Psychology of Aging: Exam 2 Review
1/134
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
135 Terms
Neuroscience
The study of the brain
Neuroimaging
Images of the brain; used for understanding normal vs abnormal functioning
Structural neuroimaging
Highly detailed anatomical features of the brain
What are two common types of structural neuroimaging?
Computed tomography (CT) and magnetic resonance imaging (MRI)
Computed tomography (CT)
-Takes only 1 minute!
Used to view structures and bones
Magnetic resonance imaging (MRI)
-Takes 15 minutes; it does NOT include radiation.
Used to view tissue and soft structures
Functional neuroimaging
Indicates brain activity using color
What are some common types of functional neuroimaging?
Positron emission tomography (PET) and functional magnetic resonance imaging (fMRI)
Positron emission tomography (PET)
How the body's organs are working
Functional magnetic resonance imaging (fMRI)
Brain activity via blood flow
Neuropsychological perspective
Compares healthy brains to those with pathological disorders
Neurocorrelational perspective
Links measures of cognitive performance to brain structures or functions
Activation imaging
Links functional brain activity with cognitive behavioral data
Why is the fMRI so important in activation imaging?
It can be used as evidence for compensatory changes, such as neuroplasticity.
Brain
The most complex organ in your body
Neurons
Main unit of the nervous system; there are billions of them inside your body.
They are cells that receive, process, and send information.
Dendrites
Receive signals from other neurons
Axons
Contains neurofibers and carries information
Terminal branches
Releases neurotransmitters
How does information in the brain travel?
Information travels from one neuron to another.
Neurotransmitters
Chemicals that travel across the synapse and are received by a neighboring neuron
Synapse
Space that exists between the neurons
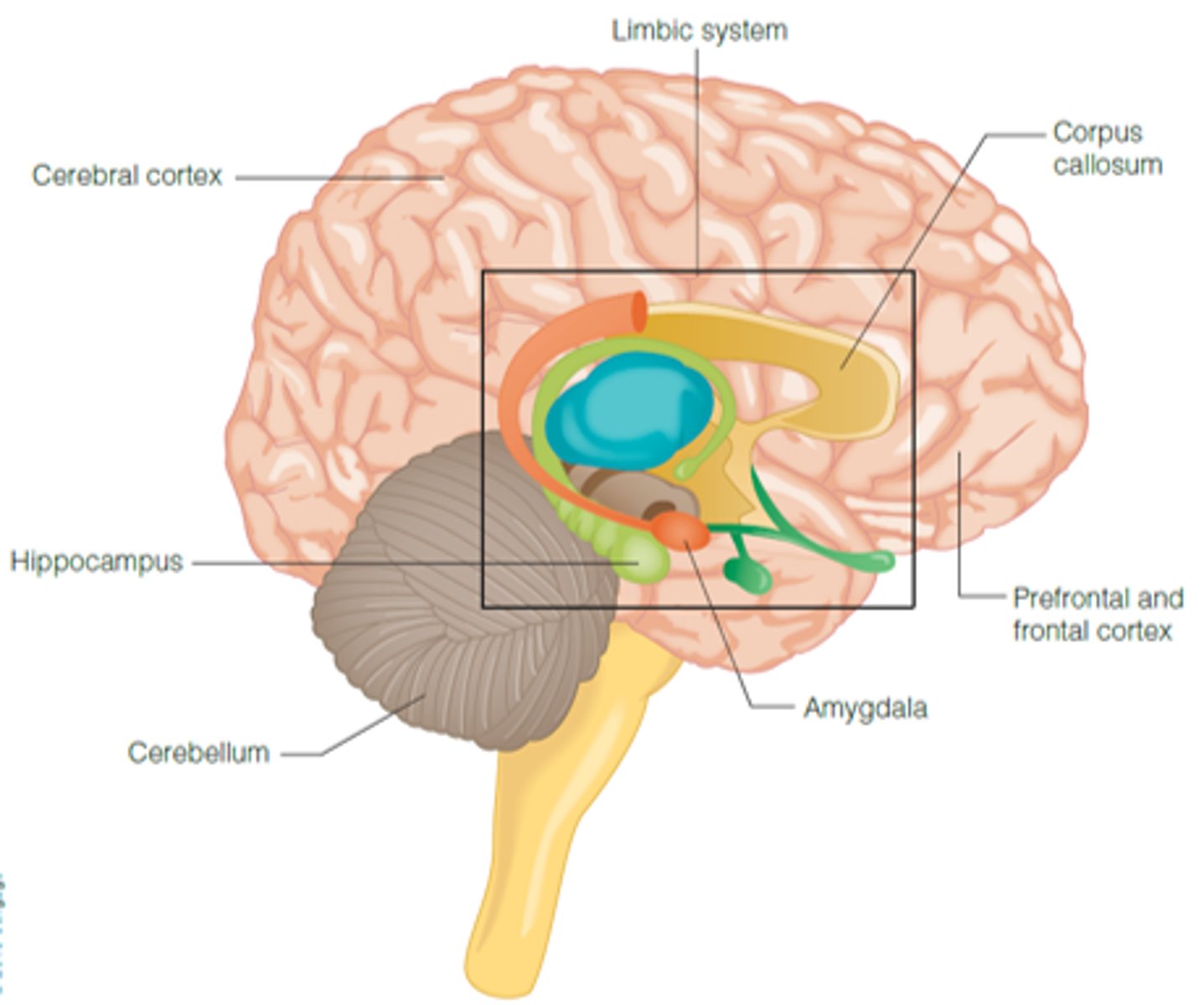
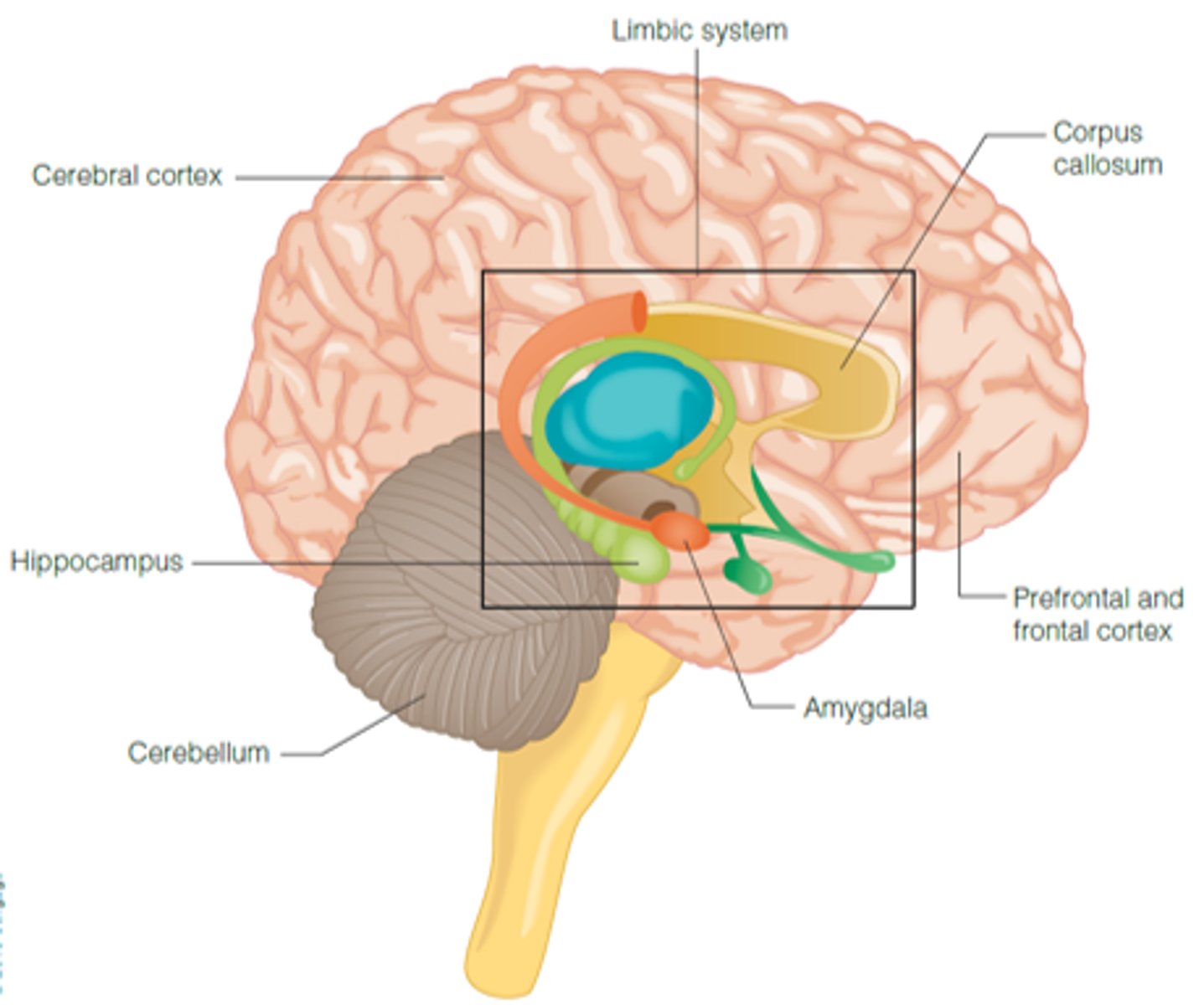
Neuroanatomy
Study of the structure of the brain, including the cerebral cortex, prefrontal, and frontal cortices.
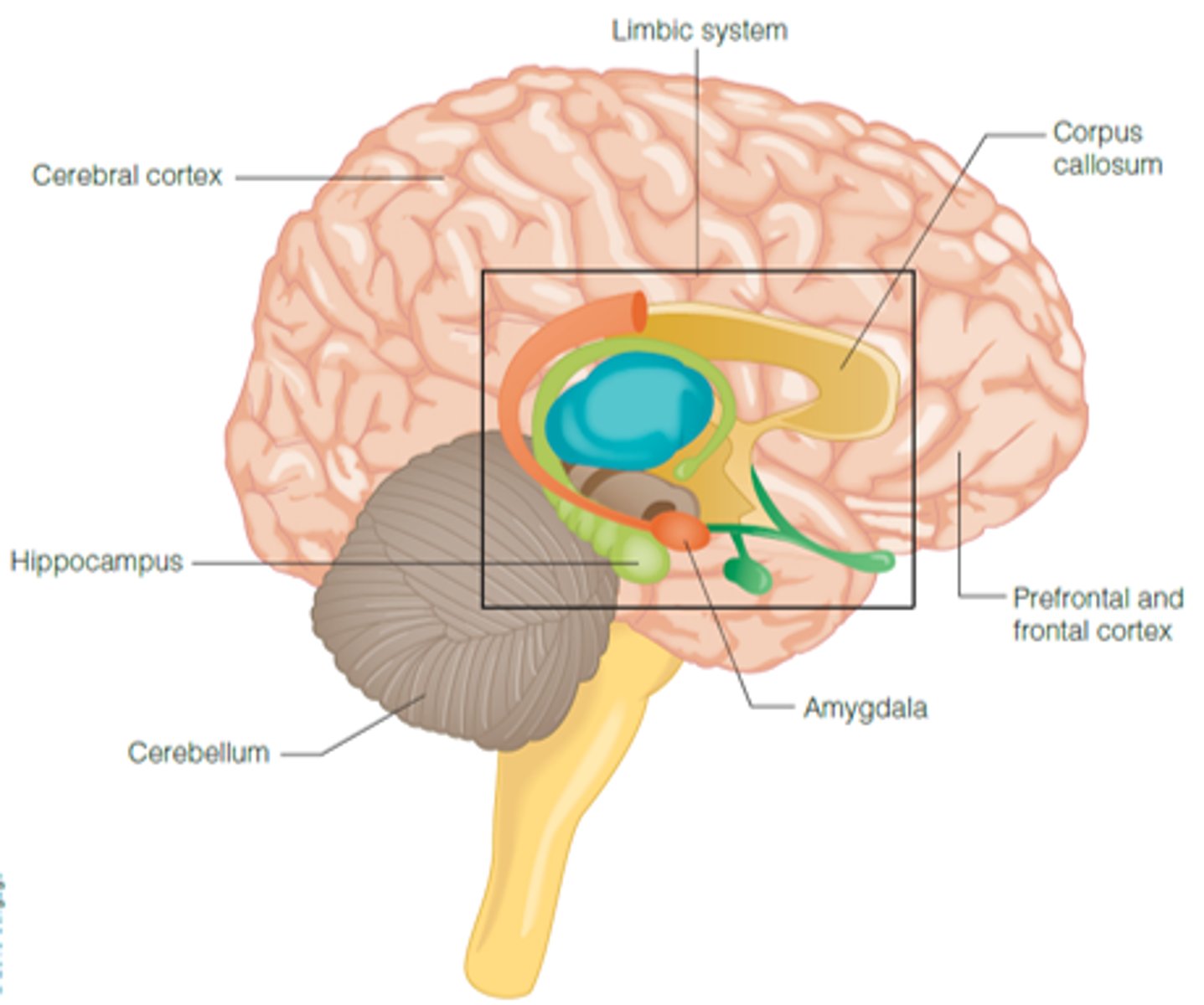
Cerebral cortex
Outermost part: contains left and right hemispheres; connected by the corpus callosum (bundle of neurons)
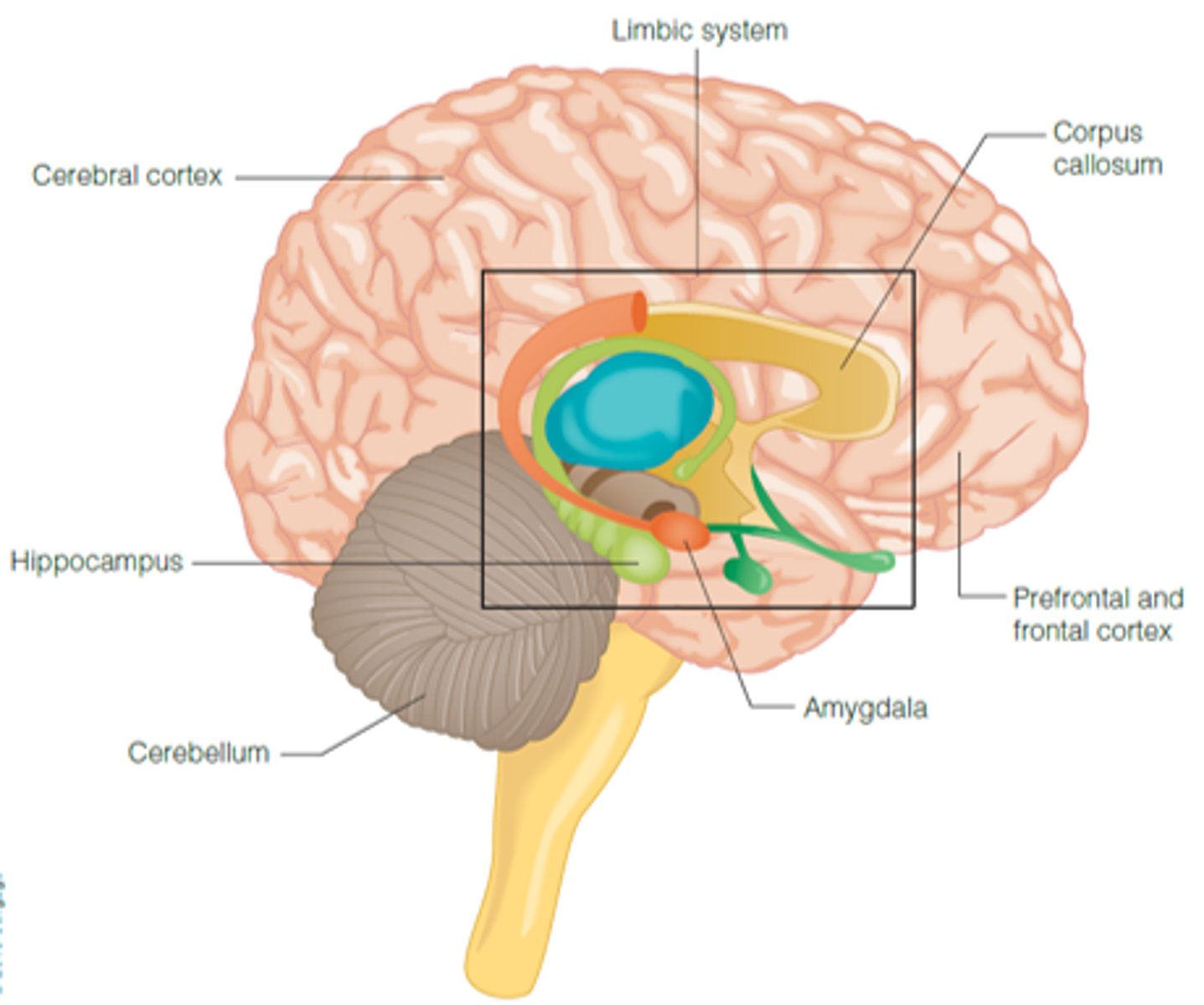
Prefrontal and frontal cortex
Involved in higher-order executive function
-Continues to develop through our mid-20's
What do myelination patterns and the pruning of gray matter tell us about aging in women?
Women historically develop faster to find stable, protective mates.
Cerebellum
Controls equilibrium and coordination of motor movements
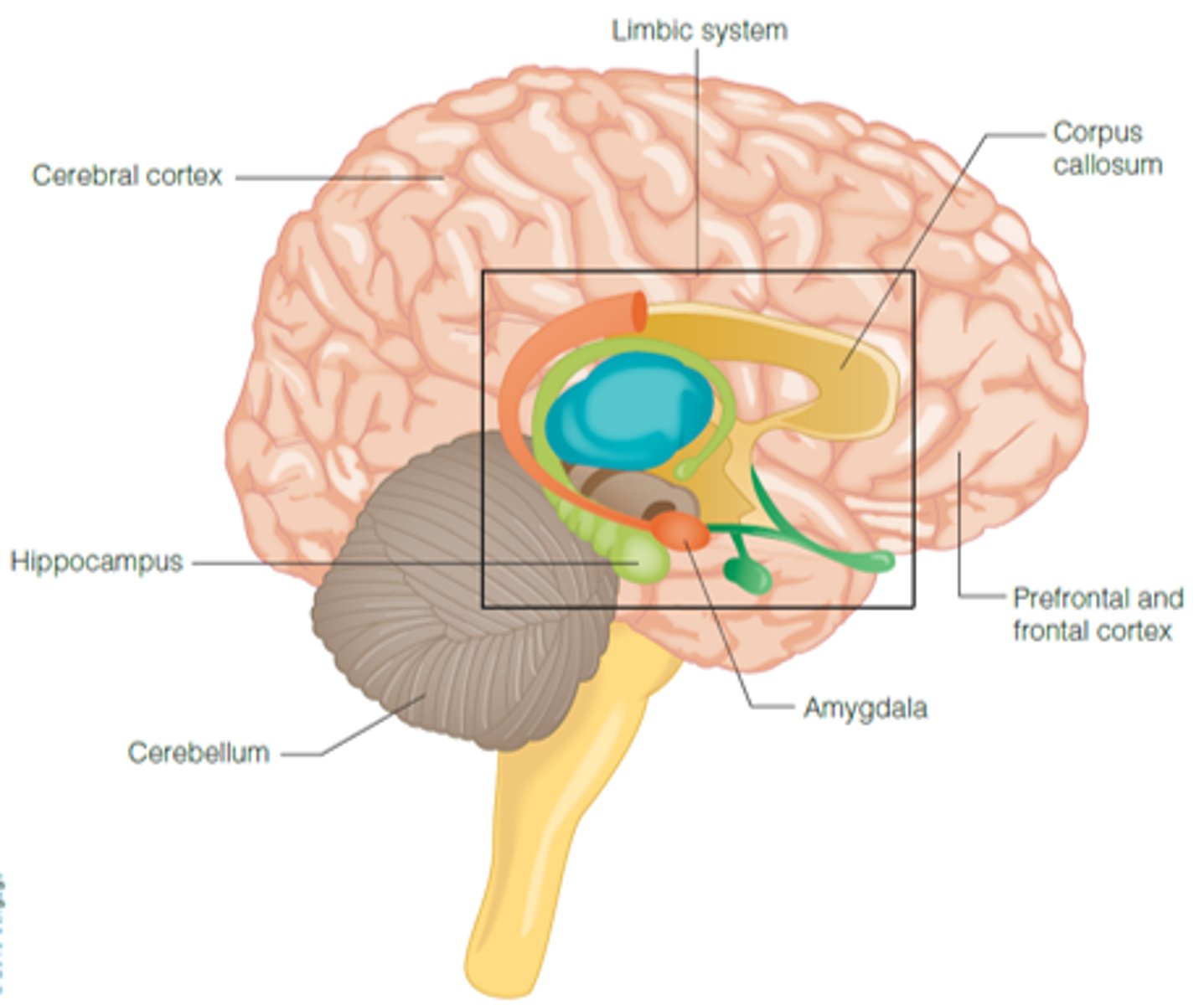
Limbic system
Emotion, motivation, long-term memory
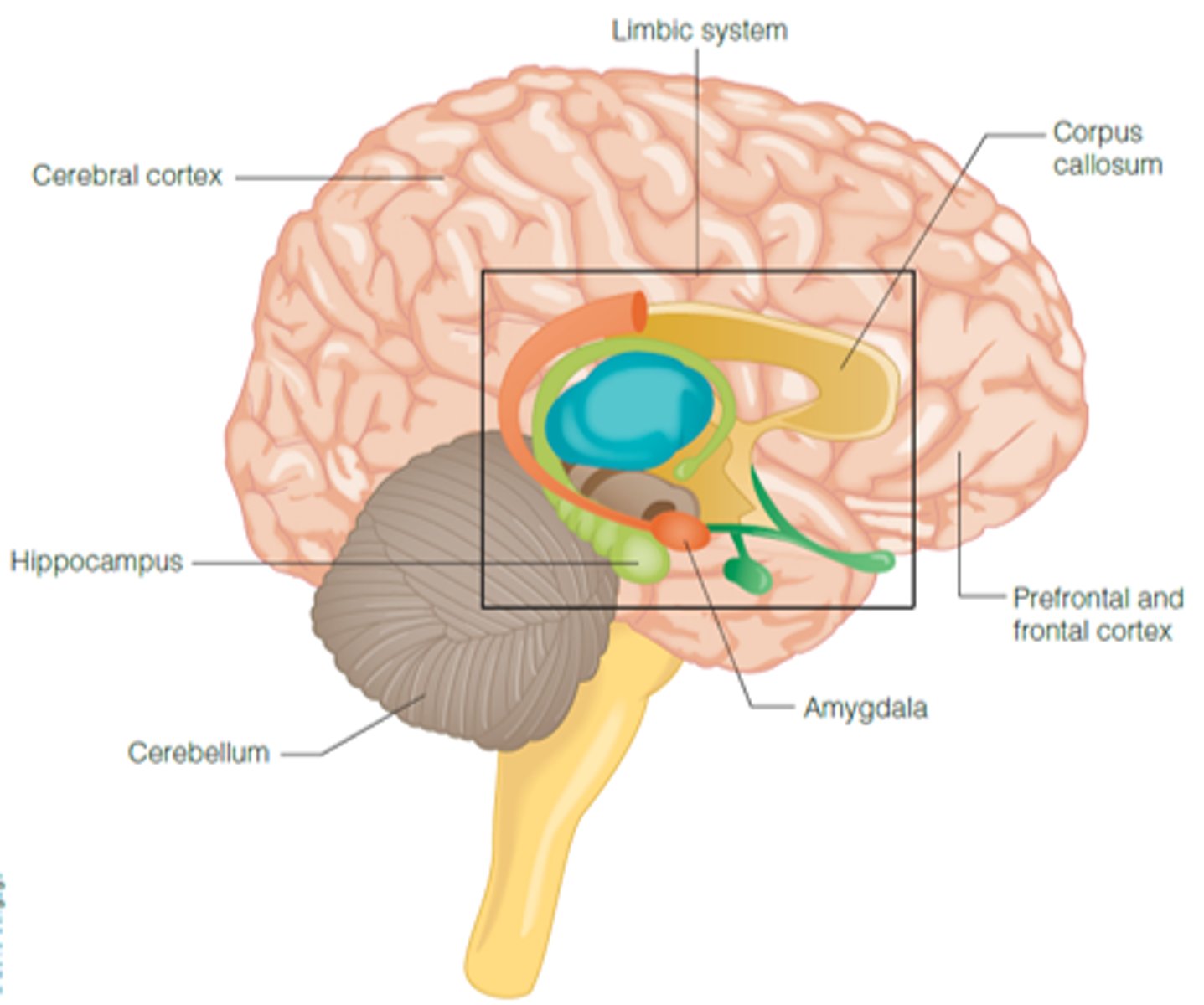
Amygdala
Main structure for emotion
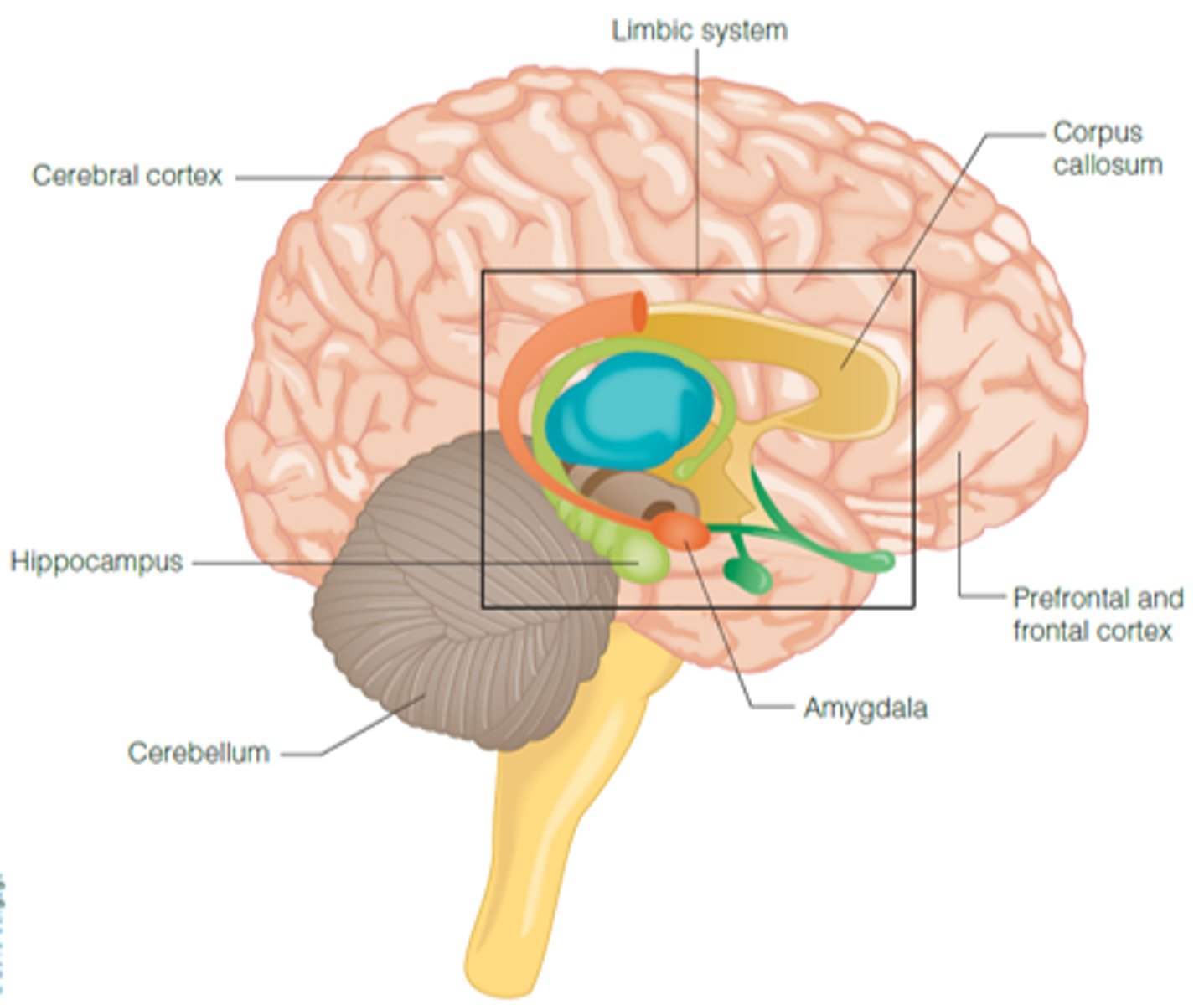
Hippocampus
Main structure for memory
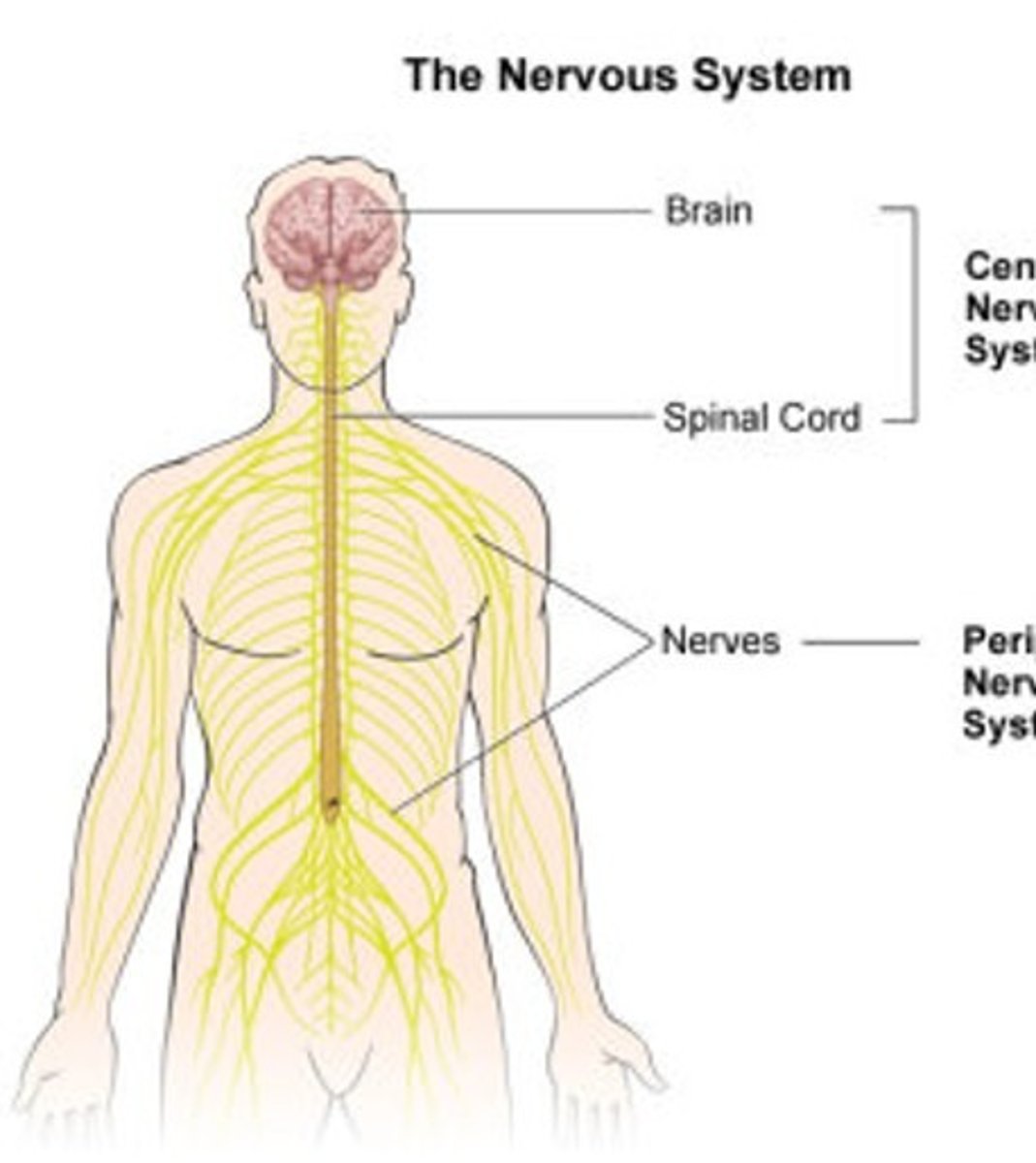
Central Nervous System (CNS)
Brain and spinal cord
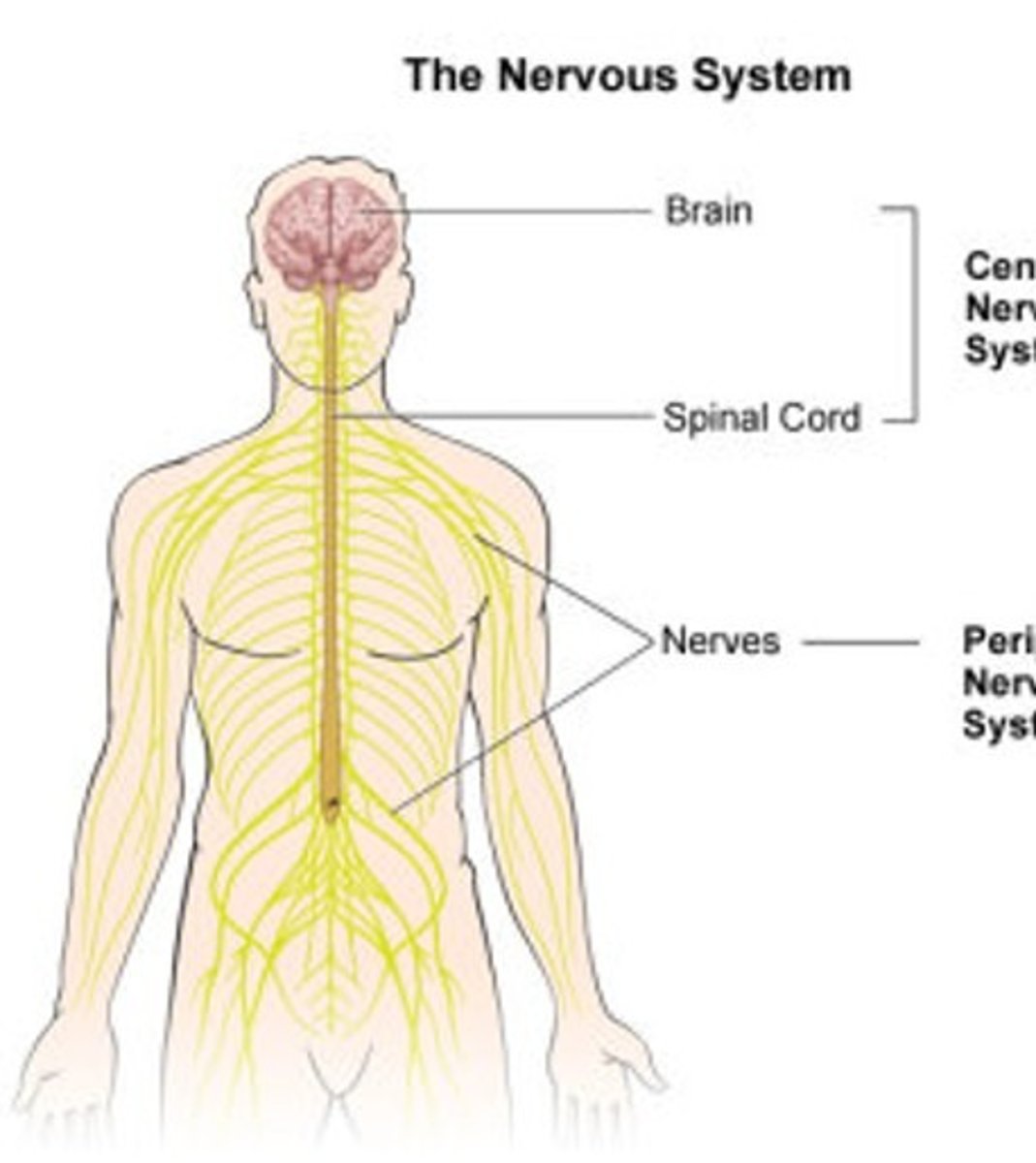
Peripheral Nervous System (PNS)
Nerves and ganglia outside the CNS
Autonomic nervous system
Controls involuntary responses and regulatory functions
What are some examples of involuntary responses and regulatory functions that the ANS controls?
Sleep and temperature
What is a drawback of aging in regard to temperature regulation?
Regulation is more difficult with age
-Older adults are more susceptible to hypothermia and hyperthermia
-In Florida, especially when power is lost during hurricanes, take better care of older adults during unpredictable weather!!!
Cognitive aging
Changes in the structure and function of the brain associated with getting older
-Some degree of this is normal!
Why is it important to study cognitive aging?
Cognitive changes impact everyone, including changes in functioning and well-being.
-Helps us design medication and interventions >> compensate for losses (Esp secondary aging)
What can be done to alleviate the effects of cognitive aging?
As we age, we have smaller social networks. Make acquaintances! (gym and community center)
What are some age-related structural changes in our brain?
There are fewer neurons, dendrites, and synapses due to the development of tangles in our axons.
-It is important to note that in someone with dementia, all of these changes occur at a much greater rate than a healthy person.
What are some additional examples of age-related structural changes in our body?
Changes occur in both healthy and pathological aging
-Changes in the production (e.g., less efficient) of major neurotransmitters
-Changes impact cognitive abilities
-Changes can result in some degree of cognitive decline
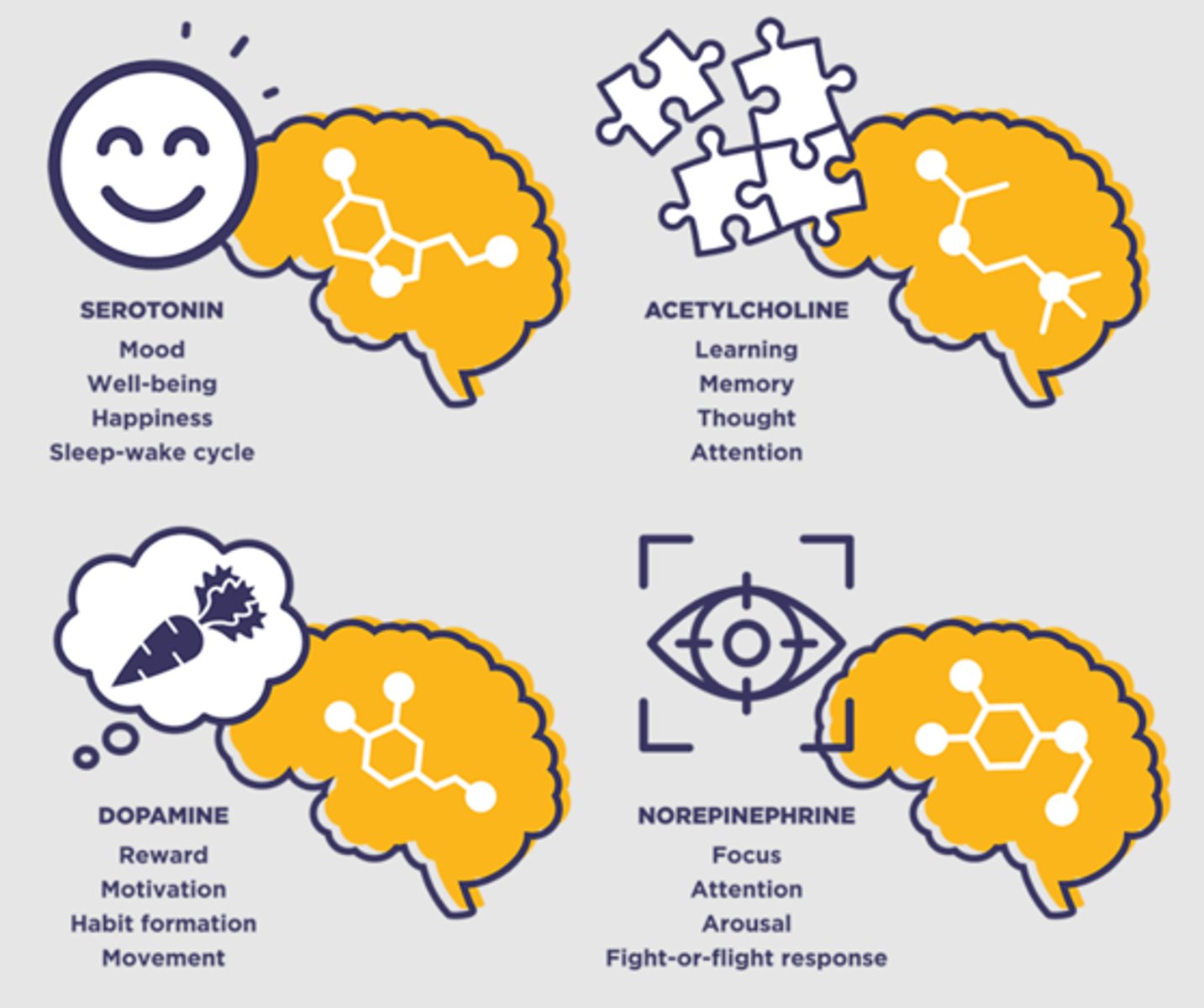
What are some examples of neurotransmitters in our brain?
•Dopamine =Memory and attention; effort and planning
•Serotonin =Mood, appetite, sleep
•Acetylcholine= Arousal, sensory perception, attention
•Norepinephrine = Motor changes
What are some activities associated with dopamine and serotonin?
Dopamine: Eating, self-care, listening to music, laughter, exercise, achievement of goals
Serotonin: Exercise, foods with tryptophan and vitamin B, sun exposure, meditation, nature walk, nurturing your gut
*Serotonin cannot be naturally produced so tryptophan is what is injected or found in foods and supplements as a serotonin equivalent because it is an amino acid that forms serotonin.

What are some structural changes in our neuroanatomy?
•Overall decrease in brain weight, approx. -2% per decade
•Apparent in the prefrontal cortex, hippocampus, and cerebellum
•Sensory and visual functions have little change
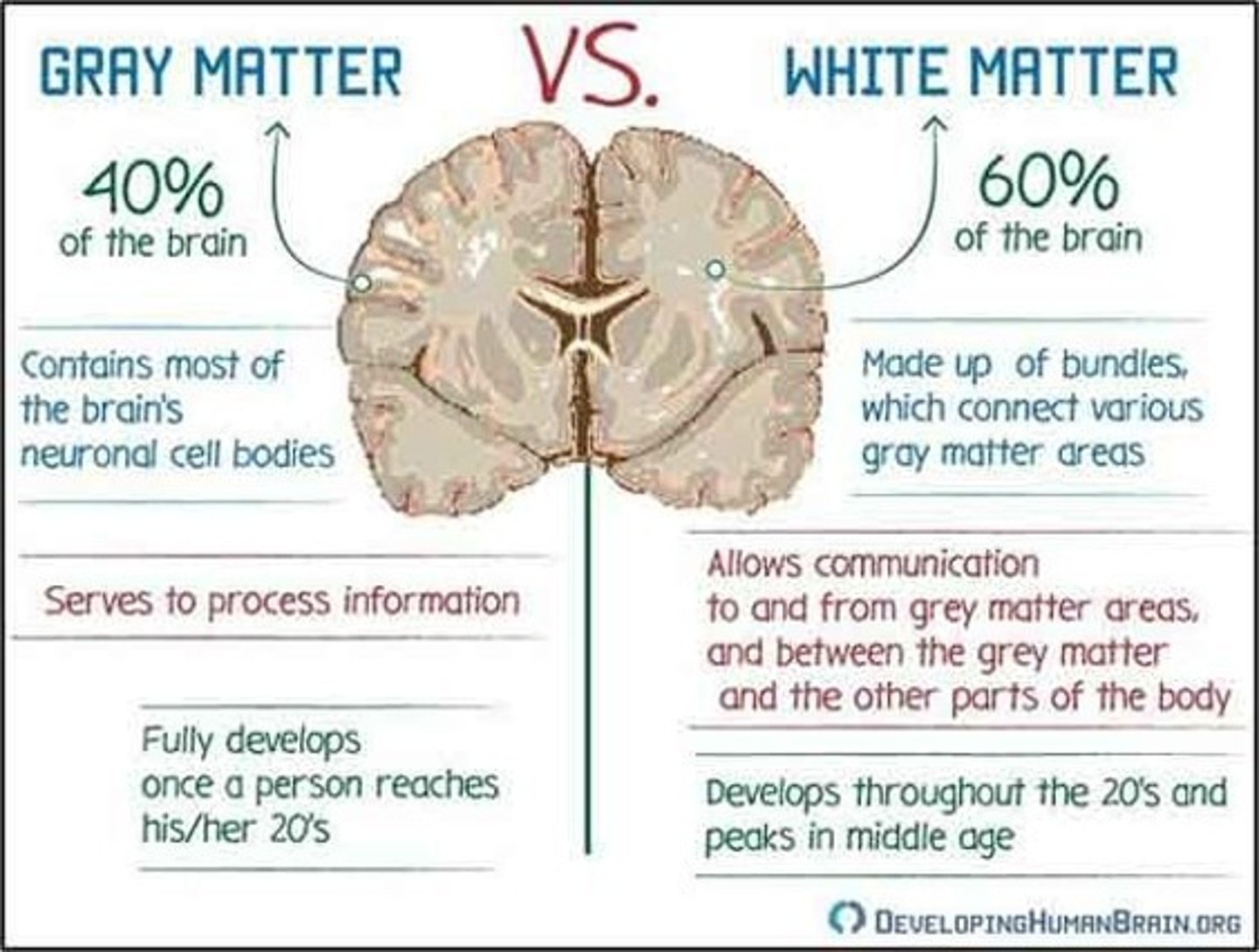
White matter
Myelin-covered axons; transmit information across the brain
•Greater deterioration with age
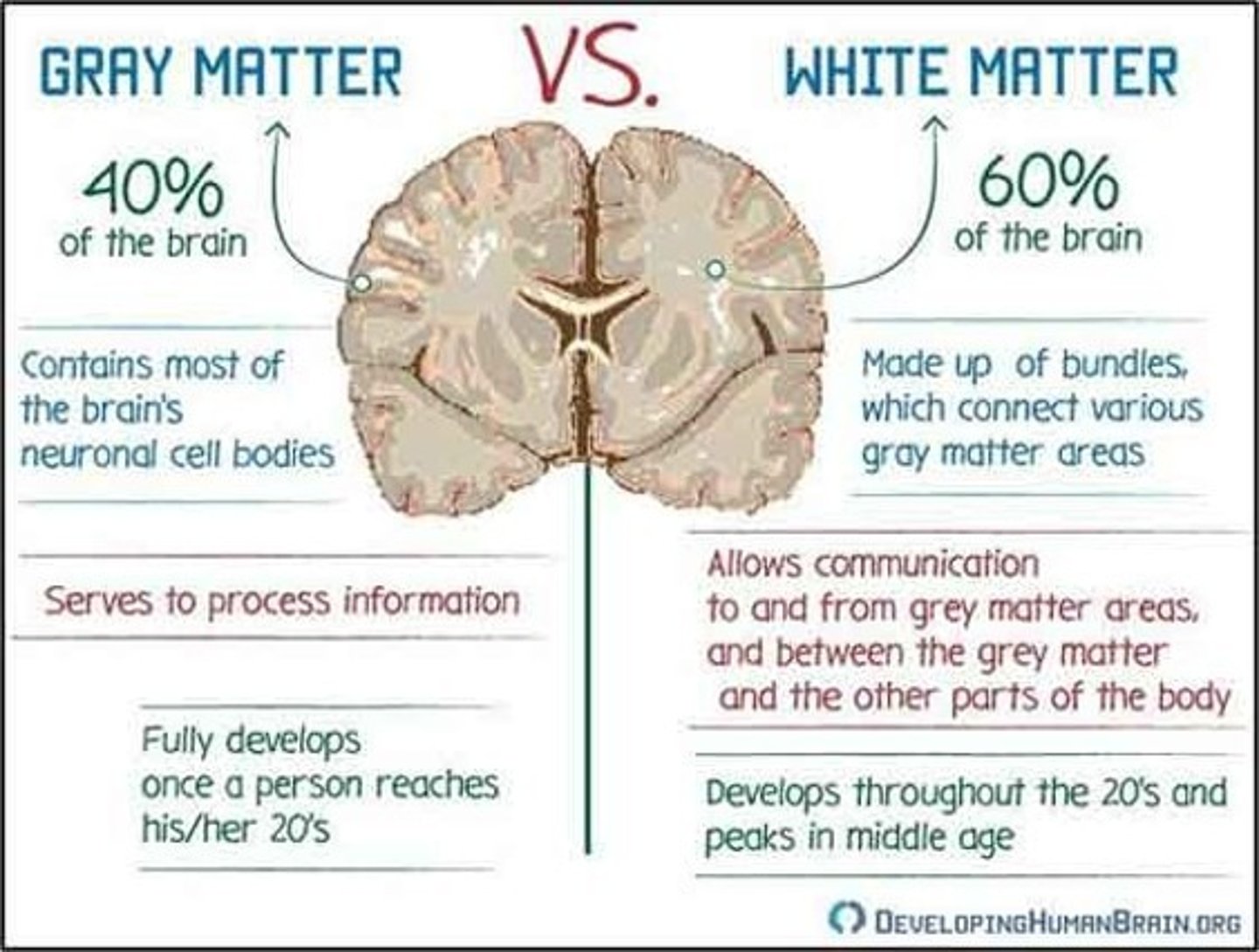
Gray matter
Neuron cell bodies, dendrites, and unmyelinated axons
•Gradual, small decreases due to age-related changes in neurons
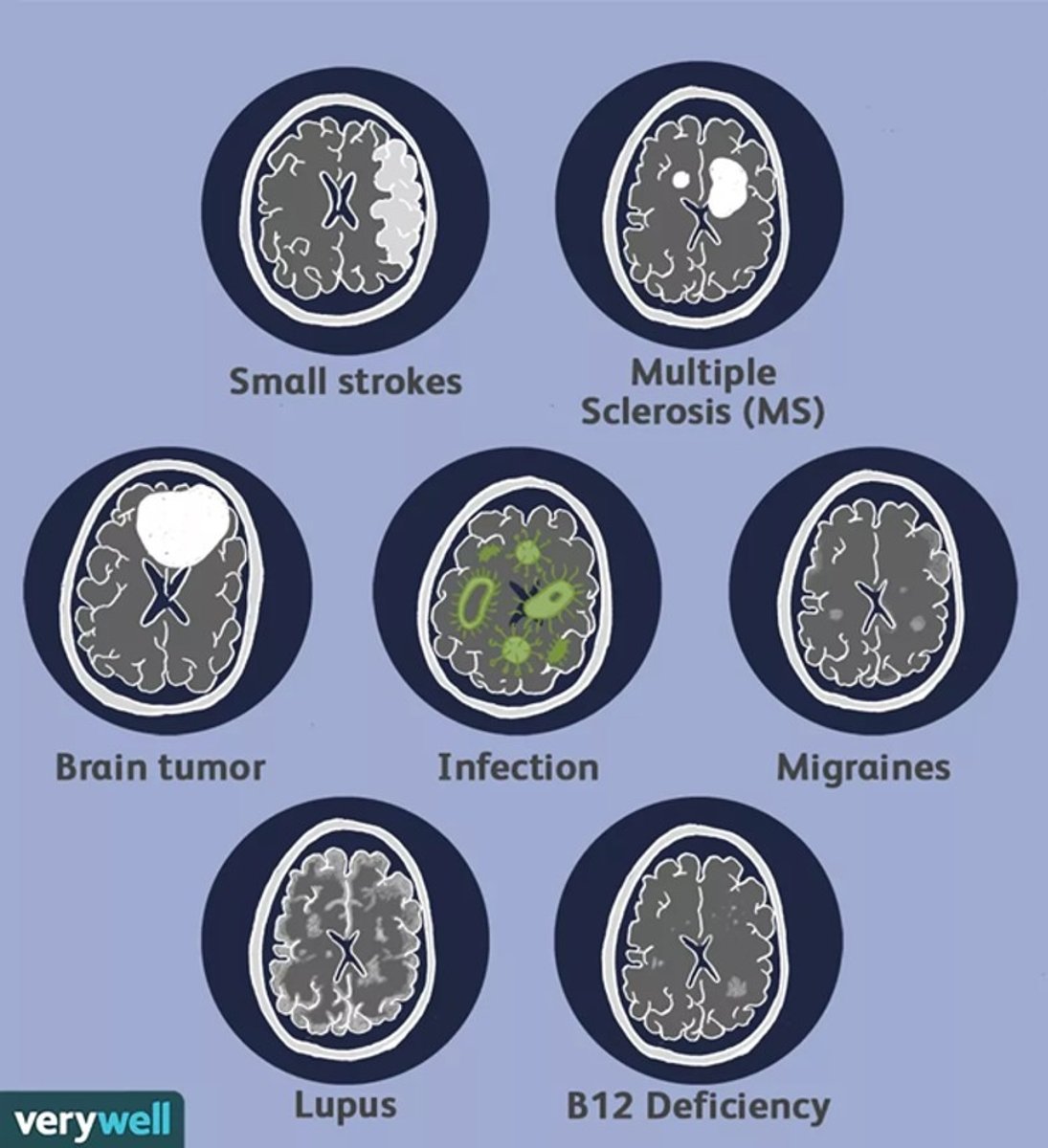
What are some structural changes in white matter due to age?
•White matter hyperintensities (WMH)
•Pathologies linked to different causes
•Bright white spots are neural atrophy
What are some changes in processing speed due to age?
•Begins to decline in our 30s
•“Thinking Efficiency”
•Leading cause of most cognitive changes
What are some changes in attention and memory due to age?
Slight decreases are common in later life
BrainHQ
•Computer-based training
•A study of more than 2,800 older adults found that people who got 10 hours of cognitive speed training plus some booster sessions were about 25% less likely to be diagnosed with Alzheimer's or another form of dementia.
•The protection lasted for 20 years!
What are some changes in executive functioning due to age?
•Declines due to WMH and reduced volume of the prefrontal cortex (see changes in white matter card)
•Reasoning about familiar topics and facts stays the same
What are some changes in language due to age?
Overall ability stays the same
What are some changes in our emotions due to age?
•Changes in prefrontal cortex and amygdala activity >> changes in emotion processing
•↑ processing of positive info; ↓ processing of negative info
•Suggests better emotion regulation
•Reflects age-related preference for positive relationships and situations (socioemotional selectivity theory)
•Older adults have increased activity in the prefrontal cortex and amygdala
•With age, more activation and connections, regardless if info is positive/negative
Positivity effect
Motivation to find meaning in life and maintain positive feelings
Bilateral activation
(Using both hemispheres) - supportive function related to age and compensation
•Suggests brains are adaptive and can reorganize to compensate for age-related changes
HAROLD
Model for brain activation patterns
-Hemispheric asymmetry reduction in older adults
•Explains reduced lateralization in older brains
•Bilateral activation lessens the impact of age-related changes
CRUNCH
Model for brain activation patterns
-Compensation-related utilization of neural circuits hypothesis
•Recruit additional neural circuits to compensate for decline, in addition to bilateral activation
•Over-activation compared to younger brains
•Effective at lower to moderate task demands
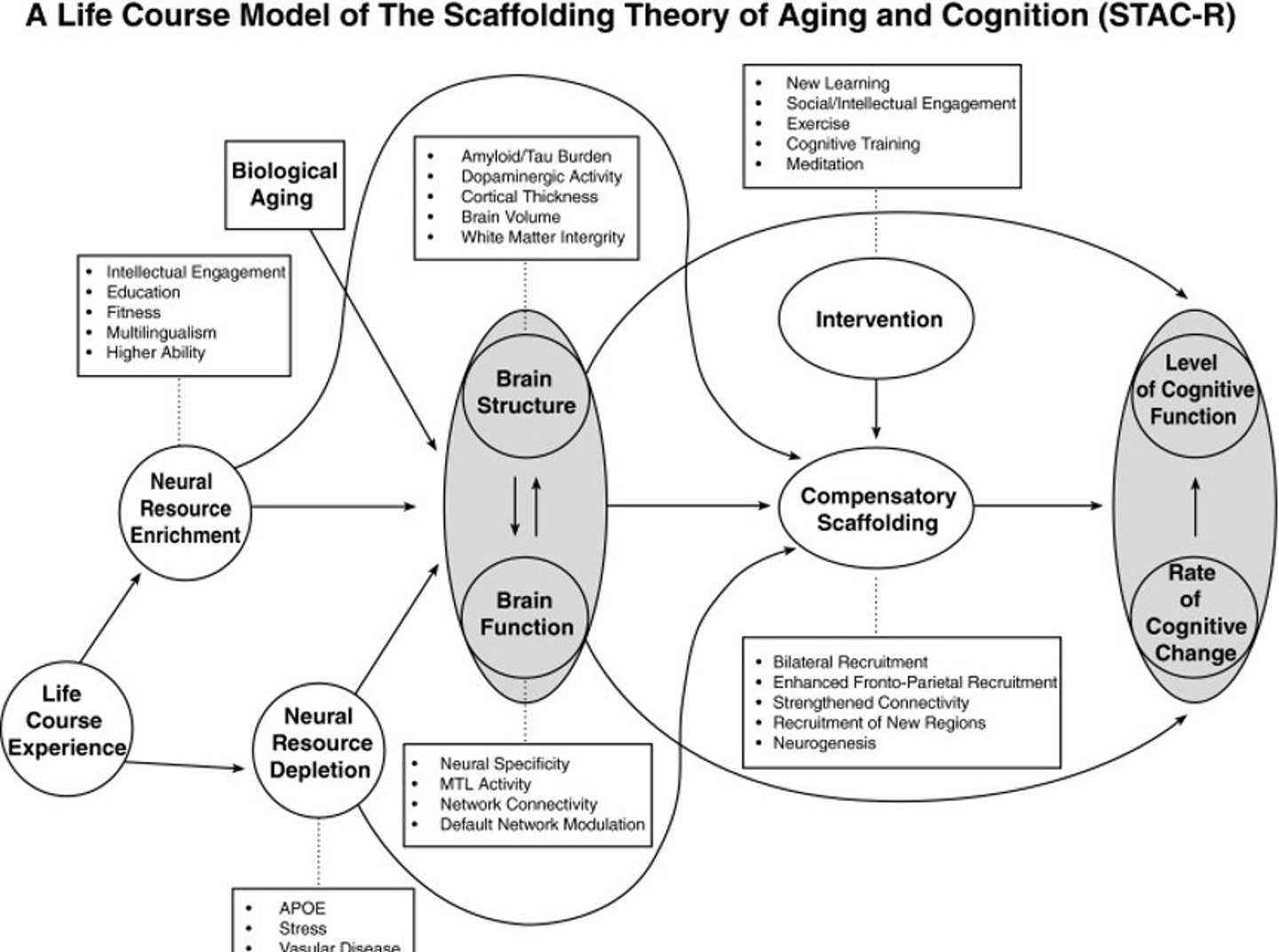
STAC
-Scaffolding theory of cognitive aging
•Aging = difficulty suppressing the default network of the brain
•Rely on backup pathways when the primary pathway fails
Neuroplasticity
Changes in the structure and function of the brain
•Result of people (and their brains) living in the world and learning from new experiences
•Creating more efficient connections to replace inefficient ones
•Possible to regain some functions after injury
-Compensation for traumatic brain injuries and strokes
Neurogenesis
Generating new neurons from neural stem cells
•Adults can create several hundred neurons in a day (slower rate than younger brains)
What are the effects of neuroplasticity on exercise?
•Brain plasticity can be enhanced by all types of exercise
•Higher aerobic fitness is related to preservation/increase in hippocampus volume
What are the effects of neuroplasticity on nutrition?
•Two patterns associated with better cognitive functioning and greater brain volume:
•Higher levels of vitamin B, C, D, E
•Higher levels of omega-3 & 6 fatty acids
•Transfats associated with less favorable cognitive function
What is cognitive reserve?
•Explains the brain's resilience and ability to adapt to challenges
•Two people may have similar amount of pathology, only one person shows symptoms
• Helps the brain work around injury, age-related changes
-Brain's ability to be flexible and adaptable with structures and functions
Why is cognitive reserve important, and how does it occur?
•It may postpone the effects of neurological diseases
•People might live longer without symptoms
-It occurs through the combination of education, healthy lifestyle, social support, physical activity, and cognitive simulation
The first sentence of the article says, "Chronic traumatic encephalopathy (CTE) is a progressive neurodegeneration associated with repetitive head trauma."
In this context, what does progressive mean?
A. A type of disease that can be reversed with treatment
B. A type of disease that is incurable
C. A type of disease that is relatively new and not well-understood
D. A type of disease that generally gets worse over time
D. A type of disease that generally gets worse over time
CTE-related lesions in the brain are different compared to aging-related lesions.
A. True
B. False
A. True
Rank the following football organizations in terms of the percentage of its athletes who were neuropathologically diagnosed with CTE (with 1 being the largest percentage, and 5 being the smallest percentage).
Hint: Use the Results section on the first page.
1. NFL
2. College football
3. Canadian Football League
4. Semiprofessional football
5. High school football
The most common cause of death for participants with mild CTE pathology was _______, while the most common cause of death for those with severe CTE pathology was _________________.
suicide; neurodegenerative
Athletes with mild CTE pathology played football for a longer amount of time, compared to athletes with severe CTE pathology.
A. True
B. False
B. False
Use Table 1 in the article to answer the following question.
The primary position of play associated with the greatest number of mild CTE cases was __________, while the primary position of play associated with the greatest number of severe CTE cases was ___________________.
linebacker; offensive lineman
In all the brains studied, CTE lesions were found in the ______.
A. cerebral cortex sulci
B. frontal cortex
C. cerebral cortex
D. lateral temporal cortex
C. cerebral cortex
Use Table 3 in the article to answer the following question.
Which of the following behavioral and mood symptoms were reported in more than half (>50%) of all participants, regardless of CTE severity? Select all that are true.
A. suicidality
B. impulsivity
C. paranoia
D. verbal or physical violence
E. depressive symptoms
F. anxiety
B, E-F
impulsivity, depressive symptoms, anxiety
Which one of the following is not considered a strength of the study?
A. All participants were exposed to the same kinds of head trauma while playing the same sport.
B. Players who had visible CTE symptoms and their families were more likely to participate in the study.
C. Clinical evaluations about the participants relied on information provided by a close informant.
D. It was the largest CTE study conducted so far, to the authors' knowledge.
B. Players who had visible CTE symptoms and their families were more likely to participate in the study.
Which of the following statements best summarizes the article?
A. Many former football players showed signs of CTE, so we can conclude that CTE is related to prior participation in football.
B. Some of the football players studied showed signs of CTE, but it is too early to suggest that CTE may be related to prior participation in football.
C. All of the football players studied showed signs of CTE, which suggests that CTE may be related to prior participation in football.
D. Many football players showed signs of CTE, which suggests that CTE may be related to prior participation in football.
D. Many football players showed signs of CTE, which suggests that CTE may be related to prior participation in football.
What is dementia?
Dementia is not one specific disease
•A group of diseases characterized by a decline in memory and other cognitive skills
•Severe enough to reduce a person's ability to perform everyday activities
•Affects 50 million people worldwide
What is the criterion for diagnosing someone with dementia?
Criterion for a Dementia diagnosis:
Must have impairment in two or more of the following:
•Memory
•Communication and language
•Ability to focus and pay attention
•Reasoning and judgment
-Visual perception
Alzheimer's disease
•Type of dementia causing problems with memory, thinking, and behavior
•Accounts for 60-80% of all dementia cases
•Progressive and fatal – symptoms gradually worsen over time and eventually lead to death
What are the risk factors for Alzheimer's disease?
•Non-modifiable – age*, family history, genetics
Age: After age 65, the risk doubles, and after age 85, the risk triples!
Early-onset Alzheimer's disease
•Early-onset (or younger-onset) AD – a rarer form of AD that affects people in their 40s and 50s
•Accounts for <5% of AD cases (~200,000 people) in the US
•Familial AD: This is a variant of early-onset AD where some cases have no known cause, but most are inherited.
What are some additional issues with early-onset Alzheimer's disease?
•Fast progression; individuals are likely to die within a few years of diagnosis
•At this age, people are still working, raising children, etc.
What are some of the causes behind Alzheimer's?
•Unclear, but some combination of risk factors
•More than 100 genes related to developing late-onset AD
Apolipoprotein E (APOE)
Gene with the strongest impact on AD!
-Protein that helps blood carry cholesterol and other types of fat through the body
What are the three alleles associated with APOE?
E2 (protective), E3 (neutral), E4 (risky)
What are the drawbacks of relying on only APOE as the cause of AD?
•APOE alone does not determine AD diagnosis
•About 40-65% of people with AD have an E4 allele, but E4 alleles don’t guarantee AD
What are 10 symptoms of Alzheimer's disease?
Memory loss, misplacing items, difficulty in decision making and judging, reduced ability in understanding visual images, confusion with time and places, mood swings, repetitive speech and writing issues, difficulty in problem solving, social withdrawal, inability to complete complex tasks
On average, people start showing symptoms of Alzheimer's in their ________.
Mid-60's
What are some changes that occur in a brain with AD?
Brain changes in AD are microscopic:
•Rapid cell death
•Beta-amyloid (Aβ) plaques
•Tau tangles
>>Result in cumulative brain atrophy
Rapid cell death
•Leads to brain shrinkage
•Mostly in the hippocampus, cerebral cortex, and ventricles
Beta-amyloid (Aβ) plaques
Beta-amyloid (Aβ) – protein that helps grow and repair neurons
•Plaques formed when sticky protein fragments become insoluble and can’t be cleared out by the brain
•Attack and destroy neurons and synapses
Tau tangles
Tau – protein that helps with cell structure (microtubules)
•Builds tracks/pathways to move nutrients and molecules
•Tangles are formed when tau begins to unravel and no longer supports the microtubules
•Tau clump together, also becoming insoluble
What are some risk factors for AD? Some of them are potentially modifiable.
•Modifiable risk factors – things that could potentially influence our risk through lifestyle and wellness
•Brain + heart health
•Eat a healthy diet
•Stay socially active
•Avoid tobacco, excess alcohol
•Exercise body and mind
May slow decline or disease onset, but no guarantees they will prevent AD
Vascular dementia
•Results from several small cerebral vascular accidents (blood clot or hemorrhage), or strokes
•Most patients have a history of cerebrovascular or cardiovascular disease
•Symptoms vary based on which brain regions are damaged
•Much faster course than AD
•Death occurs 2-3 years after onset
Lewy Body Dementia
•Lewy bodies – abnormal clumps of α-synuclein protein
•Can cause dementia, or can be present at the same time dementia occurs
•Common symptoms:
•Sleep disturbances
•Well-formed visual hallucinations
•Slowness and gait imbalance
•Mood changes and depression
Frontotemporal dementia
•Affects frontal and temporal lobes
•Cognitive symptoms at a younger age (60s)
•Executive and language dysfunction, significant behavioral and personality changes (“frontal” symptoms)
•Memory decline happens later
May be caused by genetic mutations
Parkinson's disease
•Also caused by abnormal clumps of α-synuclein protein
•Damages cells producing dopamine
•Once 60-80% of dopamine cells are damaged, characteristic motor symptoms appear:
•Very slow walking
•Difficulty getting in/out of chairs
•Hand tremors
Huntington's disease
•Progressive disease with cognitive symptoms appearing later
•Involuntary flicking movement of the arms and legs
•Hallucinations, paranoia, depression, personality changes
•Autosomal dominant disorder
•Genetic test available
Alcohol-related dementia
•Also called Wernicke–Korsakoff’s syndrome
•B1 deficiency plus chronic alcohol dependence
•Key symptom is confabulation
AIDS Dementia Complex
•Occurs primarily in people with advanced HIV
•The virus can damage brain structures and the spinal cord
•Behavioral changes and cognitive decline
CTE (Chronic Traumatic Encephalopathy)
•Progressive neurodegeneration associated with repetitive head trauma
•Similarities to AD
•Buildup of Aβ and tau proteins >> plaques and tangles
•Progressive
•Cannot confirm diagnosis until after death
No cure yet
What are the symptoms associated with CTE, including brain damage?
•Problems with thinking and memory
•Behavioral and personality changes
•Aggression, anxiety, depression, impulsivity
•Brain lesions
•Areas of brain tissue damaged through injury or disease
Appear as light or dark spots
What were the results of Article 2? (Football players and CTE)
•CTE found in 99% (110 of 111) of former NFL players
•Neuropathological features
•Tau tangles and α-synuclein in all players
•Aβ in many players (91% of severe cases)
•Severity related to duration, level, and position