Peptic Ulcer Disease
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
20 Terms
Peptic ulcer
an ulcer of the alimentary mucosa, usually in the stomach or duodenum, that has been exposed to acid gastric secretion
Aggressive factors: gastric acid from parietal cells; pepsinogen converted to pepsin from chief cells
Protective factors: mucus-bicarbonate barrier; prostaglandins epithelial cell defense; mucosal blood flow
NSAID-induced
NSAIDs irritate gastric epithelium
Can happen within mins of ingestion or with chronic use
Can result in bleeding
NSAIDs cause systemic inhibition of prostaglandin synthesis (more inhibition of COX1 than COX2 [GI toxicity related to COX1]
Helicobacter pylori (H. pylori) - gram negative
bacteria disrupts normal mucosal defense and healing mechanisms; resides in gastric epithelium
Transmitted person-to-person via: fecal-oral, oral-oral, or gastro-oral
Causes PUD, chronic gastritis, mucosa-associated lymphoid tissue (MALT) lymphoma
More
Other Causes
Zollinger-Ellison’s syndrome
Hypersecretion of gastric acid
Viral infections
i.e. cytomegalovirus (CMV)
Radiation
Chemotherapy
Vascular insufficiency
i.e. cocaine use
Inherited
i.e. condition of hyperfunctioning parietal cells
Stress-related mucosal disease (SRMC) (also known as stress ulcers)
[NOT covered in this course; addressed with critical care topics)
Risk factors
Age 65 years old
Previous PUD or upper GI complications
Chronic illness
Smoking
NSAID-related dyspepsia
Alcohol use
Previous H. pylori infection
Rheumatoid arthritis
Corticosteroid+ NSAID use
ASA + NSAID use
NSAID use > I month
High-dose NSAID use
Anticoagulant use or coagulopathy
Antiplatelet agent use
Oral bisphosphonate use
SSRI use
Exacerbating factors
Stress – may alter inflammatory response
Spices/spicy foods – causes dyspepsia
Caffeine – stimulates gastric acid
Food may bring on pain with gastric ulcers; pain can be relieved by food with duodenal ulcers
GI Bleeds
Causes
Peptic Ulcer Disease – NSAID-induced or H. pylori
Esophagitis
Mallory-Weiss tear (causes: vomiting, coughing, alcoholism)
Cancer
Stress ulcers/SRMD (in ICU population)
Varices
Determine whether a patient’s symptoms of PUD are eligible for self-treatment or medical referral is needed
Self Treatment
NSAID alternatives
Reducing alcohol
Reducing stress
Reduce spicy food, caffeine
Medicare referral
H. pylori
Indications of endoscopy
Presence of alarm symptoms
NSAID etiology has been ruled out
Suspicion for complications
Need for accurate diagnosis
History of previous H. pylori infection
Alarm symptoms
GI bleeding
weight loss
early satiety
dysphagia or odynophagia
family history of upper GI malignancy
Iron deficiency anemia
New upper GI symptoms when > 55 years of age (risk for cancer)
NSAID-induced ulcers treatment: PPIs
PPIs are best at:
Inhibiting acid secretion
Relieving ulcer symptoms
Healing ulcers
Maintaining ulcer-healing
Higher PPI dosing should be divided throughout the day for good pH control
MOA: suppresses gastric acid secretion by inhibiting parietal cells H+/K+ ATP pump
Onset: about 4 days for full effect (some acid suppression in 1-3 hours)
Agents:
Omeprazole (Prilosec OTC) - OTC
Esomeprazole (Nexium 24HR) - OTC
Lansoprazole (Prevacid 24HR) - OTC
Omeprazole + sodium bicarb (Zegerid) - OTC
Start with once daily dosing
Dexlansoprazole (Dexilant) - Rx
Rabeprazole (Aciphex) - Rx
Pantaprazole (Prontonix) - Rx
Counseling: take 30 - 60 mins before AM meal
AEs: HA, dizziness, somnolence, diarrhea/constipation, nausea; long-term: B12 deficiency, C.Difficile infection, pneumonia
Prevention of NSAID-induced ulcer: Prostaglandin Analog
Indications: prevention of NSAID-induced gastric ulcers
MOA: replaced the protective prostaglandin consumed with prostaglandin inhibiting therapies
Agent
Misoprostol: synthetic prostaglandin E1 analog
Induced uterine contraction
Used for that purpose/indication, but do not admin to women of childbearing potential for ulcer prevention
Counseling: take 4 times daily
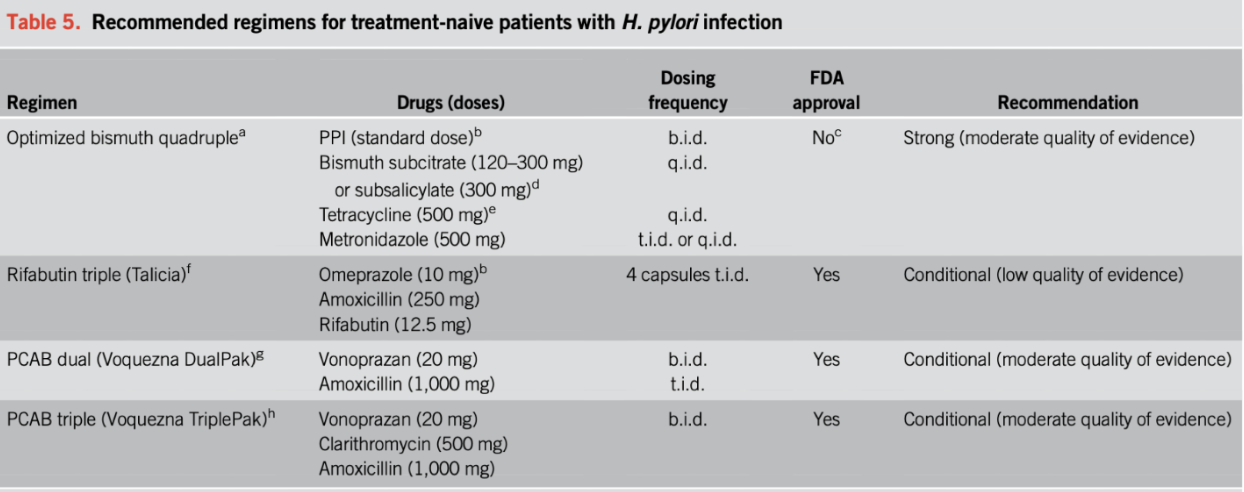
Treatment of H. pylori ulcers ACG guidelines
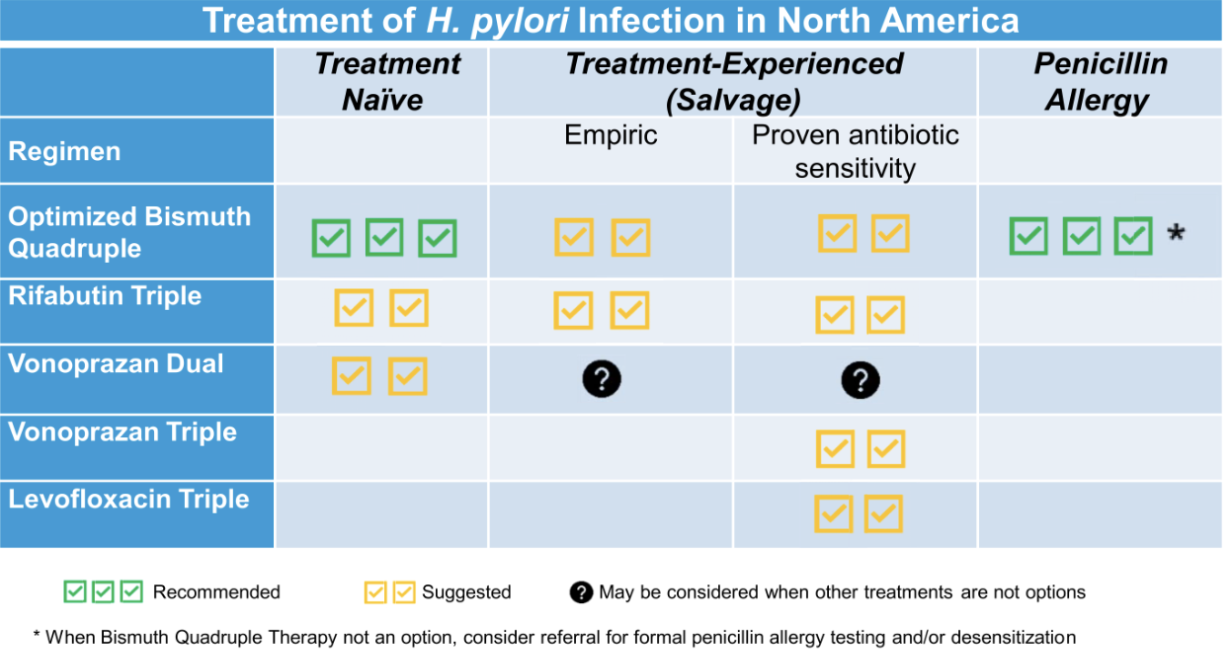
1st case or H. pyrlori
Preferred: Optimized Bismuth Quadruple Therapy (BQT)
Treatment choice in penicillin allergy
Treatment choice when antibiotic resistance rates are unknown
2nd line options
Rifabutin Triple
Vonoprazan Dual
ACG CPG initial treatment
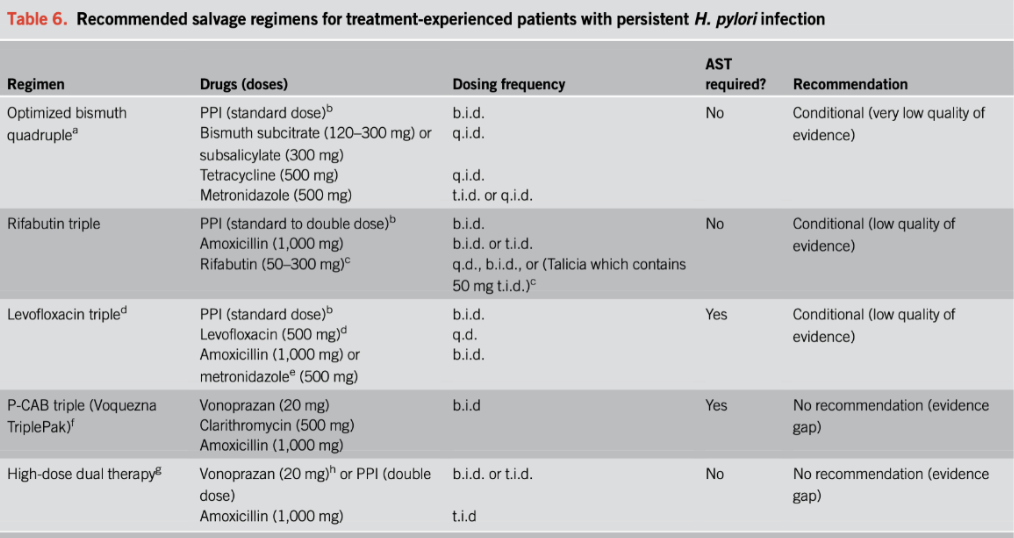
Recurrence/salvage
Empiric Options
Optimized Bismuth Quadruple Therapy (BQT)
Rifabutin Triple
Know antibiotic sensitivity
Optimized Bismuth Quadruple Therapy (BQT)
Rifabutin Triple
Vonoprazan Triple
Levofloxacin Triple
ACG CPG salvage regimens
Vonoprazan
Potassium-competitive acid inhibitor (PCAB)
20 mg twice daily
Administered with antibiotics for treatment regimen
Indication: H. pylori infection; erosive esophagitis
MOA: results in rapid and reversible inhibition of pumps and acid secretion
Rapid onset of action and full effect with 1st dose
Rifabutin
Antitubercular agent
Varied frequencies based on regimen
Administered with PPI and amoxicillin
Indication: H. pylori infection
MOA: inhibits bacterial RNA synthesis leading to cell death of H. pylori
Steps for GI bleed
Stabilize patient
Give blood, fluids
Possibly admit to ICU
Patient may need NG tube if patient aspirates
Manage underlying condition
Stop NSAIDs if applicable
Treat H. pylori if applicable
Endoscopic repair
Sclerotherapy, clips, etc.
GI bleed treatment
IV PPI therapy (esomeprazole or pantoprazole are only IV PPIs)
Dose: 80 mg IV bolus + 72 hour continuous drip
This dose raises gastric pH to enhance coagulation
Continue once daily PPI until patient considered low-risk to decrease mortality and decrease re-bleeding
Use PPI early in management of condition (even if no endoscopy available for evaluation)
Treatment of NSAID-induced ulcers
Discontinue the NSAIDs
Administer antisecretory therapy if symptoms are still present after discontinuing NSAIDS
PPI for 4-6 weeks for ulcer <1cm; 6-8 weeks for >1cm
If NSAIDs need to be continued, continue PPI for maintenance/prevention
Endoscopy if still having symptoms
If H. pylori positive, follow that treatment path
Gastric Protection for long-term NSAID use
Adding Protection
Ex. someone taking low-dose aspirin for cardiac indication, add on PPI or misoprostol if they have GI risk factors
Someone taking low-dose aspirin for cardiac indication and ibuprofen for chronic back pain, which to naproxen, and add on PPI or misoprostol
Or switch to acetaminophen if possible (if don’t need anti-inflammatory action); or decrease to lowest effective dose of NSAIDs
GI risk factors
Advanced age
Previous GI event
High dose of NSAID
Concomitant anticoagulant or corticosteroid
Cardiovascular disease
Pts would benefit from extra protection
PPI or misoprostol
Naproxen or COX2 NSAID if NSAID recommended
H. pylori Treatment
Choose regimen based on patient-specific/area-specific factors
Penicillin allergy
Resistance rates
Duration = 14-days
Choose PPI that is cost-effective and/or preferred by patient
Treatment of non-NSAID and non-H. Pylori ulcers
Ulcers not caused by NSAIDs or H. pylori
Treat gastric ulcer with PPI for 8 weeks
Treat duodenal ulcers with PPI for 8 weeks