Communicate the Army Health System (AHS) Planning
1/125
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
126 Terms
What is AHS Planning?
the focus of the medical planning process should be to quickly develop a flexible, tactically sound, fully integrated and synchronized plan that supports the tactical commander's mission
AHS Operational Framework
another example of AHS Operational Framework
United States Army Roles of Care
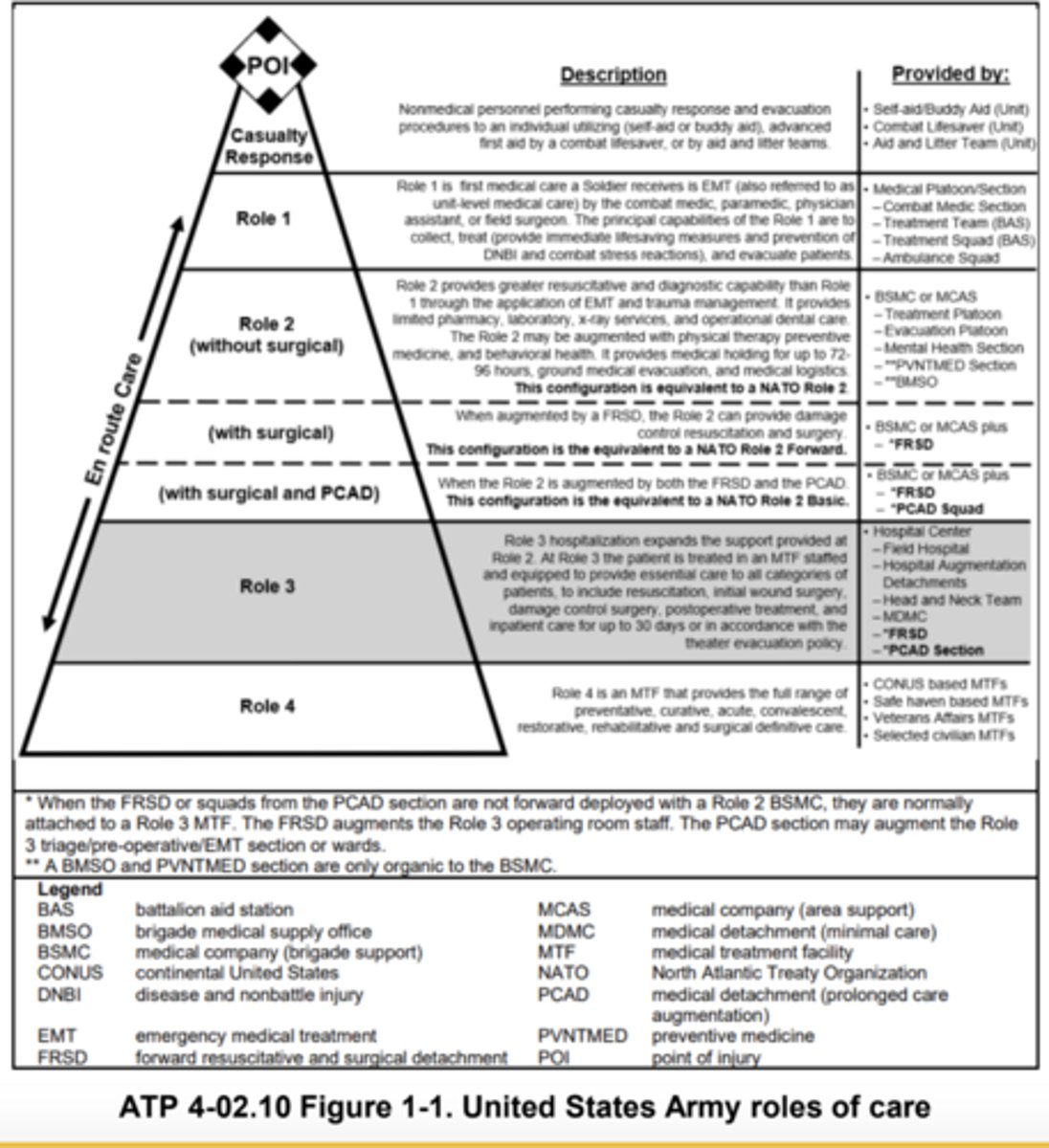
Role of the Medical Planner (MEDO)
70B - field medical assistant
- conducts timely and comprehensive planning to determine medical requirements before, during, and after all phases of operations
- conducts mission analysis to determine the allocation of AHS resources and planned locations of medical assets
- integrates the medical plans with the tactical plans
- provides commanders with a sketch of medical capabilities in their area of operations and in the operational environment
Medical platoon leader as a staff officer:
- the medical platoon leader is a part of the Commander's special staff
- the platoon leader writes the medical portion of the battalion operations order
- the platoon leader then uses the same order to issue to the platoon during subsequent TLPs
Principles of the AHS
Conformity
Proximity
Flexibility
Mobility
Continuity
Control
Conformity
- ensures that a comprehensive AHS support plan conforms to operation order (FM 4-02, 1-24)
- medical assets are arrayed on the battlefield properly
- AHS planners must be involved early in the planning process to ensure that we continue to provide AHS support in support of the Army's strategic roles of shape OEs, prevent conflict, prevail in large-scale ground combat, consolidate gains and once the plan is established it must. be rehearsed with the forces it supports
Proximity
- provides medical support at the right time and place
- medical resources employed as far forward as possible, without impeding ongoing operations
Flexibility
- recommend correcting: being prepared to, and empowered to, shift AHS resources to meet changing requirements (aTP 4-02, 1-26)
- Changes in plans or operations make flexibility in AHS support planning and execution essential
Mobility
- AHS assets remain in supporting distance to support maneuvering forces
- the mobility, survivability (such as armor plating), and sustainability of AHS units organic to maneuver elements must be equal to the forces being supported
Continuity
- patient moves through progressive, phased roles of care
- each soldier receives the care required to optimize patient outcome
- the army's future OE is likely to be complex and challenging and widely differs from previous conflicts. Operational factors will require the provision of medical care to a wide range of combat and noncombat casualties for prolonged periods that exceed current evacuation planning factors (FM 4-02, 1-30)
Control
- resources are efficiently employed
- ensure scope and quality of medical treatment meets professional standards and policies
- AHS support operations require synchronization to ensure the complex interrelationships and interoperability of all medical assets remain in balance to optimize the effective functioning of the entire system (FM 4-02, 1-31)
The 10 medical functions (image):
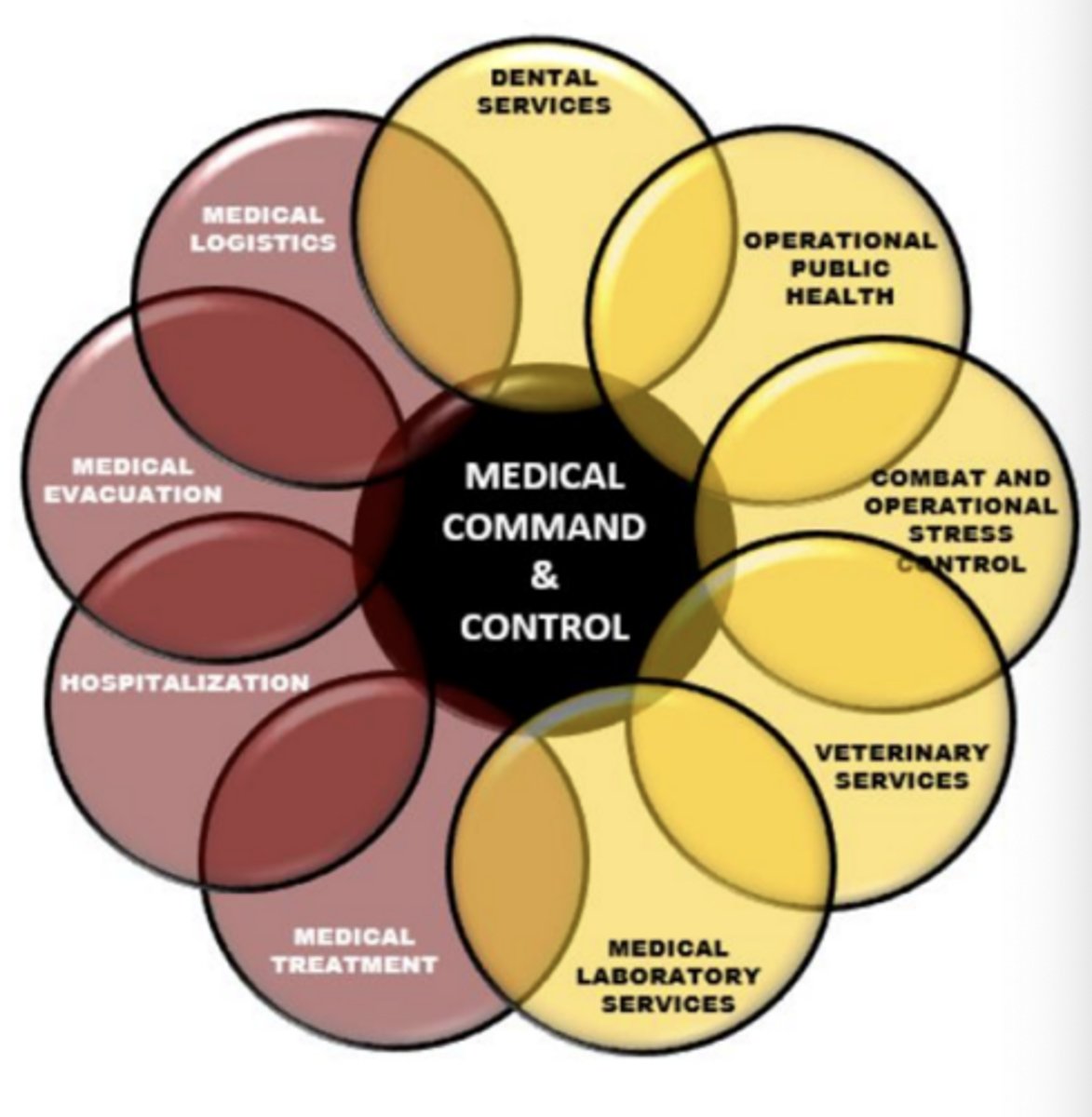
what are the 10 medical functions?
medical command and control
dental services
operational public health
combat and operational stress control
veterinary services
medical laboratory services
-
medical treatment
hospitalization
medical evacuation
medical logistics
The AHS principles apply across all 10 medical functions, synchronized through medical Command and Control (C2) through close coordination and synchronization of all ______ ______ ________
deployed medical assets
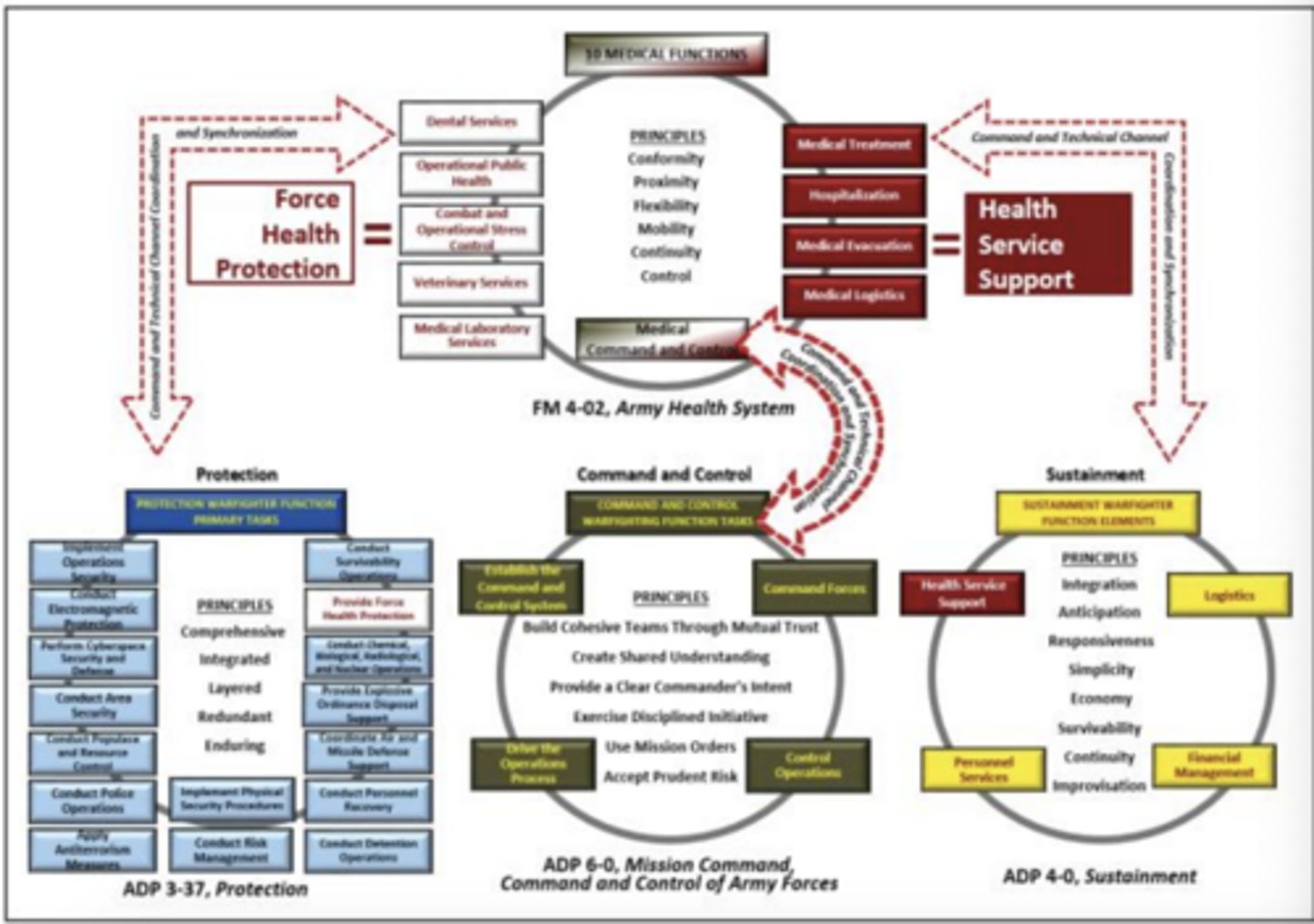
Warfighting Function Linkage image:
Principles of Planning
- understanding a situation, envisioning a desired future condition, and laying out effective ways to bring that future about
- results in a plan or order that communicates the commander's vision
- directs action to synchronize forces in time, space, and purpose for achieving objectives and accomplishing missions
- apply critical and creative thinking to understand, visualize, and describe unfamiliar problems and approaches to solving them
Medical Operational Planning Factors:
1) Be there - maintain a medical presence with the soldier
2) maintain the health of the command
3) save lives
4) clear the battlefield of casualties
5) provide state of the art medical care
6) ensure early return to duty
understanding commander's intent
commander's intent describes what constitutes success for the mission including the:
1) Operation's purpose
2) Key tasks
3) Conditions that define the end state
understanding the commander's intent enables the medical planner to do what?
plan AHS support that is synchronized with the scheme of maneuver and flexible enough to adapt
medical planners may not always receive the:
commander's medical guidance
commander's intent describes what constitutes success for the mission including _____, ______, and ______ ?
operation's purpose
key tasks
conditions that define the end state
what are the six principles of the AHS?
conformity
proximity
flexibility
mobility
continuity
control
What does MDMP stand for?
Military Decision-Making Process
MDMP overview
MDMP is an iterative planning methodology to understand the situation and mission, develop a course of action, and produce an operation plan or order.
Helps leaders apply thoroughness, clarity, sound judgement, logic, and professional knowledge so they understand situations, develop options to solve problems, and reach decisions
steps in the MDMP:
1) Receipt of mission
(WARNORD 1)
2) Mission analysis
(WARNORD 2)
3) COA development
4) COA analysis war-game
5) COA comparison
6) COA approval
(WARNORD 3)
7) Orders production dissemination, and transition
Receipt of Mission:
commanders initiate the MDMP upon receipt or in anticipation of a mission.
This step alerts all participants of the pending planning requirements, enabling them to determine the amount of time available for planning and preparation.
how many steps does receipt of mission consist of?
6 steps
Mission analysis:
Commanders (supported by their staffs) gather, analyze, and synthesize information to orient themselves on the current conditions of the OE.
They conduct mission analysis to better understand the situation and problem, and identify what the command must accomplish, when and where it must be done, and most importantly why.
how many steps does mission analysis consist of?
18 steps
COA development:
broad potential solution to an identified problem.
generates options for subsequent analysis and comparison that satisfy the commander's intent and planning guidance.
planners use the problem statement, mission statement, commander's intent, planning guidance, and various knowledge products developed during mission analysis when creating COAs.
COA development consists of how many steps?
8 steps
COA Analysis War-Game:
enables commanders and staffs to identify difficulties or coordination problem. It helps them think through the tentative plan.
Appraises the quality of each COA, but it also uncovers potential execution problems, decisions, and contingencies
influences how commanders and staffs understand a problem and may require the planning process to restart.
how many steps are in COA analysis?
eight sub-steps
COA Comparison:
objective process to evaluate COAs independently and against set evaluation criteria approved by the commander and staff.
Identifies the strengths and weaknesses of COAs, enable selecting a COA with the highest probability of success, and further developing it in an OPLAN or OPORD.
How many steps does COA comparison consist of?
3 steps
COA Approval:
after the decision briefing, the commander selects the COA to best accomplish the mission
if the commander rejects all COAs. the staff starts COA development again
If the commander modifies a proposed COA or gives the staff an entirely different one, the staff then war-games the new COA.
Publish OPORD:
The staff prepares the order or plan by turning the selected COA into a clear, concise concept of operations and the required supporting information.
the COA statement becomes the concept of operations for the plan.
The COA sketch becomes the basis for the operation overlay.
Medical Planner's Role in MDMP:
1) receipt of mission
- receive the mission
2) mission analysis
- conduct medical estimate (mission analysis)
3) COA development
- development of medical plan for each course of action
4) COA analysis (war-game)
- evaluate
5) COA Comparison
- compare each COA
6) COA approval
- recommend COA most supportable
7) orders production dissemination, and transition
- publish medical appendix to OPORD (Appendix 3 to Annex F)
what are the secen steps of Military Decision-Making Process?
1) Receive the mission
2) mission analysis
3) COA development
4) COA analysis
5) COA comparison
6) COA approval
7) Publish OPORD
AHS Support Estimate:
(also referred to as the Medical Estimate) a continuous process which systematically examines all aspects of operations. It produces the necessary task organization for decentralized execution and flexible medical support on the battlefield
Purpose of the AHS Support Estimate:
- forms the basis for the subsequent AHS support plan
- all possibilities that could affect the successful support of an operation must be considered
- contains facts and assumptions based on the staff's experience
- planners should tailor their estimates according to their mission needs
requirements determined by estimates:
estimates via number distributed in time and space (areas of patient density, possible MASCAL areas, etc.)
determine requirements for each Medical Functional Area:
- medical treatment
- evacuation and medical regulating
- operational public health
- medical logistics and blood management
- medical command and control
- hospitalization
- combat and operational stress control
- laboratory
- veterinary
- dental
who performs casualty estimates?
S-1
3 casualty estimates:
- KIA (killed in action)
- WIA (wounded in action)
- MIA (missing in action)
the medical planner refines/analyses the casualty estimate by:
- number of patients anticipated at each role of care
- areas of patient density
- enemy prisoners of war (EPWs) and civilian patient estimates
- additional assets needed for patient movement
large numbers of casualties can severely strain medical capabilities if what?
not properly planned for!!
availability of medical resources
personnel and equipment strengths and critical shortages for:
organic medical assets
attached medical elements
supporting medical units
joint service and allied medical units
host nation medical resources
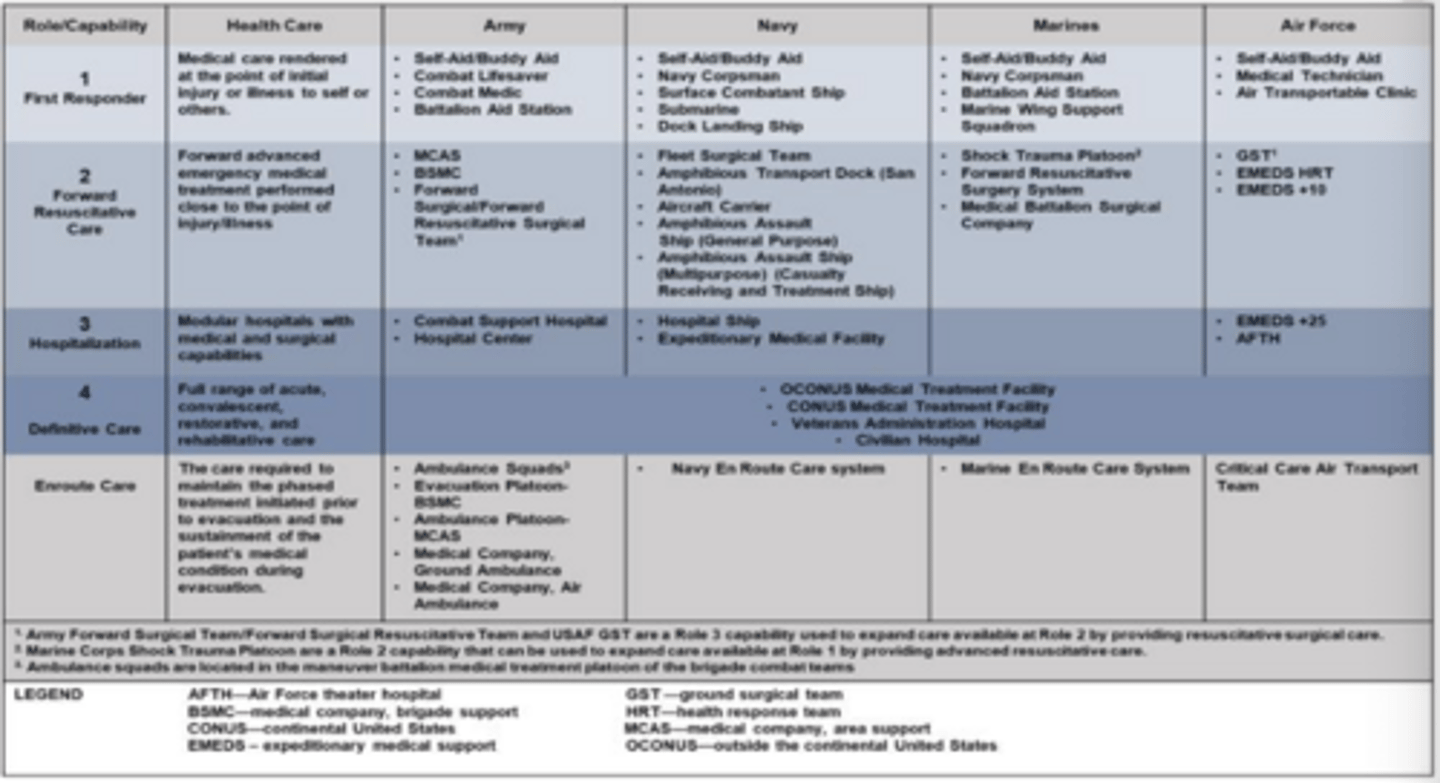
Roles of Care Comparison (image):
understanding the equivalent of Army capabilities will enable medical staff and commanders to more effectively utilize available forces in support of an operation as well as identify capability strengths and gaps.
AHS Support Considerations
the main purpose during medical analysis should be to examine the following seven areas in depth:
1) enemy situation
2) friendly situation
3) characteristics of the Area of Responsibility (AOR)
4) strengths to be supported
5) health and command
6) facts and assumptions
7) specified, implied, and essential tasks
Enemy Situation:
strength and location
combat efficiency
capabilities
logistics
EPW casualty estimate
Strength and location:
enemy elemnt's time, distance, and range
Combat efficiency:
enemy soldier's fatigue, training, and combat power
Capabilities:
NBC/Weapons of Mass Destruction (WMD)
Logistics:
enemy's ability to sustain their force
EPW Casualty Estimate:
evacuation requirements/medical supplies
Friendly Situation:
Strength and Disposition
Combat Efficiency
Rear Battle Plan
Weapon Systems
Strength and Dosposition:
U.S. allies, coalition, host nation, etc.
Combat Efficiency:
Soldier's training, morale, and experience
Rear Battle Plan:
Force protection, security, and higher medical support
Weapon Systems:
type of weapon systems being used = types of injuries
strengths to be supported
medical requirements for:
- joint services
- allied forces
- coalition forces
- refugees
- civilian population of Host Nation
- enemy prisoner of war (EPW) population
- Department of Defense (DOD) personnel
plan for adequate medical assets and medical supplies!!!
Health of the Command
Medical readiness of the soldier includes:
- immunizations
- acclimatization
- nutrition
- fatigue (sleep)
- combat and operational stress
- dental status
"The most important element of Combat Power is the _______."
Soldier
what is an area of interest?
is that area of concern to the commander, including the area of influence, areas adjacent to it and extending into enemy territory (JP 3-0).
also includes areas occupied by enemy forces who could jeopardize the accomlishment of the mission.
an area of interest varies in size and shape from operation to operation.
within assigned areas, commanders organize their operations in terms of time, space, and purpose by synchronizing deep, close, and rear operations.
characteristics of the AOR
Terrain- Obstacles, Avenues of Approach, Key Terrain, Observation and Fields of Fire, Cover and Concealment (OAKOC):
- effects on soldiers
- effects on medical eval
- primary and alternate evacuation routes
- terrain for landing zone (LZ)
- special evacuation equipment needed
- site selection for medical assets
- effect on communications
Characteristics of the AOR
Weather:
- effect on ground air evacuation
- care for wounded in adverse weather
- effect on supplies and equipment
- maintenance requirements
Characteristics of the AOR
Flora and Fauna:
- poisonous reptiles
- disease vectors
- poisonous plants
Facts:
known to be true
Assumptions:
assumed to be true in the absence of positive proof
- sometimes necessary to enable the planner to complete the estimate and decide on a COA
- May be deleted or modified as new information becomes available
areas to consider in absence of facts:
- Host Nation support
- Resupply rates
- Use of weapons of mass destruction
- Time-Frame of operation
- Status of evacuation routes
"the goal is to turn ___________ into ________."
assumptions; facts
AHS Support Plan:
varies in purpose and scope according to the size and complexity of the supported operation
the AHS support plan of a combat battalion includes (at a minimum):
- location of the casualty collection points
- location of ambulance exchange points
- location of the Battalion Aid Station
- primary and alternate evacuation routes
components of a quality plan:
- provides for accomplishing the mission
- based on facts and valid assumptions
- uses existing resources
- clearly establishes relationships and assigns responsibilities
- provides for decentralized execution of the plan
- Simple, Flexible, Controlled, and Coordinated
Key Sustainment Coordination:
G1/S1
G2/S2
G3/S3
G4/S4
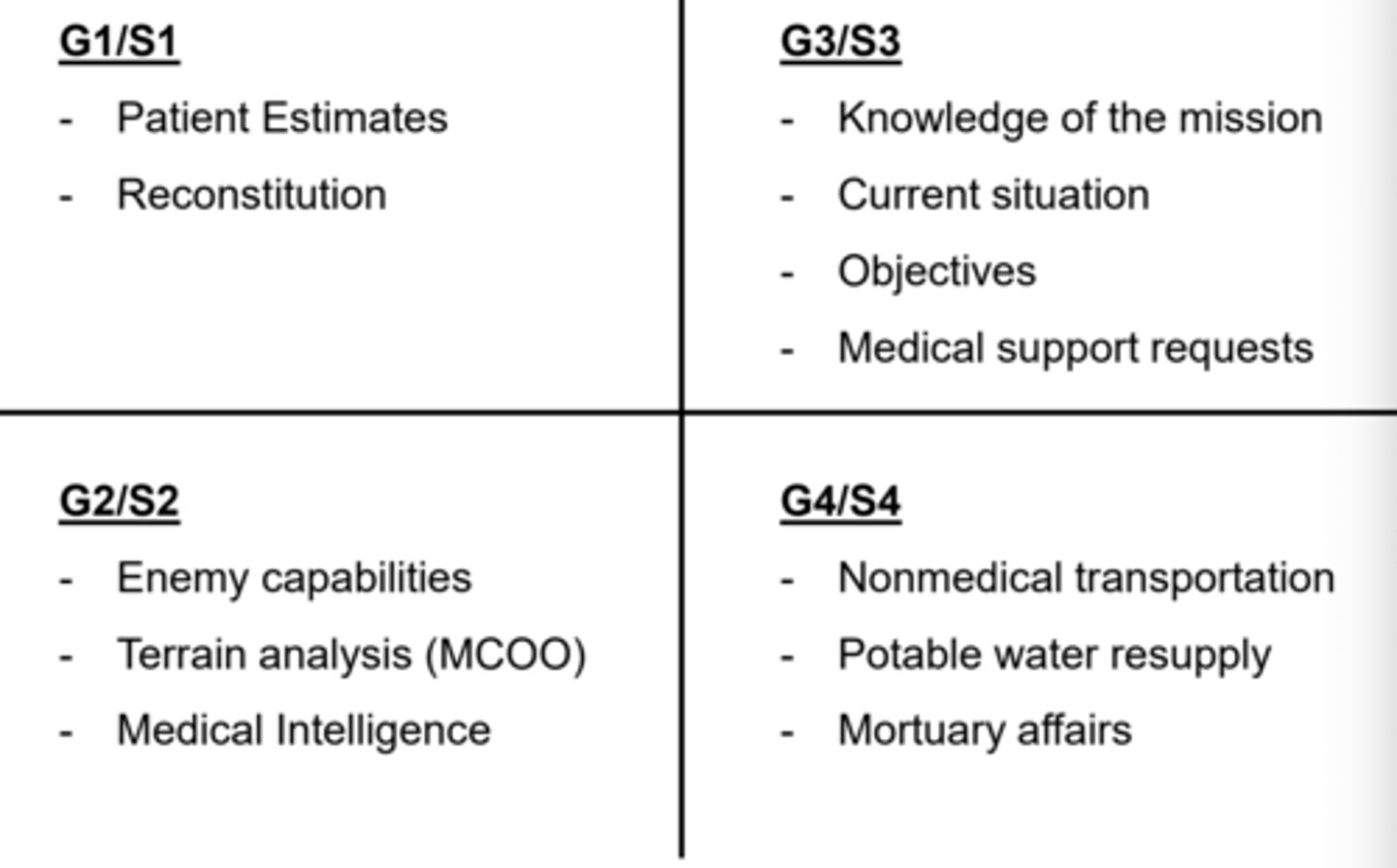
G1/S1:
- patient estimates
- reconstitution
G2/S2:
- enemy capabilities
- terrain analysis (MCOO)
- medical intelligence
G3/S3:
- knowledge of the mission
- current situation
- objectives
- medical support requests
G4/S4:
- nonmedical transportation
- potable water resupply
- mortuary affairs
Medical COA Development:
the medical plan must support the Commander's Intent and enable the accomplishment of the mission for the tactical COA developed
to develop the Medical Plan for each COA you must understand the following:
- Commander's Intent
- Tactical Scheme of Maneuver for each COA
- Task Organization of each COA
- Results from medical estimate
- Specified, Implied, and Essential Tasks
- Constraints and Limitations
- Unit Tactics, Techniques, and Procedures (TTPs)
Medical COA Development
- array medical assets
- determine command and control relationships for medical elements
- develop concept and support sketch and synch matrix
- maximize use of existing graphics and control measures
- refine the casualty estimates
- based on maneuver task organization for that COA
- do estimates at smallest level (i.e. on each OBJECTIVE)
- keep the six medical principles in mind:
- conformity, proximity, flexibility, mobility, continuity, and control
each medical COA must meet the following criteria:
feasible - can we do it?
acceptable - acceptable risk?
suitable - is it nested with the maneuver plan?
distinguishable - are there significant differences?
complete - includes all medical functional areas?
each medical COA should address medical support for each of the following:
security operations (Basic Reconnaissance Teams)
main/supporting attacks (close fight)
rear operations (BDE Staging Area, FA units, etc.)
follow-on operations (Stability OPS, Defense OPS, etc.)
identify the _______ and _______ of each medical element during COA development
TASK and PURPOSE
advantages of ground evacuation:
- least affected by weather
- more reliable
disadvantages of ground evacuation:
- speed
- obstacles
- road networks
- enemy threats (IEDs, RPG, etc.)
advantages of air evacuation:
- airlift medical supplies and medical personnel
- avoid traversing difficult terrain
- reduce patient discomfort
- range and speed
disadvantages of air evacuation:
- adverse weather
- enemy air-to-air threat
- enemy anti-aircraft weapons
- more difficult to get approval to use
considerations for COA development:
- casualty estimate
- capabilities - treatment and evacuation assets
- logistics assets - DOS, resupply rate, push-packages
- evacuation policy
- evacuation routes (air vs. ground)
- non-medical transportation assets
- Host Nation support
- Modified Combined Obstacle Overlay (MCOO)
- Enemy Situation Template
- Timeline of operation
"Scheme of Maneuver" for medical plan should include:
- task organization for medical assets
- Task and Purpose for each medical element
- Command and Control relationships
- Evacuation and Supply routes
- important maneuver graphics
- Ambulance Exchange Points (AXPs) and Casualty Collection Points (CCPs)
- evac routes (air/ground)
- location of treatment facilitates
- Pickup Zones (PZs) and Landing Zones (LZs)
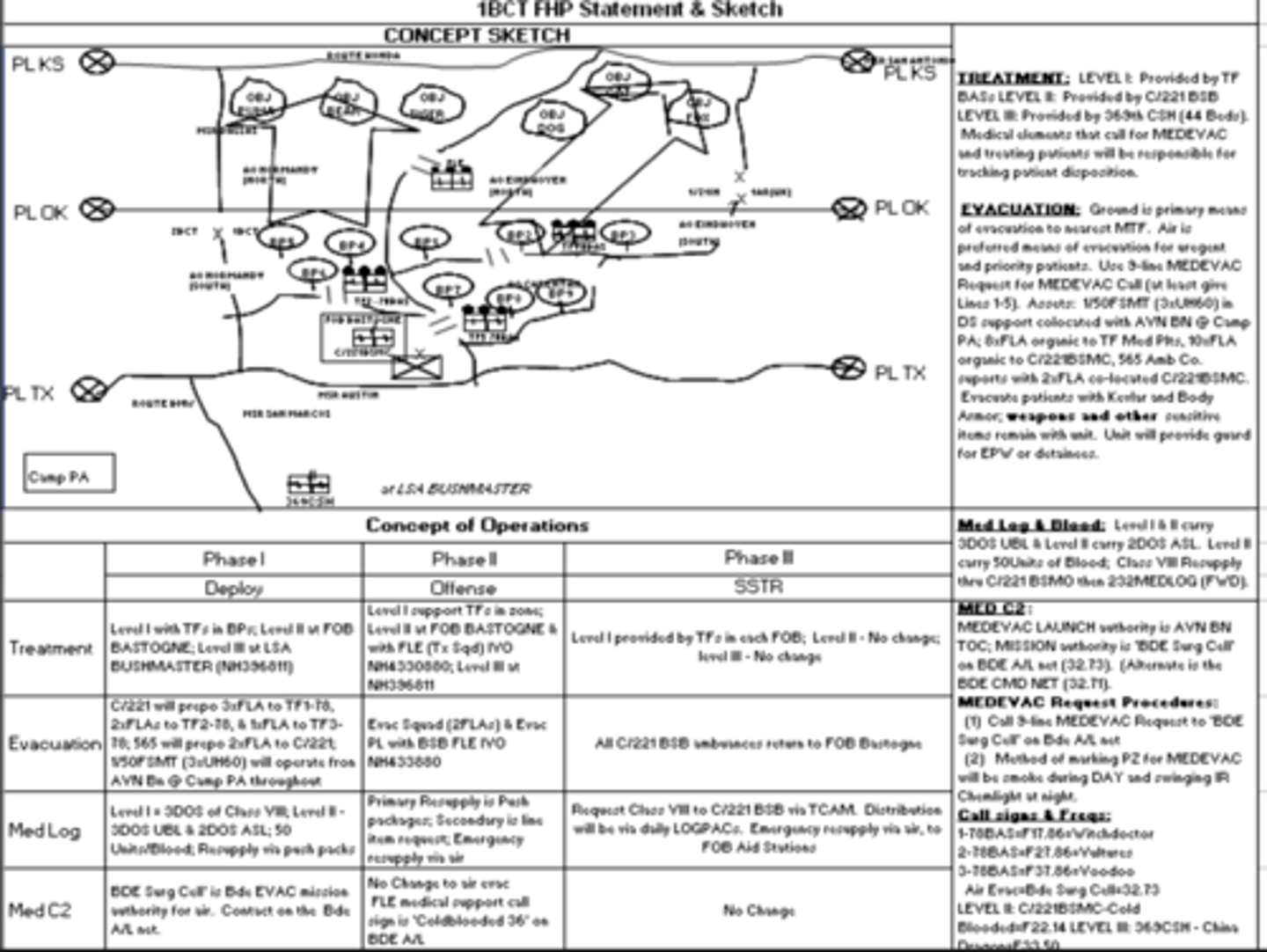
1BCT FHP Statement and Sketch:
COA Comparison and Evaluation:
as the tactical staff compares ("wargames") feasible COAs, the medical planner compares the medical plan of each COA to determine which maneuver COA can be best supported from a medical perspective
you are evaluating EACH COA from a:
medical perspective!
Medical plan evacuation criteria:
criteria is established based on the mission, Commander's Intent, and Commander's Guidance
use the Medical Functional Areas as criteria:
- medical treatment
- evac and medical regulating
- operational public health
- medical logistics and blood management
- medical command and control
- hospitalization
- combat and operational stress control
- laboratory
- veterinary
- dental
"The Wargame":
- refine casualty estimates by phase and/or event
- movement of medical assets (determine grid locations)
- decision points (add to medical synch matrix)
- requirements vs. capabilities (identify shortfalls and use to request additional support, if needed)
- time/distance analysis
- MEDEVAC/CASEVAC coverage
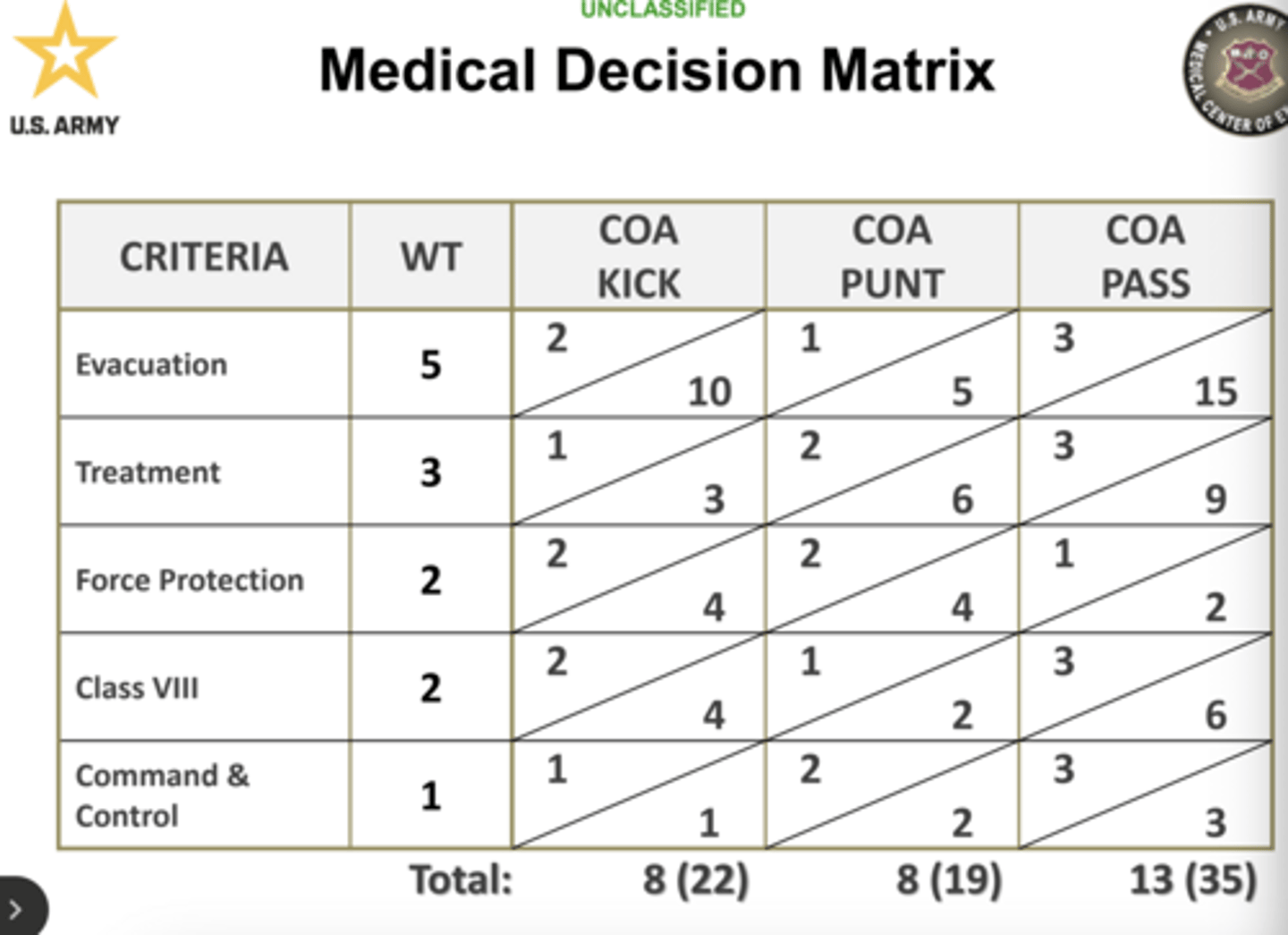
decision matrix -
- a decision matrix provides the medical planner with a tool for evaluating COAs
- criteria is established based on mission, Commander's Intent, and Commander's Guidance
- Weights are assigned to each criteria in relation to its importance in accomplishment of the medical plan
scores are totaled with lowest number being best
Medical Decision Matrix (image):
the medical planner's jobs:
- ensures medical is part of criteria for analysis of maneuver COAs
- prepared to answer Commander's questions (has done the analysis and understands all the products leading up to recommended COA)
- the commander will select a COA, modify a COA, or combine COAs to form a new one
- once the commander selects a COA, the medical planner must refine and publish the medical plan (medical appendix)
Appendix 3 (Medical) to Annex F (Sustainment) to OPORD