-Mixed (UMN & LMN)
-Unknown cause
-Decreased number of motor units (both small & large)
-Fasciculations
-Muscle weakness & wasting (commonly with resp muscles(
-Negative prognosis (death)
Fasciculations
-Spontaneous firing of dead/dying motor units
-Twitching under the skin
Alpha Motor Neuron Injury
-LMN Injury
-Wasting & weakness
-No sensory involvement (the sensory tract was not impacted)
In a lesion to UMN or LMN - is there any sensory involvement?
-UMNs & LMNs are purely motor
*Exception, if the lesion also affects the dorsal root or dorsal horn, there could be sensory deficits (ex: spinal cord injury or peripheral neropathies)
Spinal Nerve Injury
-Weakness in distribution of nerve root i.e., C5 (myotomal weakness)
-Associated sensory symptoms in same distribution i.e., C5 (dermatome)
Peripheral Nerve Injury
-Weakness and sensory loss in distribution of affected nerve(s) (terminal branches)
-Wasting if severe
Peripheral Nerve Injury Classifications
-Neuropraxia
-Axonotmesis
-Neurotmesis
Neuropraxia
-Injury to my myelin while the axon is intact
-Temporary conduction block
-Pt may complain of transient weakness

Axonotmesis
-Injury to axon & myelin but supporting connective tissue is intact
-Conduction block

Neurotmesis
-Most severe peripheral nerve injury
-Complete nerve laceration
-Injury to axon & supporting connective tissue

Wallerian Degeneration
-Results when a nerve fiber is cut or crushed (axonotmesis or neurotmesis) and part of the distal axon degenerates
Ways to Assess the PNS
-Muscle Strength
-Deep Tendon Reflexes
-Sensation testing
-Nerve specific testing (i.e., Tinnel's Test)
-Nerve conduction studies (NCS) & EMG
Which 2 ways can be used to assess the PNS (is it UMN or LMN Lesion)?
-Nerve Conduction Studies
-EMG
Nerve Conduction Studies (NCS)
-Assess nerve integrity (motor vs sensory nerves)
-Assess Neuromuscular junction (where nerve meets muscle)
Muscle Response in NCS
-Stimulate the axons and observe muscle contraction
-Record the contraction (Compound motor action potential CMAP) or M-Wave
Sensory Response in NCS
-Recorded signal is called a sensory nerve action potential (SNAP)
Compound Motor Action Potential (CMAP)
-Gives information on Amplitude, Latency, Conduction Velocity
-Combined electrical signal of all action potentials in muscle fibers firing together
Amplitude
Refers to # of axons being stimulated
I.e., if there are more axons, there is a greater amplitude
Latency
-Time between stimulation and M-wave
-Most affected by demyelination (no fast transmission of impluse)
Conduction Velocity
-Distance/Time (m/s)
(How fast an electrical impulse travels along a nerve)
-Impacted by both axonal loss and demyelination
*Less axons decreases the amplitude but if myelin is preserved then this would remain mostly unchanged
When is lower amplitude observed?
-In Peripheral nerve injuries
-ALS
*Anything that causes axonal loss
When is latency prolonged?
-Any injury that causes demyelination
What does demyelination cause?
-Longer latency
-CMAP or M-wave is spread because some neurons are affected while others are intact (axons are not in sync)
-Conduction velocity is slowed
Needle EMG
-Inserting a needle into a muscle to assess the activity from individual muscle fibers at rest and during contraction
-Size of the motor unit potential (M-Wave) tells us about underlying pathology
*Can be used to distinguish between LMN, UMN and myopathies (muscle diseases)
Motor Unit Potential
-summation of electrical activity of the muscle fibers of the motor unit
2 types of peripheral nerve recovery
-Axonal Repair & Regrowth
-Collateral sprouting
How long does it take for axonal regeneration?
-Faster closer to injury site (3mm/day)
-slower further away (1mm/day)
*When a nerve is injured, the part of the axon immediately next to the injury starts to regenerate faster
*As regenerating axon grows farther away from injury site, the regrowth slows down
2 players in Axonal Regrowth
1. Macrophages
2. Schwann Cells
Macrophages (Axonal Regrowth)
-Clear away degenerating parts of the axon
Schwann Cells (Axonal Regrowth)
-Act as a guide and stimulate regrowth of the axon
1. Form a growth cone which extends to search for target
2. Provide a framework to help guide growing axons (cell adhesion molecules guide the axon to target)
3. Secrete neurotrophic signals that promote axon growth
Is Crush better recovery or cut?
-allows for axons to have continuity and less degeneration (Schwann cell framework is less disrupted)
-The damaged segments of axon distal to _____ help guide the regenerating proximal segment
-Recovery is more rapid in this one
Rapposition Surgery
-Severed nerves are reconnected using this
-Cut nerves are salvageable if repaired within 3 months
-New Schwann cells can still grow even with a lot of damage
What happens if the injury is severe?
-Outcomes tend to be poor if the distal end of the nerve is not available for reapposition
-Less than 50% of patients recover satisfactory motor and sensory function after nerve repair
Can Peripheral Nerve Regeneration be fast-tracked?
-No
-The new pathways (even if imprecise) can be trained to become functional but regrowth cannot be fast-tracked
-Exercise helps regrowth in animals (not humans)
Collateral Sprouting
-M-wave preserved despite a decrease in number of motor units due to increase in motor unit size
-Preserved motor units sprout new axonal branches to reinnervate muscle fibers that lost their alpha motor neuron
-those muscle fibers become part of a larger motor unit — meaning one motor neuron is now controlling more muscle fibers than it originally did
Gamma Motor Neuron Example
1. standing on a bus and it suddenly jerks forward.
2. calf muscles need to contract instantly to keep you from falling.
3. muscle spindles detect the stretch in your calf muscles.
4. Gamma motor neurons have already made sure those spindles are sensitive, even though calf is partly contracted while standing.
Example of Axonal Regeneration
-Median nerve is cut at the forearm
-Part of the axon right next to the cut starts regenerating at 3mm/day
-As axons grow toward the hand muscles (farther away), the effective growth slows to 1mm/day