NPTE: GI Signs and Symptoms
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Anuria
inadequate urine output in 24 hours (<100 mL)
Endometrium
inner lining of the uterus, which is shed monthly as a result of hormonal influence
Impotence
inability to ejaculate or obtain orgasm
Nephrolithiasis
kidney stones
Urinary frequency normal vs abnormal
6-8x/day is normal but >8 is abnormal
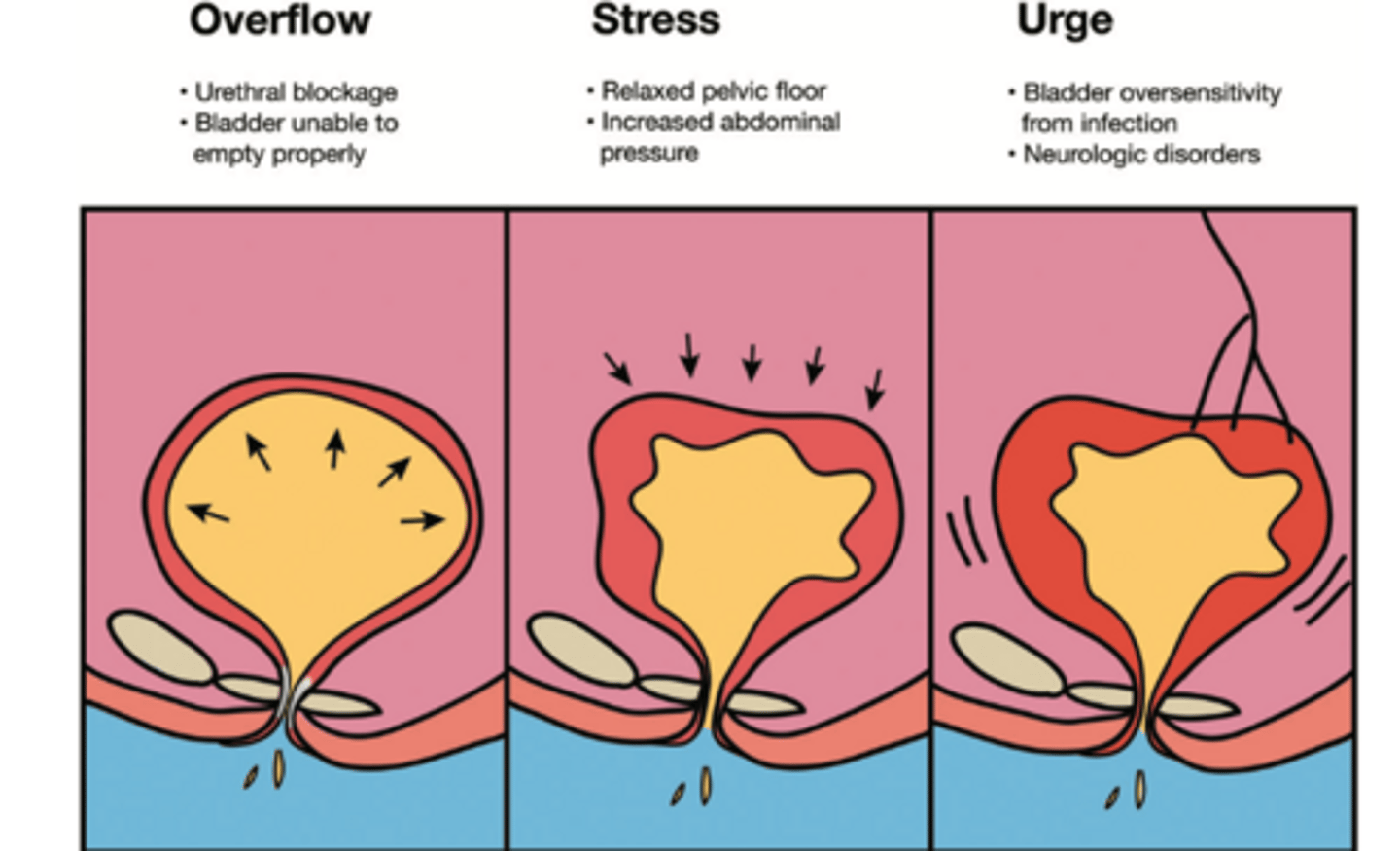
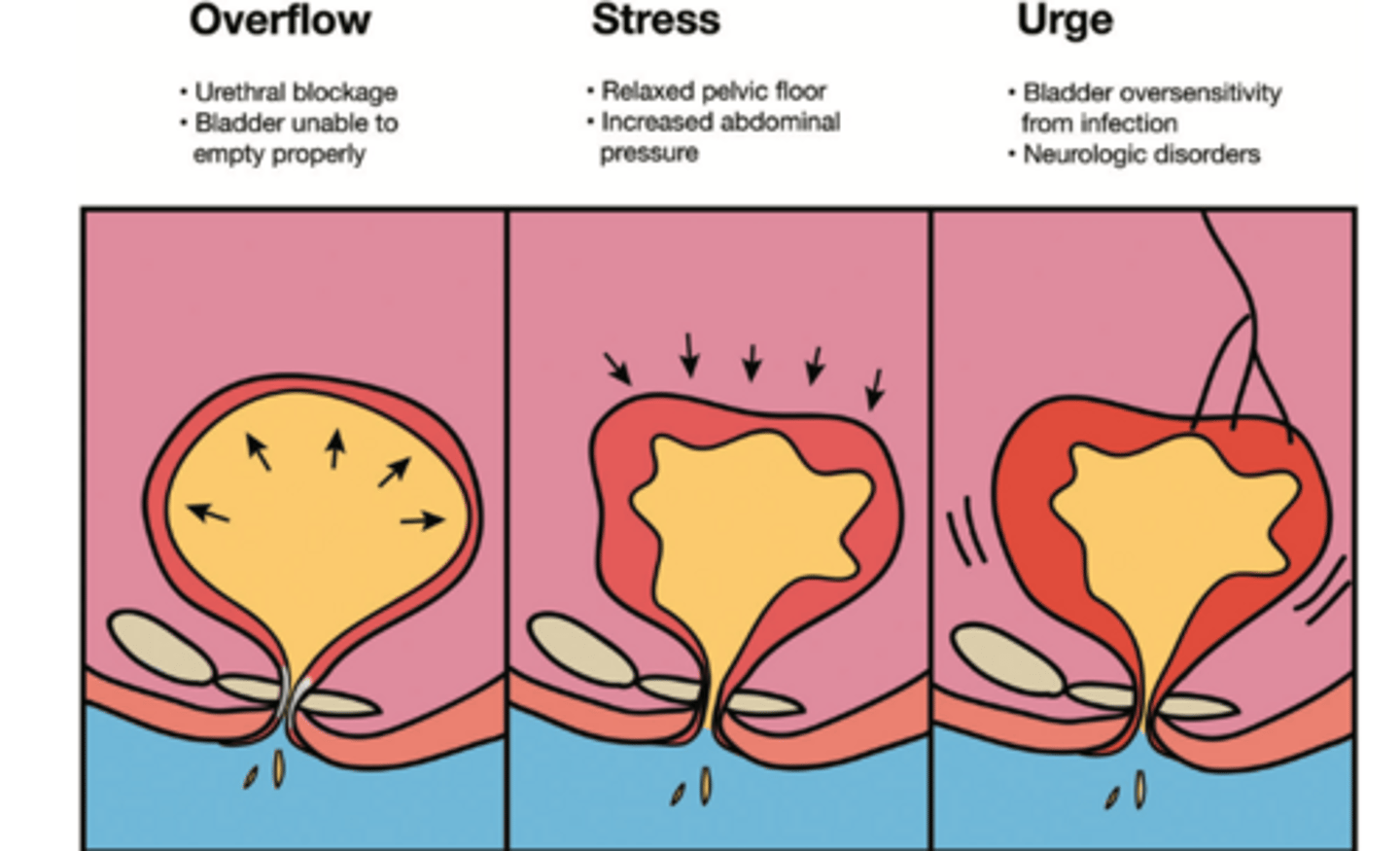
Stress incontinence
sudden involuntary leakage of urine during cough or exercise (increase in pressure)
➤ Due to muscle weakness or laxity
➤ Treatment: Pelvic floor strengthening; Electrical stimulation and biofeedback therapy for pelvic floor muscles
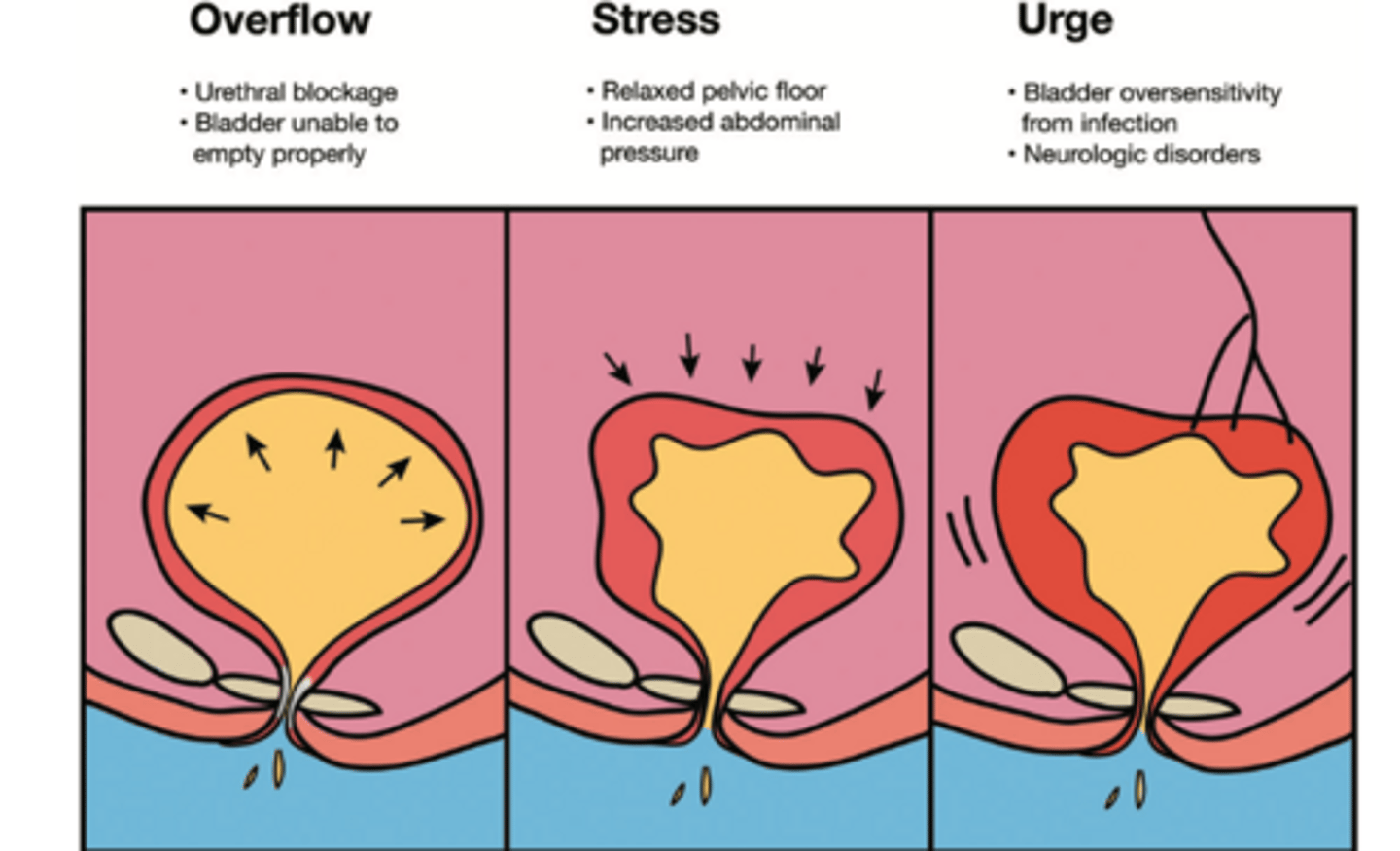
Urge incontinence
involuntary loss of urine immediately after the "urge"
➤ Involuntary contraction of detrusor muscle with strong desire to void
➤ Often idiopathic, but can be caused by medications, alcohol, bladder infections,
bladder tumor, neurogenic bladder, or bladder outlet obstruction
➤ Treatment:Treatment of infections. Behavioral modifications, Biofeedback therapy, Pelvic floor muscle training along with bladder training (scheduled voiding, urge-suppression techniques), Prompted voiding (individuals with cognitive impairments), Patients should be encouraged to manage constipation, Avoid bladder irritants such as caffeine, alcohol, nicotine, and carbonated
drinks
Functional incontinence
Incontinence due to mobility, dexterity, or cognitive deficits
Treatment:
- Eliminate clutter
- Prompt voiding
- Modify the environment to increase accessibility
- Provide functional mobility training to increase timely access to bathroom facility
Overflow incontinence
overdistention of bladder and inability of bladder to empty
completely
➤ Urine leaks or dribbles → patient does not have any sensation of fullness or emptying
➤ Causes: deficient or contractile detrusor muscle, hypotonic or underactive detrusor muscle secondary to drugs, fecal impaction, DM, lower spinal cord injury (SCI), multiple sclerosis (MS); In males, overflow incontinence is mostly due to prostatic hyperplasia, prostatic carcinoma, or urethral stricture; In females, overflow incontinence is mostly due to obstruction caused by severe
genital prolapse or surgical overcorrection of urethral detachment
➤ Treatment: Medication and catheterization
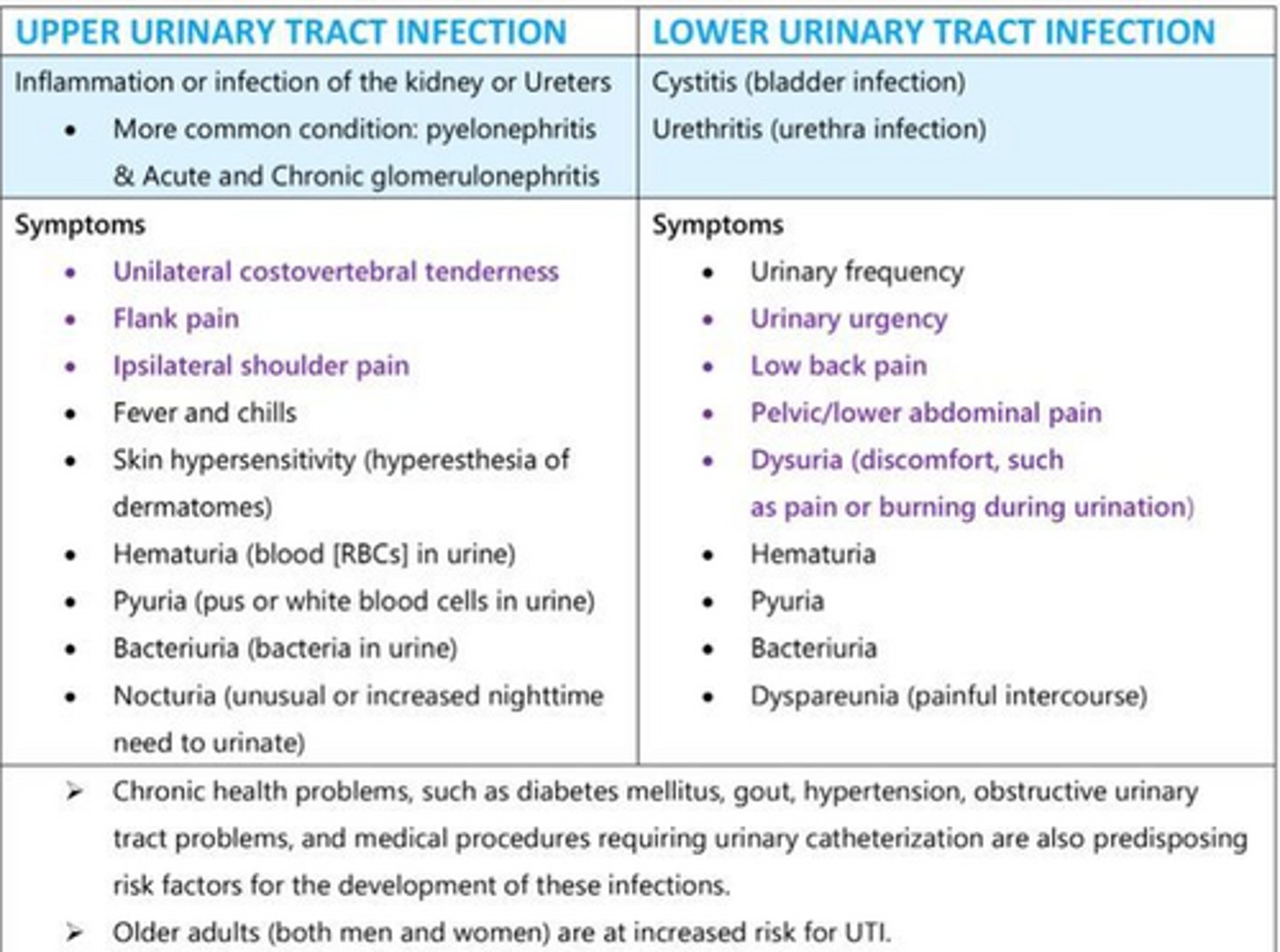
Upper vs lower urinary tract infection
Upper UTI: kidney or ureteral infections
● More serious because the lesions can be a direct threat to renal tissue
● Pyelonephritis, acute and chronic glomerulonephritis, renal papillary necrosis, and renal tuberculosis
Lower UTI: cystitis or urethritis
● Usually secondary to ascending UTIs; may also involve kidney and ureters or lymphatics
● More common in females because of their shorter urethras and the proximity of the urethra to the vagina and rectum
Spinal control for micturition originates from sacral segments
S2, S3, S4
Spastic or UMN bladder
patients with lesions that occur above T12; AKA hyperreflexic bladder
● Reflex arc is intact; bladder contracts and reflexively empties in response to a certain level of filling (difficulty holding urine)
● Bladder and sphincter dyssynergia
➤ Hyperreflexive detrusor muscle
➤ Sphincter tone is increased
● Even with small volumes of urine, the detrusor muscle contracts
● Treatment
➤ Intermittent catheterization: 3 to 6 hours
➤ Suprapubic tapping
➤ Anticholinergic medications
➤ Voiding schedule
Flaccid or LMN bladder
patients with lesions that occur below T12 AKA flaccid bladder (difficulty in voiding urine)
● No preservation of reflex arc
● Treatment
➤ Intermittent catheterization: 3 to 6 hours
➤ Poor response to medications
➤ Valsalva maneuver
➤ Credé maneuver: manually compressing lower abdomen
➤ Timed voiding program
Renal cystic disease
Renal cysts are fluid-filled cavities that form along the nephron; These cysts can lead to the degeneration of renal tissue and the obstruction of tubular flow
■ Types: Polycystic kidney disease, cystic diseases of the renal medulla, acquired cystic kidney disease, single cysts, cystic renal dysplasia, miscellaneous renal cystic disorders
■ Clinical manifestations
-Pain
-Hematuria
-Fever
-HTN
-Abdominal or flank pain
Renal calculi or kidney stones s/s and tx
crystalline structures formed from urine
S/S:
-Renal colic pain: sudden, sharp, severe pain (Pain originates deep in the lumbar area and radiates around the side and down
toward the testicles in males and the bladder in females
-Ureteral colic pain: pain radiating toward the genitalia and thighs
-Nausea, vomiting
-Hematuria
-Fever and chills
-Urinary frequency
Treatment:
-Nonsteroidal anti-inflammatory drugs (NSAIDs), narcotics, thiazide diuretics
-Adequate fluid intake and dietary modification
-Restrict high oxalate foods (eg, peanuts, spinach, chocolate, and sweet potatoes)
Hydronephrosis
when a stone blocks the flow of urine, causing urine pressure to build up in the ureter and kidney
Male sex hormones
testosterone and androgen
Erectile dysfunction causes
➤ Neurogenic causes: stroke, cerebral trauma, SCI, MS, Parkinson disease
➤ Psychogenic causes: anxiety, fear, depression, stress, fatigue
➤ Hormonal causes: decreased androgen, hypothyroidism, hypopituitarism
➤ Vascular causes: HTN, CAD, hyperlipidemia, cigarette smoking, DM
➤ Medication causes: antidepressants, antipsychotics, alcohol, antihypertensives, antiandrogens, amphetamines
➤ Increased age
➤ Surgical causes: transurethral procedures, radical prostatectomy, proctocolectomy, abdominoperineal resection
PT interventions for erectile dysfunction
-External supports (SI belt, corsets)
-Stabilization exercises
-Avoid single-leg weight-bearing exercises, excessive hip abduction, and hyperextension
-No quadruped fire hydrants
Prostatitis what is it and types
infection and inflammation of the prostate gland, causing enlargement
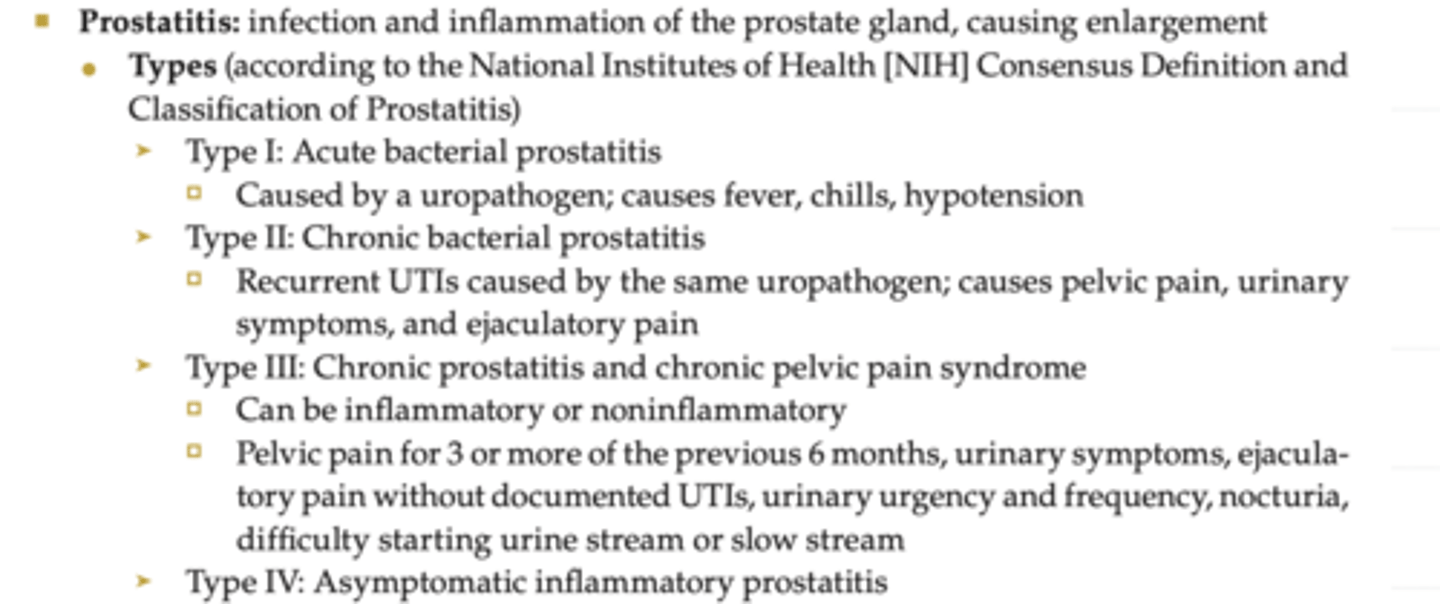
S/S of prostatitis
➤ Fever, chills
➤ Low back, inner thigh, and perineal pain
➤ Testicular or penis pain
➤ Urinary urgency and frequency
➤ Nocturia
➤ Dysuria
➤ Weak or interrupted urine stream (hesitancy)
➤ Inability to completely empty bladder
➤ Sexual dysfunction (painful ejaculation, cramping and/or discomfort after ejaculation, infertility)
➤ General malaise
➤ Arthralgia
➤ Myalgia
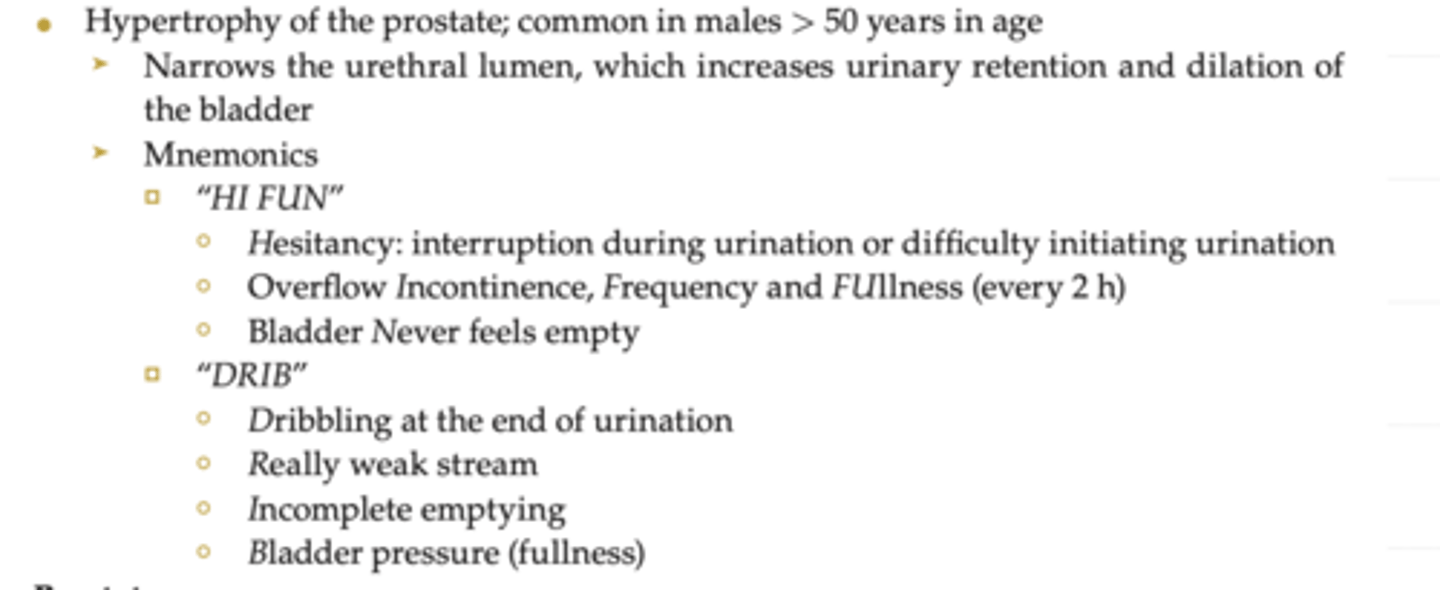
Benign prostatic hyperplasia
Prostate cancer
● Approximately 50% to 75% of men aged > 75 year have carcinoma in situ (slow growing)
● Increase in prostate-specific antigen (PSA)
➤ PSA level rises in patients with an enlarged prostate, prostate tumor, or prostate infection
Clinical S/S of BPH and prostate cancer
➤ Bladder palpable above pubic symphysis
➤ Urinary problems
Hesitancy
Weak urine stream
Dribbling at the end of urination
Frequency: urinate every 2 hours
Nocturia
● Lower abdominal discomfort → need to void
● Low back pain (LBP) and/or hip or upper thigh pain or stiffness
● Suprapubic or pelvic pain
● Difficulty having an erection
● Blood in urine or semen
External vs internal genitalia of female reproductive system
■ External genitalia: mons pubis, labia majora, labia minora, clitoris, perineal body (Urethra and anus are in close proximity, which can lead to cross-contamination)
■ Internal genitalia: vagina, uterus, cervix, fallopian tubes, paired ovaries
Ovaries functions
➤ Production and storage of ova (female germ cells)
➤ Produce sex hormones (estrogen and progesterone)
➤ Under control of hypothalamus and anterior pituitary gland
What does estrogen do?
➤ Estrogen decreases the rate of bone resorption (risk of OP and bone fracture increases after menopause)
➤ Estrogen increases the production of thyroid and increases the HDL level (increased risk of heart disease and cerebrovascular accident [CVA] after menopause)
Females taking raloxifene (estrogen) are at an increased risk of
deep vein thrombosis (stroke)
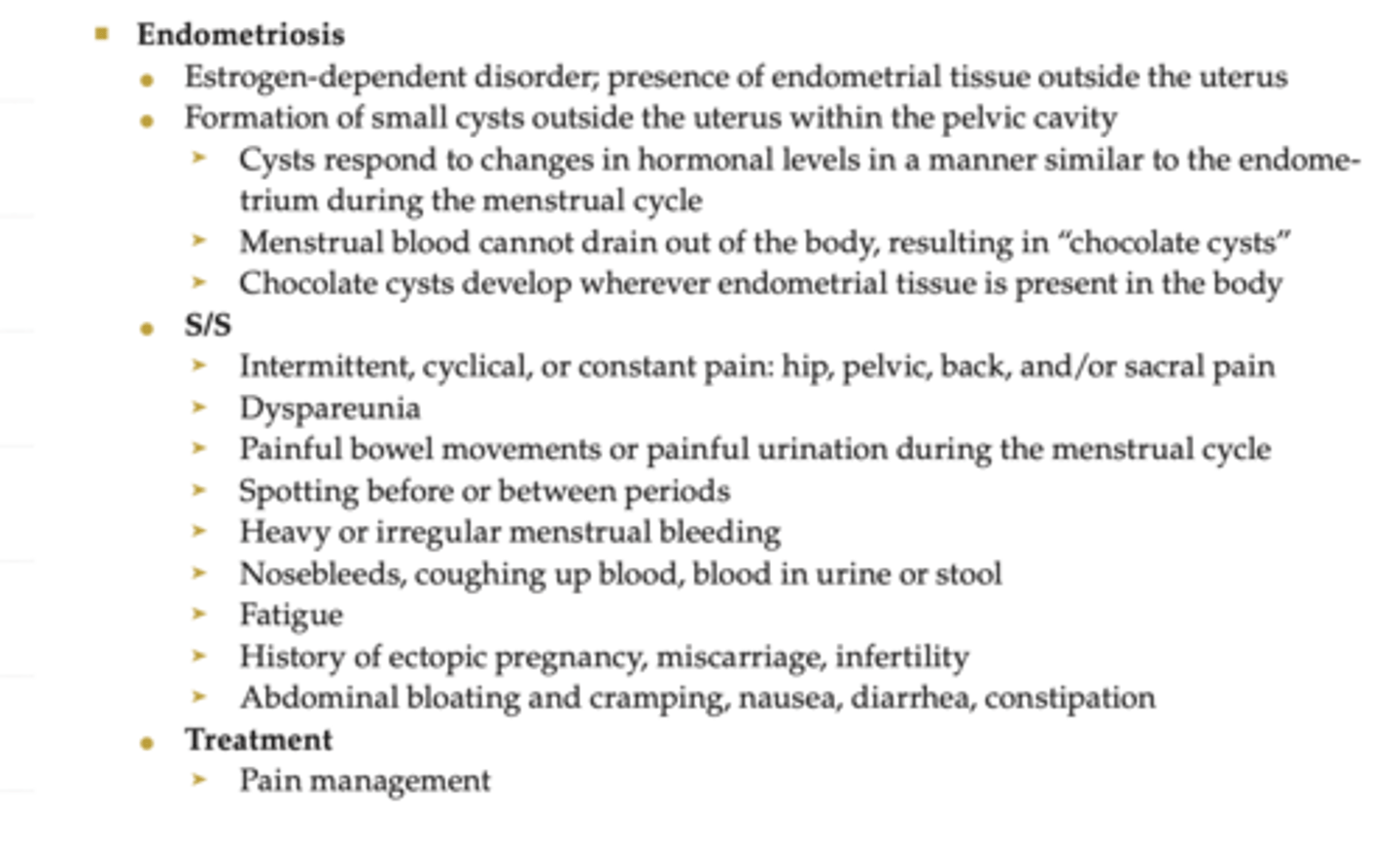
Endometriosis
Varicose veins
➤ Varicosities are aggravated during pregnancies by increased uterine weight, venous stasis in legs, increased venous distensibility
➤ Can occur in lower extremities, rectum (hemorrhoids), and vulva
➤ Usually present during first trimester and repeat pregnancies
➤ Pregnant women are more susceptible to DVT
➤ S/S: heaviness and/or aching in dependent positions
➤ Physical therapy interventions: Elevate legs; avoid crossing legs, which can press on veins; Elastic support stockings
Small vs large intestine
small: major digestive and absorption processes occur here
large: primarily absorbs water and electrolytes and stores and eliminates waste products
Accessory organs: liver, salivary glands, pancreas
aid in digestion by producing digestive secretions
GI motility: peristaltic movement
propels food and fluids by rhythmic intermittent contractions
of smooth muscle
● Except for the pharynx and the upper half of the esophagus
Vagus nerve controls
secretions and motility of GI tract
Gastrin role
secretes gastric acid in stomach; aids in digestion of proteins
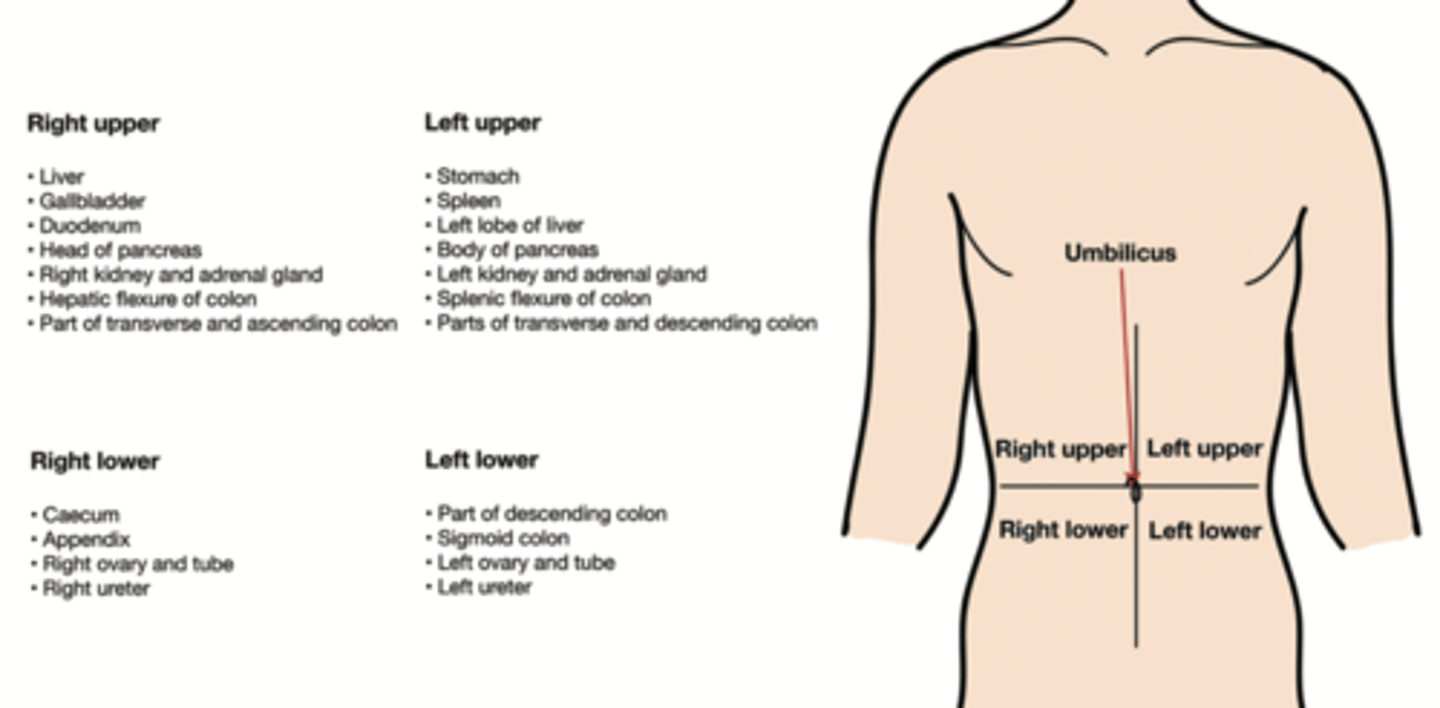
Abdominal quadrants referrals
➤ Right upper quadrant (RUQ): peptic ulcer, gallbladder pathology, head of pancreas
➤ Right lower quadrant (RLQ): appendix, Crohn disease (CD)
➤ Left lower quadrant (LLQ): diverticulitis, ulcerative colitis (UC), IBS
➤ Left upper quadrant (LUQ): tail of pancreas, spleen pathology
Referred pain felt in midback and scapula
esophagus, gallbladder, stomach, pancreas
Referred pain in shoulder
liver, diaphragm, pericardium
left: heart, diaphragm, tail of pancreas
right: gallbladder, liver, head of pancreas, peptic ulcer
Referred pain in pelvis, low back, and sacrum
colon, appendix, pelvic viscera
Referred pain from kidneys is
constant back pain that radiates upward toward thorax and anteriorly into abdomen
C diff precautions
contact (gloves, gown); life threatening diarrhea
CNS disorders that cause dysphagia
(stroke, Alzheimer disease, Parkinson disease), peptic esophagitis with stricture, GERD, neoplasm, asthma drugs, antidepressants, antihypertensives
Achalasia
condition in which the lower esophageal sphincter fails to relax and food is trapped in the esophagus
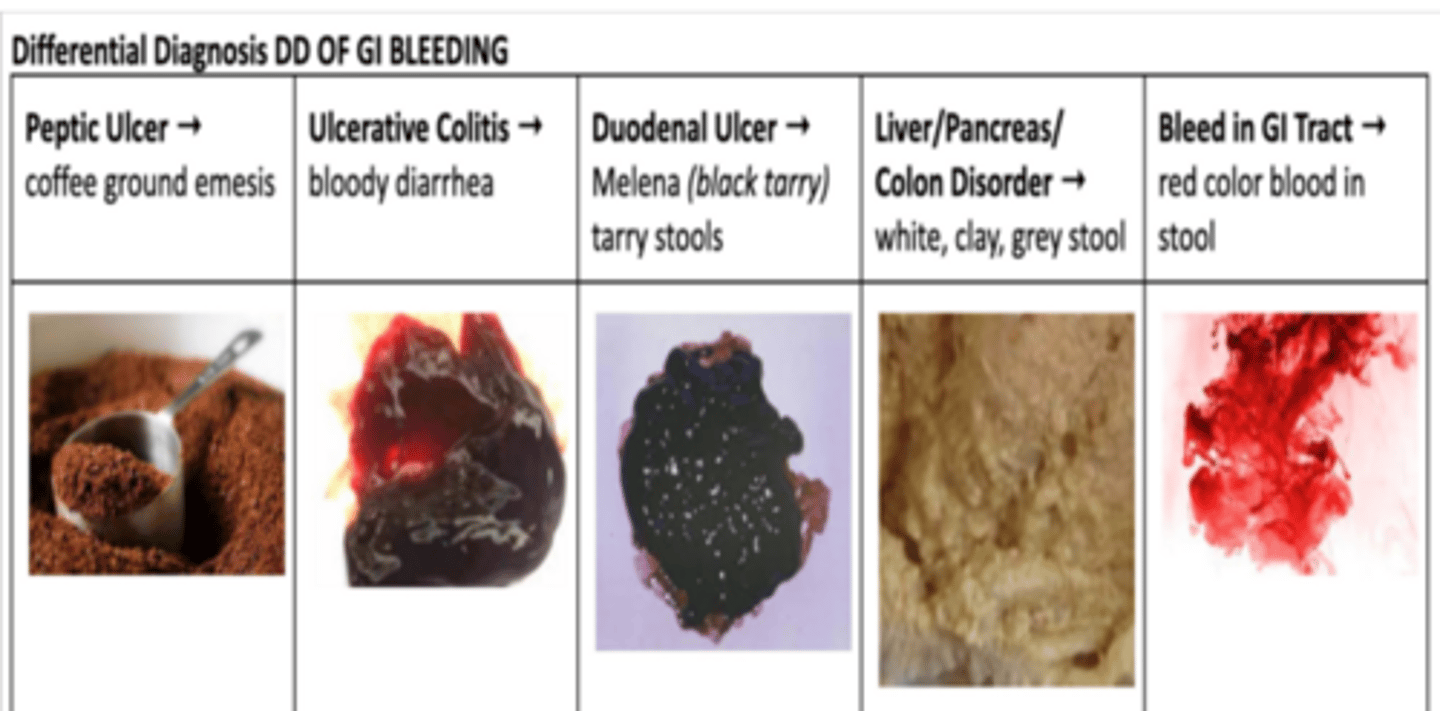
peptic ulcer, ulcerative colitis, duodenal ulcer, liver, bleed in GI tract stool types
What can cause black stools and a patient's tongue to turn black
Diarrhea medications: such as pink bismuth (bismuth subsalicylate; brand names: Pepto-Bismol, Bismatrol, Kaopectate);
Radiation therapy can cause rectal bleeding
Occult (hidden) GI bleeding
can appear as midthoracic back pain with radiation to the RUQ; can be revealed only by fecal occult blood test (brand name: Hemoccult test) and laboratory test
Hepatitis
acute or chronic inflammation of liver
causes:
➤ Viral infection
➤ Chemical agents
➤ Drug reaction
➤ Alcohol abuse
➤ Autoimmune hepatitis
➤ Biliary cirrhosis
➤ Metabolic disorders (eg, Wilson disease: too much copper accumulates in organs)
Hep A
-Acute infectious: mild to severe
-Transmission through fecal oral route (contaminated food or water)
-Prevention: good personal hygiene, hand washing, sanitation, vaccination
Hep B
-Mild (acute, usually lasts for several weeks) to severe (chronic, lifelong)
-Transmission through blood, body fluids, or body tissues (transfusion, oral or sexual contact, sharing needles); Body fluids such as spinal, peritoneal, and pleural fluids; saliva; semen;
and vaginal secretion
-Prevention: education on disposable needles, screening of blood donors, immunization
Hep C
-Acute or chronic
-Transmission through blood, body fluids (transfusion, oral or sexual contact, sharing needles), organ transplants
Hep D
-Acute or chronic
-Transmission through blood, body fluids (transfusion, oral or sexual contact, sharing needles)
-Dependent on having HBV coinfection
-Poor prognosis, liver failure
Hep E
-Acute, infectious
-Transmission through fecal-oral route (contaminated food or water)
Classic s/s acute hepatitis
Malaise, fatigue, mild fever, nausea, vomiting, anorexia, RUQ pain, occasionally diarrhea, jaundice, dark urine, clay-colored stools
S/S chronic hep
fatigue, malaise, jaundice, RUQ pain, anorexia, arthralgia, fever, splenomegaly, hepatomegaly, weakness, ascites, hepatic encephalopathy