Chapter 7 -- Femur and Pelvic Girdle
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
69 Terms
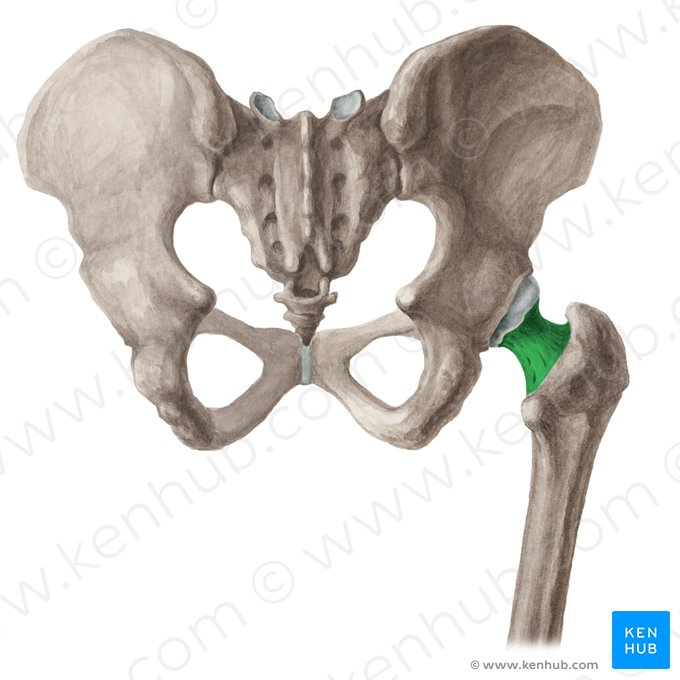
head of femur

neck of femur
common area for injury
femur
longest and strongest bone of the body

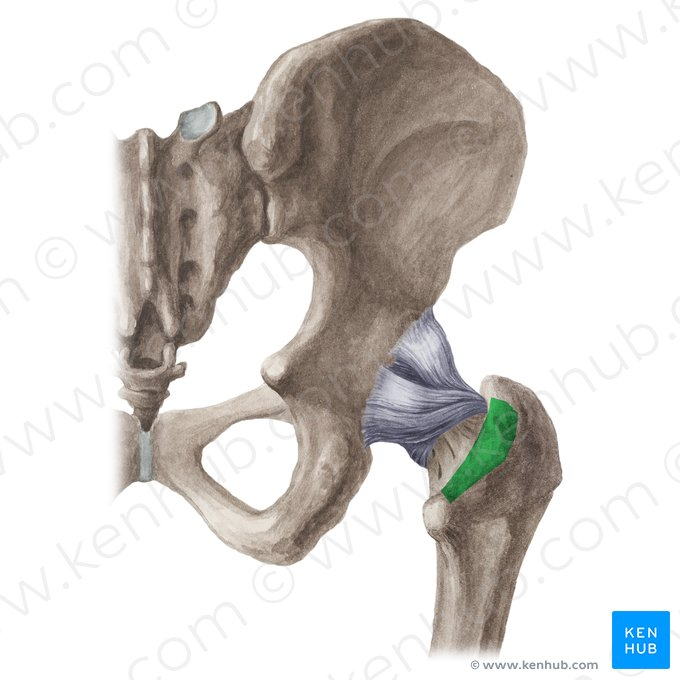
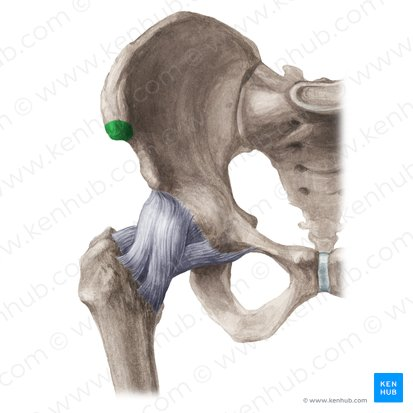
greater trochanter

body or shaft of femur

lesser trochanter
located on posterior side
intertrochanteric crest
located on posterior side
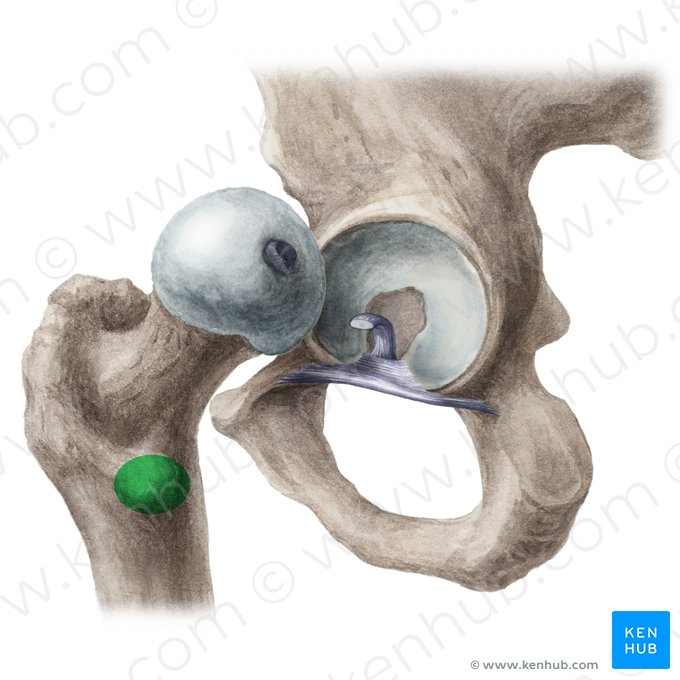
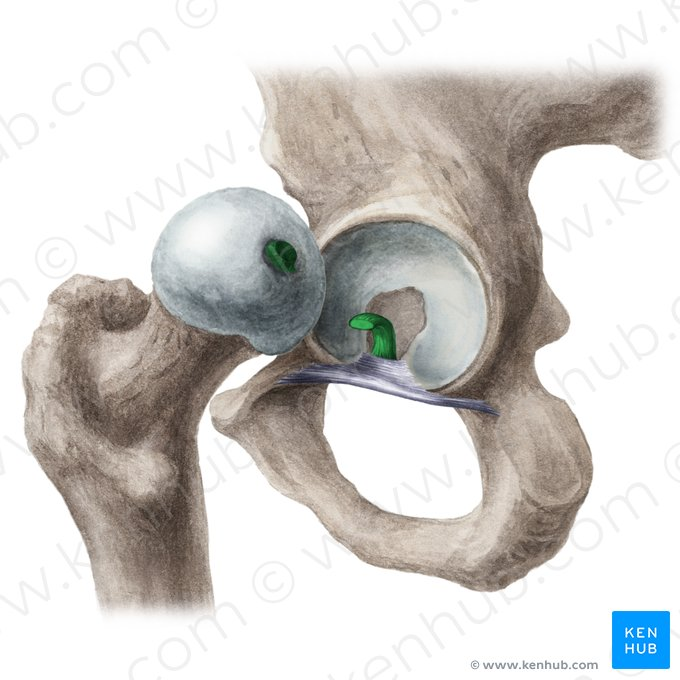
fovea capitis
serves as an attachment for ligaments
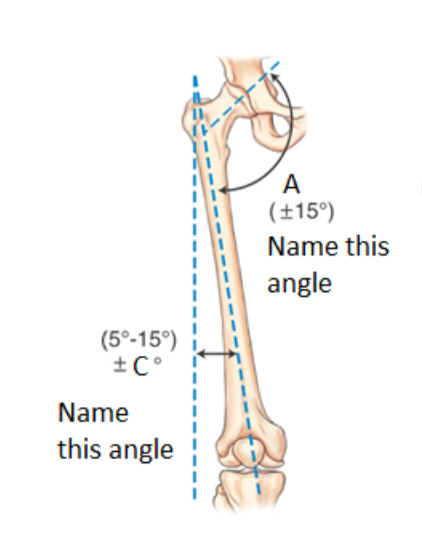
neck to shaft angle (A)
~125o
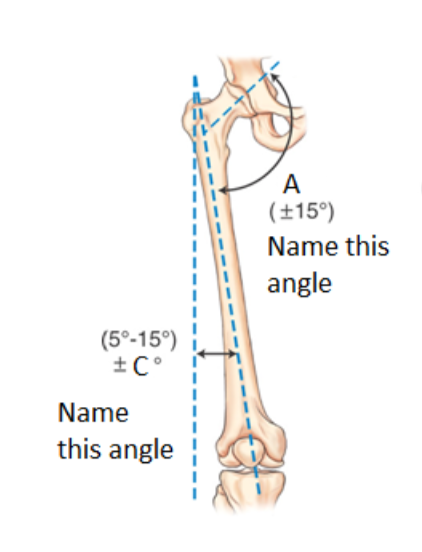
longitudinal angle (C)
~10o
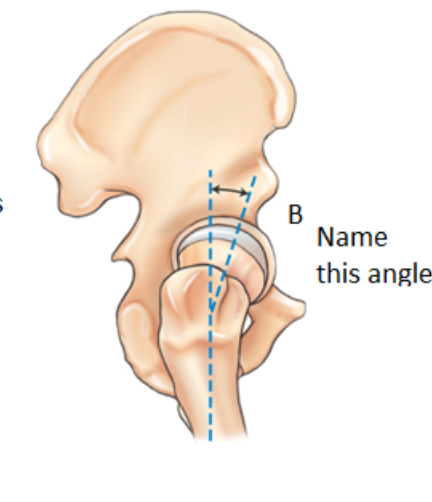
anterior angle (B)
~ 15 to 20o
taller pt angles of proximal femur
femur is more vertical (smaller longitudinal angle) with more of an angle of neck to shaft
shorter pt angles of proximal femur
femur is more medial with more of an longitudinal angle and less of a neck to shaft angle
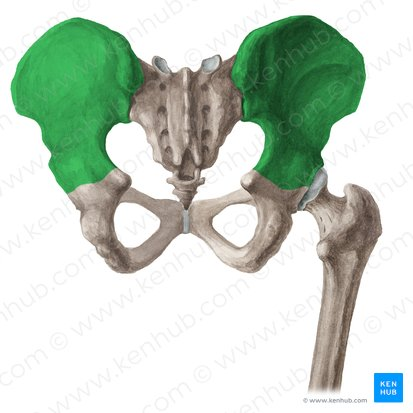
hip bones, ossa coxae, or innominate bones
made up of 3 parts (ilium, pubis, ischium) to form the acetabulum
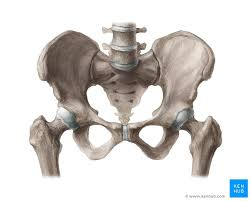
sacrum

coccyx

ilium
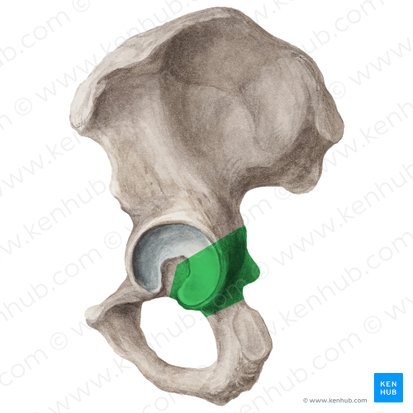
pubis
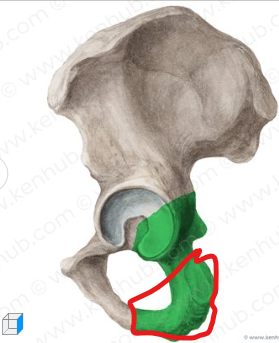
ischium

acetabulum

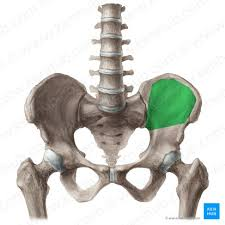
iliac crest
important positioning marker

ala or wing
can help determine rotation
body of pelvis

anterior superior iliac spine (ASIS)
anterior inferior iliac spine

posterior superior iliac spine (PSIS)

posterior inferior iliac spine

upper body of ischium
ramus of ischium

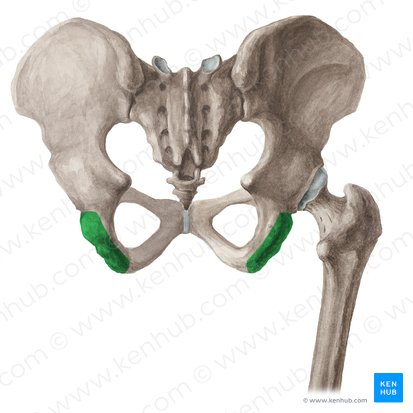
ischial tuberosity
lower body of ischium
lesser sciatic notch

ischial spine

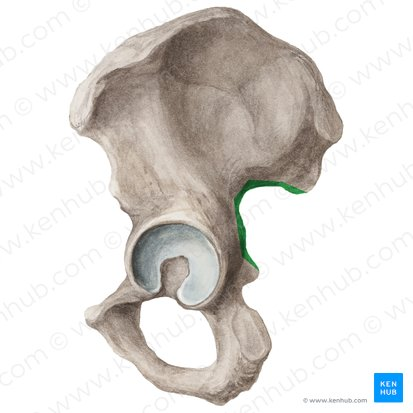
greater sciatic notch
superior ramus

inferior ramus

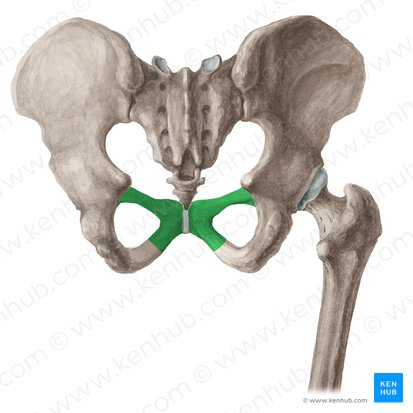
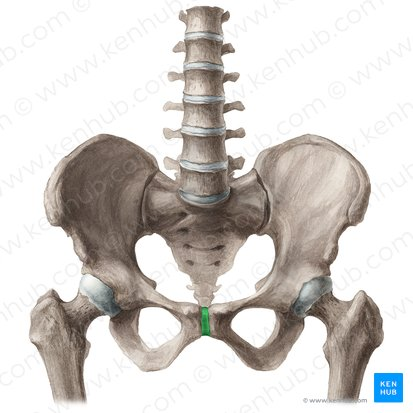
symphysis pubis
obturator foramen (p. foramina)
helps to determine direction of obliquity

body of pubis

bony landmarks of pelvis
crest of ilium, ASIS, symphysis pubis, greater trochanter, ischial tuberosity
greater or false pelvis
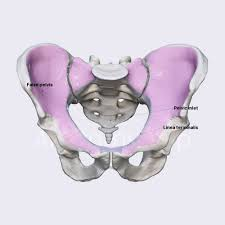
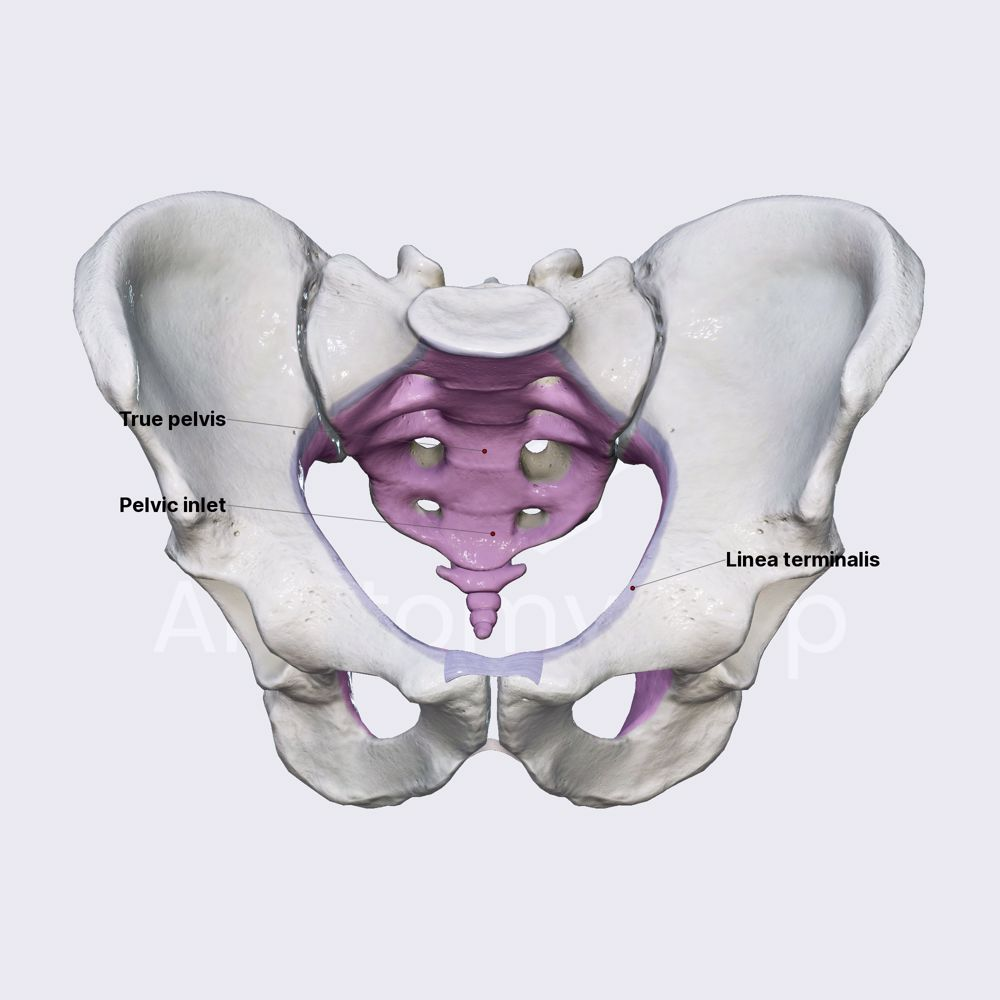
brim or inlet of pelvis

lesser or true pelvis
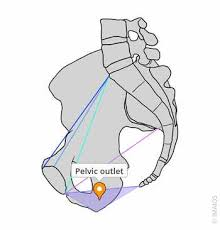
outlet of pelvis
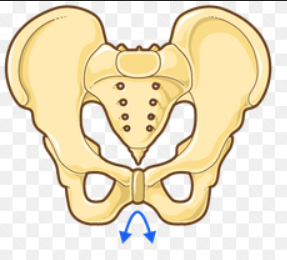
male pelvis
general shape: narrower, deeper, less flared, pelvis inlet is more oval or heart shaped
smaller or narrow angle of pubic arch ( <90o) - acute angle
shape of outlet is smaller
ischial spines have more of a protrusion into pelvic inlet
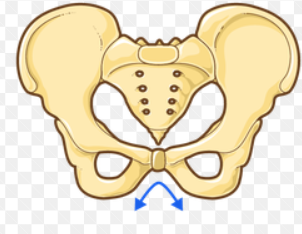
female pelvis
general shape: wider, more shallow, more flared, pelvic inlet rounder
larger or wide angle of pubic arch (>90o) -obtuse angle
shape of inlet is larger
ischial spines have less of a protrusion into pelvic inlet
sacroiliac joint
classification: synovial
mobility type: limited movement
movement type: irregular gliding
symphysis pubis joint
classification: cartilaginous
mobility type: amphiarthrodial
movement type: limited
union of acetabulum joint
classification: cartilaginous
mobility type: synarthrodial (for adults)
movement type: nonmovable
hip joint
classification: synovial
mobility type: diarthrodial
movement type: ball and socket (spherodial)
radiographic positioning considerations
exposure factors: 80 to 90 kVp
consider ages — osteoporosis, etc.
grid may be used (10cm or above)
physical marker required
collimation
hip localization method
to estimate location of hip
head is 1 ½ inches from ASIS to groin crease (right in the center of crease)
neck is 2 ½ inches from head
anatomic position
lesser trochanters visible
external position, relaxed position
lesser trochanters in profile
true AP projection
lesser trochanters not visible
15 to 20 degree internal rotation of lower legs
evidence of hip fracture
asymmetric rotation
affected limb with lesser trochanter in profile
shielding guidelines
male gonadal shielding
small contact shield, top boarder at inferior margin of symphysis pubis
abdominal and pelvic shielding
female gonadal shielding
ovarian shield for hips and proximal femora
positioning for AP (mid and distal femur)
rotate leg 5 degrees internally for true AP
CR perpendicular to femur and midpoint of IR; (lower IR margin should be approximately 2 inches [5cm] below knee joint or light field @ apex of patella)
evaluation criteria for AP (mid and distal femur)
knee joint included
distal two-thirds of distal femur
no rotation
optimal exposure factors
kVp range: 75-85
positioning for lateral (mid and distal) femur
true lateral
CR perpendicular to femur and midpoint of IR; (lower IR margin should be approximately 2 inches [5cm] below knee joint or light field @ apex of patella)
trauma lateromedial (mid and distal) femur
support under affected leg/knee and support foot/ankle in true AP position
place IR on edge against medial aspect pf thigh to include knee, with horizontal x-ray bea, directed from lateral side
evaluation criteria for lateral (mid and distal) femur
knee joint included (minimum)
in true lateral position, medial and lateral femoral condyles superimposed
no rotation
optimal exposure factors
positioning for lateral (mid to proximal) femur
proximal femur not superimposed by opposite limb
true lateral position
CR perpendicular to femur and directed to midpoint of IR (top of light field at ASIS)
suspend breathing during exposure
evaluation criteria for lateral (mid and proximal) femur
proximal one-half to two-thirds of proximal femur, including the hip joint to be shown
in true lateral position with superimposition of the greater and lesser trochanter by the femur exists with only a small part of the trochanters visible on medial side
most of greater should be superimposed by the neck of the femur
optimal exposure factors
kVp range: 75-85
positioning for AP pelvis
separate legs and feet, then internally rotate entire lower limb 15 to 20 degrees (non-trauma)
align midsagittal plane of patient to centerline of table and CR
CR perpendicular/center to IR, directed midway between level of ASIS and the pubic symphysis
approximately 2 inches [5cm] inferior to level of ASIS
suspend breath during exposure
evaluation criteria for AP pelvis
entire pelvis and proximal femora included
no rotation of pelvis evidenced by symmetric appearance of the iliac alae, or wings
lesser trochanters not visible
optimal exposure factors
kVp: 80-90