FGF and ASA risk scores
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
How is FGF calculated for non-rebreathing circuits
TV X RR = MV (minute volume)
MV x Circuit factor = FGF
What are the normal tidal volumes
15ml/kg for cats and small dogs
12ml/kg for medium dogs
10ml/kg for large dogs
How do you calculate FGF for rebreathing systems
Induction rate- 100ml/kg/min for 5-10 mins
Maintenance rate- 10ml/kg/min (0.5-1L is sufficient for those under 50kg
A maintenance rate of <0.5l/min may cause vaporiser inaccuracy
What factors affect the metabolic rate for FGF
Temperature
Age
Fitness
Why do we calculate FGF
We calculate FGF to purge the system of air and fill it with fresh gas
Also provides sufficient anaesthetic agent for rapid stabilisation of anaesthesia depth
What do we need to do to complete a pre-anaesthetic assessment and prep
Patient assessment
Patient preparation
Equipment preparations
Preparing
What comes under a patient assessment
Temperament
Cardiac
Respiratory
Temperature
Hydration
Neurological status
Pain
Clinical history
How can we reduce stress and anxiety prior to GA
Pheremones e.g. flyway and adaptive
Sedatives e.g. gabapentin and trazodone
Oromucosal e.g. dexmedetomidine gel
When should we do PABS
When is an echo indicated
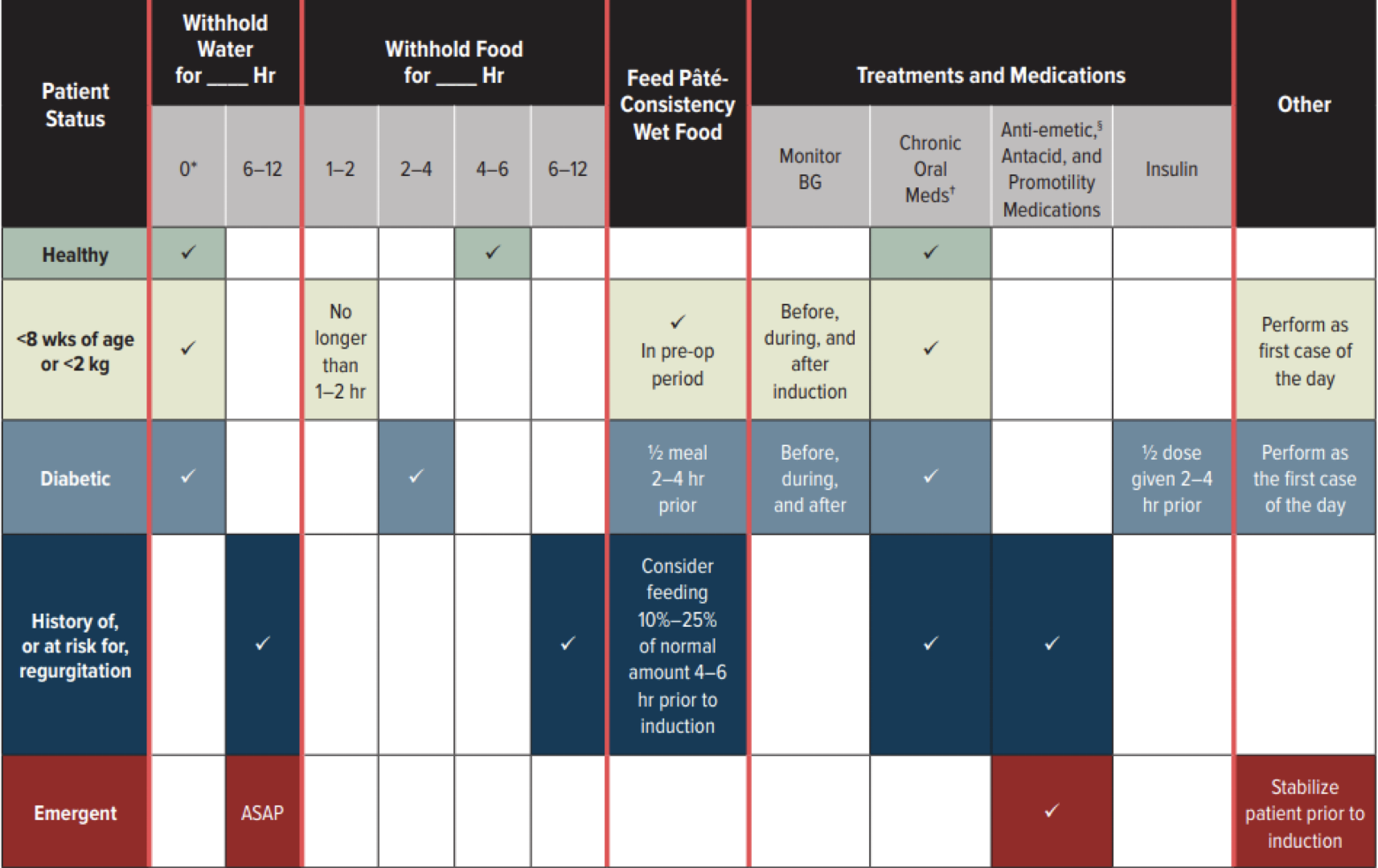
When should we fast patients before GAs
How can we reduce regurgitation + / - aspiration
Omeprazole
In dogs 1mg/kg oral omeprazole given twice in 24hrs before anaesthesia significantly reduces acidity of gastric pH
Maropitant
Reduction of opiate and alpha-2 adrenergic agonist reduces nausea and vomiting, total opiate and inhalational requirements and visceral nociception
Smoother recovery transitions and faster return to eating post-op
What equipment do we need to prep
Oxygen
Flowmeter
Vaporiser
Scavenging
Paperwork
How do we check breathing systems
Visually inspect and leak test
Close APL valve for leak test and reopen fully
Check soda lime for exhaustion
Check inside tubing of coaxial system for leaks
Open APL valve when done
What do we need to take into account when ASA grading
Species-are you familiar with the anatomy, physiology, disease, pathology and pharmacology
Equipment- are you familiar with the equipment you are using
Breed (if relevant)- does the breed you are anaesthetising have an increased ris
What is grade 1 ASA score
Normal healthy animal
No detectable underlying disease
What is grade 2 ASA score
Slight to mild systemic disease
Causing no obvious clinical signs or incapacity
Neonates
Geriatric
Obese
What is grade 3 ASA score
Mild to moderate systemic disease
Causes clinical signs
What is ASA grade 4
Extreme systemic disease
Constitutes a threat to life
What is ASA grade 5
Moribund and not expected to survive for more than 24 hours without surgery
What considerations need to be made when choosing drugs
Patient
Temperament
ASA grade
Age
Breed
Procedure/surgery
Aim
Analgesia required?
ADD MORE FROM RECORDING
What do owners need informed consent about
Cost
Procedure breakdown
Risks
Benefits of procedure
What should be part of the checklist
Pre-induction
Check patient
Check equipment
Check staffing
Pre-procedure
Communicate safety concerns
Recovery
Check all procedures are done prior to recovery
Analgesia plan
Ongoing monitoring-hand over to ward team to monitor/anaesthetic nurse
What are the main considerations for positioning
Well padded
Neutral position
Avoid overextension and/or flexion
Consider pain e.g. OA
Avoid eye trauma
Avoid damage to trachea/ETT obstruction – e.g. breathing system pulling on ET tube
What are the considerations for dorsal recumbency
Diaphragm pressure-worsened by abdominal distension (all organs come up and push on diaphragm)
Hypoventilation
CV effects- reduced venous return and cardiac output (worse in large breeds)
What are some general positioning considerations
Avoid excess movement/position changes- increased risk of regurgitation/aspiration
Avoid limbs hanging over the edge of a table or use suitable padding- avoid compartment syndrome
Ensure heat sources are not too hot and are well protected to prevent burns
Disconnect the anaesthetic circuit from the ET tube when repositioning—prevents tracheal damage
Give time in sternal when turning from one lateral recumbency to another due to atelectasis (collapsed lungs)
Anal/perineal surgeries may require a head down angle (trendelenberg position)- causes hypoventilation