Erosion
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
44 Terms
What are the 4 forms of non-carious TSL?
1. attrition - tooth to tooth contacts
2. erosion - progressive loss of dental tissue caused by chemical processes without bacterial involvement
3. abrasion - non tooth wearing of the teeth often habit associated
4. abfraction - fracture of the enamel at the cervical region
What is the definition of dental erosion?
The progressive loss of dental tissue caused by chemical processes without bacterial involvement.
What is the critical Ph?
The pH (5.5 enamel and 6.3 for dentine and 6.7 for cementum) at which a solution is just saturated with respect to a particular solid.
What happens above/below the critical Ph?
Above: the solid can be precipitated as the solution is super saturated
Below: the solution is able to dissolve the solid as it is undersaturated
What does the critical Ph depend upon? (2)
1. depends on the solubility of the solid
2. depends on the concentrations of the relevant mineral constituents of the solution
In the case of dental erosion what are the relevant solids (3) and what is the solutions? (2)
Relevant solids: calcium, phosphate and fluoride
Solution - saliva and food/drink
What is the critical PH for demineralisation to occur for CARIES? why is this constant?
The critical Ph for caries is 5.5. this is constant as the solution is contained within the bacterial biofilm therefore there is no real variation in the mineral concentration of it.
What is the critical Ph for erosion and what does it depend upon?
There is no critical pH for dental erosion as it depends on the saturation of the solution with the relevant solids.
What is the definition of titratable acidity?
The amount of strong base required to neutralise an acidic solution.
What does a high titratable acidity indicate?
The higher the titratable acidity of a drink, the longer it can maintain its low Ph when buffered or diluted.
What is the rough Ph of saliva?
pH 7
What solids does saliva contain and what property does this give it?
It contains calcium and phosphate so has buffering capacity (this capacity depends upon the conc of calcium and phosphate).
What effect does acid exposure to enamel have? 4
1. leads to softening of the surface
2. leads to increased roughness resulting in the apperance of etched enamel
3. continued attacks lead to bulk material loss with remaining surface exhibiting demineralisation
4. partially demineralised layer is more vulnerable to physical forces (brushing grinding etc) leading to loss of tooth volume
What are the 3 steps in the histopathology of erosion?
1 - softening of the enamel (no loss yet)
2 - partial material loss and softening of the underlying surface
3 - significant loss of material through physical forces on the softened enamel
How does the erosion of dentine differ to that of enamel?
The loss of dentine volume occurs faster than in enamel due to lesser mineral content.
What are the 3 main sources of extrinsic acids?
1. dietary
2. medications- vitamin c and aspirin
3. environmental- chemical workers
What is more important in erosion regarding drinks, frequency or quality?
Frequency
What 2 habits associated with drinks lead to more erosion?
1. drinking from feeding bottles
2. frothing and swishing drinks
Why are alcoholic drinks especially bad for erosion? (3)
- typically acidic
- increased likelihood of reflux
- risk of vomitting
What are the 3 main sources of intrinsic acids?
1. GORD- gastro-oesophageal reflux disease
2. eating disorders
3. rumination
What is GORD?
Gastro- oesophageal reflux disease- it is the back flow of gastric acid into the oesophagus
What are the risk factors of GORD? (4)
1. obesity
2. pregnancy
3. high fat diet
4. alcohol
What symptoms do people with GORD present with? (4)
heart burn, bad taste, erosion and dysphagia
What conditions may GORD and regurg of gastric acid be associated with in children? (4)
1. LIVER disease
2. GI disease
3. RESPIRATORY disease
4. NM disorders
What are the two most common eating disorders and what are they often associated with? (2)
Anorexia nervosa and Bulimia nervosa.
These are often associated with other psychiatric disorders eg depression and anxiety.
What are signs of an ED? (9 both physical and behavioural)
- Changes in behaviour
- changes in habits or activities
- weight loss
- withdrawal symptoms
- signs of vomitting
- enlarged SG glands
- loss of menstrual cycle
- stunted growth
- fainting/dizziness
What is the definition of anorexia nervosa?
The failure to eat in the absence of any physical cause - to the extent the patient is 15% below the expected body weight.
What is anorexia nervosa commonly associated with? (4)
- distorted body image
- fear of gaining weight
- excess exercise
- vomitting
What is bulimia nervosa?
It is recurrent episodes of binge eating followed by self induced vomitting.
What is rumination syndrome and what is its cause?
A rare condition in which there is effortless often repetitive regurgitation of recently ingested food into the mouth. This food may be chewed and swallowed again or spat out. There is no known cause but is likely voluntary/learned behaviour.
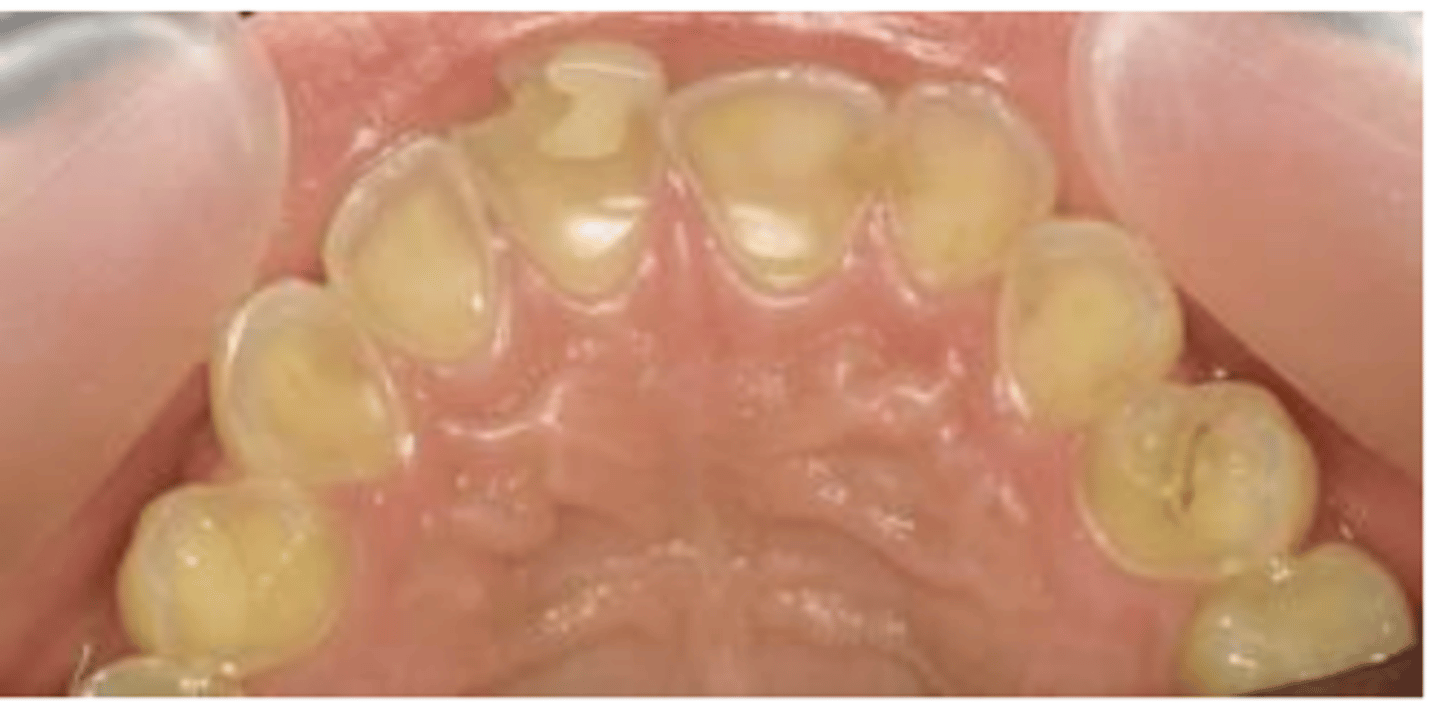
What is the classic presentation of erosion? (2) (what teeth and what surfaces)
1. predominately affects the anterior maxillary teeth and mandibular molars
2. palatal and occlusal surfaces most commonly involved
What are the early signs of erosion? (3)
1. loss of surface features of the teeth eg rounding off incisal edges
2. teeth become smooth and shiny
3. incisal edges become more translucent
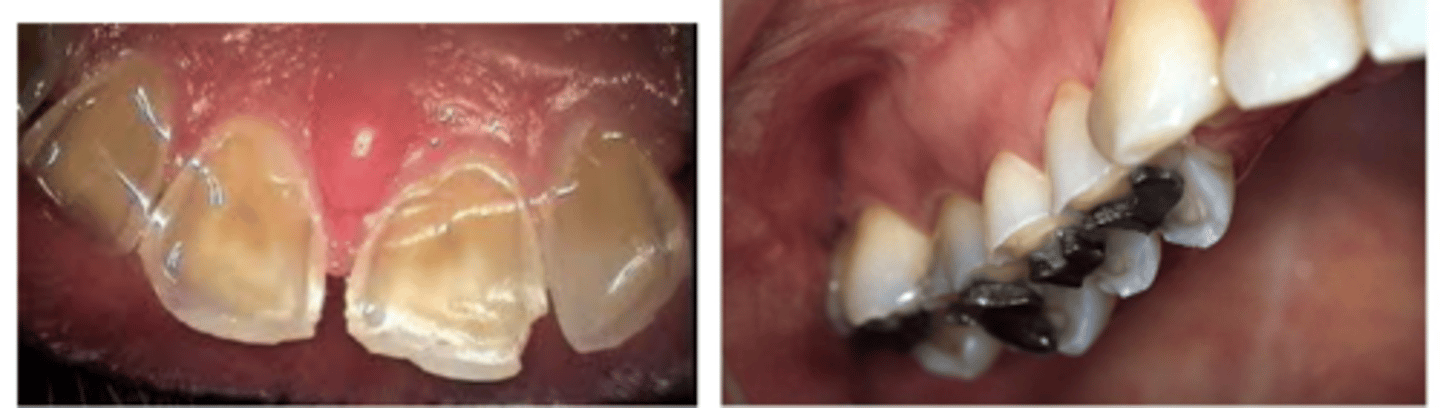
What are the later signs of erosion? (3 anterior 2 posterior and one general)
- thinning and chipping of incisal edges
- chamfer edges at gingival margins
- darkening of teeth (dentine shines through)
- dentine exposed and v sensitive
- proud restorations
- cupping of occlusal surfaces (perimolysis)
What can occur when there is ADVANCED erosion? (3) (more than late erosion)
1. teeth become noticeably shorter as incisal edges lost
2. shine through and exposed pulp
3. pulpal inflammation leading to necrosis and PA pathology
How is erosion different in the primary dentition?
The enamel and dentine are thinner so erosion can progress rapidly.
How can you modify diet to limit erosion? (8)
1. education of the types of food and drinks which can cause erosion
2. limit acid food and drinks to mealtimes
3. chew sugar free gum (saliva increase)
4. finish meal with milk or cheese (calcium and phosphates)
5. don't sip acidic drinks over long times
6. no frothing or swishing acidic drinks
7. no brushing 30 mins after acidic exposure as demineralised enamel more vulnerable to forces
8. rinse mouth after vomiting
How can you desensitise the exposed dentine in erosion? (4)
1. high fluoride mouth wash (0.05% NaF) for 7+
2. high F tooth paste - 2800ppm 10-15 and 5000ppm for 16+
3. fluoride varnish - 22,600ppm
4. tooth moose (CPP-ACP)- casein phosphopeptide amorphous calcium phosphate
How can you monitor erosion? (4)
1. photos
2. study models
3. silicone matrix of worst affected area
4. clinical indexes eg BEWE
When do you provide restorations in erosion cases?
How can you stabilise these teeth?
1. provide restorations once the aetiology is under control
- can stabilise during the monitoring period with direct GIC/compsoite restorations.
What are the treatment objectives when restoring eroded teeth? (4)
1. resolve sensitivity
2. restore missing tooth surface
3. precent further tooth tissue loss
4. maintain balanced occlusion
How would you treat:
- small areas of exposed dentine causing sensitivity
- large areas of exposed dentine (2)
- exposed pulps (2)
in the primary dentition?
1. small area - cover the area with GIC/composite
2. large area - cover with composite crowns (anterior) or SSC for the posterior regions
3. exposed pulps - pulp therapy/extract
How would you treat:
- chipped incisal edges and cusps (2)
- labial surface defects
- palatal surface defects (2)
in perm dentition?
1. chipped edges and cusps - direct or indirect composite
2. labial surfaces - porcelain veneers in adults
3. palatal surfaces - cast nickel-chrome or gold veneers
How can you treat posterior teeth affected by erosion in the perm dentition? (2)
- cast gold/nickel chrome or composite onlays to cover exposed dentine and restore height of the tooth
What is the Dahl effect and how is it used in erosion cases?
Dahl effect - where a localised appliance or restoration is used to increase the interocclusal space for restorations.
This can be used when there is no space interocclusally for a restoration so delicately placer a high restoration or removable Dahl appliance.