Mydriatics and Cycloplegics: Understanding Adrenergic Receptors in Biology
1/140
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
141 Terms
what is the sympathetic nervous system?
- branch of the autonomic nervous system that opposes physiological effects of the parasympathetic division
- FIGHT & FLIGHT
- adrenergic branch
what is the parasympathetic nervous system?
- branch of the autonomic nervous system that opposes physiological effects of the sympathetic division
- REST & DIGEST
- cholinergic branch
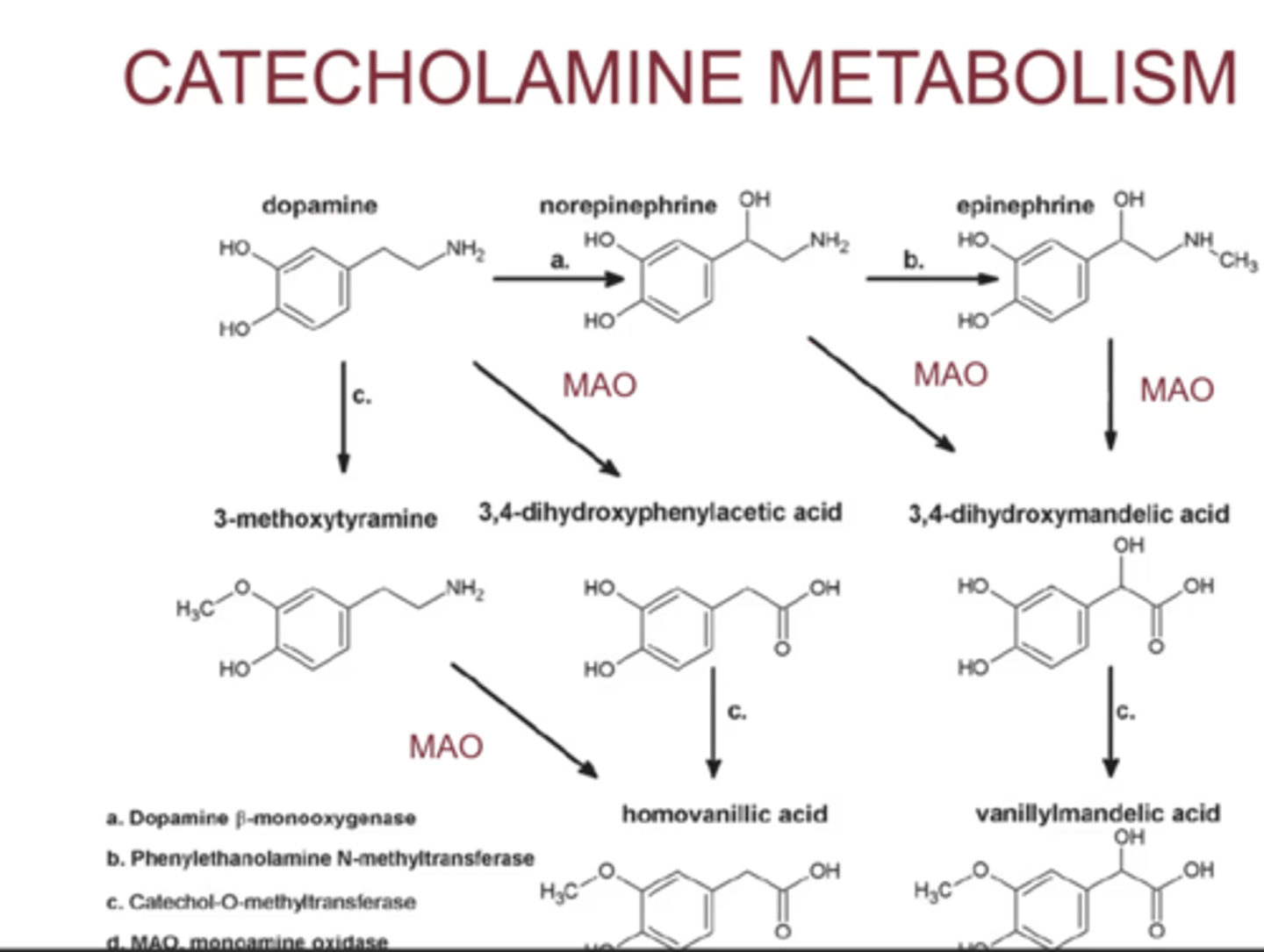
What are catcholamines?
- biogenic amines derived from phenylalanine/tyrosine including dopamine, epinephrine and norepinephrine; produced from tyrosine in the adrenal medulla and postganglionic fibers of the sympathetic nervous system
what are MAO?
- monoamine oxidase; an enzyme of catecholamine metabolism
what are COMT?
- Catechol-O-methyl transferase; an enzyme of catecholamine metabolism
what is Miosis?
- pupillary contraction
what is midriasis?
- pupillary dilation
what is Cycloplegia?
- paralysis of the ciliary body musculature responsible for accommodation
- done by blocking M3 on the ciliary body
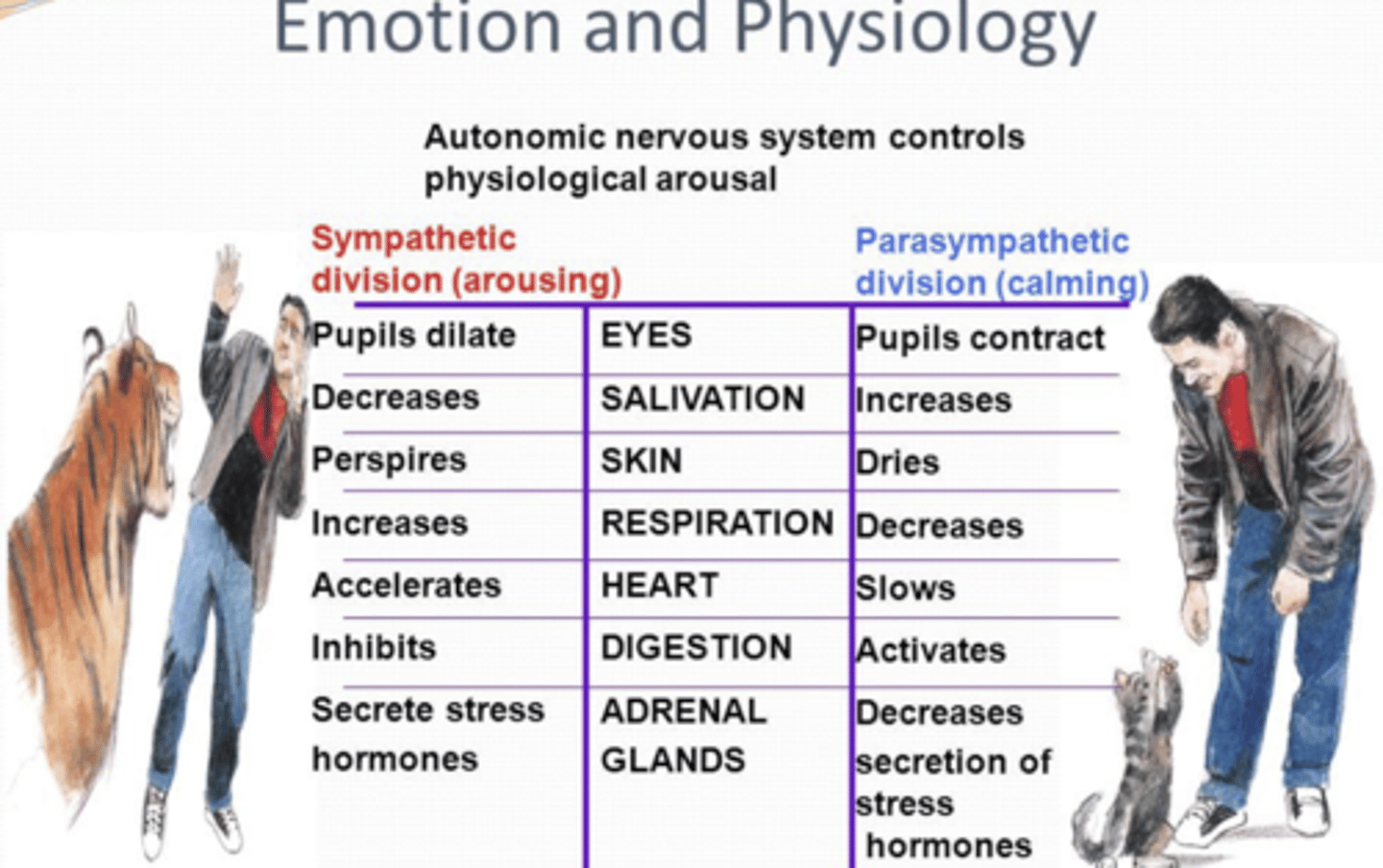
what happens to the eyes during sympathetic vs parasympathetic innervation?
- symp: mydriasis
- parasymp: miosis
what happens to lids during sympathetic innervation?
- symp: retract
what happens to skin during sympathetic vs parasympathetic innervation?
- symp: perspires
- parasymp: dries
what happens to salivation during sympathetic vs parasympathetic innervation?
- symp: decreased
- parasymp: increases
- same with lacrimation for eyes
what happens to respiration during sympathetic vs parasympathetic innervation?
- symp: increases
- parasymp: decreases
what happens to the heart during sympathetic vs parasympathetic innervation?
- symp: accelerates
- parasymp: slows
what happens to digestion during sympathetic vs parasympathetic innervation?
- symp: inhibits
- parasymp: activates
what happens to adrenal glands during sympathetic vs parasympathetic innervation?
- symp: secretes stress hormone
- parasymp: decreases secretion of stress hormone
what is the precursor for norepinephrine and epinephrine?
- dopamine
where is norepinephrine secreted vs epinephrine?
- norepinephrine: done postganglionically at the synaptic clefts (more important when dealing with pharm)
- epinephrine: into bloodstream by adrenal medula
does the body have higher concentration of norepinephrine or epinephrine?
- norepinephrine also found in bloodstream
- exist in concentrations 3x higher than epinephrine in normal conditions (not fight or flight response)
- dopamine gets converted to norepinephrine and norepinephrine gets converted to epinephrine
- MAO metabolizes dopamine, norepinephrine, and epinephrine into the middle acids, then eventually vanilla acids at the bottom
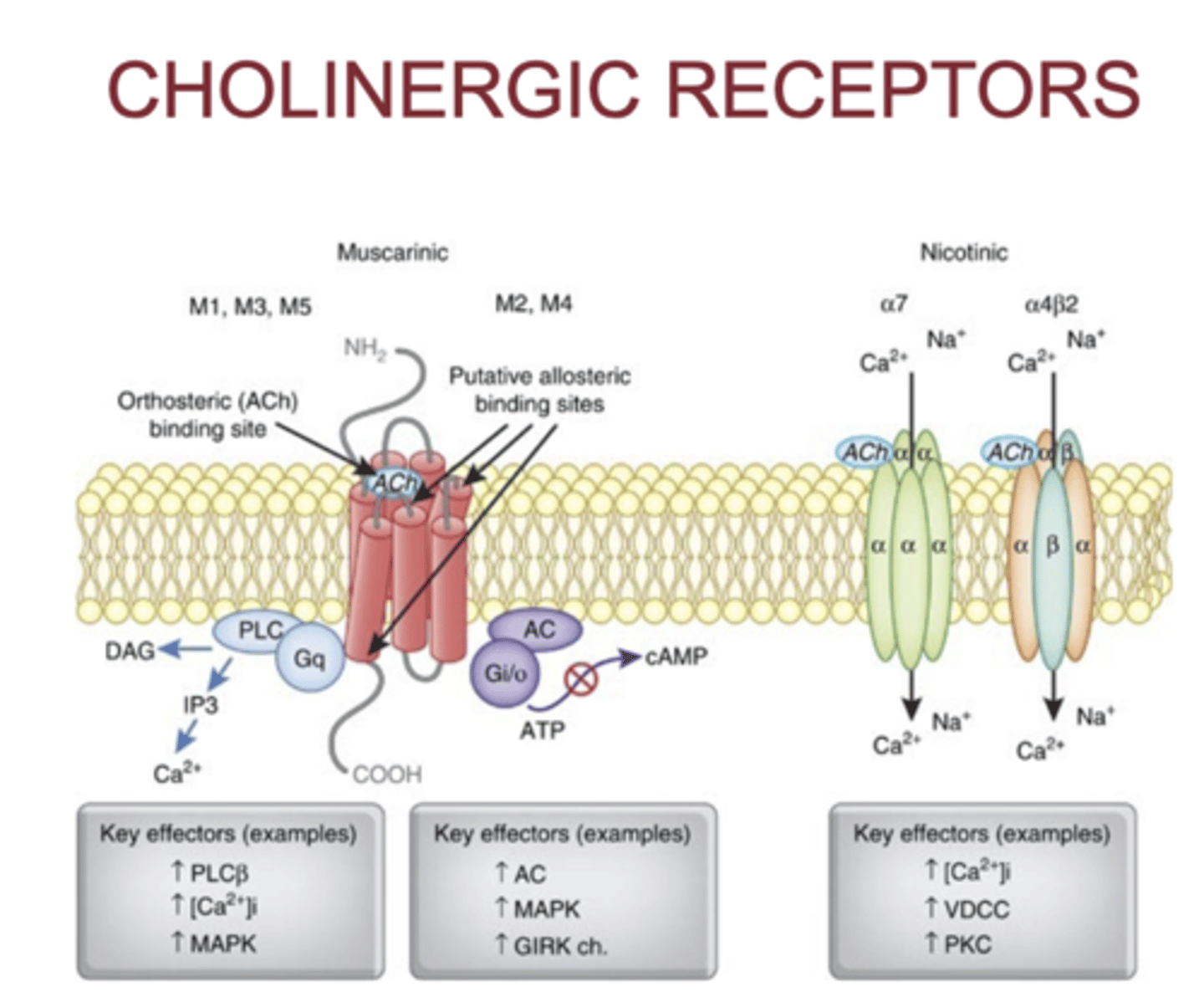
what is the neurotransmitter for the parasympathetic nervous system?
- acetylcholine
what kind of channels are acetylcholine nicotinic receptors?
- ligand gated ion channel
- Acetylcholine binds → the channel opens
- Na⁺ flows in
- K⁺ flows out
- Membrane depolarizes → excitation
- They do NOT use G-proteins.
- They open immediately (fast synaptic transmission).
what kind of channel are Beta adrenergic and acetylcholine muscarinic receptors?
- g coupled protein receptors
- ALL ADRENERGIC ARE G PROTEIN RECEPTORS
- sympathetic ganglion run down the spinal column from the brain stem and are adjacent to each part of the spinal cord

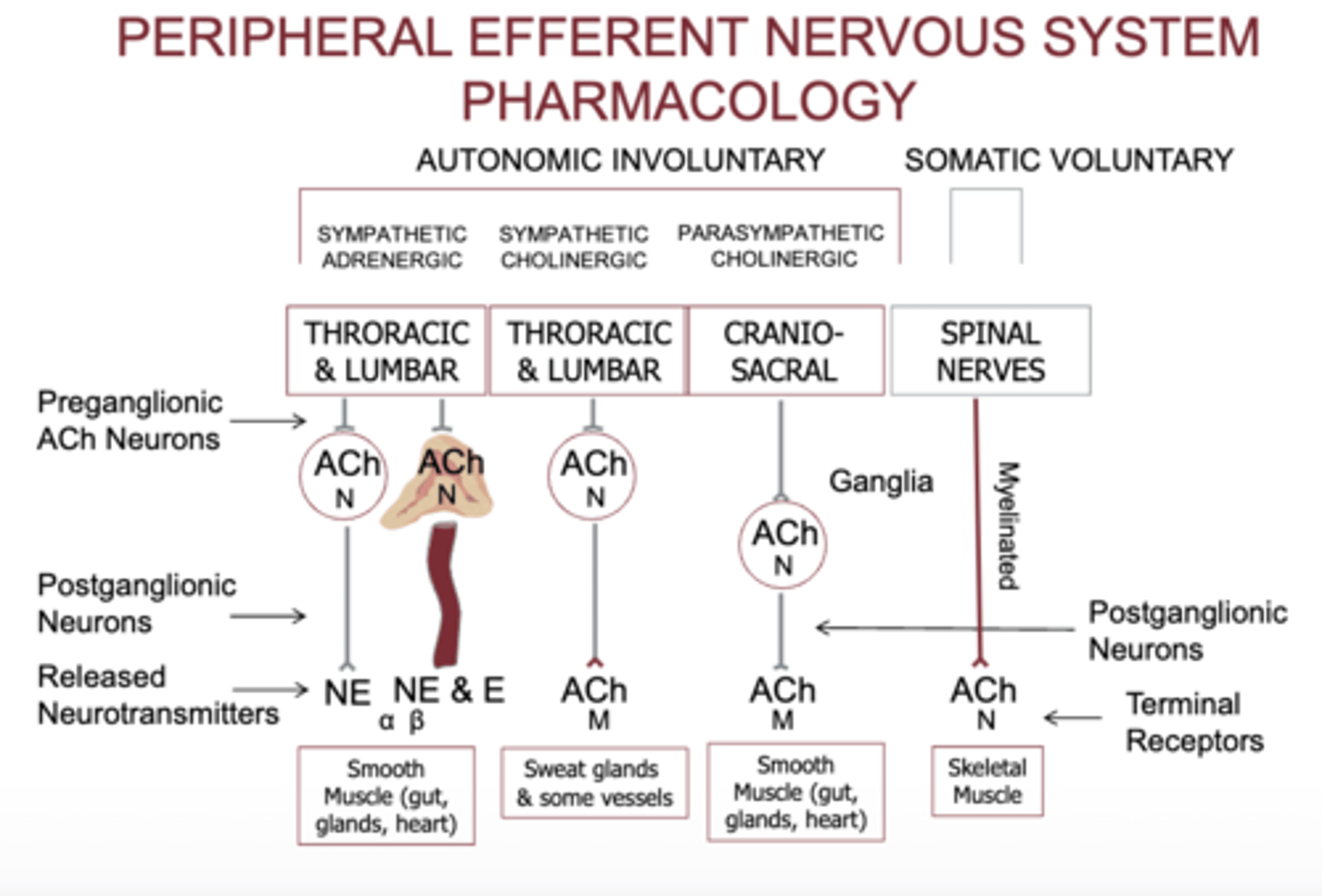
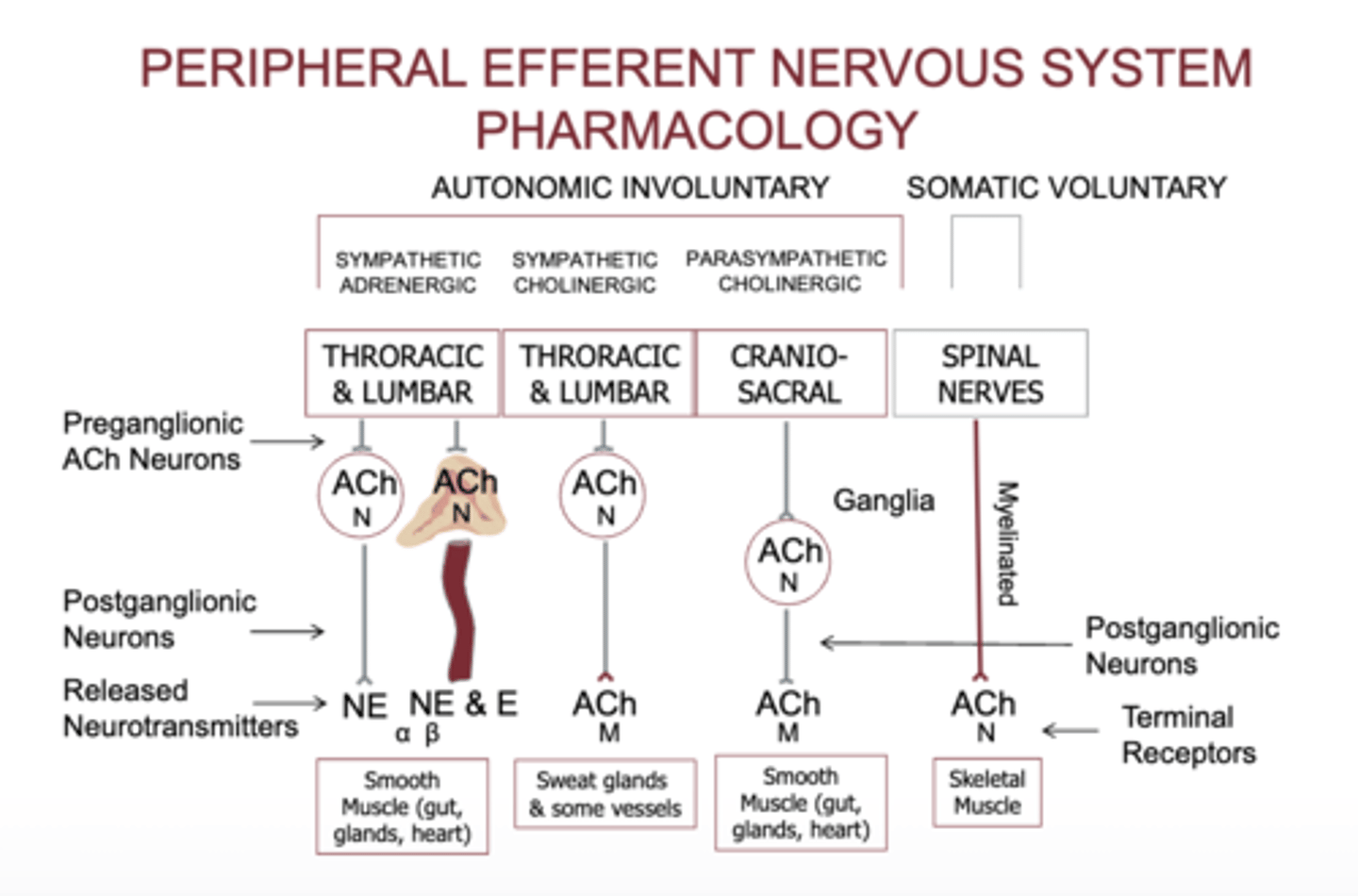
peripheral efferent nervous system pharmacology
1. SYMPATHETIC ADRENERGIC SYSTEM (most organs)
Preganglionic neuron
Comes from thoracic & lumbar spine (T1–L2)
Releases ACh
Receptor on ganglion = Nicotinic (N) → ion channel
Postganglionic neuron
Releases NE (norepinephrine) or E (epinephrine)
Target organ receptors
α or β adrenergic receptors (all are GPCRs)
What it controls
Smooth muscle
Cardiac muscle
Glands
Blood vessels
2. SYMPATHETIC CHOLINERGIC SYSTEM (sweat glands)
This is the exception to the “sympathetic uses NE” rule.
Preganglionic
ACh → Nicotinic
Postganglionic
Also releases ACh (instead of NE)
Target organ receptors
Muscarinic (M) receptors
What it controls
Sweat glands (eccrine)
Some blood vessels in skeletal muscle
3. PARASYMPATHETIC SYSTEM
Preganglionic neuron
From cranial nerves + sacral spine (S2–S4)
Releases ACh → Nicotinic (N)
Postganglionic neuron
Releases ACh again
Target organ receptors
Muscarinic receptors (M)
Controls
Smooth muscle (gut, airways, bladder)
Glands (saliva, tears, mucus)
Heart (slows HR)
4. SOMATIC SYSTEM (voluntary movement)
No ganglia — one long motor neuron.
Neuron releases
ACh
Target receptor
Nicotinic muscle receptor (Nm) → ion channel
Controls
Skeletal muscles
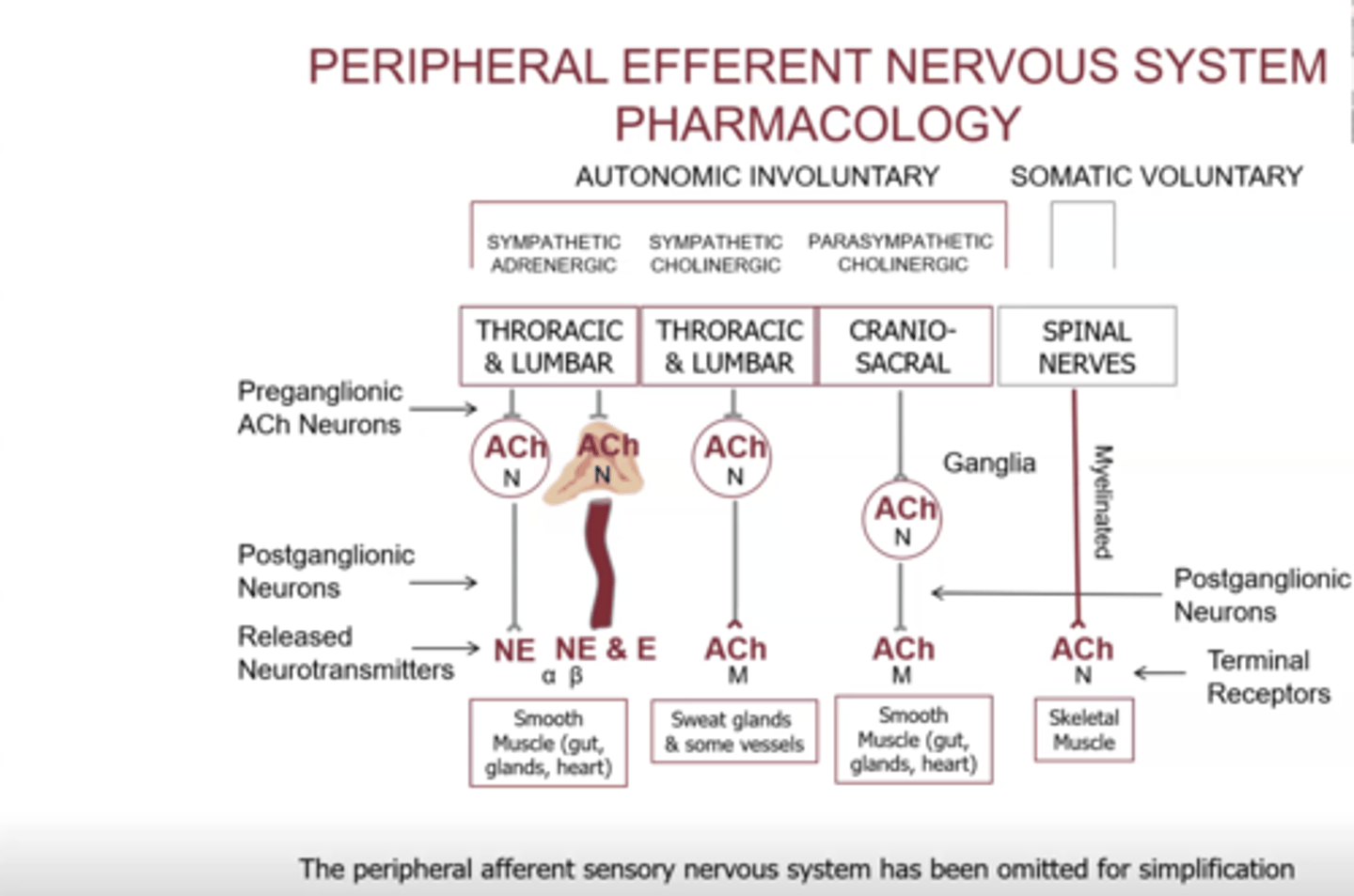
what is autonomic involuntary vs somatic voluntary?
- autonomic involuntary: we do not have control, non myelinated
- somatic voluntary: we do have control, myelinated
why is somatic voluntary myelinated?
- has to travel far distance
- long extension cord
why is autonomic involuntary unmyelinated?
- does not have to travel far
- goes down spinal cord and travels to adjacent area
- multiple extension cords put together
what happens in the sympathetic cholinergic system?
- thoracic and lumbar region have preganglionic fibers that synapse with nicotinic receptor with acetylcholine
- eventually bind to acetylcholine postganglionically to muscarinic receptors, which control gland and vessels
- when stimulated, we begin to sweat due to sympathetic pathway
what is the neurotransmitter for preganglionic receptors in peripheral efferent NS?
- always acetylcholine FOR BOTH sympathetic and parasympathetic
- preganglionic neurotransmitter is always acetylcholine
- second column: adrenal medulla releases both norepinephrine and epinephrine
- all preganglionic receptors are nicotinic
- post ganglionic a variety of receptors, nicotinic not usually involved postganglionically
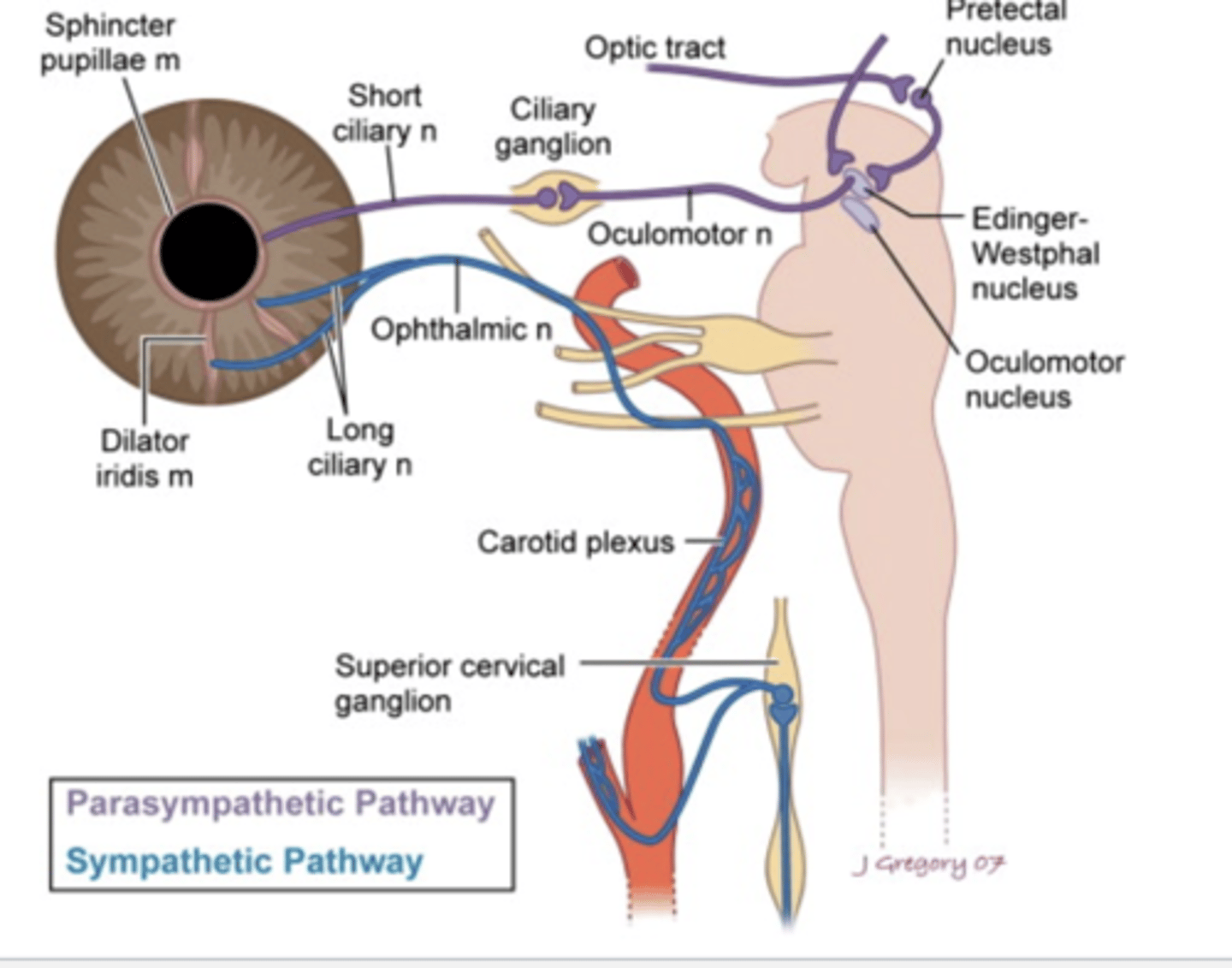
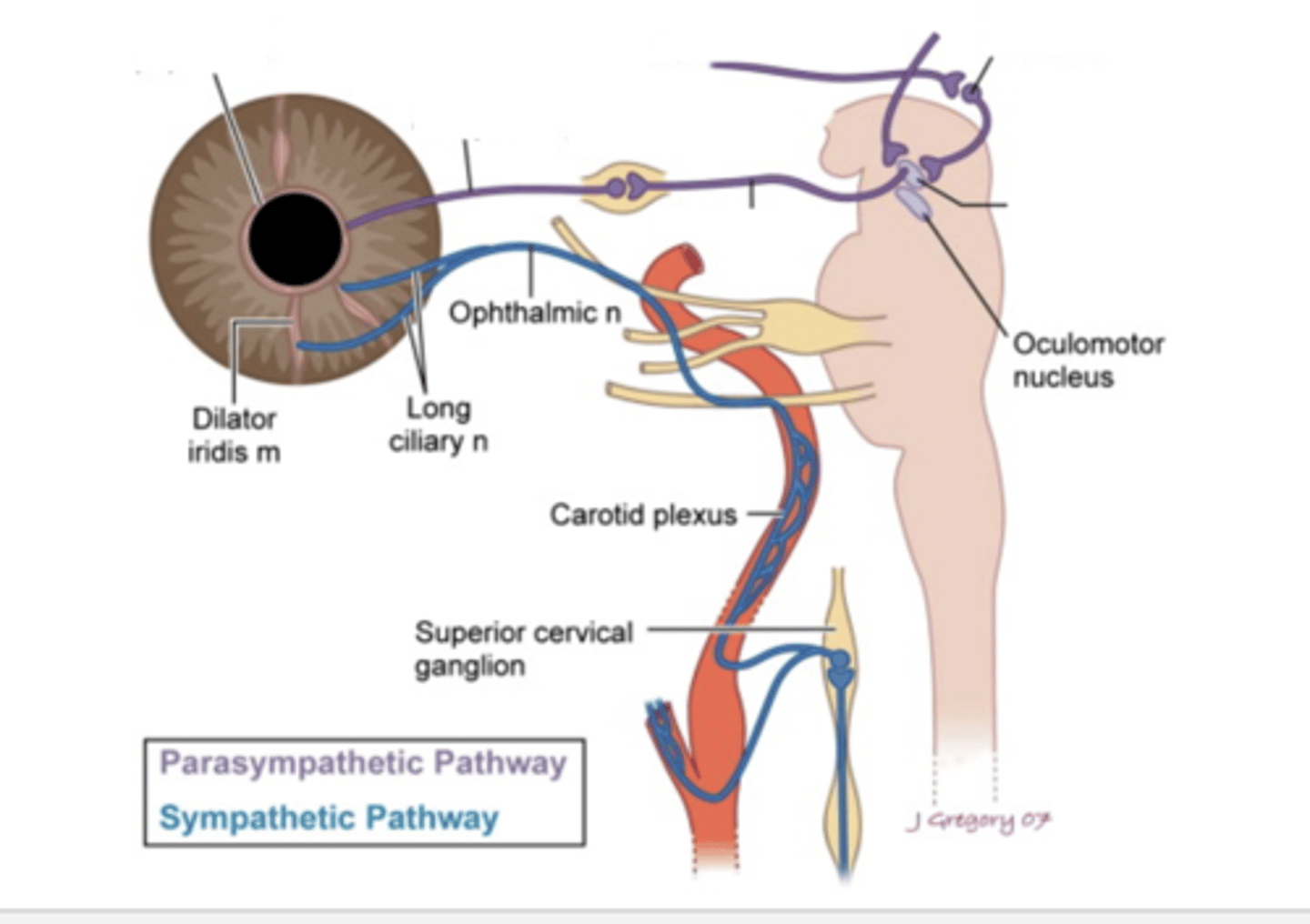
PARASYMPATHETIC PATH
- retina before optic tract, detects light
- in pupillary reflex reaction, optic nerve bypasses LGN, does not synapse there, goes straight to pretectal nucleus
- synapses on both EW nucleus
- travels along CN3 to ciliary ganglion
- short ciliary nerve to iris sphincter
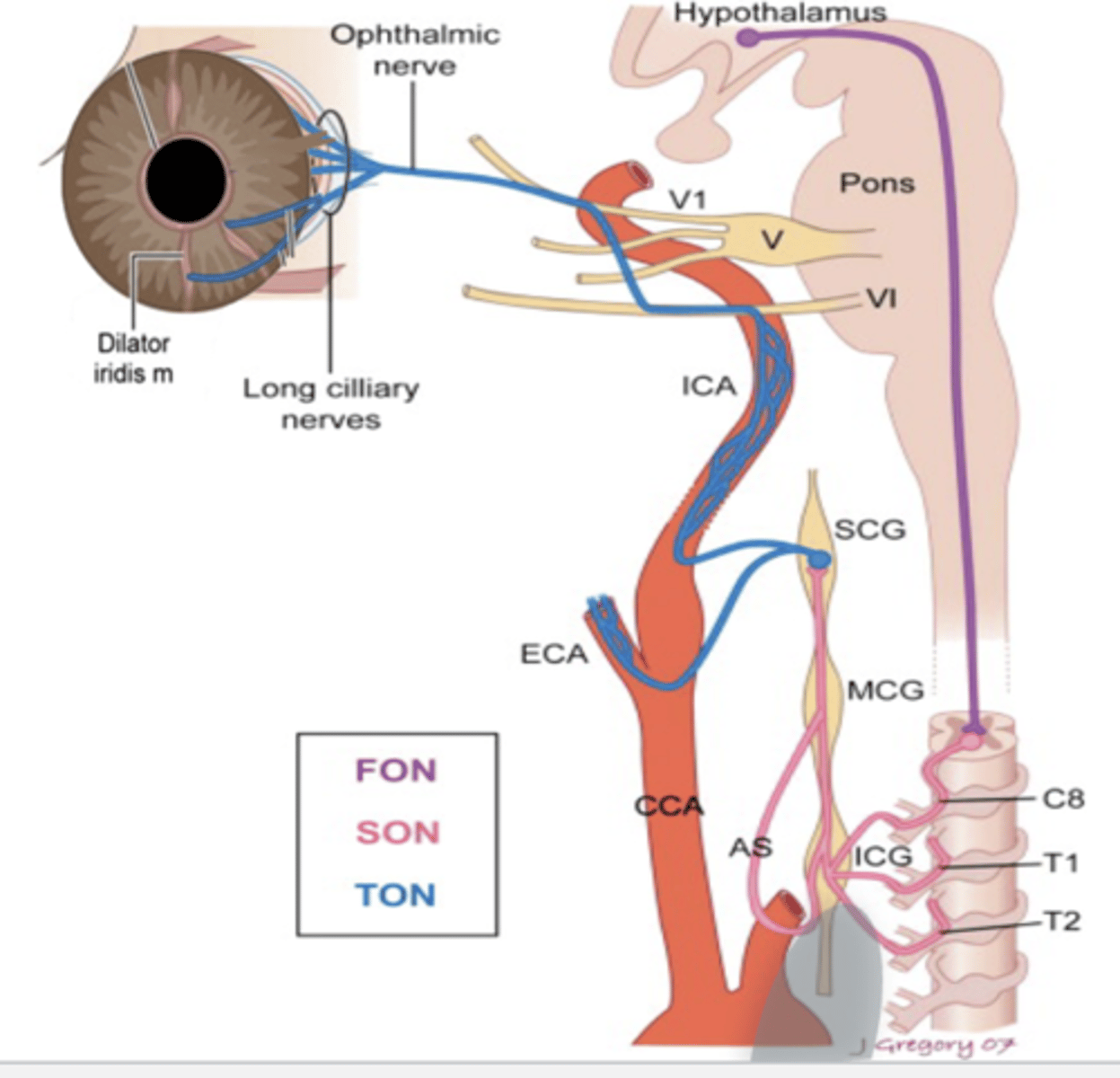
1. hypothalamus senses fact that there is less light available
2. travels down pons, brainstem to first order neuron to C8, T1, T2 (ciliospinal center of Budge Waller, first extension cord)
3. synapses with second order neuron then travels up to inferior cervical ganglion, medial cervical ganglion, and superior cervical ganglion.
(basically goes down the neck/spine, then goes back upwards)
- important area bc adjacent to heart is lung
- if there is tumor of the lung it is along the apex of the second order neuron
- interferes with pupil dilation
- HORNER's
4. synapses with third order neuron, goes up internal carotid artery (could also horner's if there is lesion along ICA, now considered postganglionic)
5. goes to V1, long ciliary nerve, iris dilator, cause mydriasis
6. norepi is only released at the end terminal to bind onto the A1 receptors at the iris dilator for mydriasis
what is the horner triad?
- ptosis
- miosis
- anhidrosis (no sweating)
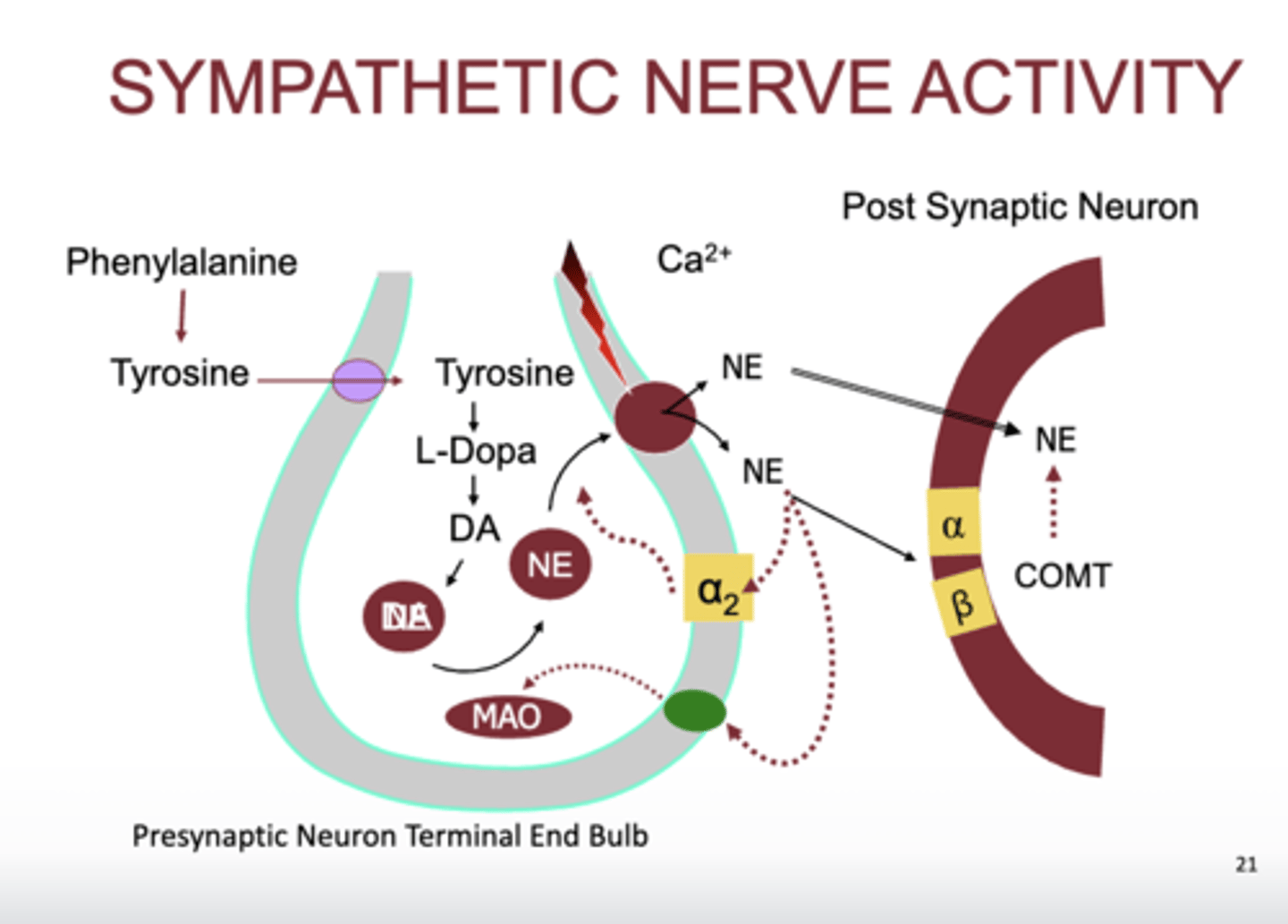
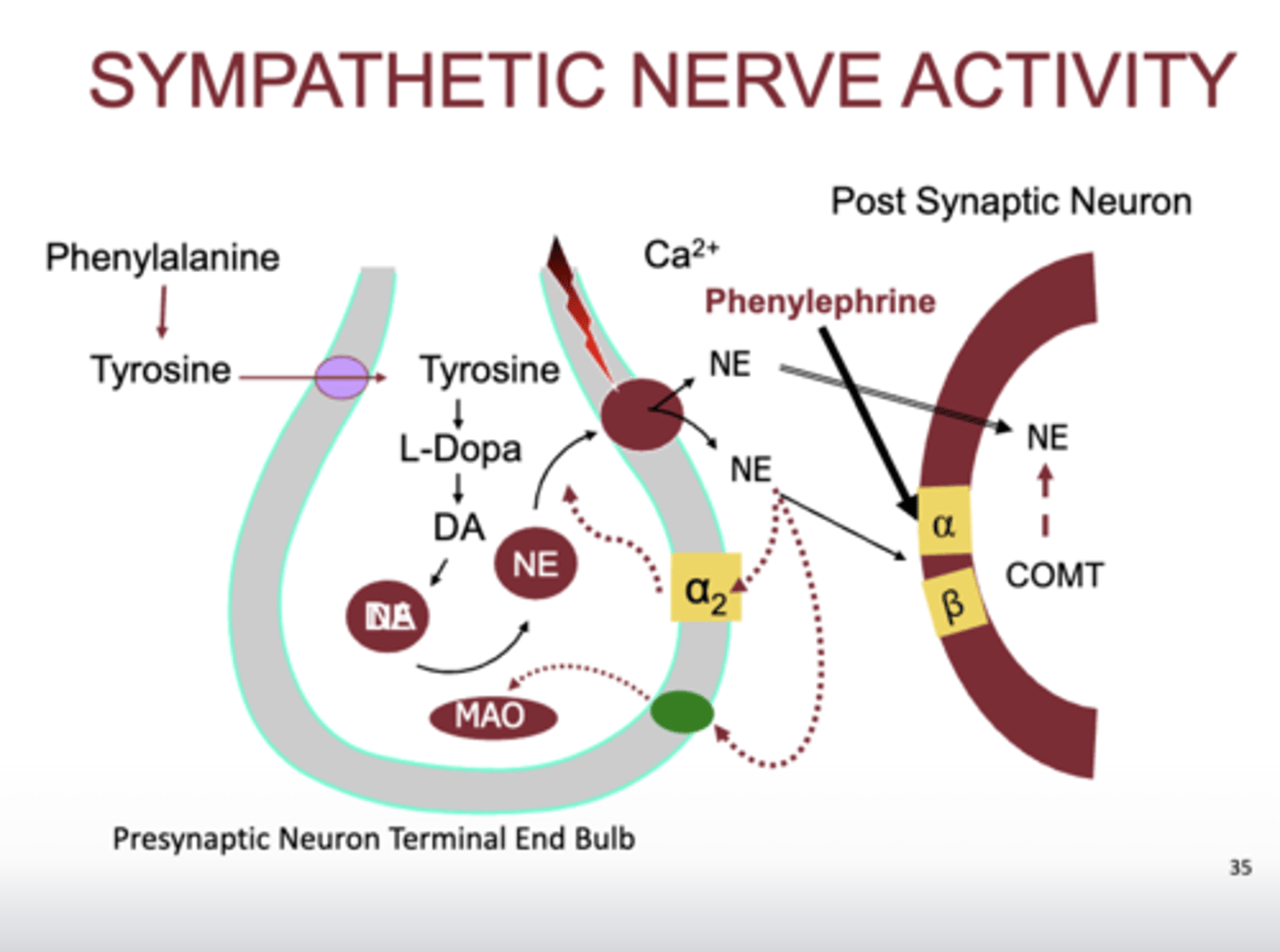
(where a2: presynaptic terminal, space is between synaptic cleft, red is post-synaptic neuron)
- takes place on postgang on sympathetic pathway
- pheylalanine and tyrosine are part of our diet
- tyrosine gets absorbed into the presynaptic terminal and gets converted into L-Dopa
- L-Dopa becomes dopamine
- Dopamine goes into vesicles and gets converted into norepinephrine
- upon depolarization, which causes calcium channels to open and calcium to go into the presynaptic terminal, causes vesicles to release norepinephrine into synaptic cleft
- norepi binds to primarily alpha 1, beta if there is too much
- if there is too much norepi, then it gets metabolized by COMT in the synaptic cleft or on/in the postsynaptic terminal.
- also if there is too much norepi, it binds back to alpha 2 telling presynaptic terminal to release less norepi
- too much norepi will also bind with norepi reuptake receptor, bringing it back in to be metabolized by MAO
- release of norepi is influenced by Ca+, GCPR are on the binding sites for norepi
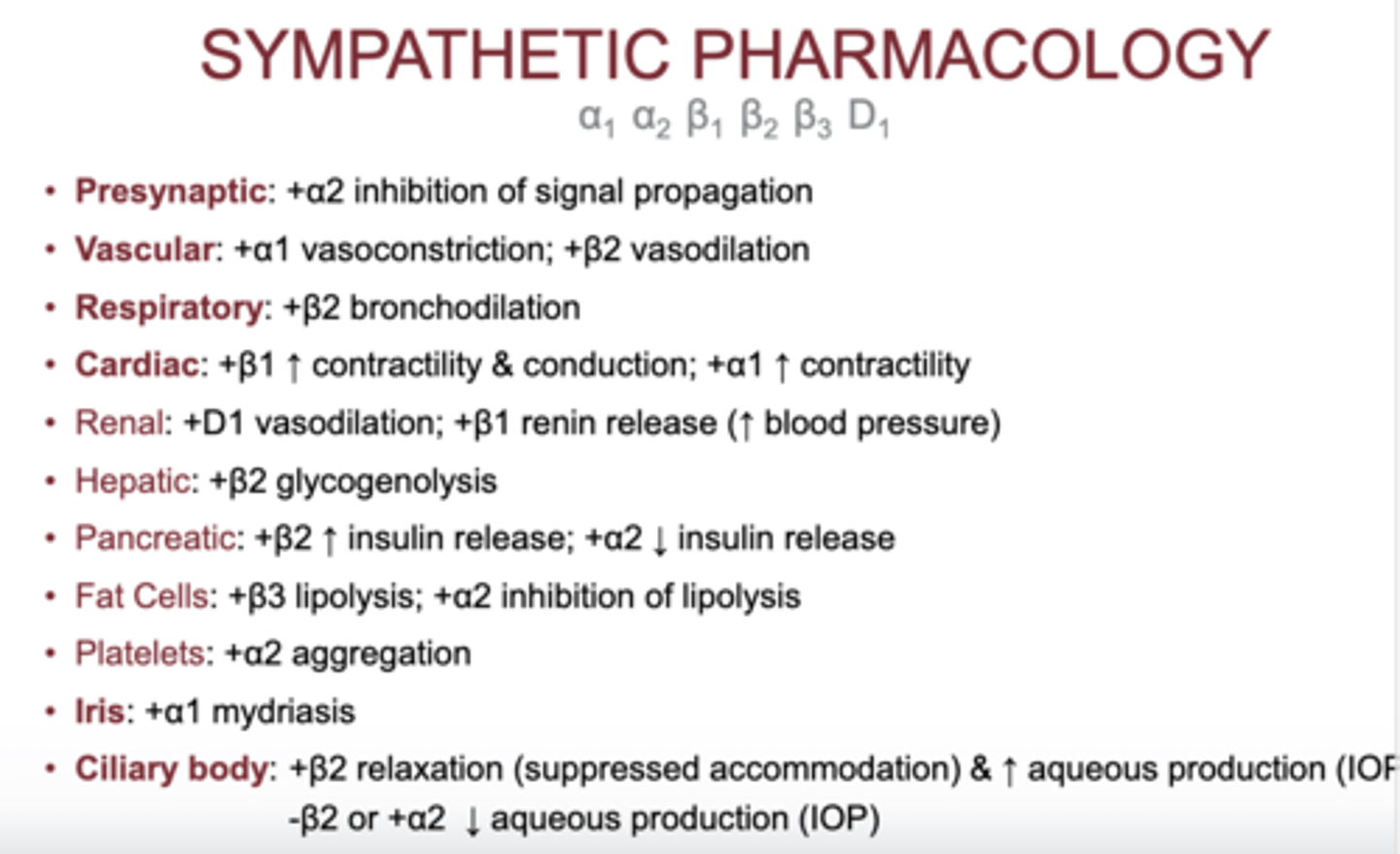
what type of sympathetic receptor is on the presynaptic terminal?
- A2
- stimulation of A2 causes inhibition of signal propagation
- prevents the release of norepinephrine
what type of adrenergic receptors does the vascular system have?
- A1
- B2
what does stimulation of A1 on vascular system cause?
- vasoconstriction
what does stimulation of B2 on vascular system cause?
- vasodilation
what kind of adrenergic receptors does the respiratory system have?
- B2
what does stimulation of B2 on respiratory system cause?
- bronchodilation
what kind of adrenergic receptors does the cardiac system have?
- B1
- A1
what happens when there is stimulation of B1 on the cardiac system?
- increase contractibility and conduction
what happens when there is stimulation of A1 on the cardiac system?
- increase contractibility
what kind of adrenergic receptor does the iris have?
- A1
what does stimulation of A1 of the iris cause?
- mydriasis
what adrenergic receptors does the ciliary body have?
- B2
- A2
- they do opposite things, both located on the non-pigmented ciliary epithelium
what does stimulation and inhibition of B2 on the ciliary body cause?
- stimulation: relaxation, suppress accommodation and increase aqueous production
- inhibition: decrease aqueous production
- when stimulated cAMP causes in increase in aqueous humor
- when blocked, there is no formation of cAMP
what does stimulation of A2 on ciliary body cause?
- decrease aqueous production
- when stimulated, it decreases adenylate cyclase which decreases cAMP, when there is low cAMP, less aqueous production
does epinephrine or norepinephrine bind better to A1?
- NE > E; also stimulated by high dose D
does epinephrine or norepinephrine bind better to A2?
- NE>E
does epinephrine or norepinephrine bind better to B1?
- E = NE; also stimulated by high dose D
does epinephrine or norepinephrine bind better to B2?
- E >> NE
- in respiratory rescue we inject epinepheine not norepinephrine
how does alpha 1 affect the eye?
- when A1 stimulated:
- mydriasis (radial iris muscle contraction)
- increase interpalpebral aperture (Muller's muscle)
how does alpha 2 affect the eye?
- Modulate aqueous generation by the ciliary body
- a2 on the ciliary body, when stimulated, prevents the formation of aqueous
how does beta 2 affect the eye?
- Suppress accommodation
- when blocked, reduces aqueous production
what medications are Sympathomimetic Amines?
- adrenergic agonist
- Phenylephrine
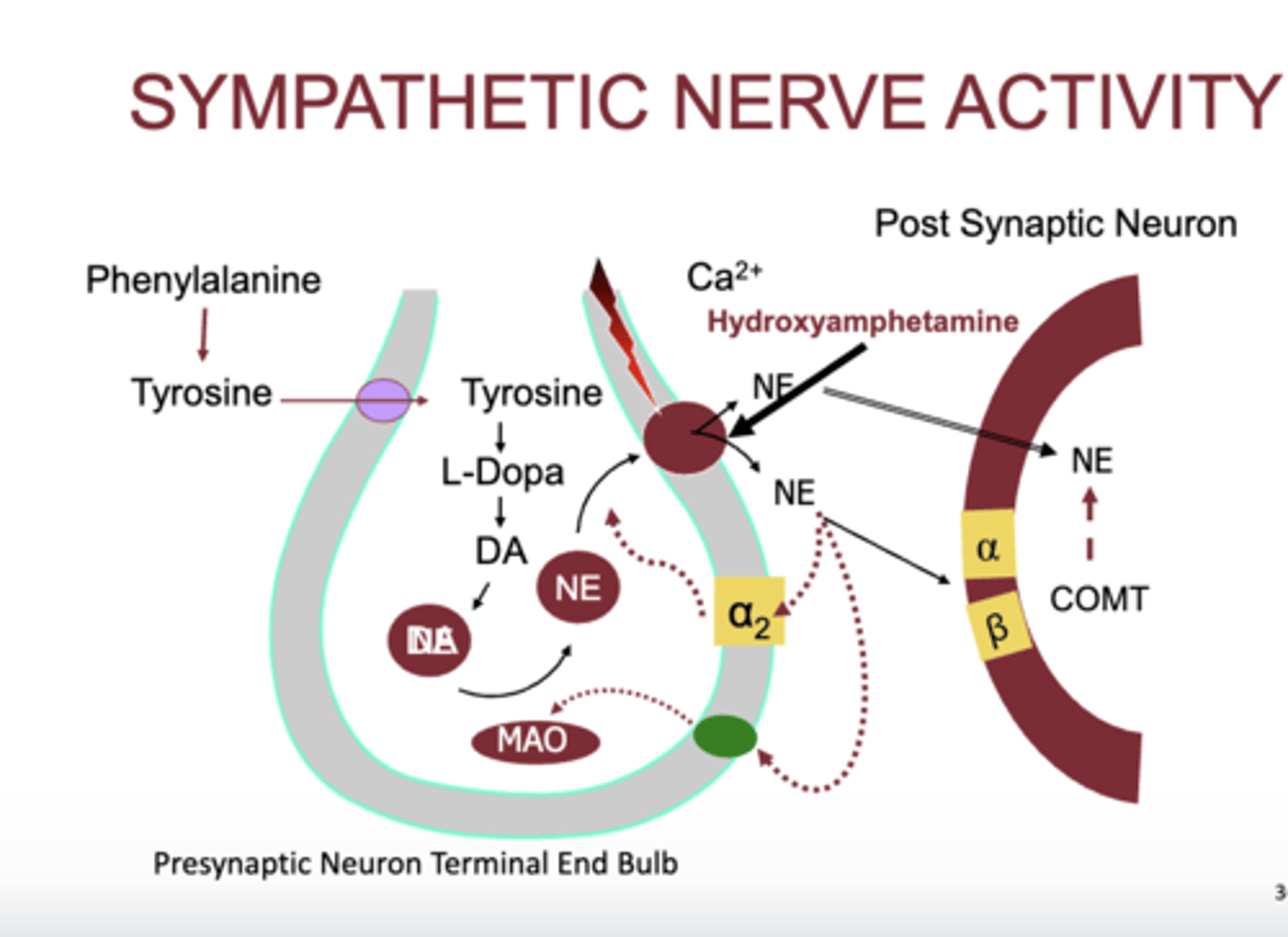
− Hydroxyamphetamine (PAREMYD ® ), combo medication
- hydroxyamphetamine is an indirect alpha agonist
what OCT drops for dry eye relief are adrenergic agonist?
- (Imidazolines, also vasoconstrictors)
- oxymetazoline
- naphazoline
- tetrahydrozoline
- OTC Brimonidine (Lumify)
(problem with these medication is risk of dependence, eye will remain red without it)
(no dependence with OCT lumify)
what is upneeq?
- 0.1% oxymetazoline
- FDA approved drop indicated for the use of acquired blepharoptosis
how does phenylephrine work?
- α1 -receptor selectivity; some indirect effects via norepinephrine release
- contracts iris radial muscles which cause dilation
- beta receptor stimulation occurs at much higher doses
what are the common formulations of phenylephrine?
- 2.5%, 10%, 1%
1% is for horners
when is max mydriasis and how long does it last for with phenylephrine?
- max mydriasis in 45-60 min
- duration 6-7 hours
what would we use phenylephrine for?
− Conjunctival blanching (vasoconstriction)
− Mild accommodation suppression ~2D
− Lid retraction
− IOP reduction (+α2 ), very little amount
what are special uses for phenylephrine?
- Posterior synechiae breakage (10%)
− Pre-LASIK vasoconstriction (10%)
− Inhibition of iris cysts (caused by echothiophate)
− Horner’s evaluation (1%), (lower does has to be made, very sensitive bc no activity being taking place at dilator muscle)
− Distinguish episcleritis from scleritis
what medications are synergist to phenylephrine?
- drug interations
- ENHANCED PHENYLEPHRINE EFFECTS
- MAOIs (selegiline)
- TCADs (blocks reuptake of norepi and seratonin)
- NDRIs
- atropine
what medications are antagonistic to phenylephrine?
- drug interactions
REDUCED EFFECTS OF THE FOLLOWING:
• Methyldopa - alpha-2-agonist cause peripheral vasodilation
• Beta blockers
- selective a1 blockers
what are adverse effects of phenylephrine?
− Photophobia, blur, glare
− Allergic dermatoconjunctivitis
− Rebound miosis & congestion
− Anterior chamber pigment liberation
− Systemic hypertension → reflex bradycardia
what are contraindications to the use of phenylephrine?
− Avoid 10% in neonates/elderly and pregnancy? Category C
− History of CVD or MI, uncontrolled DM1, aneurysm, advanced arteriosclerosis, idiopathic orthostatic hypotension
what is HYDROXYAMPHETAMINE?
− Indirect acting: promotes norepinephrine release from nerve terminals
− Negligible direct α & β receptor stimulation
− Contraction of iris radial muscles
− No accommodation suppression (1% formulation)
- phenylephrine bind directly to A1, give it sympathetic activity, lid to go up, mydriasis, vasoconstriction
why do we dilate a patient?
- standard of care for all new patients
- last to be performed in exam sequence
- bilateral almost under every circumstance
- may be sectoral* i.e. create a keyhole pupil
what would you expect pupil size in patient with tamsulosin?
- miotic
- a1 antagonist
- hydroxyamphetamine causes the release of norepinepheine
- indirect acting agonist
- norepinephrine then binds to A1
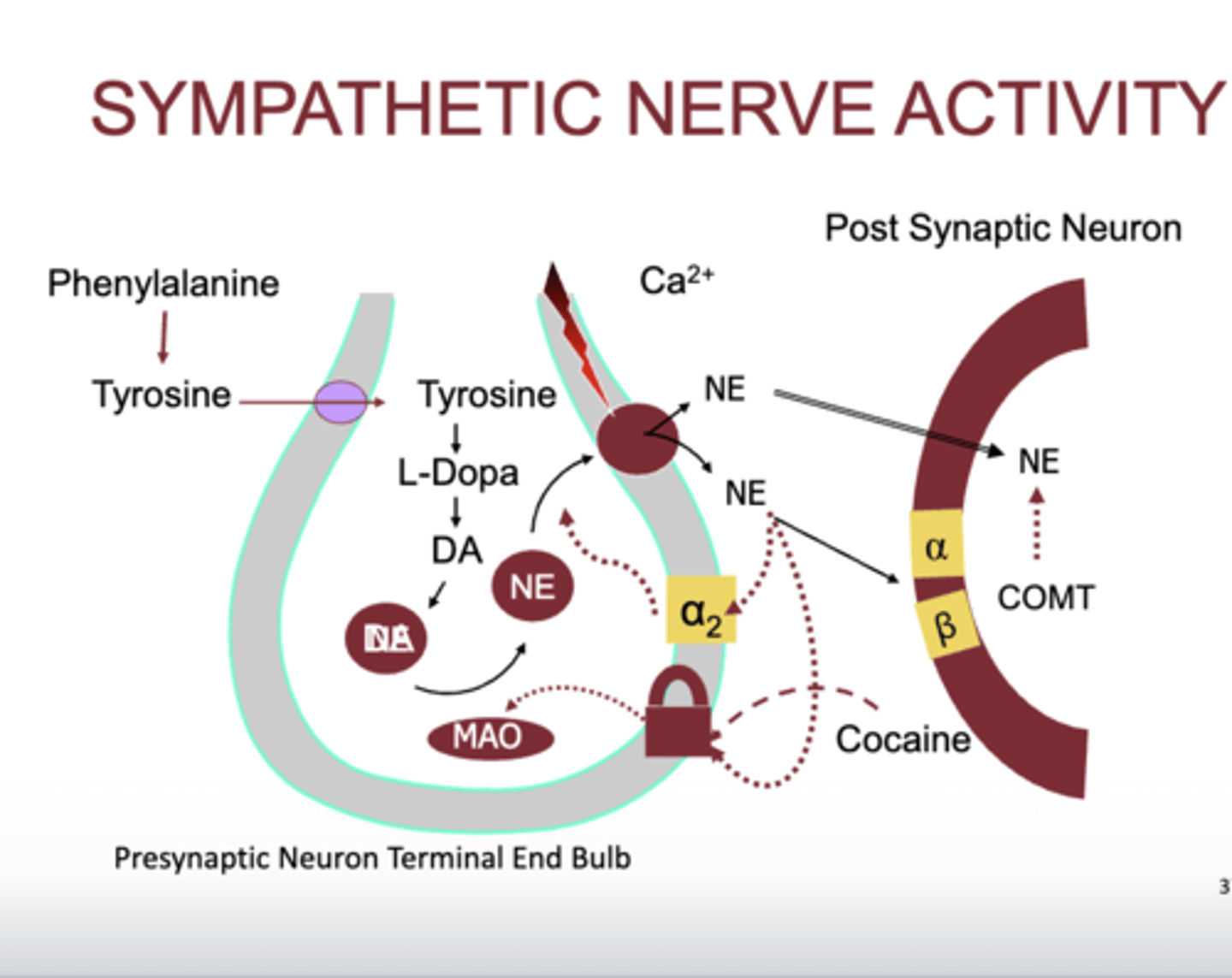
- cocaine blocks the norepinephrine retake receptor
- leads to norepinephine in synaptic cleft
who are poor dilation candidates?
- Homocystinuria & Marfan's syndrome: ectopia lentis risk
- Pregnancy: use Tropicamide;consult OB/GYN
- Pigmentary or exfoliative glaucoma; transient IOP elevation
how do we use dilation to get an angle estimation?
− Gonioscopy > Van Herick > shadow test
− Commonly large in myopes and aphakes
what are contraindications for dilation?
− Iris supported intraocular lens
− Subluxated lens or intraocular lens
− Extremely narrow angle
− Angle closure history without laser peripheral iridotomy (LPI)
what are factors affecting dilation?
reduced sensitivity
- age related miosis
- unstable diabetes
- post op pupils
- posterior synechiae
- dark iris
- pseudoexfoliation syndrome
who would have increase sensitivity to dilation?
- down syndrome

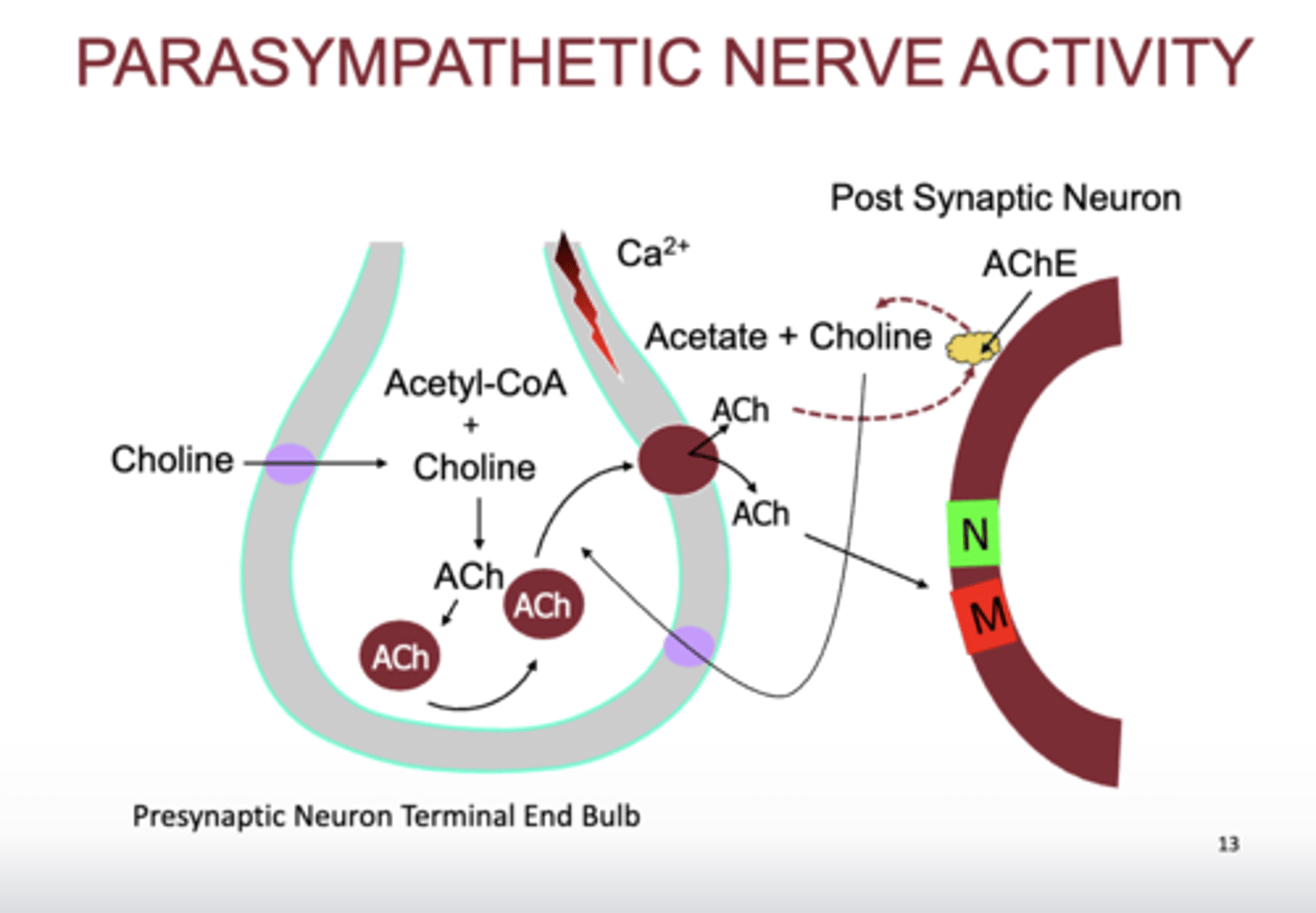
how is acetylcholine metabolized?
- Acetylcholinesterase (AChE) is ubiquitously distributed and surrounds nerve terminals
- Butyrylcholinesterase (BChE) circulates in plasma (same as pseudocholinesterase, which metabolize ester anesthetics)
- main receptors that ACh bind to
- Muscarinic
- Nicotinic
- cholinergic receptor located on preganglionic and somatic voluntary
- muscarinic also found in sweat glands, some vessels, and smooth muscles
what cranial nerves have parasympathetic cholinergic pathway?
- CN3, iris sphincter for miosis
- CN7, connected to lacrimal gland
- 9, 10 as well
- PARASYMPATHETIC PATH
- retina before optic tract, detects light
- in pupillary reflex reaction, optic nerve bypasses LGN, does not synapse there, goes straight to pretectal nucleus and crosses afterwards
- synapses on EW nucleus
- travels along CN3 to ciliary ganglion
- short ciliary nerve to iris sphincter
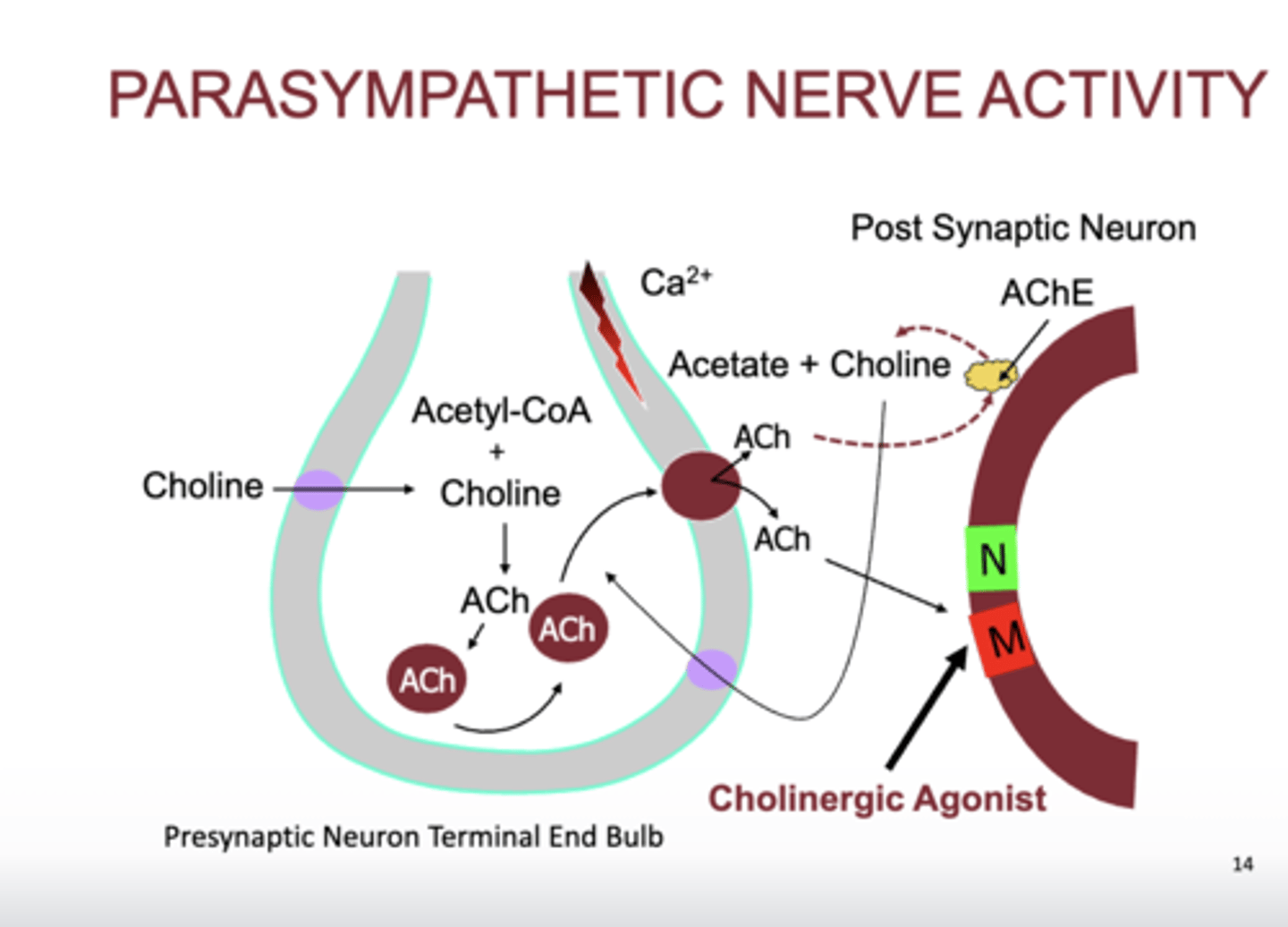
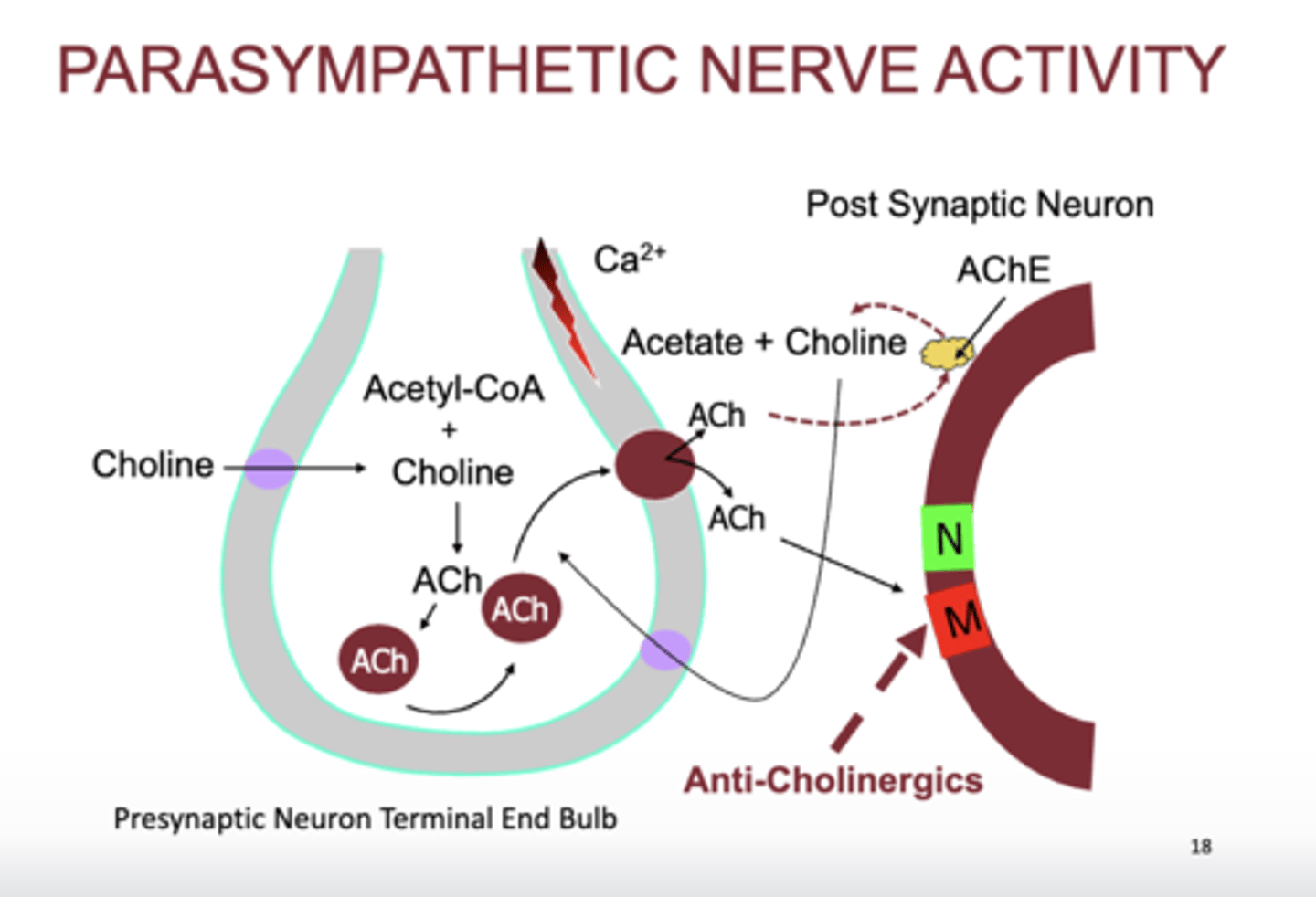
- choline is in our diet
- binds with Acetyl CoA
- forms ACh
- ACh goes into presynaptic vesicles
- depolarization occurs, Ca rushes in, tells ACh to be released
- binds to nicotinic or muscarinic
- it is broken down by AChE
- Choline is brought back into presynaptic terminal by choline reuptake transporter
-cholinergic agonist cause parasympathetic activity
- these only bind to the MUSCARINIC RECEPTORS not nicotinic, no skeletal muscles are affected
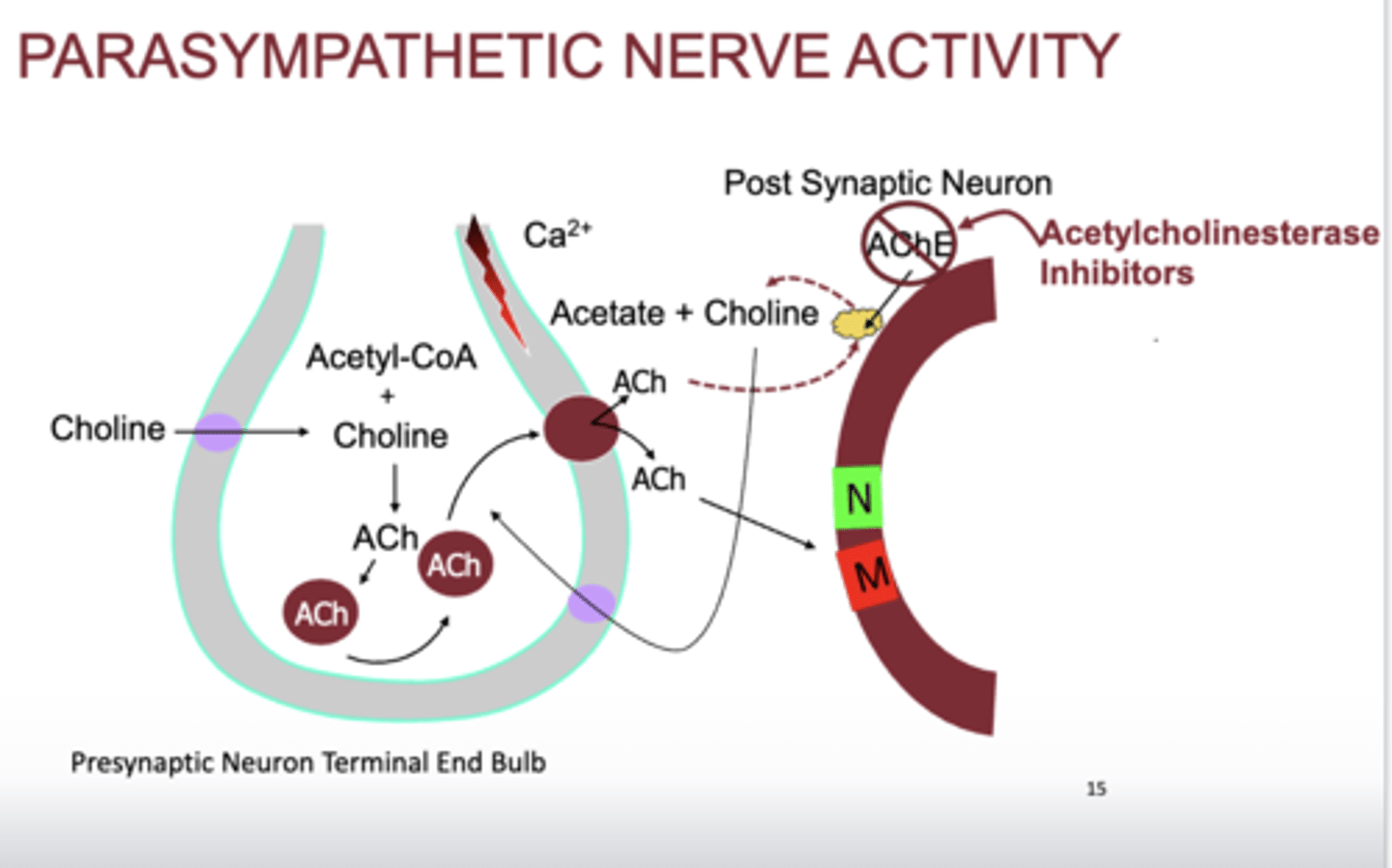
- AChE inhibitors cause parasympathetic activity
- prevent breakdown of ACh
- edophonium
- pyridostigmine
- neostigmine
- donezapil
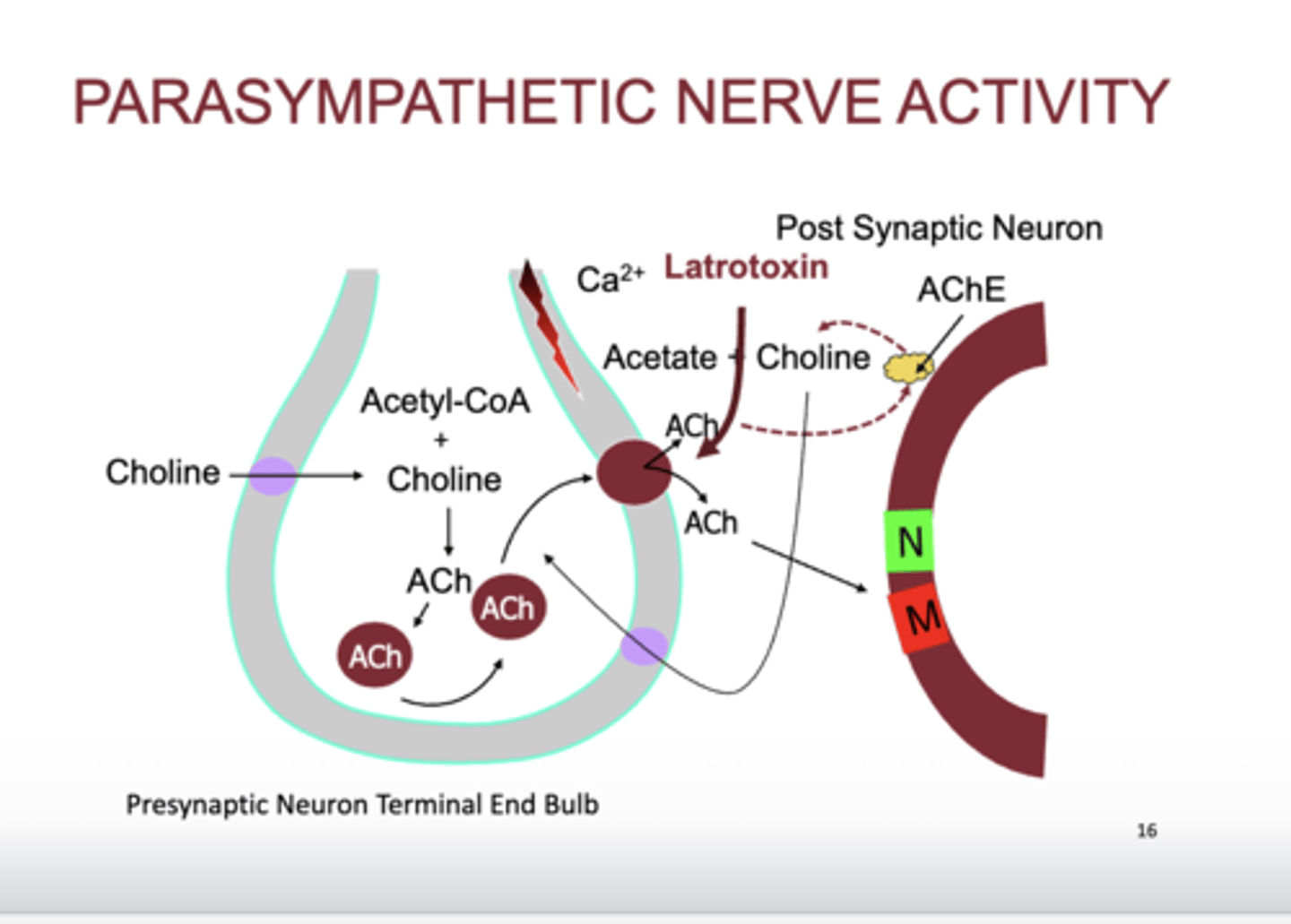
- Latrotoxin causes us to release all of ACh at the same time, parasympathetic activity
- causes cramping due to ACh binding onto the nicotinic receptors on skeletal muscles and muscarinic on smooth muscles, black widow venom
- similary to hydroamphetamine (sympathetic)
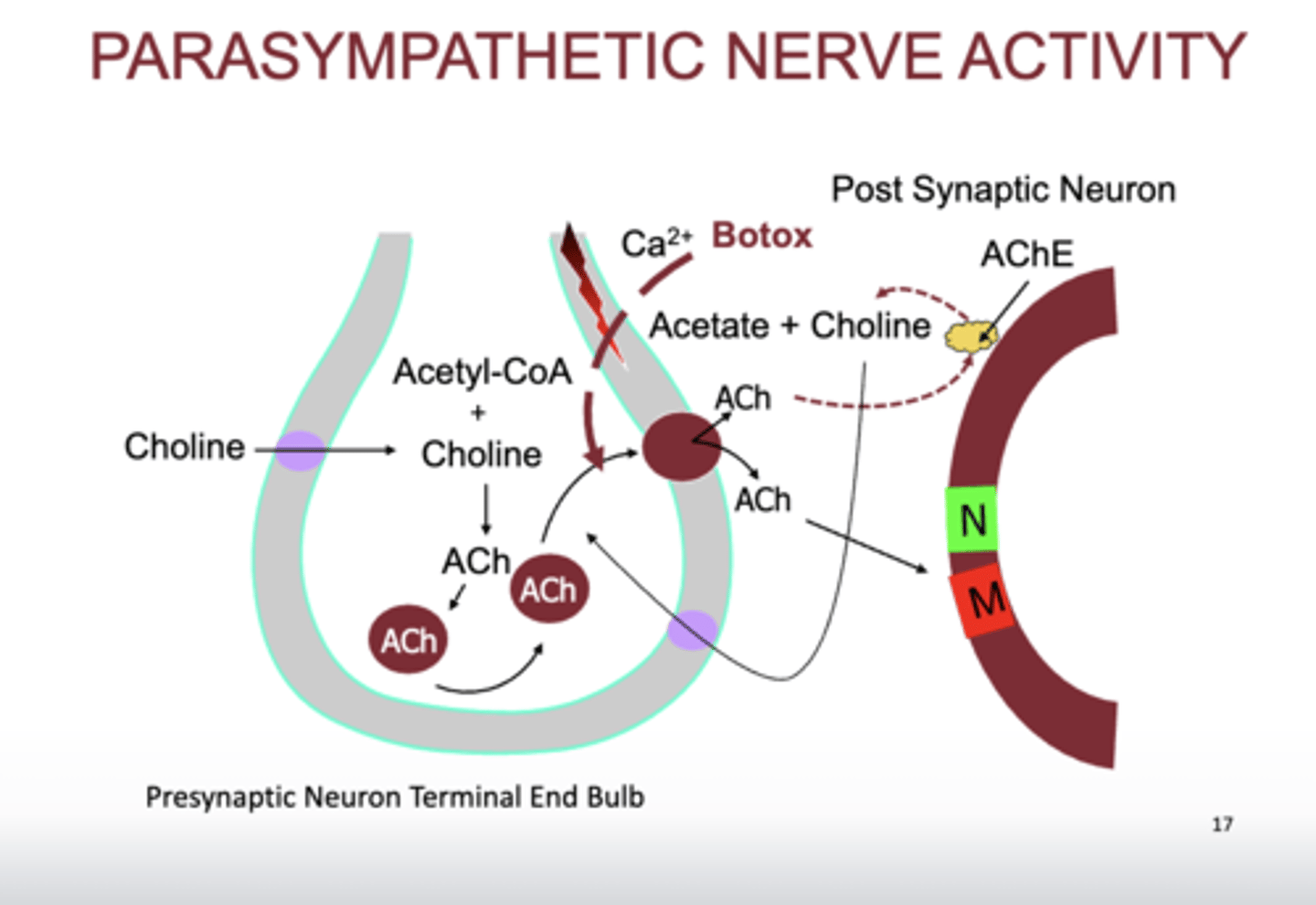
- botox prevent release of ACh
- less ACh, less parasympathetic activity
- anticholinergics inhibit muscarinic
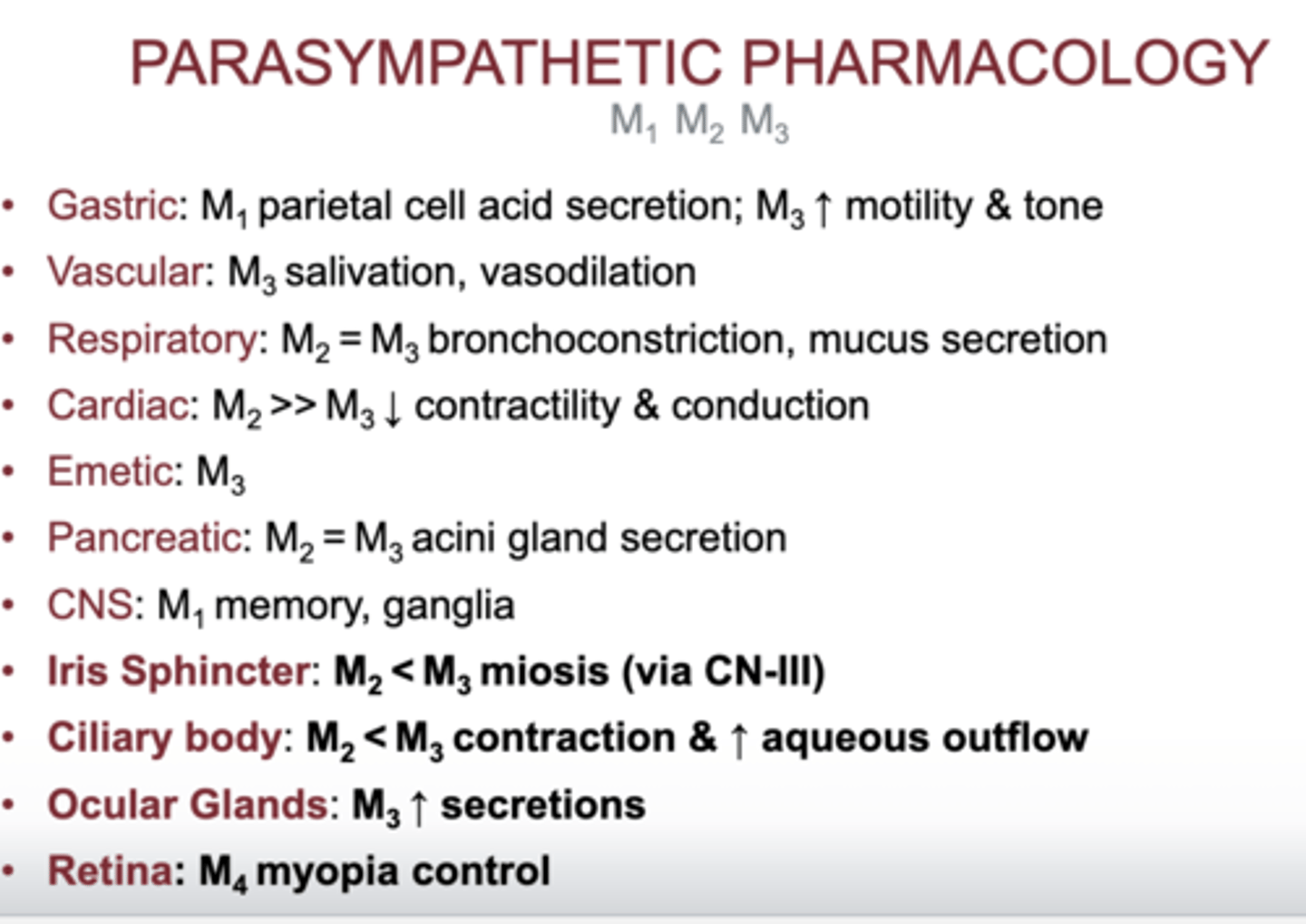
what kind of cholinergic receptors does the iris sphincter have?
- M2< M3 mioisis
what kind of cholinergic receptor does the ciliary body have?
- M2< M3 contraction and aqueous outflow
- stimulation causes contraction of ciliary body, therefor activates accommodation and miosis
- indirectly, it causes aqueous outflow bc contraction of the ciliary body opens up the TM
what kind of cholinergic receptors does the ocular glands have?
- M3 increase secretion
- cholinergic agonist will cause an increase in lacrimation
what kind of cholinergic receptors does the retina have?
- M4 myopia control
how does atropine help in amblyopia?
- used to impair vision in the normal eye to force the use and development of the amblyopic eye
• May require higher dosing in dark eyes
how does atropine help with anterior uveitis?
- inhibits ciliary body spasm, lens to iris position, vessel permeability (blood aqueous barrier)
- less pain, photophobia
- break synechiae
- improve blood aqueous barrier