Ocular injury
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
A.Closed globe injury——→contusion, lamellar laceration, superficial foreign body
B.Open globe injury———> laceration——→ pernetrating, perforating
intraocular foreign body
rupture
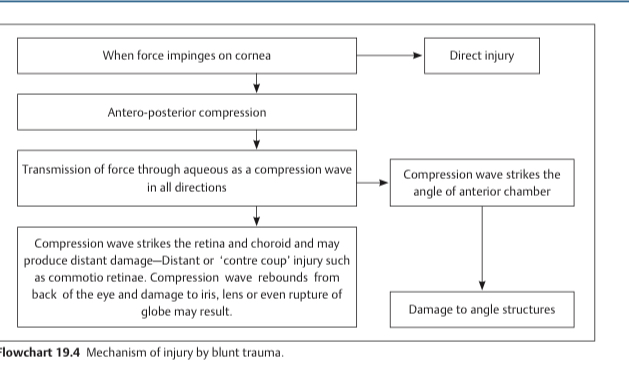
Mechanical injury
Mode of injury
CLosed globe injury clinical features
SIngle full thickness wound without an exit wound caused by a sharp object
Penetrating injury
Two full thickness wounds of the eyewall with both an entry and an exit wound caused by a sharp object.
Perforating eye injury
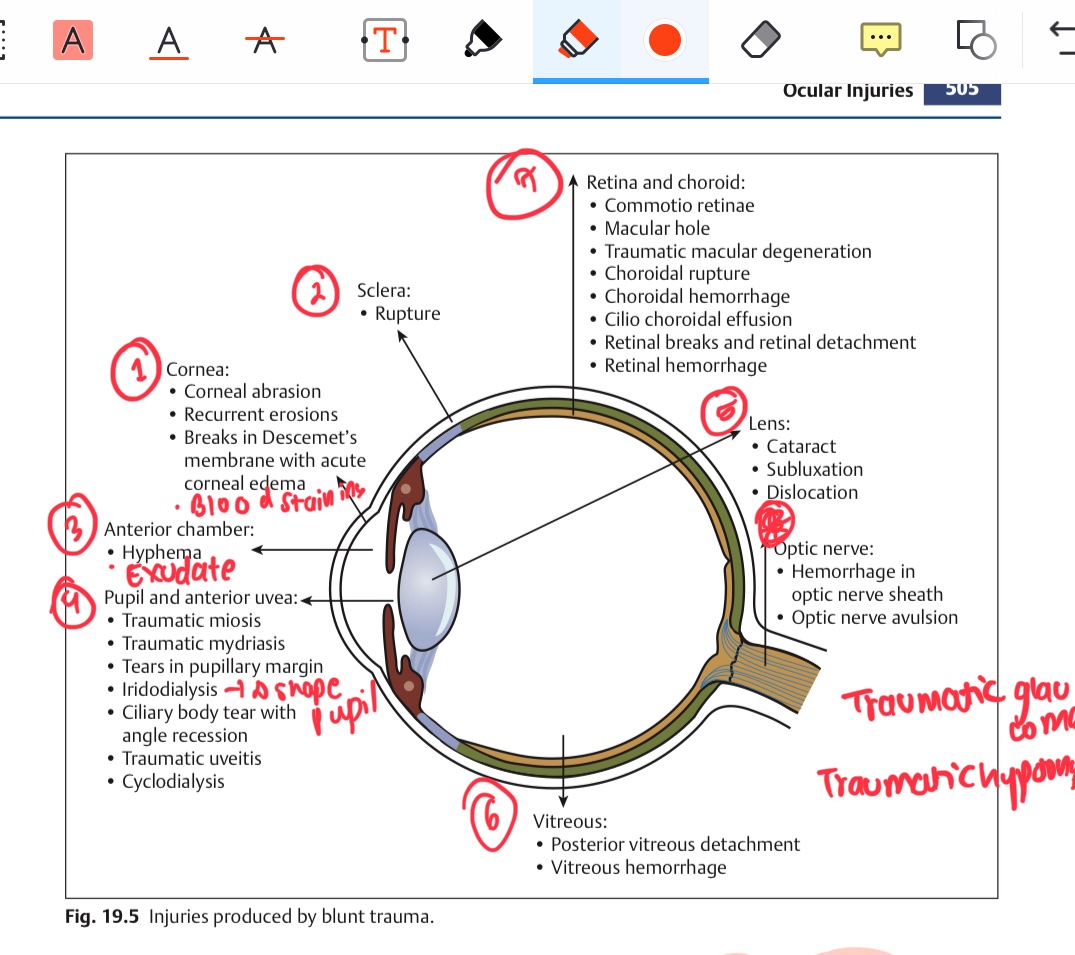
Mechanical effects of the trauma
Introduction of infection
Post traumatic iridocyclitis
sympathetic ophthalmiitis
Effects of penetrating/perforating injury
Cornea-superficial stroma and sometimes deep strona
Conjunctiva-sulcus subtarsalis,fornix, bulbar conjunctiva
Where is extraocular foreign body commonly impacted?
In the conjunctiva-
Removal by a cotton swab or clean handkerchief if present in the lower fornix, sulcus subtrasalis and the canthi if visble
In bulbar conj-hypodermic needle after topical anaesthesia
In the cornea- topical anaethesis, lid seperation using universal speculum -wet cotton swab stick if fails foreign body spud or hypodermic needle, if magnetic strong magnet used, bandage and pad containing antibiotic oinment for 24-48 hrs, antibiotic eye drops are instilled 3-4 times a day for about a wee.
Treatment of extraocular FB
causing inflammatory reaction-
iron steel, copper
causing infection
woood, stone, organic substances
inert fb-gold,glass,silver,plstic, paltinum, lead pellets
Types of intraocular fB
history
ocular examination-visual acquity, wound entry, slit lamp examination, goniosocopy, iop emasurment, fundus exmaination.
plain xray orbit-anteroposterior and lateral views
localizaation of iofb-
radiography": limbalring method- a metallic ring aboout the size of cornea is stitched at the limbus and xray is taken one in anteropost view and threee on lat view where pt is looking up down and straight. iofb localised with relation to the limbal metallic ring.
usg localisation
ct scan -best method
Investigations of IOFB
fb in anterior chamber- direct cornela incision towards the fb 3mm internal to the limbus and over the quadrant directly above the fb.
in the iris tisssu- secto iridectomy containing the fb
in the viterous and retina - viterous- pars planasclerotomy(5mm from the limbus)
intraretinal- sclerotomy adjacent to fb
forceps removal after three pore pars plana vitrectomy for non magnetic fb
Treatment of iofb
Alkalo injury— ammonia
Most common chemical injury
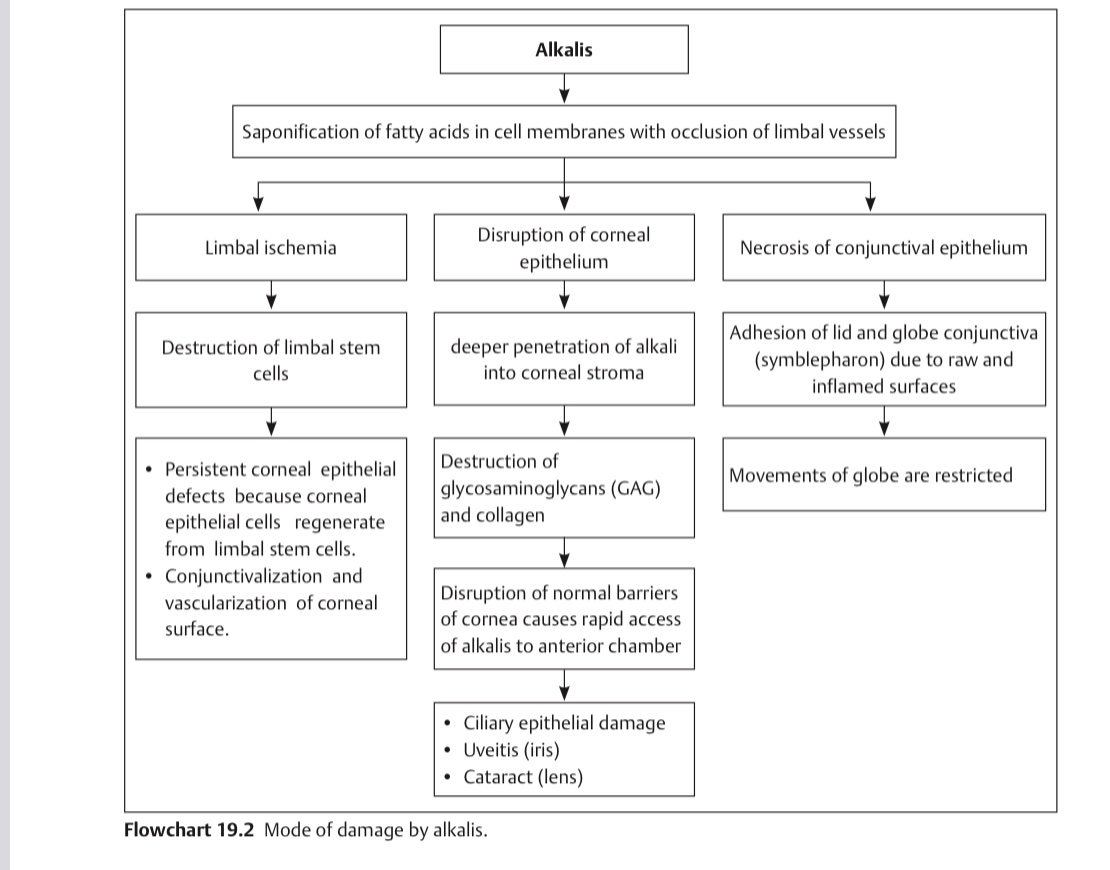
MOA of alkali injury
a. stage of acute ischaemia-
conjunctiva-edematous, red, congested, copious purulent dicharge. cornea-sloughing, oedema, opacification
iris-vary inflamed, iris and pupil body =replaced by granulation tissue.
b. stage of reaparation- conjunctiva and corneal epithelium regenerate, corneal vascualrization, inflammation of the iris subsides.
c. stage of complications- development of symblepharon, corneal ulceration, secondary glaucoma, complicated cataract
Clinical picture of alkali injury
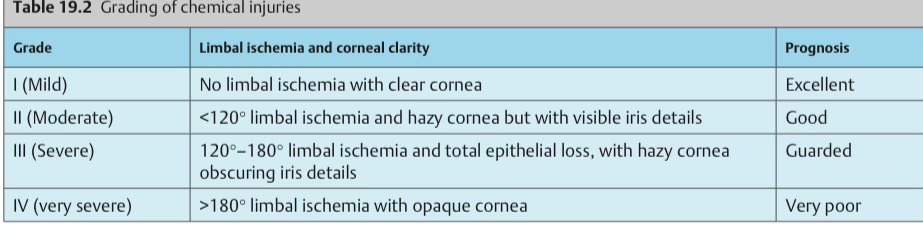
Grading of chemical burns
Irrigation with normal saline or balanced salt solution atleast for 30mins or till ph becomes normal.water can be used if not available
Removal of retained particulate matter
Debridment of necrotic corenal epith for proper epithelixations
Immediate treatment of chemical burns
first week-prophylcatic antibiotic drops, topical cycloplegics, steroids
2md-3rd week-nsaids instead for steroids
after 3rd weeek- steroids again, ascorbic acid, citric acid, tetracyclines, tear substitutes, preservation of symblepharon formation
Subsequent treatment for chemical burns
Limbal stem cell transplantation
Amniotic membrane grafting
COrneal transplantaiton
division of symblepharon
Surgical methods for chemical injuries
FLoor of the orbit and medial wall
posteromedial portion
Blow out fracture most commonly involved wall
Diplopia, enophthalmos, orbital and lid emphysema, infraorbital nerve hopesthesia, tear drop sign
Blow out frracture clincal features
degenerative changes produced by an iron foreign body
rusty oval deposits arranged radially around the ant epith anda capsule of lens—pathognomic
iris-stained greenish and later reddish brown
retina—-pigmentary degeneration
degeneration of TM-secondary open angle glaucoma
Siderosis bulbi
due to copper iofb
kayser-fleischner ring- gilden brown ring due to deposition of copper in the persipheral parts of DM of cornea
Sunflower cataract-posteriot capsule of lens ma deposition
retina-golden plaques at posterior pole reflect light with a metalli sheen
Chalcosis
Management of blow out fracture