(7) Salt and Water Balance; Hormonal Regulation
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
50 Terms
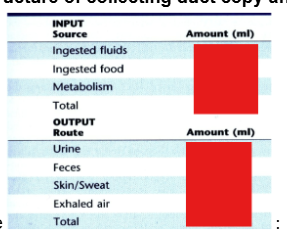
Complete the table
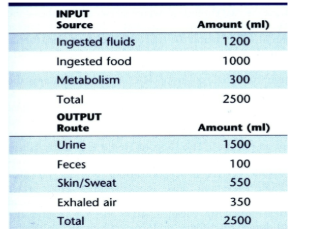
Your body filters about ~--- liters a day but you only produce about ~--- L of urine
180; 1.5
The kidneys regulate plasma osmolality by regulating —-
urine osmolality (either creating a dilute or concentrated urine)
A dilute urine results from what?
reabsorption of salt from tubule segments impermeable to H2O. These segments include the ascending limb, thick ascending limb and distal tubule (this segment is referred to as the diluting segment due to its ability to actively reabsorb NaCl and collecting duct)
A concentrated urine results from what?
Reabsorption of H2O (by osmosis) from tubule segments that are exposed to a hyperosmotic interstitium. These segments include Proximal tubule, descending limb, distal tubule and collecting duct.
t/f when creating a concentrated urine, the fluid in the tubule after the TAL is hyperosmotic
false; it is always hyposmotic no matter if the urine is being concentrated or diluted
There is no difference in the mechanism of generating a concentrated or diluted urine up until what structure of the nephron?
early distal convoluted tubule
The ability to concentrate urine requires what 2 things?
1)H2O-permeable, distal nephron segments 2) a hyperosmotic medullary interstitium
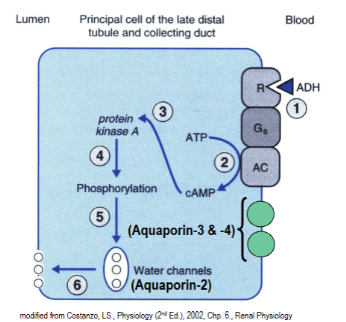
Anti-diuretic hormone
released by posterior pituitary. Acts on principal and principal-like cells of the collecting duct of the nephron. Causes stimulation of aquaporin-2 water channels and causes them to be inserted into the apical (lumenal) membrane. Overall it stimulates water reabsorption.
Principal and principal like cells are sensitive to what two important hormones that we discuss?
aldosterone and antidiuretic hormone (ADH)
Other name for ADH and why?
Arginine vasopressin (AVP) because it’s a powerful vasoconstrictor.
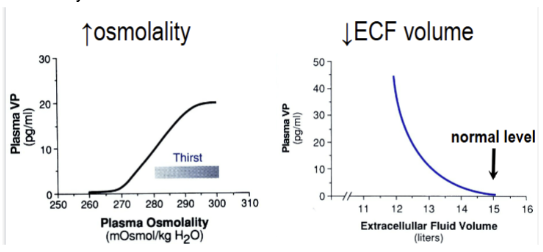
Primary stimulus for ADH and secondary stimulus
primary= increase in osmolality and secondary=a substantial decrease in extracellular fluid volume.
What can cause increased plasma osmolality?
not drinking or losing fluid through sweating
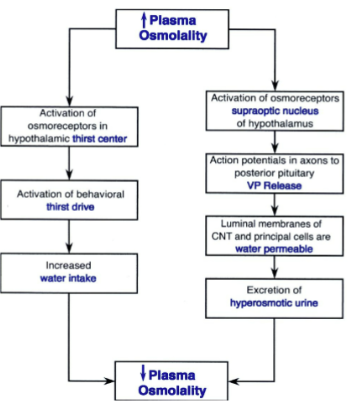
Show how an increase in plasma osmolality is responded to by the brain and kidneys
VP=ADH
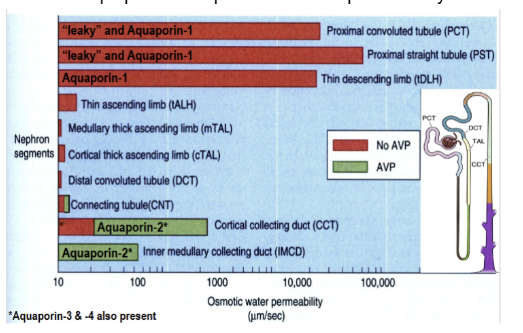
Show how permeable to water each segment of the nephron is with and without AVP and what aquaporin is responsible for this permeability
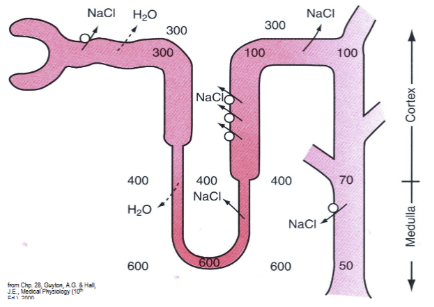
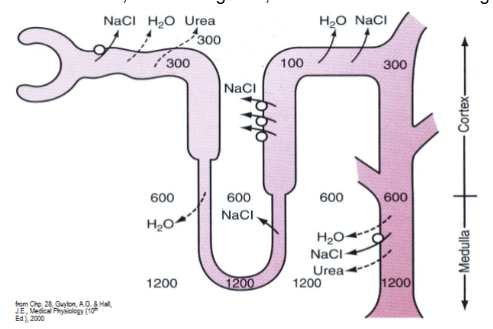
Show the osmolality of tubule fluid relative to the plasma in a diuretic state vs antidiuretic state
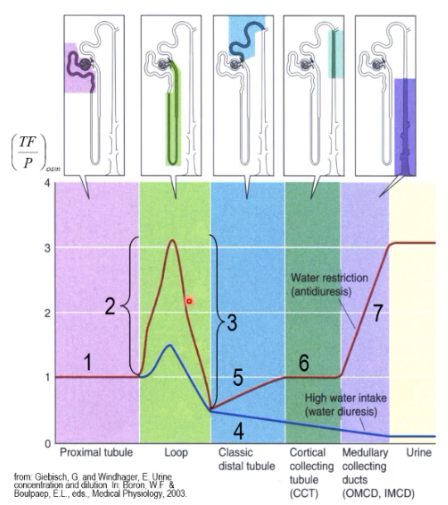
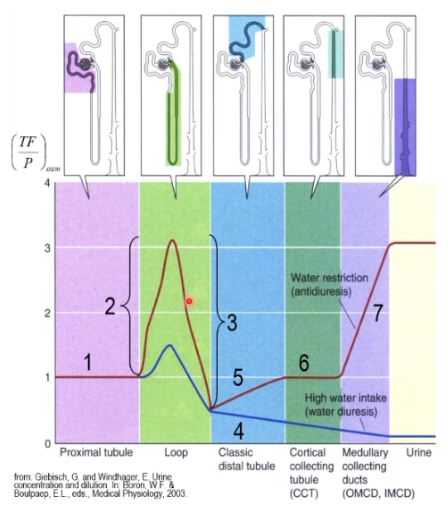
Using the chart, explain what happens at each number for the anti-diuretic state
PT reabsorbs isosmotic fluid. 2. tDLH reabsorbs H2O. 3. tALH and TAL reabsorb salt. 4. Distal segments are H2O impermeable in the absence of ADH (diuresis). Further NaCl reabsorption dilutes the fluid. Distal segments are H2O permeable in the presence of ADH (anti-diuresis). Thus: 5 & 6. Osmolality rises and matches that of the interstitium by the end of the ICT and throughout the CCT. 7. Osmolality rises as the H2O- permeable tubule descends into the progressively hyperosmotic medulla.
Antidiuresis vs diuresis
Diuresis is the kidneys' process of filtering excess fluid from the blood to produce a large volume of dilute urine (occurs when hydrated or plasma osmolality is low), while antidiuresis is the opposite process where the kidneys conserve water, resulting in a small volume of concentrated urine (occurs when dehydrated or plasma osmolality is high).
What nephrons are especially important in generating a hyperosmotic medullary interstitium
juxtamedullary nephrons
Fluid moving down the tDLH becomes — as it moves toward —
concentrated as it moves toward the hyperosmotic medulla
How does the ascending limb of henle contribute to producing a concentrated interstitium?
Reabsorption of NaCl by the ascending limb creates an interstitial-TF gradient and increases [NaCl of the]interstitium, which gets amplified by countercurrent TF movement that progressively concentrates NaCl deeper in the medulla
Show the loop countercurrent multiplier
each cycle involves the following steps- 1) “single-effect”, whereby passive and active solute movement in the ascending limb generates a 200-mOsm gradient. (solute from ascending limb moves to interstitium) 2) Osmotic equilibration of the descending limb and the interstitial fluid. (fluid from descending limb moves in response to solute) 3) Tubule flow, whereby the concentrated tubule fluid is driven towards the tip of the loop.

What does the countercurrent multiplier achieve?
builds and maintains a hyperosmotic (highly concentrated) interstitial gradient deep within the renal medulla. This gradient enables the kidneys to passively reabsorb water from the collecting ducts, ultimately concentrating urine and preventing dehydration.
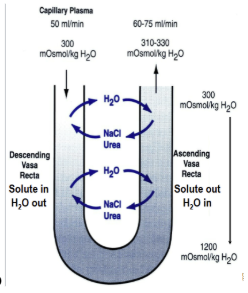
How is the hyperosmotic medulla not “washed out” by blood vessels
Vasa Recta (passive countercurrent-exchange mechanism to retain the hyperosmotic medulla). Vasculature. There is also reduced blood flow
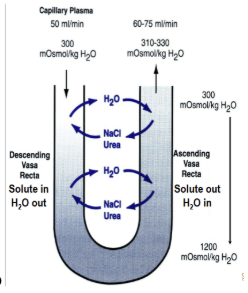
Vasa recta
peritubular capillaries for deep juxtaglomerular nephrons. Helps to maintain hyperosmotic medulla via a passive countercurrent-exchange mechanism where the salt is picked up as it goes down with the loop of henle is lost again as it goes back up with the loop
t/f the vasa recta prevents ALL wash-out that occurs in the hyperosmotic medulla of the kidney
false; it just greatly reduces it
The hyperosmotic interstitium is composed of what solutes?
both NaCl and urea
The —- concentration rapidly rises as you move deeper into the medulla of the kidney
urea
Show the difference in how osmolality of NaCl increases vs how urea increases as you move deeper into the medulla of the kidney
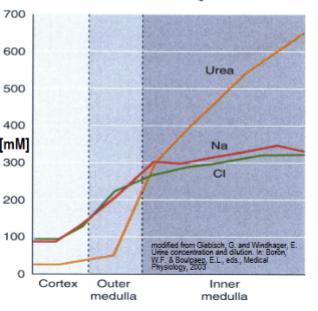
Urea recycling concentrates urea in the inner medulla to ~--- mOsm
600
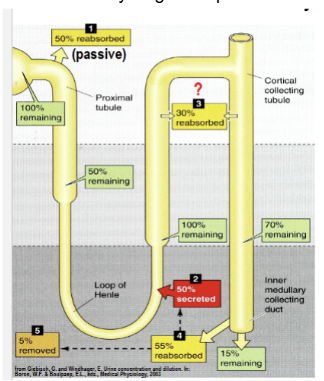
Show and explain what urea recycling is
The tip of the tDLH and tALH secrete ~50% of filtered urea. renal physiological process where the kidneys reabsorb and secrete urea multiple times. This mechanism builds a high solute concentration in the renal medulla, enabling the body to conserve water and excrete highly concentrated urine
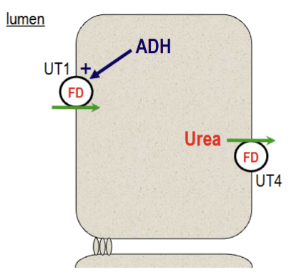
How does ADH affect urea recycling?
concentrated urea in the inner medullary collecting duct (IMCD) is reabsorbed in the presence of ADH. ADH stimulates UT1 (via phosphorylation) activity and expression. UT1 and UT4 are two facilitated transport mechanisms.
How does a diuretic (taking in lots of water) affect urea recycling
in the absences of ADH, urea recycling slows and overall urea concentration in the interstitium falls. This means that less water is reabsorbed.
List the factors that affect urinary concentration
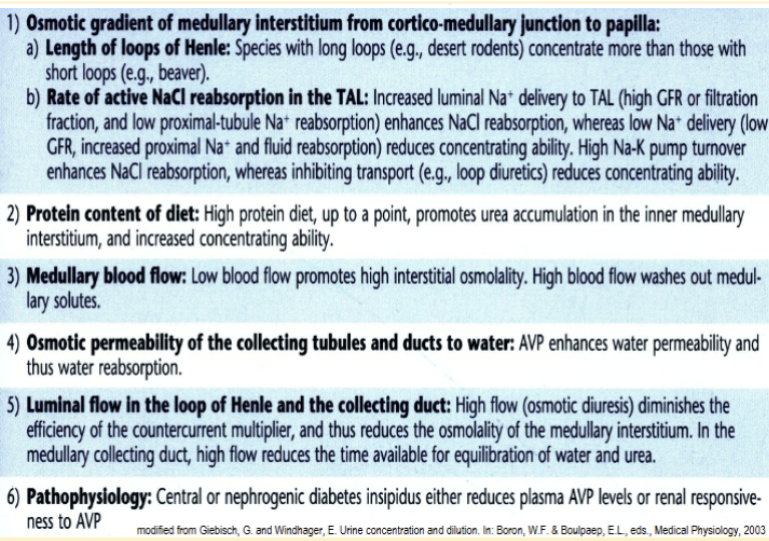
Length of the loop of henle-How does it affect urinary concentration?
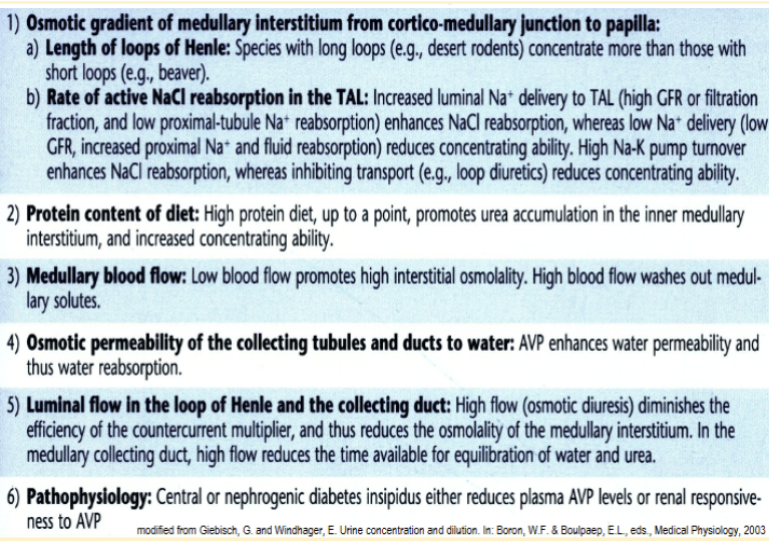
Rate of active NaCL reabsorption in the TAL-How does it affect urinary concentration?
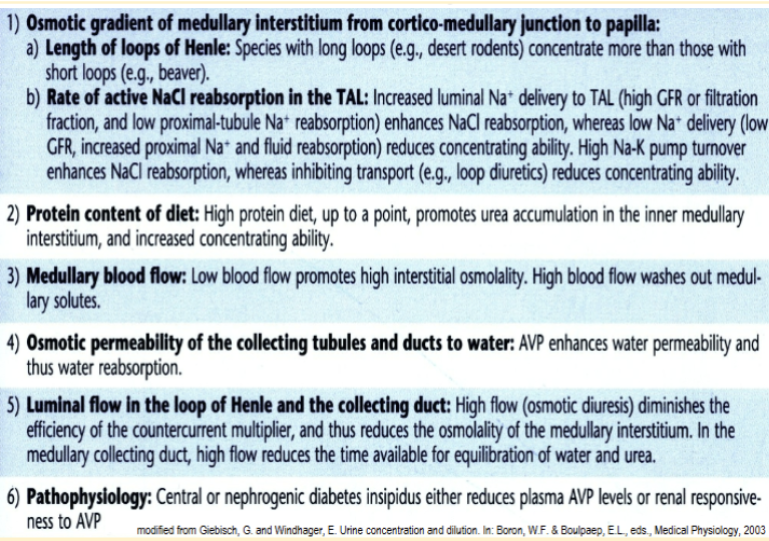
Protein content of diet--How does it affect urinary concentration?
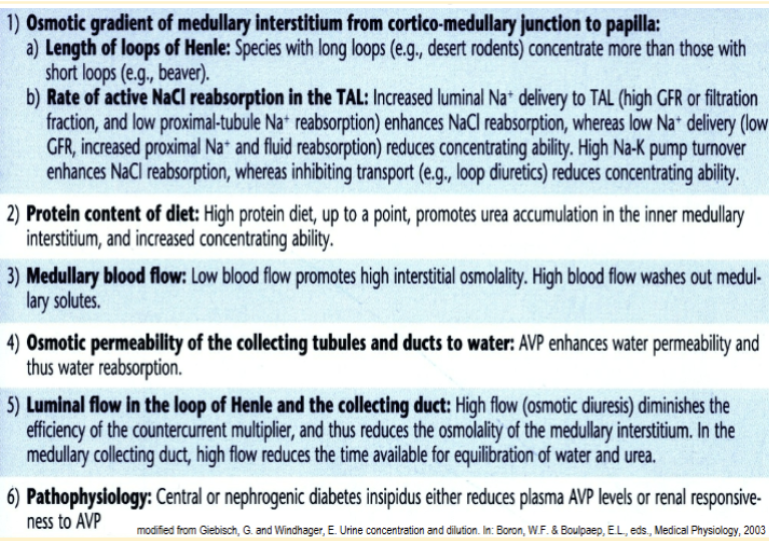
Medullary blood flow--How does it affect urinary concentration?
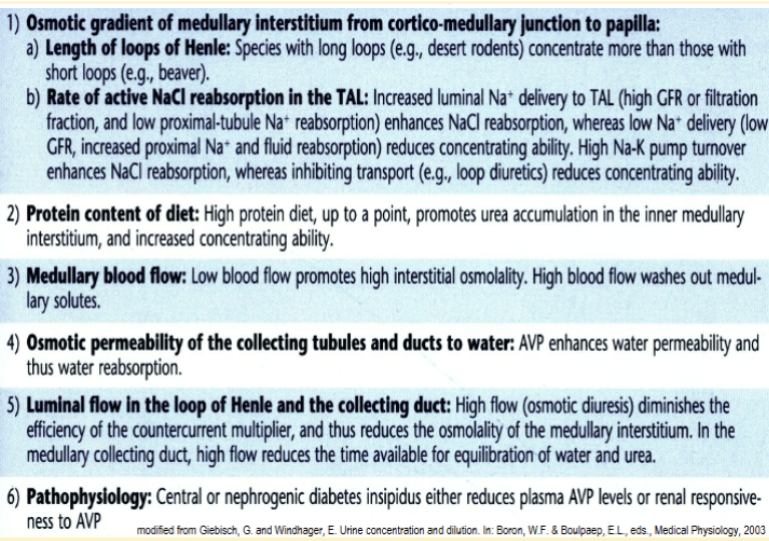
Osmotic permeability of the collecting tubules and ducts to water--How does it affect urinary concentration?
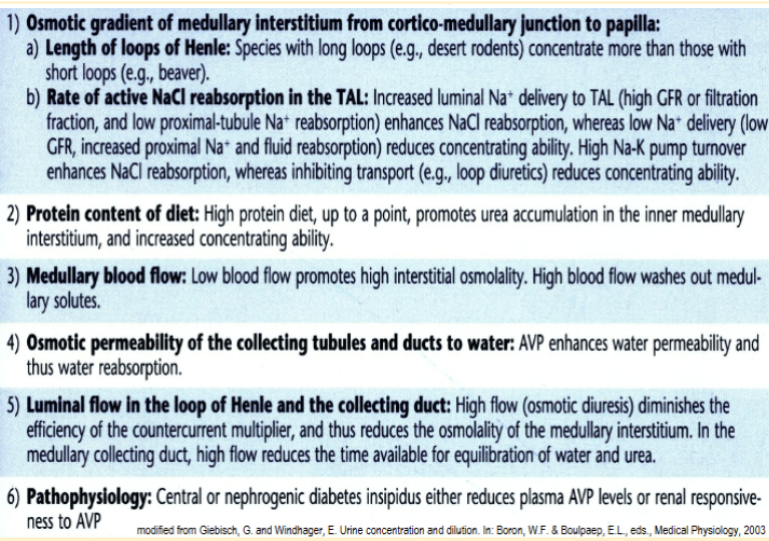
Luminal flow in the loop of henle and the collecting duct--How does it affect urinary concentration?
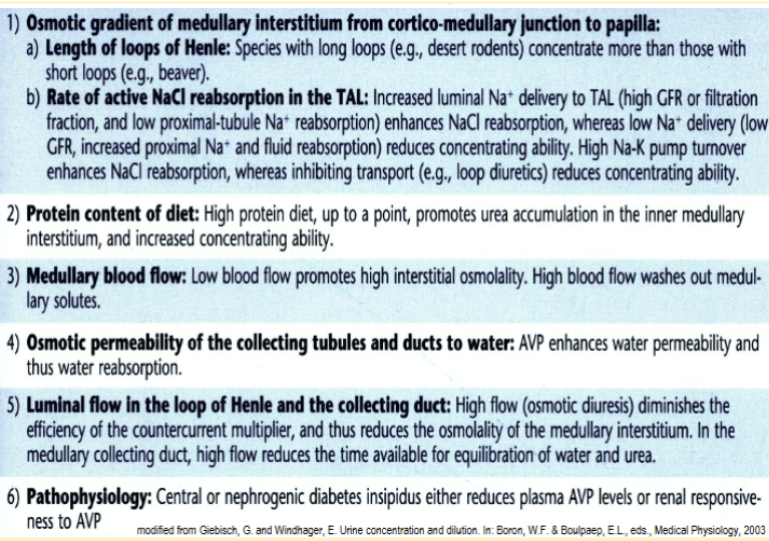
Pathophysiology--How does it affect urinary concentration?
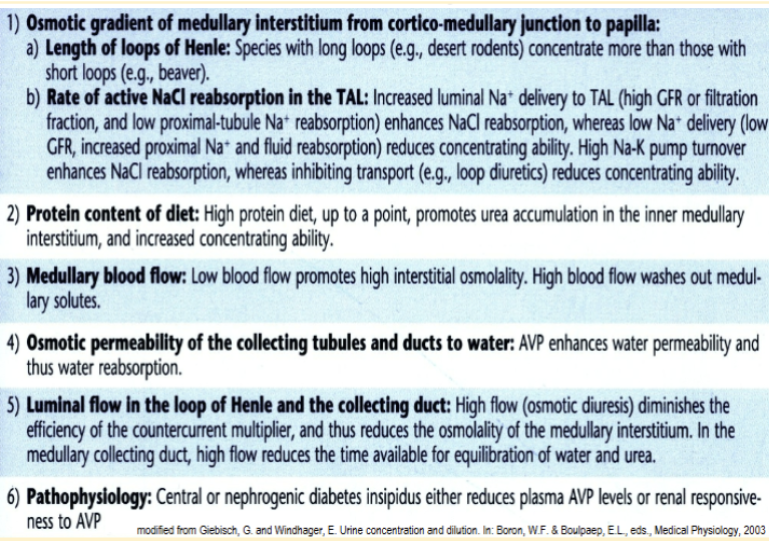
Central vs nephrogenic diabetes insipidus
central diabetes insipidus is caused by a lack of antidiuretic hormone (ADH) production in the brain, while nephrogenic diabetes insipidus occurs when the kidneys fail to respond to the ADH
What can be used as a sign of elevated ADH
concentrated urine
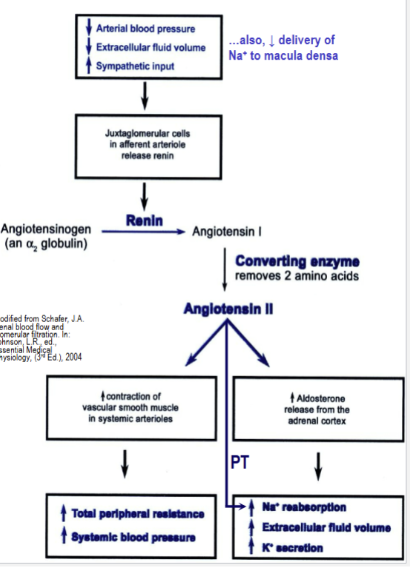
Show RAS (renin-angiotensin system) and how it regulates BP and ECF volume
renin releases are triggered by lowered BP, lowered ECF volume and lowered delivery of Na+ to macula densa.
Contraction alkalosis
when the body loses significant fluids and angiotensin II levels are high due to activated ras, the sodium proton exchanger will be activated causing secretion of H+ which can lead to alkalosis as too much HCO3- is reabsorbed in order to reabsorb more Na+.
Show how the body reacts to a state of hypovolemia
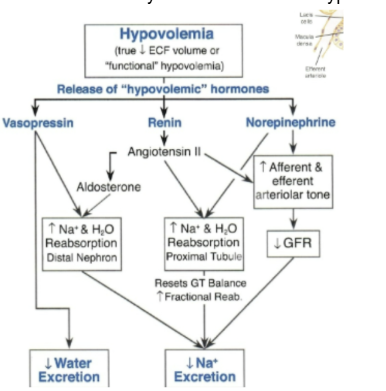
True hypovolemia va “functional” hypovolemia
true hypovolemia is a volume contracted state caused by loss of blood or body fluid. Functional occurs due to loss of perfusion in certain organ systems (particularly the heart). This fools the body into thinking that its in a volume contracted state
Show how the body reacts to hypervolemia

Atrial Natriuretic peptide (ANP)
natriuretic hormone released in response to a volume expanded state. Increases GFR and inhibits Na+ reabsorption in IMCD which leads to increased Na+ excretion.

Hypervolemia
volume expanded state in the body in which there is higher than normal amount of blood or body fluid.