Looks like no one added any tags here yet for you.
why is it important to immobilise the area under surgical investigation
to avoid reflexes and spasms during surgery
relexes are not suppresed until deep anaesthesia
which type of motor neuron is relevant her e
the somatic motor neuron and innervation because its for skeletal muscle
describe somatic motor neurone
single motor neuron connecting CNS to the skeletal muscle
cell bodies are in the brain stem
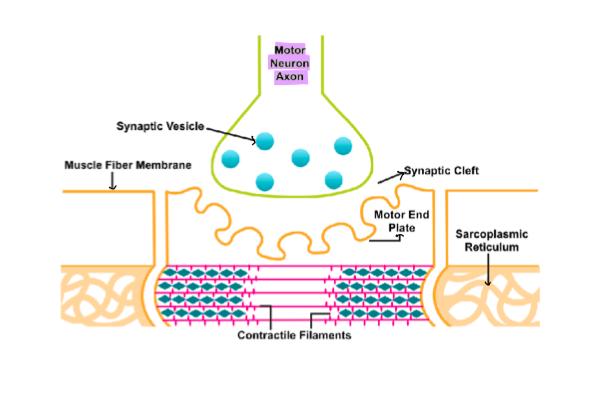
neuromusclar junction
where a motor neuron communicates with a skeletal muscle fiber to facilitate muscle contraction.
which receptor does ACH bind to at skeletal muscle NMJ
nicotinic receptors
briefly describe ACh release at the NMJ
describe the structure of the nicotinic receptor on the motor end plate
ligand gated ion channel
contain a,b,s, and y subunits
two ACH bind
CNS and ganglioin nACHr have different subunits
describe how muscle contraction occurs after ACh is released into the synapse
Ach binds to nicotinic receptors
= NA+ influx
= End plate potential
=NA channels open
= AP in the muscle cell membrane
= Muscle contraction
what is excitation-contraction coupling in skeletal muscle
na+ driven action potential opens l-type calcium channels
stimulates CICR from intracellular stores and muscle contraction
what do NMBA’s interfere with
with the post synaptic action of ACh
two types of NMBAs and relationship with nicotinic receptor
non-depolarising agents : nicotinic antagonists
Depolarising blocking agents: weak nicotinic agonists
example of non-depolarising agent
d-turbocurarine
causes paralysis by blocking NMBM but NOT nerve conduction of muscle contractility
around how many rnicotinic eceptors does d-turbocurarine need to block to have effect
90% bc there is alot of Ach released at NMJ
causes decrease in end plate potential
name a synthetic derivative of d-turbocurarine
rocuronium
describe effect of Tubocurarine on neuromuscular transmission
reduces the end plate potential amplitude so that no action potential is generated
what is recovery from non depolarising NMBA’s determined by
by susceptibility to cholinesterase’s and clearance
properties of Rocuronium
non-depolarising agent
fast onset
intermediate duration
side effects of non-depolarising blockers
hypotension (ganglion blockade)
tachycardia - M2 blockade (some of the drugs)
Bronchospasm’s (histamine release from mast cells)
Respiratory failure - assisted ventilation used
Autonomic ganglion block at high doses
Why might hypotension and tachycardia occur with non depolarising agents
hypotension → ganglion blockade
tachycardia → M2 blockade
example of depolarising agent
succinolylcoline + suxamethonium
how do depolarising agents work
2 phases but basically agonise receptors and desentisise it until muscle is flaccid
phase 1 block of depolarising agents
agent binds to Ach receptor and remains bound
= prolonged depolarisation
= prevents muscle from repolarising
phase 2 block of depolarising agents
the persistent stimulation causes desensitisation (doesn’t respond to the repolarisation)
= channels no longer open in response
= Muscle becomes flaccid as calcium is taken into stores
advantages of depolarising nMBA
rapid onset
short duration of action
less likely to elicit histamine release
side effects of depolarising NMBA
bradycardia - direct muscarinic action
potassium release - inc in cation permeability
prolonged paralysis
increased intraocular pressure
post-operative pain
why can hyperkalaemia be caused by depolarising agents
Normally, during muscle activation, small amounts of potassium ions leak out of muscle cells into the bloodstream as part of the cellular depolarization process.
when succinylcholine causes a sustained depolarization= more significant release of potassium from the muscle cells into the extracellular fluid.
other uses of NMBA
lethal injections
electroconvulsive therapy
what is neostigmine and how does it cause reversal of NMBA
Achcholinesterase inhibitor
raises synaptic AXh
reverses non depolarising block
potentiates depolarising block
can neostigmine cross the BBB and why
no bc its lipid insoluble = minimised CNS effects
how quickly does neostigmine work
within 1 minute
peak effect in 10 minutes
when is the elimination half life of neostigmine prolonged
in renal disease
side effects of neostigmine
bradycardia
increases PONV and GI disturbances
why can