Cervical Spine and TMJ Screening
1/106
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
107 Terms
What are the two main clinical decision rules for the neck following trauma?
canadian C-spine rule, and NEXUS low risk rule
What is step 1 of the canadian c-spine rule?
high risk factors (>65, dangerous mechanism, paresthesia) --> image
What is step 2 of canadian c-spine rule?
low risk factors (simple rear end MVC, ability to sit, ambulatory, delayed onset, absence of c-spine tenderness) --> if no, image
What is step 3 of canadian c-spine rule?
rotate neck 45 degrees left and right --> if no, image
What are the criteria for the NEXUS low risk rule?
1. no midline tenderness
2. no focal neuro deficit
3. normal alertness
4. no evidence of intoxication
5. no painful injury that might distract from c-spine
Is CT or radiography preferred for neck trauma?
CT
With radiography, where were the majority of fractures missed?
C1-2 or C7
What are the three types of reference lines in the c-spine?
anterior spinal line, posterior spinal line, spinolaminar line
What is the anterior spinal line?
reference line along margin of anterior aspect of vertebral bodies
What is the posterior spinal line?
reference line along posterior margin of vertebral bodies
What is the spinolaminar line?
reference line along the junction of laminae and spinous processes
What lies between the posterior spinal line and spinolaminar line?
cord/canal
What can you see with an open mouth radiograph view?
odontoid, C1 and C2
What is "swimmers view" on a radiograph?
shoulder flexed above head to allow better visualization of cervicothoracic junction by reducing superimposition of humeral heads and dense shoulder musculature (but CT better, if available)
What are the typical causes of odontoid fractures in young patients?
high impact trauma/MVAs
What are the typical causes of odontoid fractures in older adults?
low energy falls
Why are odontoid fractures more difficult to detect on radiography?
with advanced degenerative changes, it can be hard to discriminate
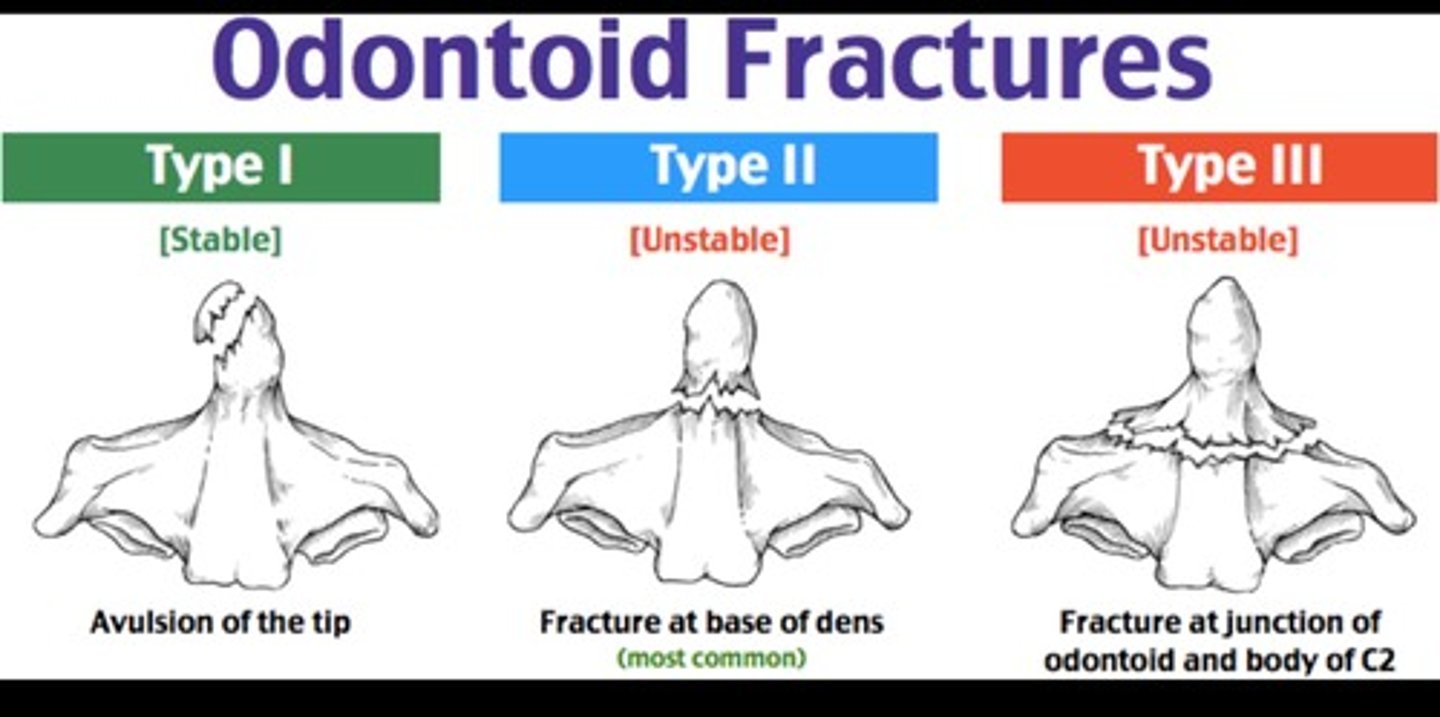
What is the most common type of odontoid fx?
type II (horizontal fracture across base)
What is the primary risk factor for traumatic odontoid fxs in >60 years?
osteoporosis
What worsens the prognosis of odontoid fxs?
neuro deficitis
What is a major predictor of the course after an odontoid fx?
frailty/health status at time of fx
What is Steels Rule of 3rds?
1/3 cord, 1/3 dens, 1/3 free space (free space often spares cord)
In older adults, what are the 3 signs most predictive of injury severity with ground level falls (odontoid fxs)?
1) midline tenderness
2) focal neuro deficit
3) indicators of trauma on head or face
What sheer the odontoid when the head is forced into extension (anterior trauma)?
anterior arch of atlas
What sheer the odontoid when the head is forced into flexion (posterior trauma)?
transverse ligament
When do MRI's have a greater role in acute C-Spine fxs?
if obvious neuro deficit
What condition makes odontoid fractures more common without a precipitating event?
RA
What does odontoid fx in RA mimic?
atlantoaxial subluxation (multidirectional instability)
When is CT vs MRI better to visualize rheumatoid dens?
CT: erosions
MRI: cord or brainstem encroachment
What occurs with atlantoaxial subluxation?
weakening/laxity of transverse ligament, causing C1 to slip forward and decrease room for the cord (commonly asymptomatic)
What is the Anterior Atlanto Dens Interval (AADI)?
distance between anterior arch of C1 and dens of C2
What is the normal anterior atlanto-dens interval (AADI)?
< 3 mm
What happens to the anterior atlanto-dens interval with flexion vs extension?
flexion --> increases, extension --> decreases
Who is more at risk for anterior atlanto subluxation?
1. RA has last >10 years
2. disease is erosive
3. severe RA
In patients that are high risk for A-A subluxation, what may be prudent to include in exam?
neuro exam (hyper-reflexia, plantar response, gait disturbance, Hoffmans)
What exercises should be avoided in patients w/ unstable AA?
isometric extension and retraction
How is the posterior atlanto dens interval effected in flexion vs extension?
flexion = decreases, extension = increases
How do DMARDS effect A-A subluxation?
prevents development of new instability but does not halt established lesion progression
What is progression of instability/subluxation (with RA) predicted by?
1. pre-existing subaxial instability (lower)
2. NOT taking biologic agents
Does peripheral joint involvement increase or decrease risk of cervical subluxation?
increase
What are the risk factors for RA related sublization?
- lower BMD
- female
- younger age of onset
- steroid Rx
- hand or foot joint erosions
- increased markers of disease activity (c-reactive protein)
- previous joint surgery
What reduces risk for RA related subluxation?
- less severe peripheral joint involvement
- no need for corticosteroid admin
- no need for peripheral joint surgery
- lower c-reactive protein levels
Is atlantoaxial impaction/basilar invagination more or less severe than subluxation?
more severe
What are the symptoms of basilar invagination?
- neck pain
- cough headache
- lower cranial nerve palsies
- corticospinal signs (UMN)
- hydrocephalus
- cerebellar dysfunction
- syringomyelia
- syringobulbia
What conditions may basilar invagination accompany?
- chiari malformation
- down syndrome
- klippel feil syndrome
- osteogenesis imperfecta
- RA
- Pagets disease
Is basilar invagination a good or poor prognosis?
poor (neuro involvement)
What is the most common symptom of craniovertebral instability?
neck pain!! (followed by: restricted neck movement, limb weakness, paresthesia, bladder/bowel)
What disorders put a patient at a higher risk for instability?
connective tissue disorders
What are symptoms of clinical instability?
- Neck fatigue ("I can't hold my head up.")
- Better with a collar or external support
- Feeling like the neck is unstable
- Frequent cracking/self-manipulation
- Sudden sharp pain with movement
- Poor coordination
- Jerky or abnormal neck movement
What features were consistently positive in the Cervical Instability Tool?
- intolerance to static posture
- better with external support/unloaded
- muscles feel tight/stiff
- fatigue and inability to hold head up
What is Lhermitte's signs?
electric shock sensation down spine with neck flexion (suggests spinal cord involvement)
Why have flexion/extension radiographs fallen out of favor?
do not change clinical management (MRI better)
What degenerative changes is MRI most sensitive in detecting?
- disc height loss
- loss of signal from dessication
- annular fissures
- osteophytes
- end plate changes
- herniation
What degenerative changes are commonly associated with severe neck pain?
kyphosis curvature, spondylolisthesis and annular tear
What degenerative changes are commonly associated with persistent neck pain?
kyphosis curvature, spondylolisthesis, endplate changes
What is Klippel-Feil Syndrome (KFS)?
congenital fusion of 1 segment or more (most common at C2-5) --> adjacent segments have to move more
What is the most frequent finding with Klippel-Feil Syndrome (KFS)?
limited CROM
What is Sprengels deformity?
Congenital elevation of the scapula associated with Klippel-Feil Syndrome (KFS)
What is the most common location of spondylotic radiculopathy?
C5-6 and C6-7
What is the most common cause of cervical radiculopathy in older adults?
bony origin (osteophytes); disc herniations in younger
What is the modality of choice for diagnosis of radiculopathy?
MRI
What is the average regression timeline of cervical disc herniations?
9 months
What is the clinical prediction rule for radiculopathy?
- ULTT (medial)
- ipsi rotation <60
- reduction of symptoms with traction
- spurlings
*** all 4 = 90% post-test probability
What was the most specific finding for radiculopathy?
diminished reflexes
With motion, which levels have the greatest foraminal changes?
C3/4 and C4/5 (less at 5/6 and 6/7)
Compared to MRI, what has 97% specificity for cervical radiculopathy diagnosis?
ULTT (especially median)
What is the typical population of cervical spondylotic myelopathy?
men, age 64+ (associated with smoking and diabetes)
What is the most common level of cervical myelopathy?
multilevel with C5/6
What are the symptoms of cervical myelopathy?
weakness, numbness in hands and other paresthesias, loss of dexterity, incontinence (later), sensory disturbances
What are the signs of cervical myelopathy?
-motor defects
-thenar atrophy
-Lhermittes
-spasticity of LE
-flaccid paralysis of UE
-impaired gait
-manual dexterity loss
-hyper-reflexia
-babinski and hoffmanns reflexes
-inverted brachioradialis
-ankle myoclonus
-romberg sign
-hand numbness
What is the most common early sign of cervical myelopathy?
UE sensory symptoms/hand and motor function
What are the most common outcome measure predictors of cervical cord compression?
- 6 m walk time
- shorter step length at max pace
- 5xSTS
- SLS
- slower steps
What is the 15 sec grip and release test?
closing hand to grasp then opening to extend fingers as rapidly as possible (normal = 25-30 reps)
*** slows with myelopathy
What is the finger escape test?
patient holds fingers extended and adducted for 30 sec (postiive = abd or flexion of ulnar side digits)
What is cervical spondylotic myelopathy?
narrowing of spinal canal with cord compression - often from osteophytes at disc/vertebral junction
What were the contributors to loss of space for cord?
1. degenerative multilevel disc pathology (89.7%)
2. enlargement of ligamentum flavum (56.8%)
3. ossification of PLL (10.5%)
Why is cervical spondylotic myelopathy often overlooked or misattributed?
false negative tests are routine (21% of patients awaiting surgery did not show a single positive test)
What reflex changes might you get in a cervical myelopathy exam?
biceps/brachialis --> finger flexion
triceps --> elbow flexion
What is the DOWN Questionnaire for cervical myelopathy?
1. Dropping things
2. Off balance
3. Weakness
4. Numbness or tingling
In ACR appropriateness criteria, which imaging modality is preferred for cercical myelopathy/stenosis?
MRI (CT Myelopathy when contraindicated)
What is the prognosis if signal changes occur in spinal cord?
very bad --> usually permanent deficits
What type of MRI is the most sensitive for myelopathy?
diffusion tensor imaging (DTI)
Other than the cord, where else can cervical myelopathy be observed?
higher center atrophy observed in primary somatosensory cortex, primary motor cortex, somatosensory association cortex, supplementary motor area
What are the benefits of MRI vs CT Myelegram?
MRI: assessment WITHIN neural elements, spatial relationships around neural elements, non invasive
CT (plan B): contrasts allows assessment of spatial relationships
Who is Posterior Longitudinal Ligament ossification more common in?
asian men in 5/6th decade
What is the most common presentation of PLL ossification?
cervical myelopathy (often clinically silent/not characterized by pain)`
What imaging modality is best for ossification?
CT
What ligamentous structures are often involved with whiplash associated disorder?
- alar lig
- transverse lig
- tectorial membrane
- post O-A membrane
What significance difference can be seeing on MRI with whiplash associated disorder?
muscle composition of deep cervical muscles (increase in fatty infiltrate and CSA)
How is functional score correlated with increased fatty infiltrate in WAD?
lower functional score (quality over quantity with muscle)
Why do those with ankylosing spondylitis and down syndrome have a greater need for imaging with WAD?
greater propensity for fractures and instability
What is Os Odontoideum?
Failure of the base of the dens to form an osseous union with C2 body (small association with down syndrome)
What is Dens hypoplasia?
odontoid not large enough to be secured by transverse ligament (leads to instability; association with down syndrome)
What is adjacent segment disease?
Degeneration at levels adjacent to a spinal fusion due to additional stress (segment below > segment above)
What is a cervical rib?
extension of C7 transverse process that is typically an incidental finding
What can a cervical rib increase the risk for?
brachial plexus injury > thoracic outlet
Why is a pancoast tumor often overlooked?
presents like an MSK condition
What is the most common complaint with pancoast tumor?
shoulder pain, usually medial scapular (also back and chest)
What are the signs of a pancoast tumor?
- negative spurling (CANT REPRODUCE)
- decrease tricep strength/reflex
- decrease grip strength
- positive ULTT
- sensory disturbance medial arm - ulnar distribution
- HORNERS
What are the symptoms of Horners Syndrome?
- miosis (ipsi pupil constriction)
- ptosis (drooping eyelid
- facial anhidrosis and flushing
- anisocoria (asymmetrical pupils)
- apparent enopthalmos (sunken eye look)
- sympathetic loss