chapter 12- personality disorders and impulse control disorders
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
personality disorders
overly rigid and maladaptive patterns of behavior and ways of relating to others that reflect extreme variations on underlying personality traits
personality disorders features
these problem traits become evident by adolescence or early adulthood
estimated 9% of general population is believed to be affected by personality disorders
people with personality disorders often fail to see how their own behaviors are seriously disrupting their live
people with personality disorders tend to perceive their traits as ego syntonic— natural parts of themselves
people with anxiety disorders and mood disorders tend to view their behaviors as ego dystonic — do not see their behaviors as parts of their self-identities
personality
set of distinctive psychological traits and behavioral characteristics that make each of us unique and help account for the consistency of our behavior
dsm and personality disorders
classifies personality disorders in three categories called clusters:
cluster A: people who are perceived as odd or eccentric; includes paranoid, schizoid, and schizotypal personality disorders
cluster B: people whose behavior is overly dramatic, emotional, or erratic; consists of antisocial, borderline, histrionic, and narcissistic personality disorders
cluster C: people who often appear anxious or fearful; includes avoidant, dependent, and obsessive-compulsive personality disorders
cluster A personality disorders
paranoid personality disorder
schizoid personality disorder
schizotypal personality disorder
paranoid personality disorder
tendency to interpret other people’s behavior as deliberately threatening or demeaning
paranoid personality disorder features
overly sensitive to criticism
question sincerity and trustworthiness of friends and associates
difficulty forming relationships
do not have outright paranoid delusions
prevalence: 2.3 - 4.4% of American
schizoid personality disorder
social isolation; described as loner or eccentric; lacks interest in social relationships
schizoid personality disorder features
emotions appear blunted; rarely experience anger, joy, or sadness
faces show no emotional expression
prevalence unknown
some cases, they harbor deep sensitivity about people and animals they cannot express
schizotypal personality disorder
difficulty forming close relationships; display behaviors, mannerisms and thought patterns viewed as odd; not disturbed enough to merit a diagnosis of schizophrenia
schizotypal personality disorder features
lack coherent sense of self
lack capacity for empathy
difficulty forming relationships
social anxiety linked to paranoid thinking
may experience unusual perceptions or illusions, but not enough for it to be psychotic
schizotypal personality disorder features cont
may develop:
ideas of reference: believing others are talking behind their backs
magical thinking: possessing 6th sense
attach unusual meanings to words, speech may be vague but not incoherent to be considered schizophrenia
prefrontal cortex is not affected like schizophrenia
cluster B disorders
antisocial personality disorder
borderline personality disorder
histrionic personality disorder
narcissistic personality disorder
antisocial personality disorder
disorder characterized by antisocial or irresponsible behavior and lack of remorse for misdeeds
antisocial personality disorder features
tend to be impulsive and fail to live up to commitments to others
show superficial charm and at least average intelligence
little anxiety and lack feelings of guilt or remorse
psychopath and sociopaths are considered to have antisocial personalities
antisocial and criminal behavior decline with age
sociocultural factors and antisocial personality disorders
most common among people in lower socioeconomic groups
antisocial personality disorder prevelence
6% men
2% women
limited to ages 18 or older
pattern of behavior for younger children are diagnosed as conduct disorder
early forms of antisocial behavior we see in childhood and adolescence include:
truancy
running away
initiating fights
use of weapons
forcing someone into sexual activities
physically cruel to people or animals
deliberate destruction of property
fire setting, lying, stealing, robbery, and assaulting others
antisocial behavior and criminality
associated, but not all criminals have antisocial personalities
most are law abiding citizens
antisocial personality is composed of two dimensions
personality dimension
behvaioral dimension
most antisocial ind show both
personality dimension
consists of traits such as superficial charm, selfishness, lack of empathy, callous and remorseless use of others, and disregard for others’ feelings and welfare → this type applies to people who don’t become law breakers
behavioral dimension
characterized by adoption of generally unstable and antisocial lifestyle; including frequent problems with law, poor employment history, and unstable relationships
psychopathic traits can be grouped into four basic factors
interpersonal factor: characterized by superficiality, grandiosity, and deceitfulness
affective factor: characterized by lack of remorse, empathy, failure to accept responsibility for misbehavior
lifestyle factor: characterized by impulsivity and lack of goals
antisocial factor: characterized by poor behavioral control and antisocial behavior
borderline personality disorder
characterized by features such as deep sense of emptiness, an unstable self-image, a history of turbulent and unstable relationships, dramatic mood changes, impulsivity, difficulty regulating negative emotions, self-injurious behavior, and recurrent suicidal behaviors
borderline personality disorder features
uncertain about their personal identities
cannot tolerate being alone
fear of abandonment leads to clinginess, demanding in their personal relationships
clinginess pushes people away
rejection— real or imagined— may enrage them
feelings towards others is intense and shifting
most common among latino americans
men with BPD show more violent or aggressive behavior and self harm than women
borderline personality disorder was originally used to refer to individuals whose behavior appeared to be on the border between neuroses and psychoses
usually maintain better contact with reality than people with psychoses, but may show signs during times of stress
core feature of BPD is difficulty regulating emotions
troubled by intense emotional pain and chronic feelings of anger
feelings of emptiness and shame are common
lack ability to thoughtfully plan their actions in advance, and will act impulsively without considering the consequences
BPD prevelence
1 in 10 commit suicide, 3 out of 4 attempt suicide
women show more inwardly directed aggression, such as cutting or other forms of self mutilation
men show more outward expressions of aggression
diagnosed in early adulthood
impulsive behavior might include:
spending sprees
gambling
drug abuse
splitting in BPD
inability to reconcile the positive and negative aspects of one’s experience of oneself and others
histrionic personality disorder
characterized by excessive emotionality and an overwhelming need to be the center of attention
histrionic personality disorder features
tend to be dramatic and emotional but emotions seem shallow and exaggerated
previously called hysterical personality
tend to be flirtatious but too wrapped up with themselves to develop intimate relationships
use their physical appearance to draw attention to themselves grow restless quickly with routine, and crave stimulation
narcissistic personality disorder
characterized by an inflated self image or grandiose sense of themselves and an extreme need for admiration
narcissistic personality disorder features
share features with histrionic personalities, but have more inflated view of themselves and less melodramatic than people with HPD
most people diagnosed are men
preoccupied with fantasies of success and power, ideal love, or recognition for brilliance or beauty
extremely sensitive to rejection
interpersonal relationships are strained
usually one sided, seek people who will serve their interests and nourish their sense of self importance
cluster C disorders
avoidant personality disorder
dependant personality disorder
obsessive compulsive personality disorder
avoidant personality disorder
terrified of rejection and criticism that they may be unwilling to develop relationships with others without ardent reassurances of acceptance
avoidant personality disorder features
have few relationships with others
affects 0.5-1% of general population
features of social withdrawal, but interested and feelings of warmth towards others
fear public embarassment
stick to routines and exaggerate the risks or effort involved in trying new things
often comorbid with social phobia
heightened amygdala activity in people with APD compared to healthy controls in social situations
dependent personality disorder
people who have an excessive need to be taken care of by others
dependent personality disorder features
leads them to be overly submissive and clingy in relationships
extremely fearful of separation
seek advice in making even the smallest decision
avoid positions of responsibility
may agree with outlandish statements about themselves and do degrading things to please others
must be viewed through cultural lense
dependent personality disorder features cont
diagnosed more frequently in women
linked disorder to increased risk of mood disorders and social phobia, as well as suicide and health problems
hypertension, cardiovascular disorder, and gastrointestinal disorders
link between disorder and smoking, eating disorders, and alcoholism
obsessive compulsive personality disorder
includes excessive orderliness, perfectionism, rigidity, and need for control over one’s environment
obsessive compulsive personality disorder prevelence
2.1-7.9% of population
twice as common in men as in women
obsessive compulsive personality disorder features
do not experience obsessions or compulsions
preoccupied with perfection they cannot complete work on time
stingy with money
difficulty making decisions in fear of wrong choice
inflexible and rigid in morality and ethics
overly formal in relationships and difficulty expressing feelings
categories or dimensions problems with the classification of personality disorders
problem with categories, too black and white
where to draw the line?
personality disorders’ features to some degree show up in all of the population,
when does it become abnormal
dimensional model
personality disorders dimensional model
depicts personality disorders as maladaptive and extreme variations of personality traits commonly found within general populaiton rather than discrete categories
limitation of dimensional model is we lack clear guidelines for setting cutoff scores
five factor model problems with the classification of personality disorders
neuroticism or emotional instability
extraversion
openness to experience
agreeableness or friendliness
conscientiousness
problems distinguishing personality disorders from other clinical syndromes
overlap
comorbidity is quite common
people receiving diagnosis for a personality disorder usually meet criteria for more than one
difficulty distinguishing between normal and abnormal behavior
confusing labels with explanations
psychodynamic perspectives of PD
traditional freudian theory focuses on problems arising from Oedipus complex
more recently theories focused on earlier pre-Oedipal period during which infants develop identities separate from their parents
Hans Kohut Psychodynamic perspective on PD
theory of self psychology
argues that what matters most is how the self develops
whether the person is able to develop self-esteem, values, and a cohesive and realistic sense of self opposed to an inflated narcissistic personality
believed people with narcissistic personality mount a facade of self importance to cover up feelings of inadequacy
narcissistic personalities may become enraged by others whom they perceive have failed to protect them from disappointment or have declined to shower them with reassurance, praise, and admiration
early childhood involves normal stage of healthy narcissism
infants feel powerful, empathetic parents reflect their childs perceptions
gradually, unrealistic expectations dissolve
lack of parental empathy sets stage for pathological narcissism
develop damaged self concepts and feel incapable of being loved and admired
involves facade of self perfection that cloaks perceived inadequacies
otto kerberg perspective on PD
views BPD in terms of a failure in early childhood to develop sense of constancy and unity in one’s image of oneself and others
BPD individuals cannot synthesize positive and negative elements of themselves and others into complete stable wholes
they shift back and forth between pure idealization and utter hatred → referred to splitting
margaret mahler psycho persp on PD
explained BPD in terms of childhood separation from the mother figure
normally children gradually differentiate their own identities from those of their mothers → process called separation-individuation
mother may disrupt normal separation-individuation by refusing to let go of the child or by too quickly pushing child toward independence
limitation of the theory psych persp
largely based on inferences drawn from behavior and retrospective accounts of adults rather than observation
learning theory persp on PD
focus on maladaptive behaviors rather than disorders of personality
interested in identifying the learning histories and environmental factors that give rise to maladaptive behaviors
childhood experiences shape pattern of maladaptive habits
example: children discouraged from speaking their minds may develop dependent behavior pattern
excessive discipline may lead to OCPD
Millon suggests histrionic personality disorder may be rooted in childhood experiences in which social reinforcers are connected to a child’s appearance and willingness to perform for others
social cog theorists on PD
emphasize the role of reinforcement in explaining origins of antisocial behaviors
Ullman and Krasner propose people with antisocial personalities failed to learn to respond to other people as potential reinforcers
albert bandura on PD
studied observational learning in aggressive behavior
children most likely imitate violent role models who get their way with others by acting aggressively
limitation is grounded in theory rather than observations
family perspectives on PD
evidence links childhood physical or sexual abuse or neglect to development of
personality disorders (BPD and antisocial personality)
splitting may be result of learning to cope with unpredictable and harsh behavior from caregivers
childhood loss of parental figures is also common with BPD
parental overprotection or authoritarianism are implicated in the development of dependent personality traits
OCPD may develop as result of living in strongly moralistic and rigid family environment
Parental rejection or neglect are connected to antisocial personality disorder → may not develop warm feelings of attachment
genetic factors of PD
evidence suggests genetics play roles in antisocial, narcissistic, paranoid, and borderline personality disorders
parents and siblings of people with personality disorders such as antisocial, schizotypal, and borderline types are more likely to be diagnosed with these disorders themselves
personality traits are associated with interactions of genetic factors and life experiences
lack of emotional responsiveness biological factor of PD
people with antisocial personalities can maintain composure in stressful situations → lack of anxiety may explain failure of punishment
most people experience galvanic skin response when anxious, but people with antisocial personalities experienced lower levels
may be underresponsive to threatening stimuli, explaining lack of anxiety
craving for stiumulation model biolog persp on PD
explanation for antisocial personalities lack of emotional response in terms of levels of stimulation necessary to maintain optimum level of arousal
people with antisocial personalities tend to crave excitement and stimulation
may need more stimulation than normal people to maintain interest and function normally
brain abnormalities biolog persp on PD
link BPD and ASPD to dysfunctions in parts of brain involved in regulating emotions, making thoughtful decisions, and restraining impulsive behaviors
prefrontal cortex and limbic system are responsible for these
neurological basis to lack of empathy and concern seen in antisocial personalities
differences in brain structure in amygdala and prefrontal cortex may explain consequences of behavior and impulse control issues
sociocultural persp on PD
lower socioeconomic class associated with antisocial personality disorder
stressors are associated with increased likelihood of child abuse and neglect
childhood maltreatment may lead to cycle of violence → multigenerational
children in poverty may be exposed to negative role models such as drug dealers
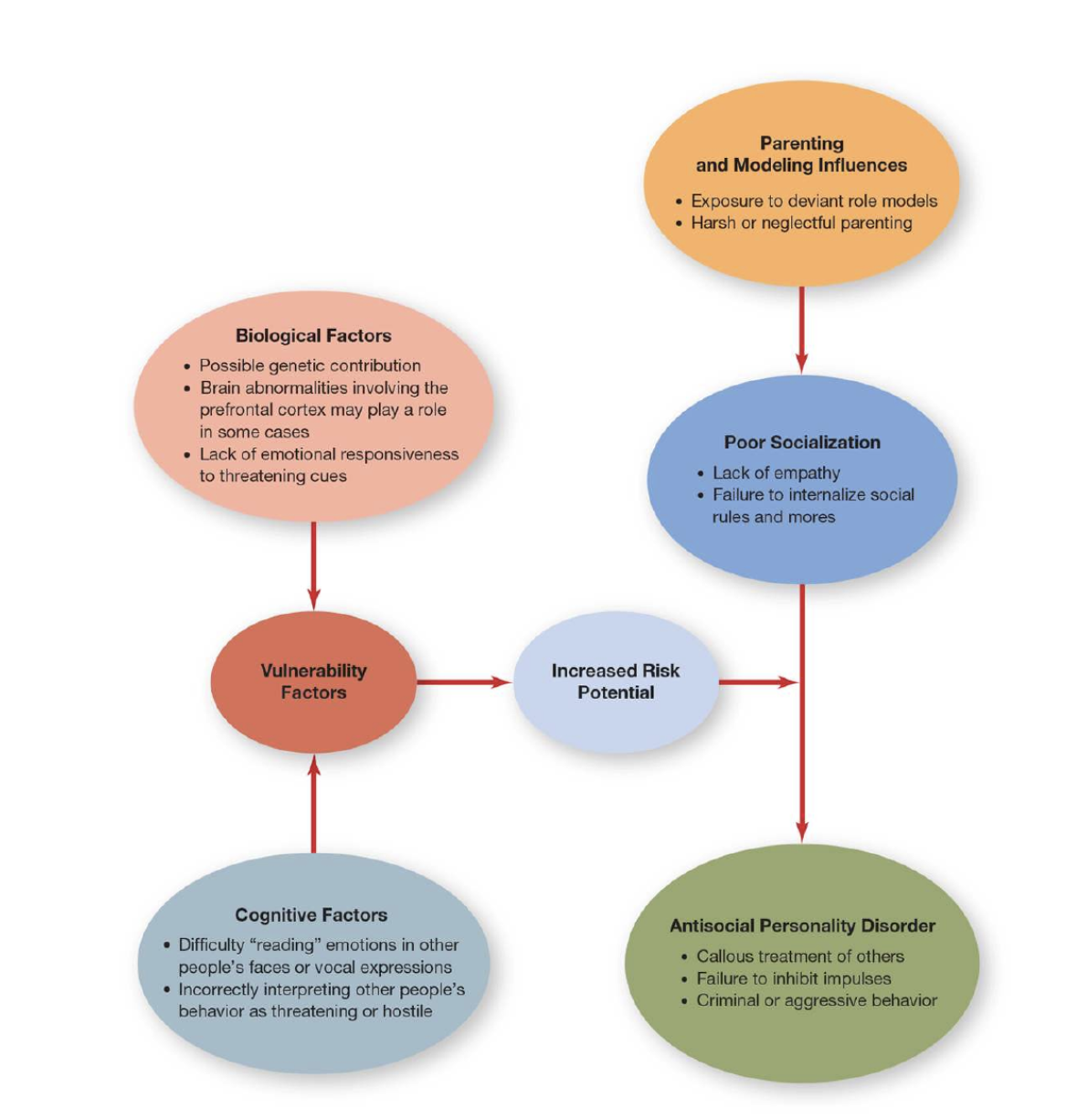
multifactorial model of antisocial personality disorder
psychodynamic approaches treatment of PD
psychodynamic oriented therapies focus on clients awareness of how their behaviors cause problems in their close relationships
therapists take more direct, confrontational approach that addresses the client’s defenses than would be the case in traditional psychoanalysis
with BPD, psychodynamic therapists help clients better understand their own and other people’s emotional responses in the context of their close relationships
cbt approaches for PD
CBT focuses on changing client’s maladaptive behaviors and dysfunctional thought patterns rather than their personality structures
may use behavioral techniques such as modeling and reinforcement to help clients develop more adaptive behaviors
show good results in personality disorders characterized by anxiety
CBT benefits in BPD patents
antisocial adolescents are usually placed in residential programs and includes behavioral treatment
most rely on token economies
Marsha Linehan’s technique called dialectical behavior therapy (DBT) is specifically designed to treat BPD
DBT combines CBT and buddhist mindfulness meditation to help BPD patients accept and tolerate strong negative emotions and learn more adaptive ways of relating to others
DBT also helps adolescence with borderline features and high risk of suicide
DBT helps clients improve relationships with others, develop problem solving skills, and learn more adaptive ways of handling confusing feelings
therapists offer acceptance and support
biological approaches to PD
drug therapy does not directly treat personality disorders
some antidepressants and antianxiety drugs can treat depression and anxiety in people with personality disorders
neurotransmitter activity is implicated in aggressive behavior → SSRIs can help temper feelings of anger and rage
atypical antipsychotics have helped aggressive and self destructive behavior in people with BPD, but effectiveness is mixed
impulse control disorders
characterized by difficulties in controlling or restraining impulsive behavior
kleptomania
IED
pyromania
kleptomania
characterized by repeated acts of compulsive stealing
kleptomania features
objects usually have little value or use to the person
person may give them away, return them secretly, discard them, or keep them hidden
thefts are unmotivated by anger or vengeance
fewer than 1% of population have the disorder
kleptomaniacs experience pleasurable excitement or gratification from stealing
psychodynamic viewed kleptomania as a defense against unconscious penis envy in women and castration anxiety in men
little research on treatment, but behavioral approaches have been successful
Intermittent Explosive Disorder
characterized by repeated episodes of impulsive, uncontrollable aggression in which people strike out at others or destroy property
Intermittent Explosive Disorder features
core feature is impulsive aggression
even minor provocations or perceived insults can lead to aggressive outbursts
people with IED experience tension before outburst and relief afterwards
they feel remorse
links between trauma, violent behaviors and development of IED
links between disorder and serotonin
functioning of prefrontal cortex may be impaired
psychological treatment in form of anger management may help
pyromania
characterized by repeated acts of compulsive fire setting in response to irresistible urges
pyromania features
small percentage of arsonists have pyromania, most set fires out of anger or revenge
fire setting may also be associated with antisocial personality disorder
origins are unknown, but morbid fascination with fire from early age is a sign
setter may feel excitement by watching firefighting event, or feel feelings of empowerment
treatment involves CBT