APPLIED PK: Exam 1
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
1st gen ASMs
Carbamazepine
Phenytoin (Special MOAs)
Valproic Acid
2nd Gen ASMs
Lamotrigine
Levetiracetam
IV ASMs
Phenytoin (Dilantin)
Fosphenytoin (Cerebryx)
Levetiracetam (Keppra)
Phenytoin dosage (loading + maintenance)
Loading → IV: 20mg/kg (max 1,500 mg)
Maintenance → PO: 300 mg QHS
Fosphenytoin dosage (loading + maintenance)
Loading: 20 PE/kg (max 1,500 mg)
Maintenance: N/A
Levetiracetam dosage (loading + maintenance)
Loading: IV 60 mg/kg (max 4,500 mg)
Maintenance: PO 1,000-1,500 mg BID
_ will precipitate out of solution in 1-2 hours. Must use within 1 hour.
Phenytoin IV
_ is dosed as phenytoin equivalents (PE) to make dosing interchangeable with phenytoin
Fosphenytoin
Which side effect of occurs with IV loading with phenytoin but is much less likely to occur with FOSphenytoin IV loading amd why?
Purple glove syndrome occurs with IV loading with phenytoin, but is much less likely to occur with fosphenytoin loading because propylene glycol does not need to be added to fosphenytoin solution for IV administration
What kind of monitoring is required if phenytoin is intravenously loaded?
Close BP monitoring (hypotension) and ECG monitoring (arrythmias)
Rate of Fosphenytoin IV administraion
150 mg/min
Rate of Phenytoin IV admin
50 mg/min
T/F: Phenytoin administered with tube feeds increases the absorption of phenytoin in the gut
F → reduces
Must stop tube feeds ~_ hours prior and ~_ hours after phenytoin administration
2
What is the total and free therapeutic window for Phenytoin/Fosphenytoin?
Total: 10-20 mg/L
Free: 1-2 mg/L
In normal individuals, phenytoin is _% protein bound
In patients with low protein status there is less <_% protein binding
90
90
T/F: Only bound phenytoin is pharmacologically active
F → Free phenytoin
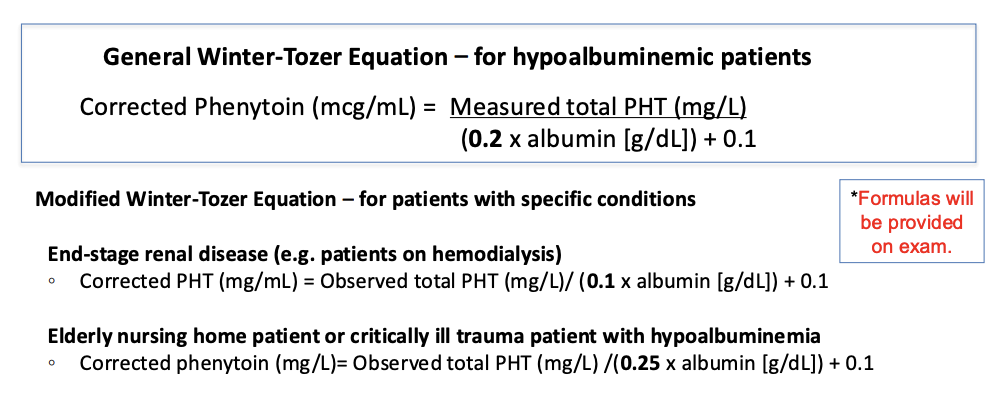
FM was IV loaded with phenytoin and started on an appropriate NG phenytoin maintenance dose. His vitals and labs remain as above. His phenytoin trough level comes back at 9 mg/L. The doctors request your assessment and recommendation regarding his phenytoin therapy. Which Winter-Tozer equation is the most appropriate to use?
Corrected PHT (mg/mL) = Observed total PHT (mg/L)/ (0.1 x albumin [g/dL]) + 0.1
9/(0.1×2.5) + 0.1. = 25.7
ASMs: Broad Spectrum Inducers
Carbamazepine
Phenytoin
Phenobarbital
Selective CYP3A Inducers
Topiramate (TPM) at high doses (>200 mg/day)
Oxcarbazepine (OXC) at high doses (>900-1200 mg/day)
Broad Spectrum Inhibitor
Valproic Acid (VPA)
Inducers increases CYP or UGT enzyme activity
Increases OR decreases: Clearance of other drugs metabolized by CYP or UGT
Increases OR decreases: Levels of other drugs metabolized by CYP or UGT
Increases
Decreases
What is the DDI b/w CBZ + PHT?
CBZ increases clearance of PHT via CYP2C9/2C19 induction
PHT increases clearance of CBZ via CYP2C9/2C19 induction
Can cause subtherapeutic levels → Breakthrough seizures
What is the DDI b/w Lamotrigine + PHT?
PHT increases clearance of LTG via UGT induction
Can cause LTG subtherapeutic levels → Breakthrough seizures
What is the DDI b/w VPA + PHT?
VPA decreases clearance of PHT via CYP inhibition
Causes supra-therapeutic PHT levels → toxicity
What is the DDI b/w VPA + LTG?
VPA decreases clearance of PHT via UGT inhibition
Causes supra-therapeutic PHT levels → toxicity (e.g. rash/SJS)
What ASM requires dose adjustment in patients with renal disease?
Levetiracetam
T/F: Phenytoin has linear elimination.
F → Non-linear elimination
T/F: Elimination rate of phenytoin decreases at higher doses
T
T/F: A small change in PHT dose can lead to a large increase in phenytoin levels
T
Typical phenytoin dose is _mg daily.
Capsules are available in _mg and _mg.
300
30, 100
What your body does to a drug
PK
What the drug does to your body
PD
_ are antifungals used to treat a variety of fungal infections
Triazoles
Anticoagulation (apixaban, aspirin, clopidogrel) Case:
DDI
MOA
PLAN
DDI: Pharmacodynamic
MOA: Decreases risk for thrombosis but all increase bleeding risk when used together
PLAN: D/C Aspirin, Use Clopidogrel b/c data suggests you do not lose efficacy D/C aspirin
Anti-seizure medication (lamotrigine, oral contraceptive pills) Case:
DDI
MOA
PLAN
DDI → PK
MOA → Oral contraceptive pills decrease lamotrigine levels via UGT1A4 induction
PLAN →
This is likely a shared decision making situation that involves seeing what the patient would be comfortable with:
a. Continue as planned and accept the risk of having a breakthrough seizure
b. Increasing lamotrigine dose and still having a risk of breakthrough seizure (if dose increase insufficient) or increasing risk for lamotrigine adverse effects
c. Switching birth control to a medication that is either continuous with no placebo week while adjusting the lamotrigine dose or picking a non-oral contraceptive (e.g., IUD)
d. Measure lamotrigine levels prior to starting Yaz to establish a baseline, then check levels after initiation and titrate lamotrigine dose to achieve
Antimicrobials (posaconazole, rivaroxaban) Case:
DDI
MOA
PLAN
DDI → PK
MOA → Posaconazole is a relatively potent CYP3A4 inhibitor while rivaroxaban is a CYP3A4 substrate → Increased Rivaroxaban lvls → Bleeding
PLAN → Switch one of these agents to minimize the risk of bleeding → May switch Posaconazole w/ Isavuconazole
Anti-seizure medications (topiramate, oral contraceptive pills) Case:
DDI
MOA
PLAN
DDI → PK
MOA → Topiramate induces CYP3A4 metabolism, leading to faster metabolism of the hormones in birth control pills
PLAN → Let the patient know that there is a minor interaction with oral contraceptives and topiramate but at her dose of topiramate it should not be an issue to proceed.
Digoxin reversal agent
Digifab
Digifab indication
Life-threatening situations or large acute ingestions
T/F: Digifab reversibly binds to Digoxin
F → Irreversibly
Digoxin levels cannot be measured for _ after Digifab administration
Weeks
In Digifab, monitor for resolution of [] and [] A.E
Arrhythmias
G.I
Digoxin target levels w/ A.F
<1.2 mcg/L
Digoxin target levels w/ H.F
0.5-0.8 mcg/L
Optimal time to measure Digoxin lvls after administration
At least 6-12 hrs
12-24 hrs: Optimal
Optimal time to measure Digoxin lvls after administration w/o loading dose
3-5 days
T/F: Digifab dose is based on whether digoxin dose is known and timing of toxicity
T
Factors that would increase digoxin levels
Verapamil
Amiodarone
Quinidine
Hypothyroidism
Renal dysfunction (increase Scr.)
Heart failure
Factors that would decrease digoxin levels
Hyperthyrodism (decreased TSH)
Digifab acute unknown dose
10-20 vials and monitor closely
Digifab acute known dose
Digoxin load in mg / 0.5 mg digoxin bound per vial
Digifab chronic unkown dose
6 vials and monitor closely
Digifab chronic known dose
(Digoxin SS level x wt) / 100
Toxic effects of Digoxin are more likely at levels > _mcg/L in all pts
2
What are the toxic S.E of Digoxin?
N/V, Diarrhea
Brady/tachy cardia, EKG changes, hyperkalemia
Visual s/x: Blurred vision, color changes, yellow
Increased mortality in HF pts with levels > _ mcg/L
1
What is Digoxin’s Vd?
2 compartment model
Initially distributes to plasma and other rapidly equilibrating tissues
Then distributes to more slowly equilibrating tissue
Digoxin usual dosing
0.125-0.25 mg
Lidocaine usual dosing
Bolus 1-1.5 mg/kg followed by continous infusion of 1-4 mg/min
Lidocaine PK can be altered by:
Heart failure
Liver dysfunction
Critical illness
Concur
Severe trauma
Concurrent methods
Lidocaine therapeutic concentrations
1-5 mg/L
Minor CNS effects of Lidocaine can be seen at _-_mg/L
3-5
Seizures of Lidocaine have been seen at >_mg/L
9
Calculate bolus dose (LD) using _
Calculate total dose using _
Vi
Vd
Vd of Lidocaine decreased with _
CHF
Severe trauma and critically ill
Higher lidocaine levels!
Vd of Lidocaine increased with _
Chronic liver disease
Lower lidocaine levels!
Lidocaine sampling time
4-8 after therapy
T/F: Lidocaine requires no renal adjustment
T
T/F: Lidocaine has a high first-pass effect
T