DSA06 - Pathology of the Ovaries, Uterus, and Fallopian Tubes
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
41 Terms
STRATUM BASALIS:
Minimally hormone responsive and serves to replenish the stratum functionalis following menses
What is this layer of the Endometrium and what is its function?
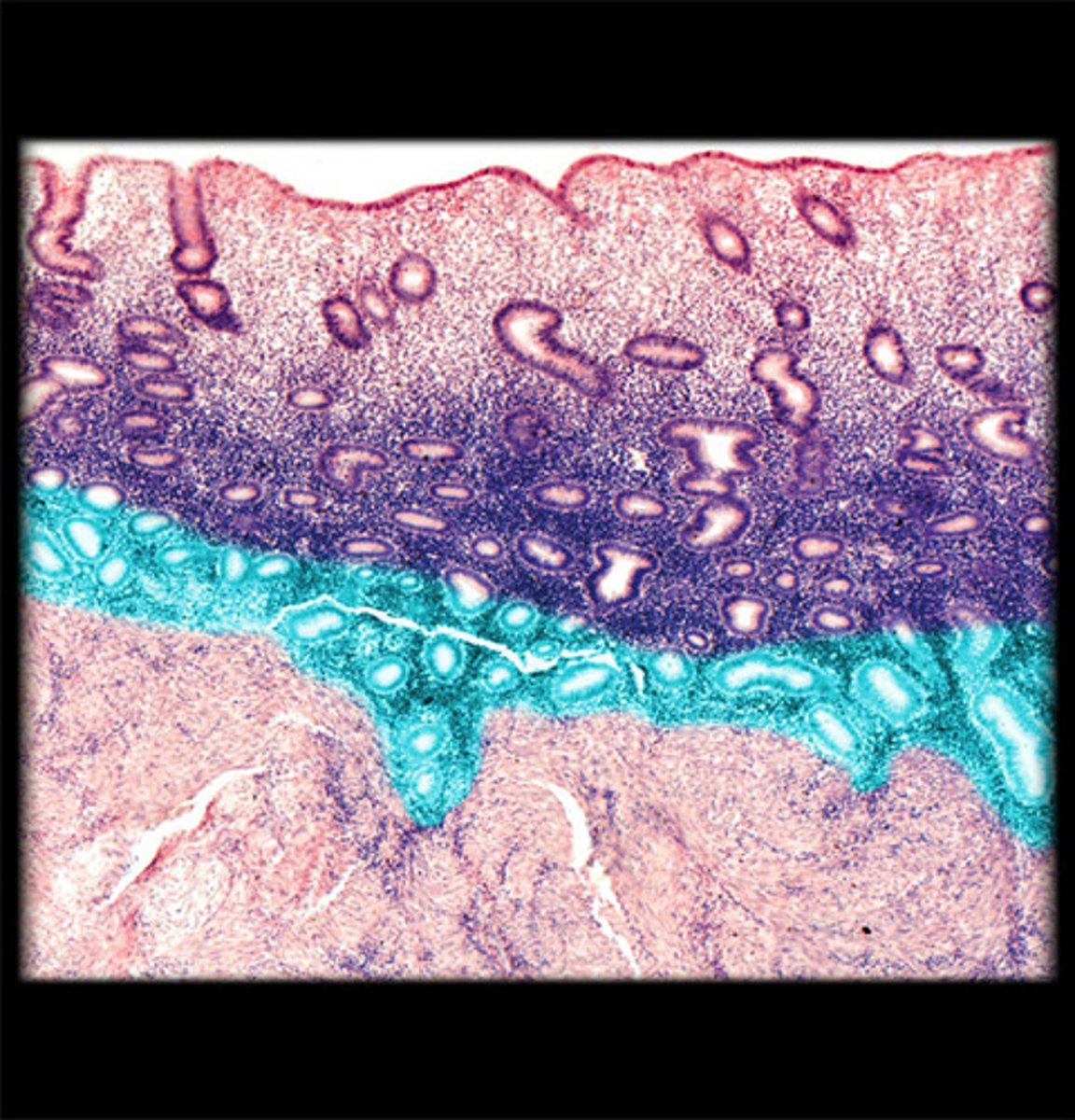
STRATUM FUNCTIONALIS:
Hormone RESPONSIVE superficial layer of endometrium; undergoes functional and morphologic changes throughout menstrual cycle; shed during menses
What is this layer of the Endometrium and what is its function?
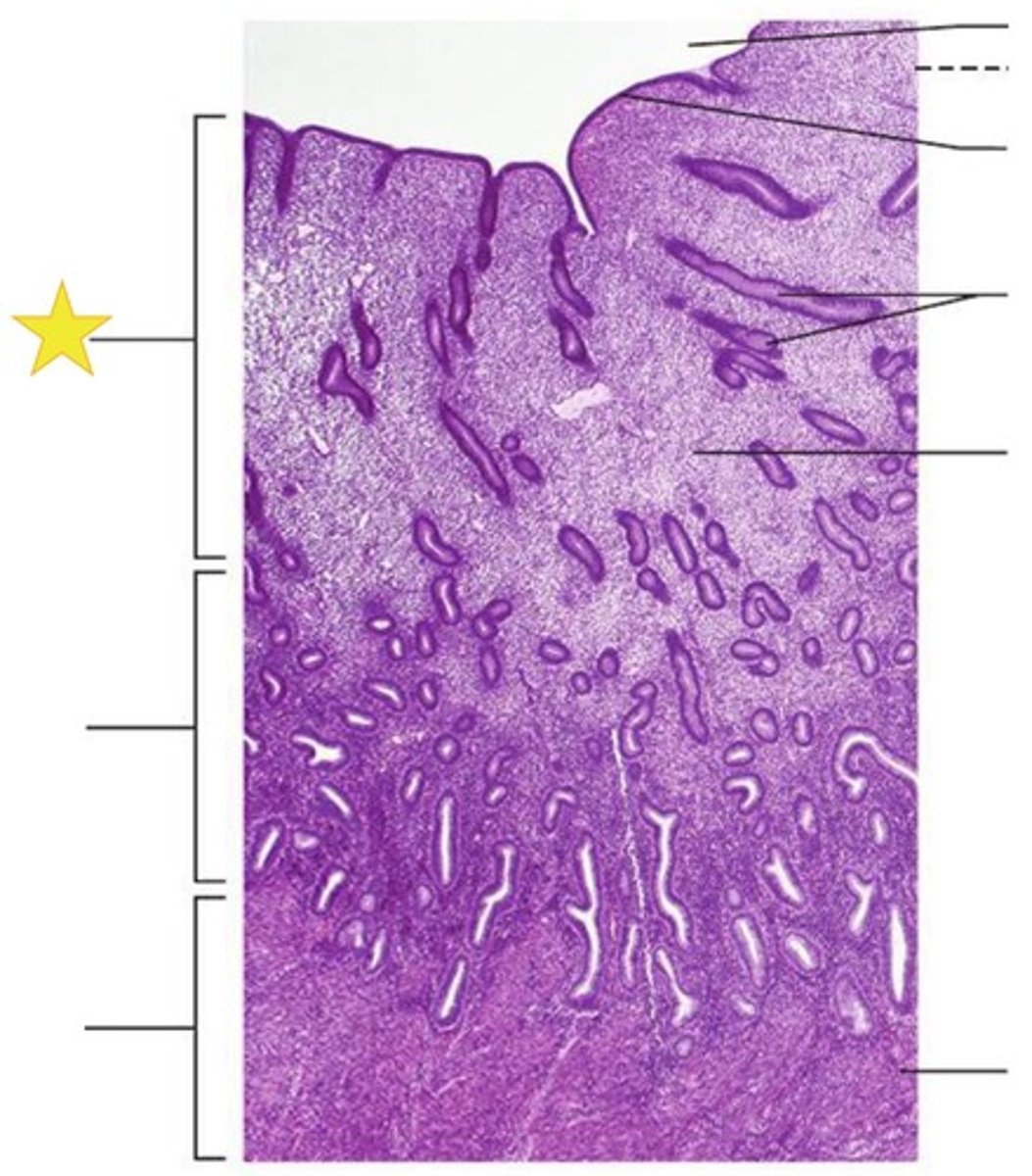
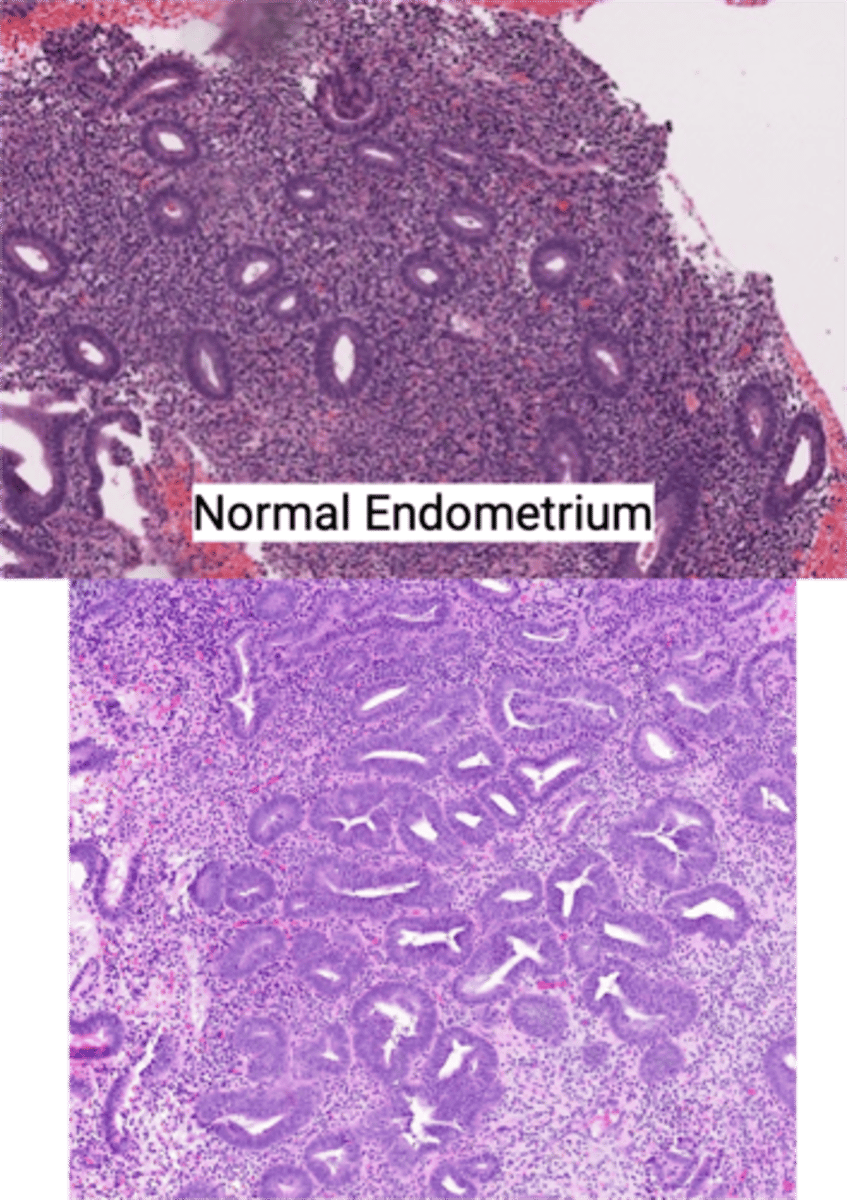
PROLIFERATIVE PHASE
-Tubular glands w/ columnar cells showing pseudostratified nuclei + scattered mitoses
-Dense Stroma
-GROWTH OF PROLIFERATIVE ENDOMETRIAL GLANDS & STROMA (ESTROGEN DRIVEN)
What phase of the menstrual cycle is shown in the Endometrium? Describe it
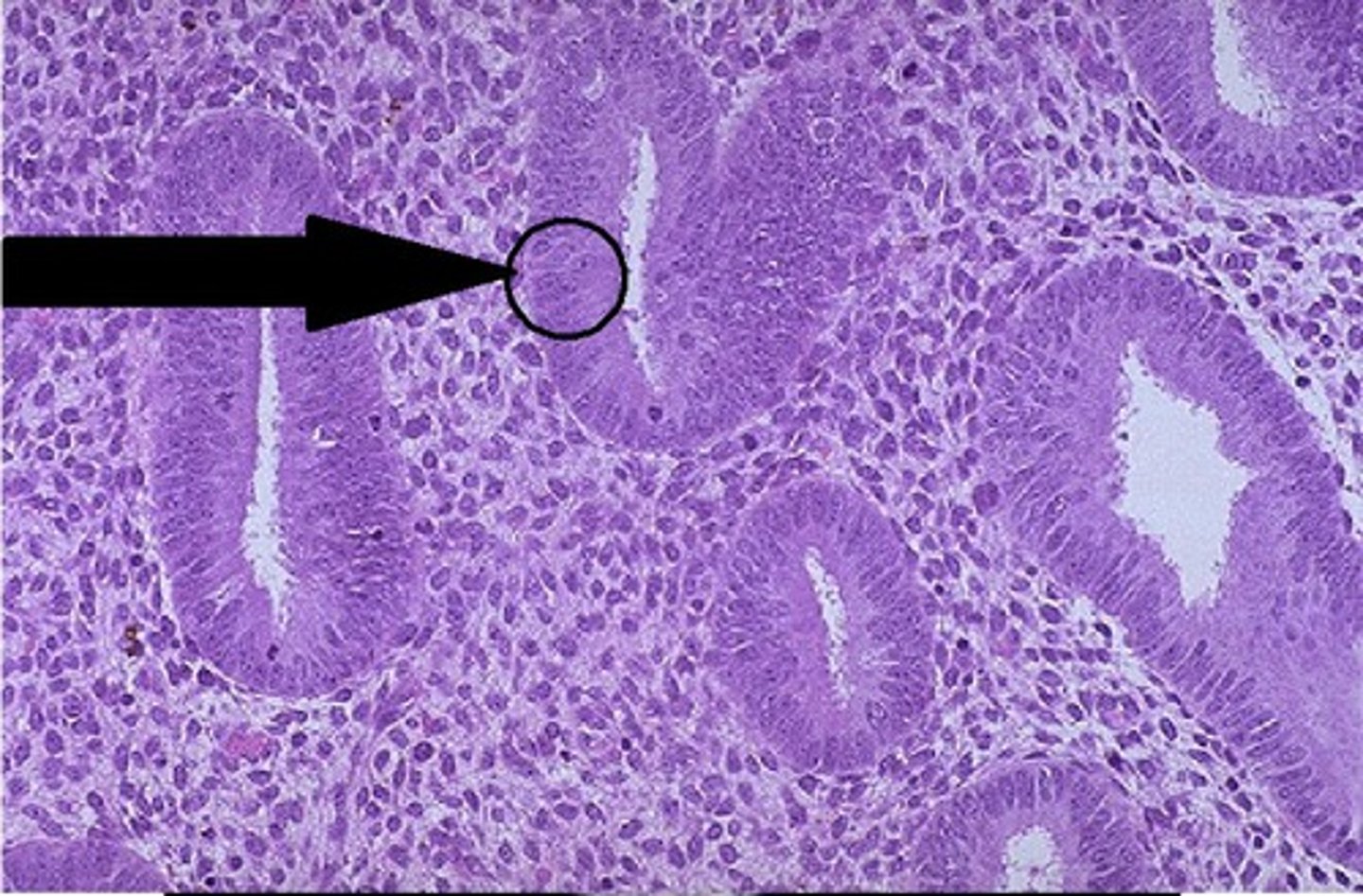
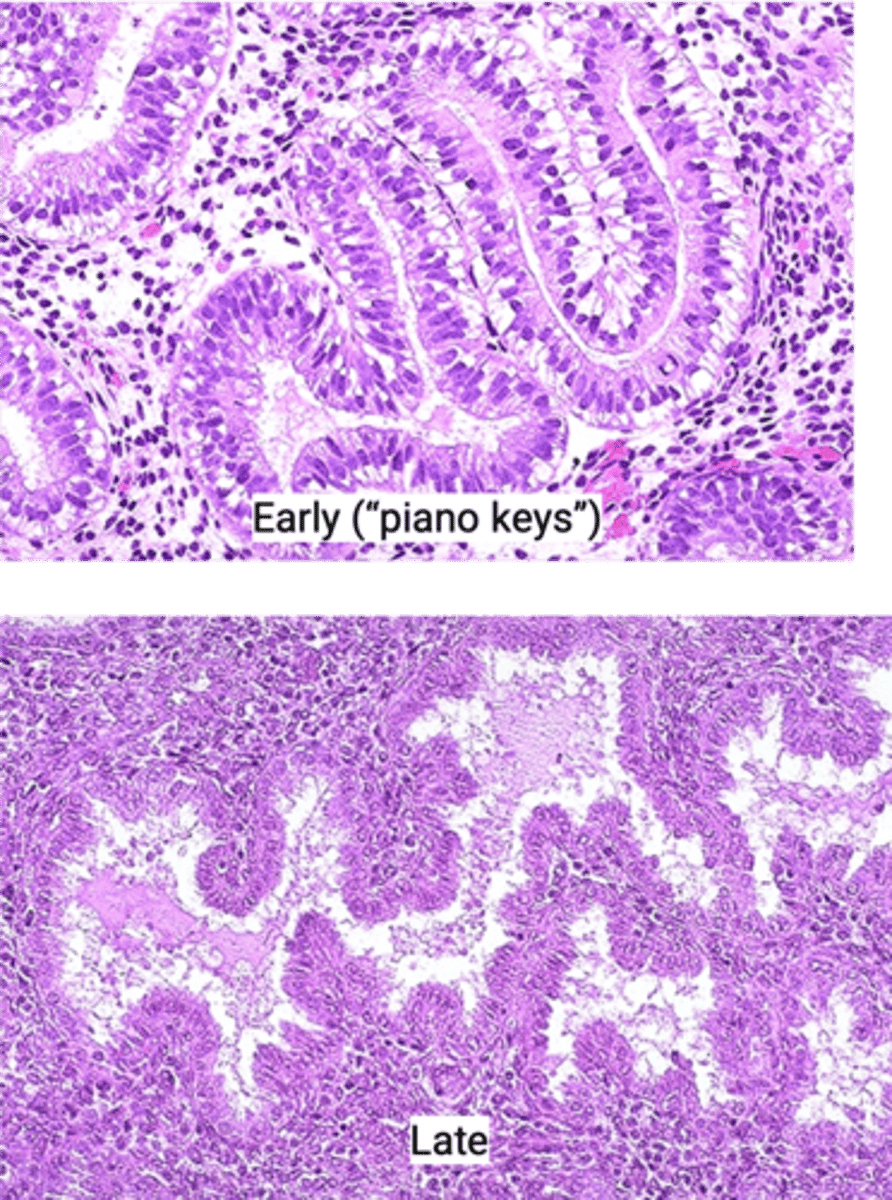
EARLY SECRETORY (Piano keys - aka glands w/ prom subnuclear vacuoles) --> MID-LATE SECRETORY (tortuous glands w/ lots intraluminal secretions + precidual changes to stroma)
PROGESTRONE DRIVEN (prep for implantation)
What phase of the menstrual cycle is shown in the Endometrium? Describe it
ACUTE Endometritis
Define Condition:
NEUTROPHILIC INFILTRATION of endometrium
-Hx: UNCOMMON
-Path: D/t Bacterial Infex related to retain POC after miscarriage OR delivery (nidus for infex)
Chronic Endometritis
Define Condition:
LYMPHOCYTIC Infiltration of Endometrium
-Hx/Path: From retained POC, Ascending Infex (Chlamydia/Gonorrhea), or IUD
-Dx: Lymphocytes + Plasma Cells
> If Granulomatous = Histiocytes (seen in TB/Immunocomp pts)
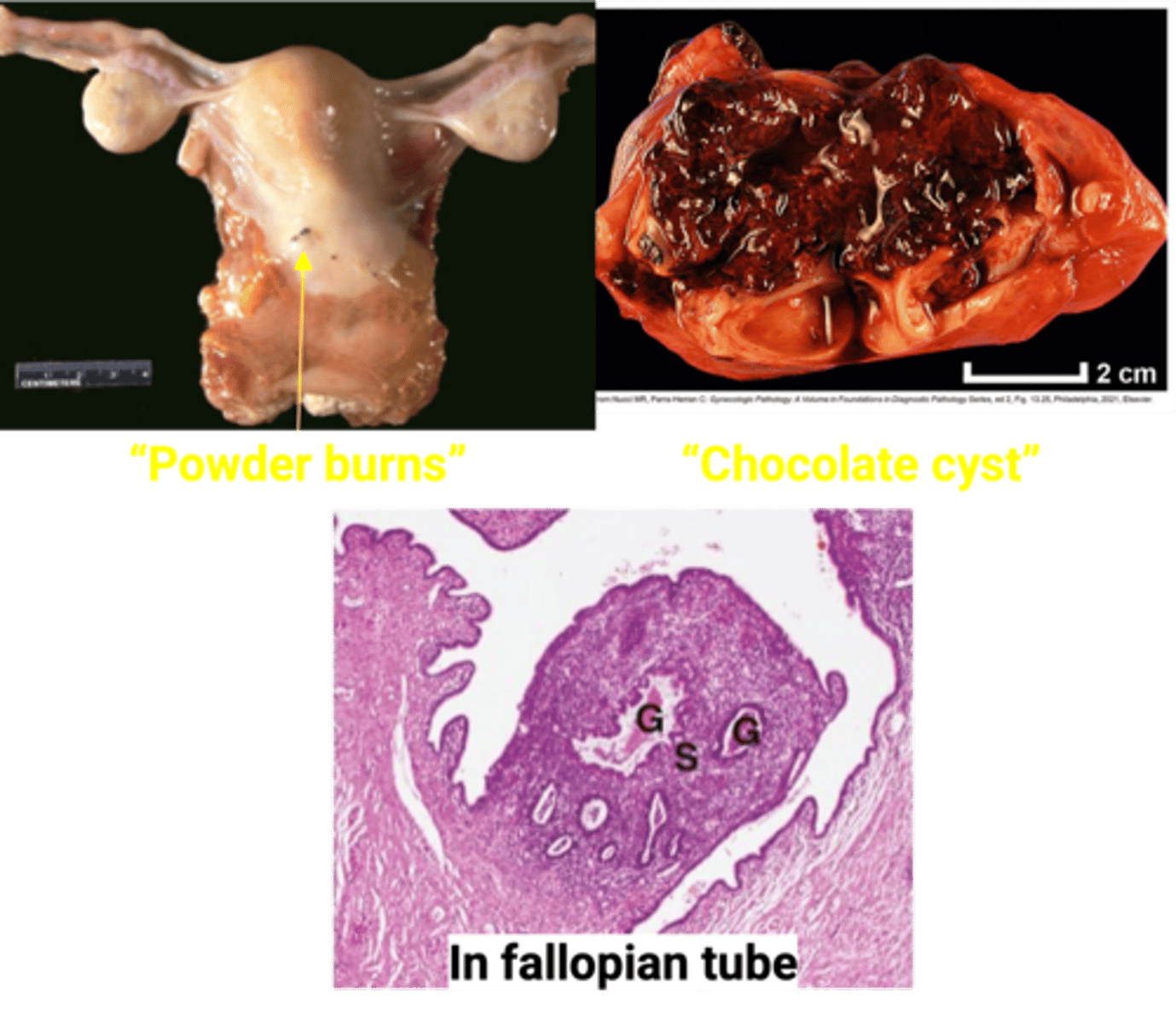
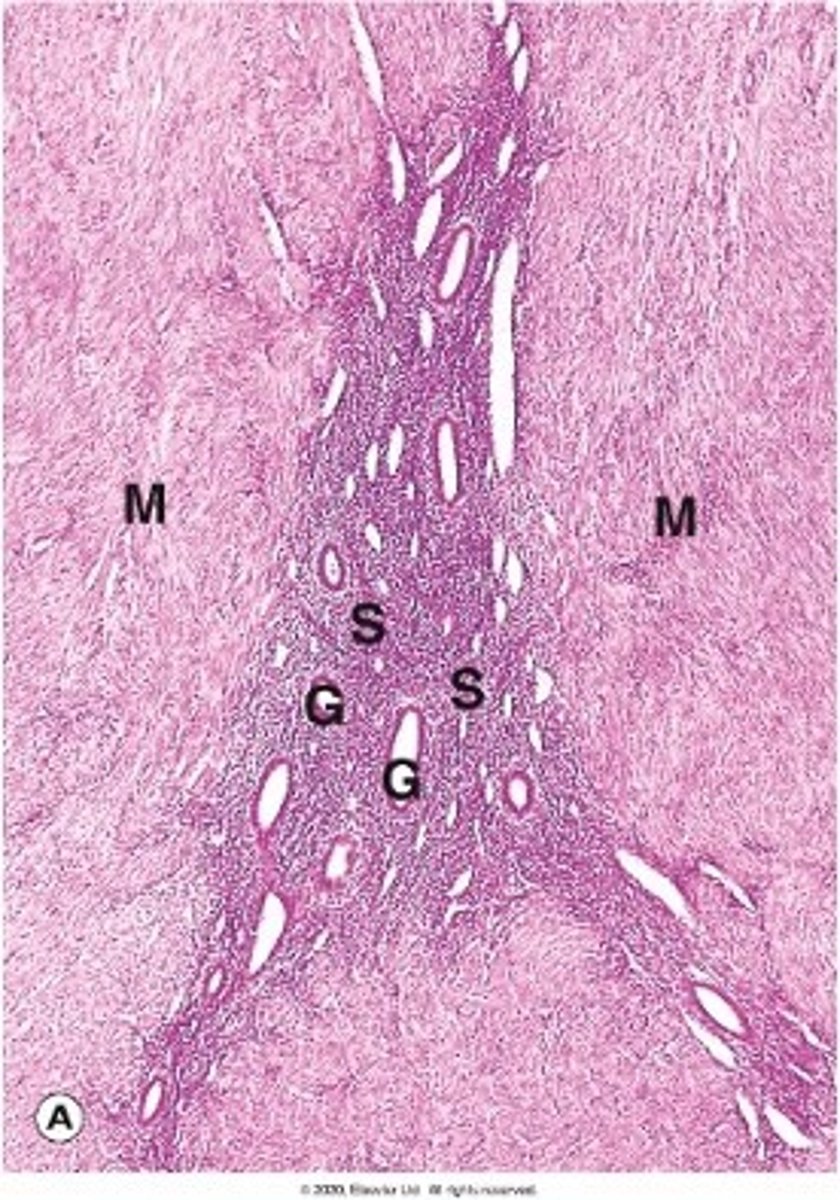
Endometriosis
Define Condition:
Presence of endometrial glands and stroma outside the uterus
-Hx:
> 10% of Reproductive Age Women
-Path:
> Theories:
>> Retrograde menstruation
>> Metastasis
>> Coelomic metaplasia of multipotent cells
> ANYWHERE (usually multifocal); Common Locations:
>> Ovary (MC Site)
>> Ant/Post cul de sac
>> Post Broad Ligaments/Uterosacral Ligaments
>> Fallopian Tubes
-Sx/PE: CYCLIC & CHRONIC PAIN
-Dx:
> Gross
>> Dark Spots (Foci look like "powder burns or gunshots")
>> May see Endometriomas (chocolate cysts)
>> Normal sized uterus
> Micro:
>> Endometrial glands and stroma +/- Hemosiderin (CHRONIC HEMORRHAGE)
-Prog:
> Infertility (esp if in ovarian/tubes --> obstruction from keeping egg fertilized)
> RISK OF CARCINOMA at SITE (esp at OVARY)
Adenomyosis
Define Condition:
Endometrial tissue in the myometrium
-Hx:
> Endometriosis in other sites
-Path: May be due to invagination of basal layer of endometrium or metaplasia of remnant progenitor cells
-Sx/PE: Abn Bleeding & Pain
-Dx:
> Gross: Enlarged Uterus + Thickened Uterine Wall
Endometrial Polyp
Define Condition:
Hyperplastic protrusion of endometrium
-Hx: A/w TAMOXIFEN (Anti-estrogenic effects on breast BUT weak pro-estrogenic effects on endometrium)
-Path: MOSTLY Benign
-Sx/PE:
> Usually Asx
> Abn Uterine Bleeding
-Dx: Histo = Polypoid endometrial lesion with thick walled blood vessels and cystically dilated glands
NON-ATYPICAL Endometrial Hyperplasia
Define Condition:
Increased gland to stroma ratio or glandular density
-Hx: Prolonged excess estrogen unopposed by Progesterone
> Obesity
> PCOS
> Estrogen Hormone Tx
-Dx: Histo
> Hyperplasia WITHOUT Atypia
> ONLY ARCHITECTURAL changes -> MORE glandular density, crowded glands but nuclei look normal
-Prog: 1-3% progress to endometrioid endometrial adenocarcinoma
> Increasing molecular abnormalities (PTEN, MLH1, and KRAS) play a role in the development of endometrial endometrioid adenocarcinoma
ATYPICAL Endometrial Hyperplasia
Define Condition:
Increased gland to stroma ratio or glandular density
-Hx: Prolonged excess estrogen unopposed by Progesterone
> Obesity
> PCOS
> Estrogen Hormone Tx
-Dx: Histo
> Hyperplasia WITH Atypia OR Endometrial Intraepithelia Neoplasia (EIN)
> Architectural changes AND atypical nuclei -> ↑↑ glandular density, back-to-back glands and enlarged, rounded nuclei with open chromatin and prominent nucleoli
-Prog: Dependent on CELLULAR ATYPIA
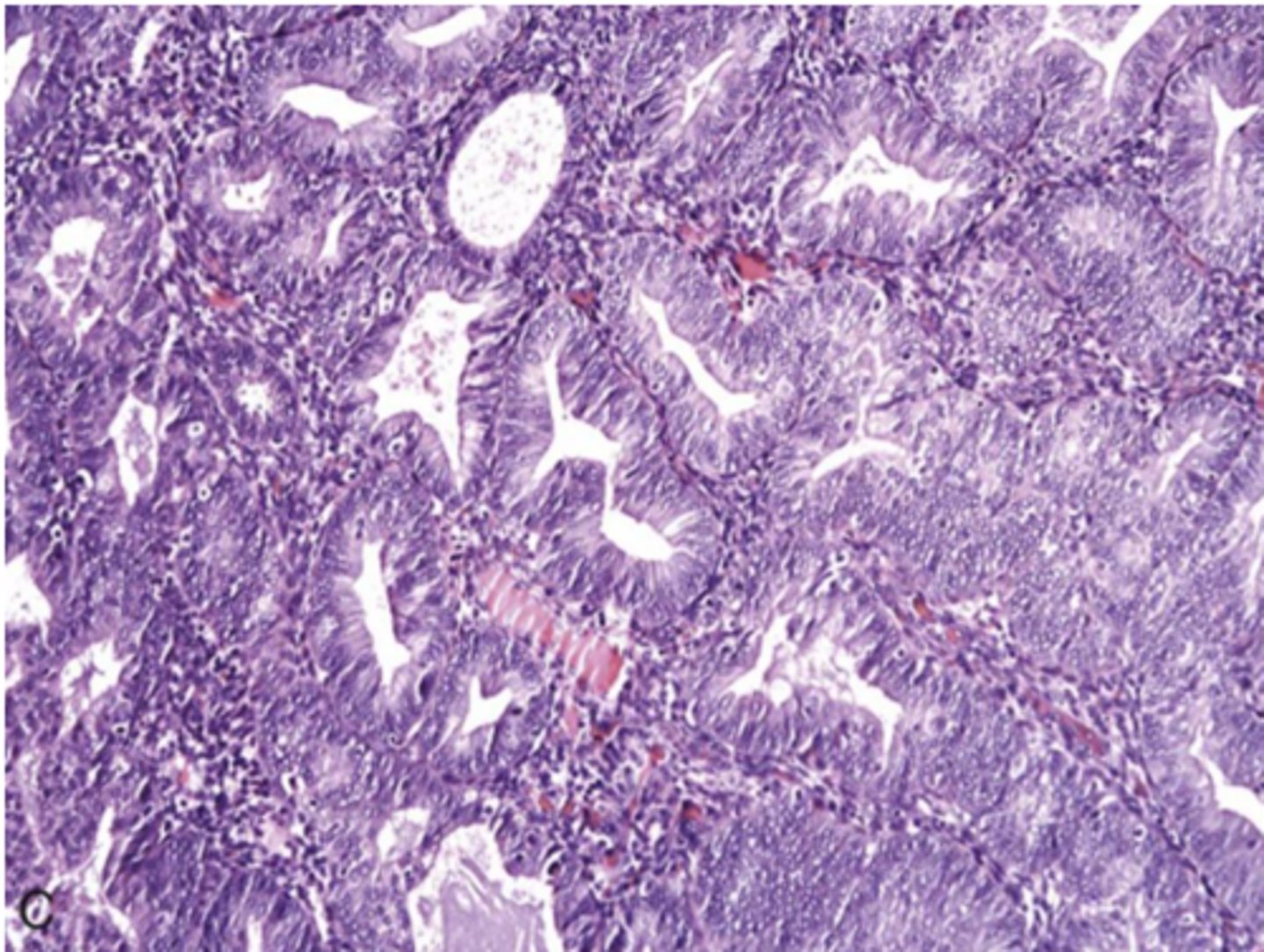
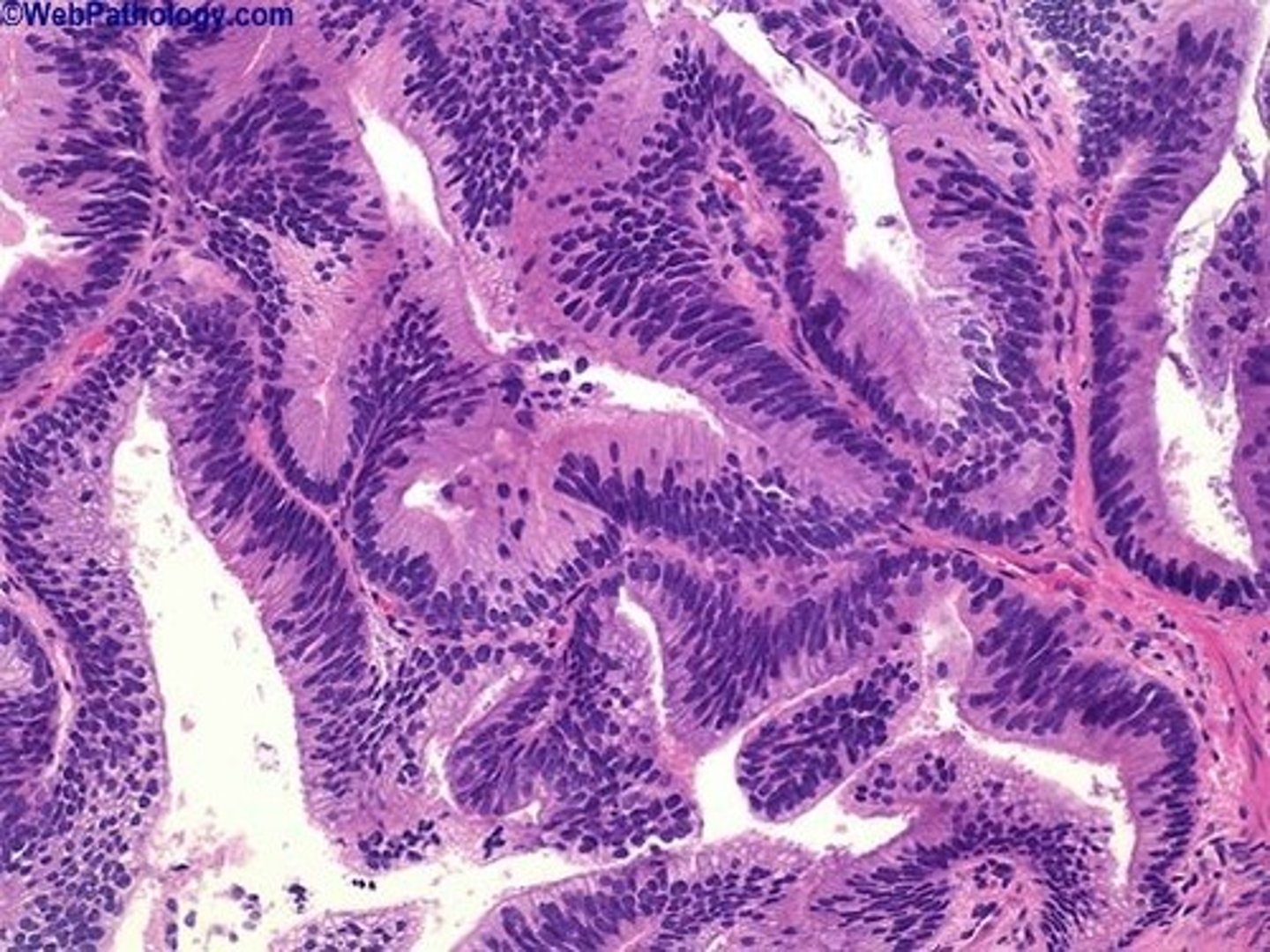
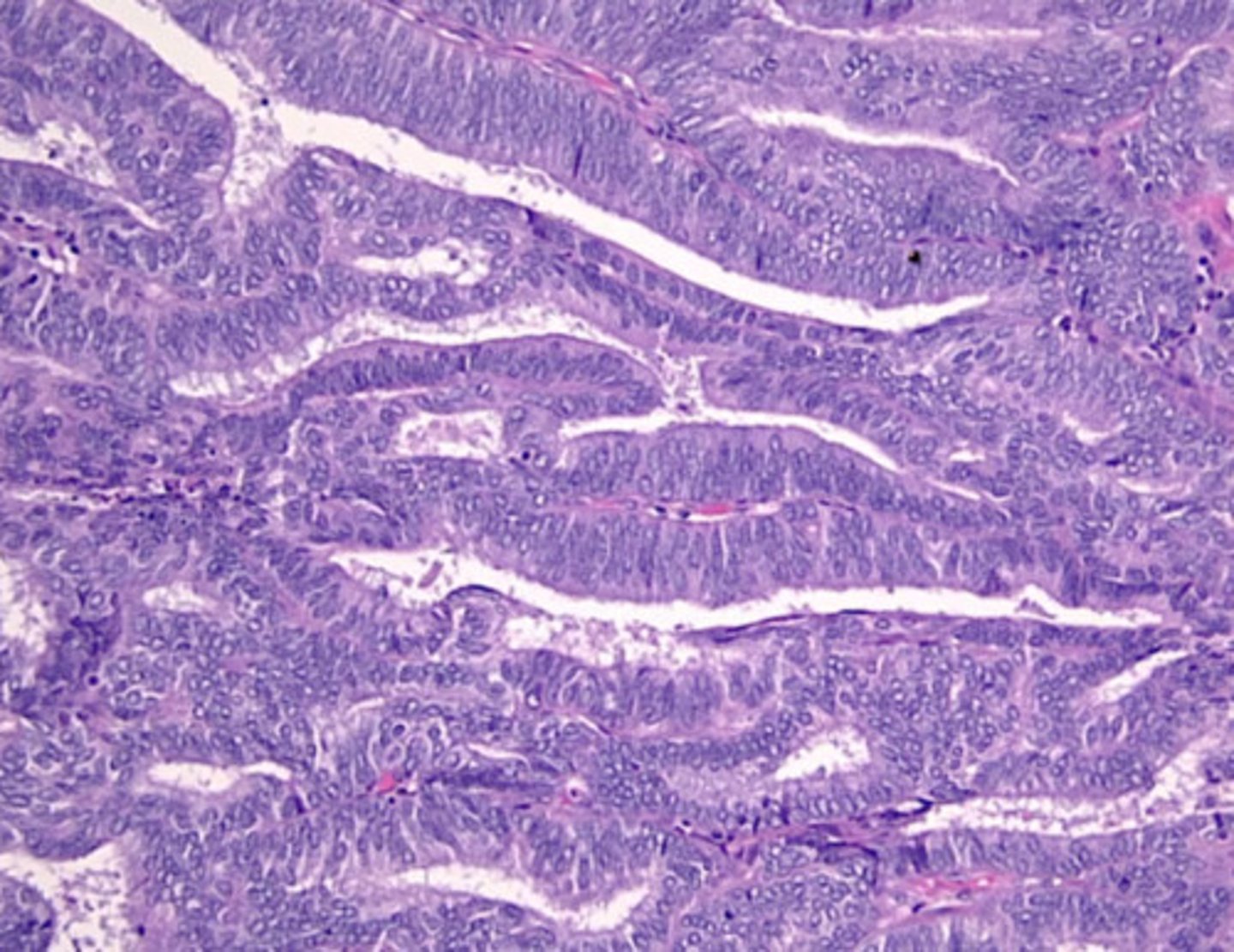
Endometrial Adenocarcinoma
Define Condition:
MC Gynecological Cancer in Resource Rich countries
-Hx:
> Post-Menopausal Females
> A/w PTEN tumor suppressor gene --> INACTIVATION (70%) or DNA mismatch repair gene mutation (Lynch syndrome/HNPCC)
> Exposure...
>> Obesity
>> Early menarche
>> Late menopause
>> NULLPARITY
>> Infertility w/ anovulatory cycle
>> Estrogen secreting ovarian tumors
-Path: Arises from endometrial hyperplasia (ESTROGEN DEPENDENT) --> Spreads via INVASION of myometrium and direct extension into other pelvic organs
-Sx/PE: Abn Uterine Bleeding
-Dx: Histo
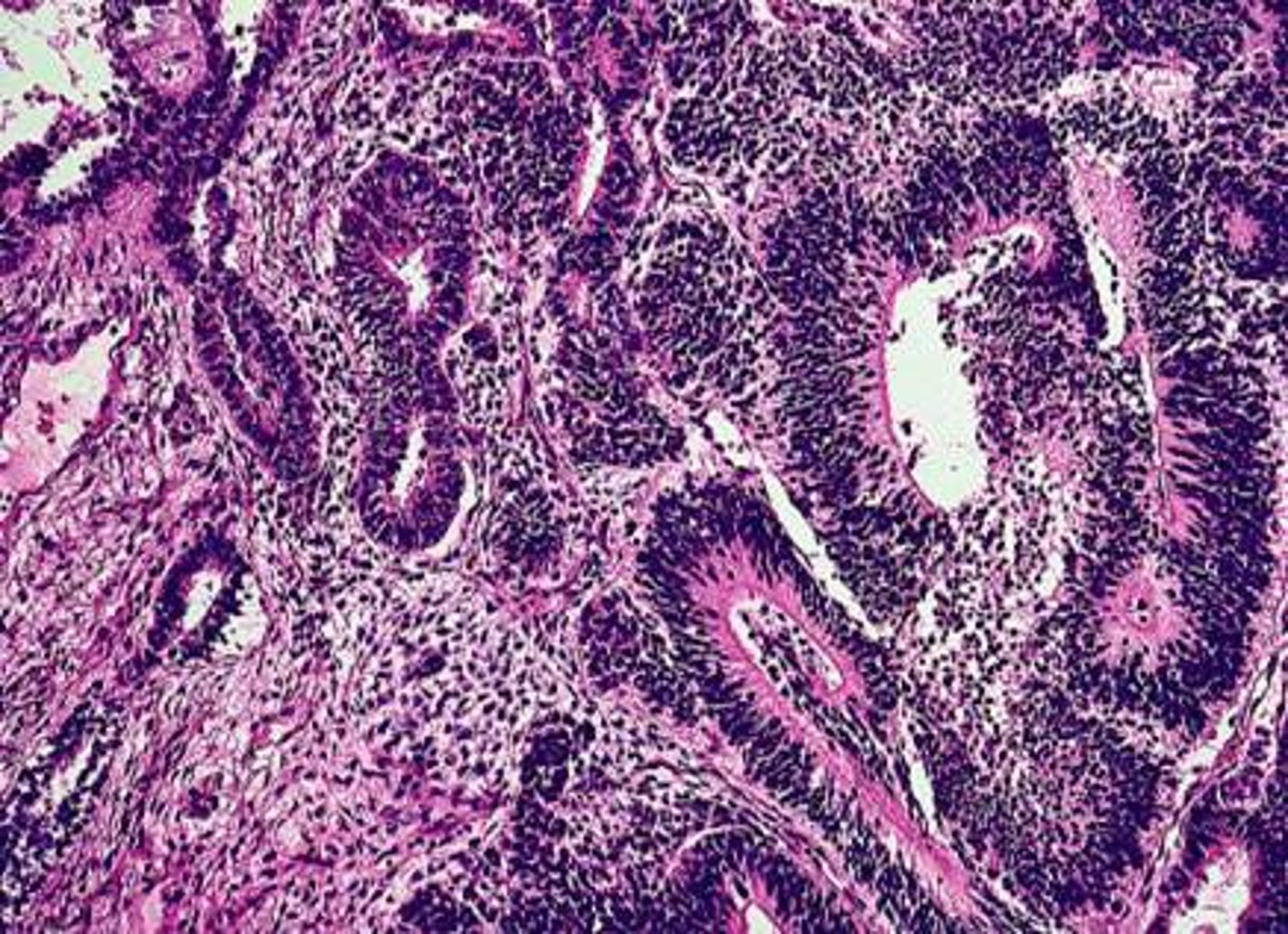
> “Endometrioid” - similar to proliferative endometrium
> Confluent atypical endometrial glands without intervening stroma
-Prog: 90% 5 yr survival with low stage
Endometrial Serous Carcinoma
Define Condition:
MC Gynecological Cancer in Resource Rich countries
-Hx:
> Post-Menopausal Females (70s-80s & Non-Obese)
> 15% of endometrial cancers
> "MOST SERIOUS"
-Path: Serous endometrial intraepithelia carcinoma (SEIC) --> Arise in a setting of endometrial atrophy, NOT estrogenic stimulation
TP53 mutations in 90% of tumors
-Sx/PE: Abn Uterine Bleeding
-Dx: Histo
> Papillary Growth (marked cytologic atypia, atypical mitotic figures, prominent nucleoli)
> Psammoma bodies (round, laminated calcifications)
-Prog: DEPENDENT ON TUMOR STAGE (HIGH STAGE --> POOR PROGNOSIS)
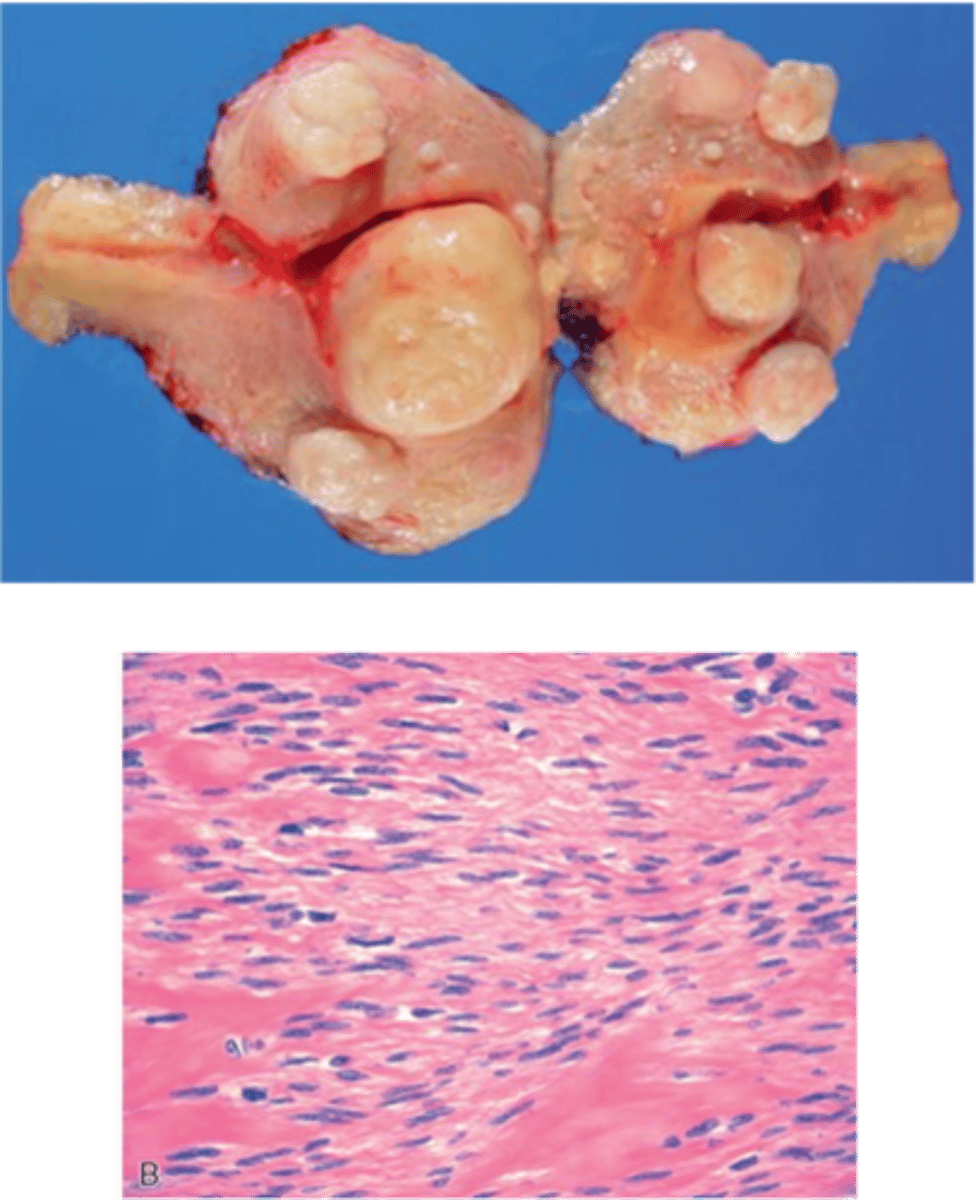
Leiomyoma (AKA Fibroid)
Define Condition:
Benign smooth muscle tumor
-Hx:
> MC Gyno Tumor
> Pre-menopausal women
-Path: Growth stimulated by ESTROGEN
-Sx/PE:
> Asx
> Abn Uterine Bleeding
> Pelvic Pain
> Infertility
-Dx:
> Gross:
>> Rubbery, yellow-white "WHORLED" nodules
>> Multiple nodules
>> Can areas of degeneration
> Histo: Whorled bundles of smooth muscle in a “school of fish” or fascicular pattern, rare mitoses, long slender nuclei
-Tx:
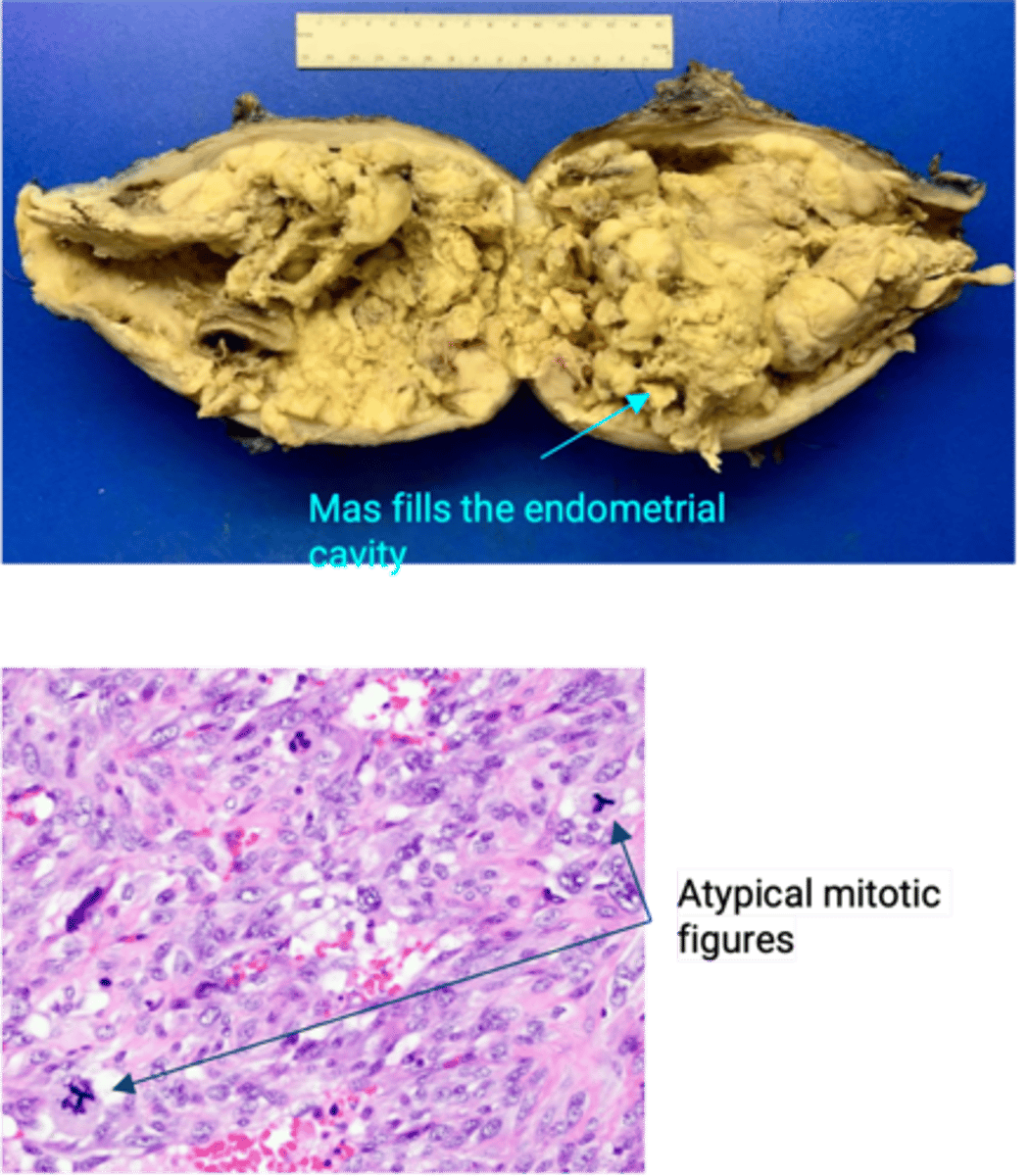
Leiomyosarcoma
Define Condition:
Malignant smooth muscle tumor
-Hx:
> UNCOMMON
> Postmenopausal women
-Path: Arise DE NOVO (NOT from leiomyoma)
-Dx:
> Gross: Malignant smooth muscle tumor
> Histo: nuclear atypia, increased mitotic activity, and necrosis
-Prog:
> Depends on TUMOR GRADE
> High recurrence rate with 50% of tumors metastasizing to lung, brain, and bone - Can disseminate through abdominal cavity
Benign Paratubal Cysts
Define Condition:
MC Benign Lesions in Fallopian Tubes

Salpingitis
Define Condition:
Inflammation of Fallopian Tubes
-Hx: MCC = Gonorrhea (60%) and Chlamydia
-Prog:
> TOA --> Adhesions & Infertility
> Risk of Ectopic Pregnancy
Serous Carcinoma of Fallopian Tubes
Define Condition:
-Path:
> Mutation = TP53
>> If BRCA1/2 mutation --> High Grade
> Precursor lesions = Serous Tubal Intraepithelial Carcinoma (STIC)
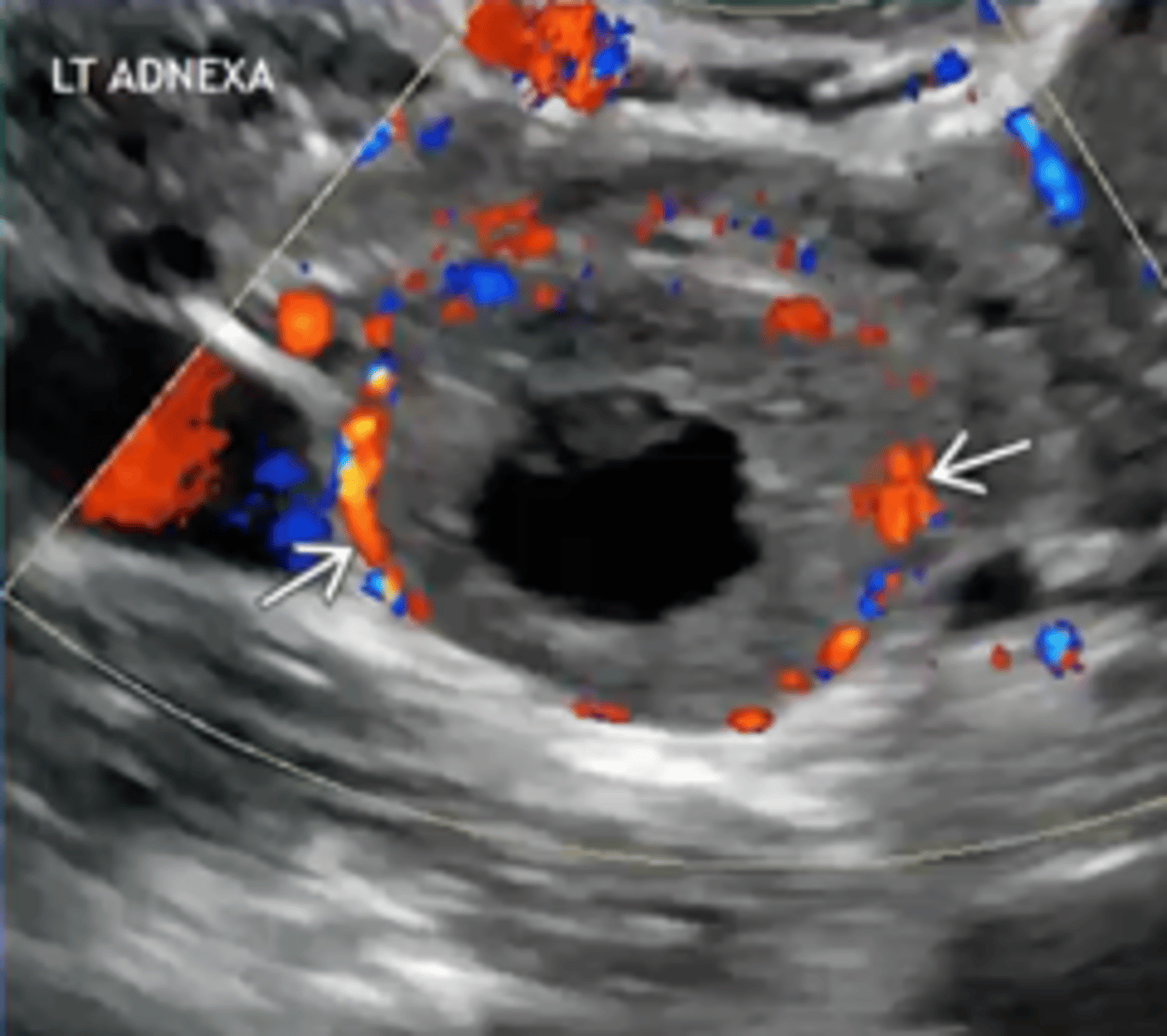
Follicular Ovarian Cyst
Define Condition:
-Hx:
> Usually functional (result of ovulation)
> MC Ovarian mass in Young Females
-Path: D/t failure of follicule to rupture and ovulate
> Lined with Granulosa cells ==> Excess Estrogen
-Sx/PE: Asx (may rupture/hemorrhage --> Adnexal Torsion)
-Prog: Resolves spontaneously
Corpus Luteal Ovarian Cyst
Define Condition:
-Path: D/t failure of corpus luteum to involute after ovulation ==> Excess Progesterone
-Sx/PE: Asx (may rupture/hemorrhage --> Adnexal Torsion)
-Prog: Resolves spontaneously
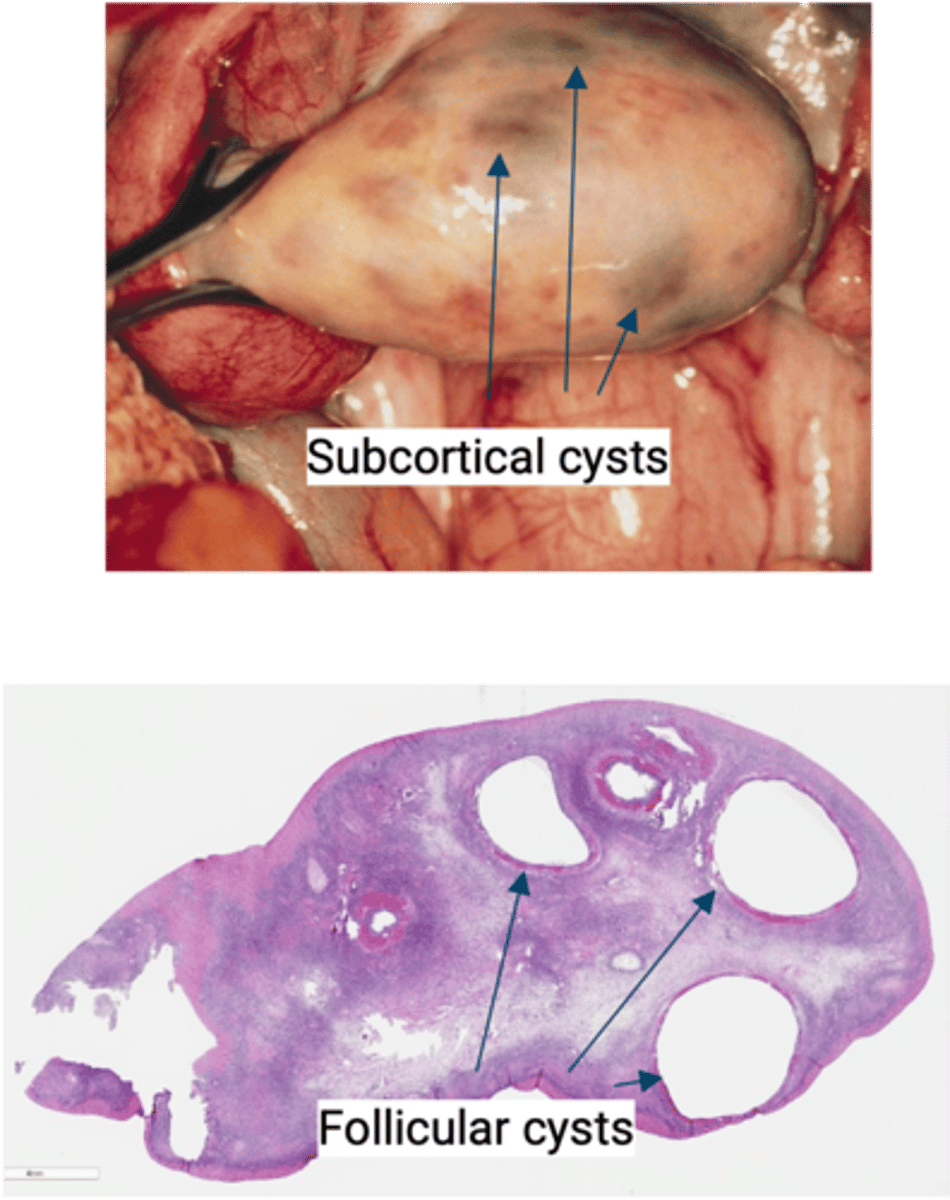
Polycystic Ovarian Syndrome (PCOS)
Define Condition:
Multiple ovarian follicular cysts due to hormone imbalance
-Hx:
> A/w insulin resistance
> Obese, Young Women
-Path:
> High BMI -> insulin resistance -> may cause abnormal GnRH pulsation -> ↑LH -> theca cells to ↑androgens
> Estrone feedback ==> Decreased FSH ==> Cystic degeneration of follicles --> Multiple follicular cysts & anovulation ==> Risk of Endometrial Cancer
-Sx/PE:
> Hirsutism (d/t Increased Androgens)
> Infertility
> Oligomenorrhea
-Dx:
> Labs:
>> LH = HIGH (LH:FSH > 2)
>> FSH = LOW
> Gross: Enlarged ovaries studded with subcortical cysts, lack of corpus luteum cysts due to anovulation
> Histo: multiple variably sized follicular cysts
-Prog:
> Endometrial Cancer Risk
> T2DM (Insulin Resistance) in 10-15 yrs
Ovarian Surface Epithelial Tumors (from coelomic epithelium lining ovary)
What are the most common type of ovarian tumors?
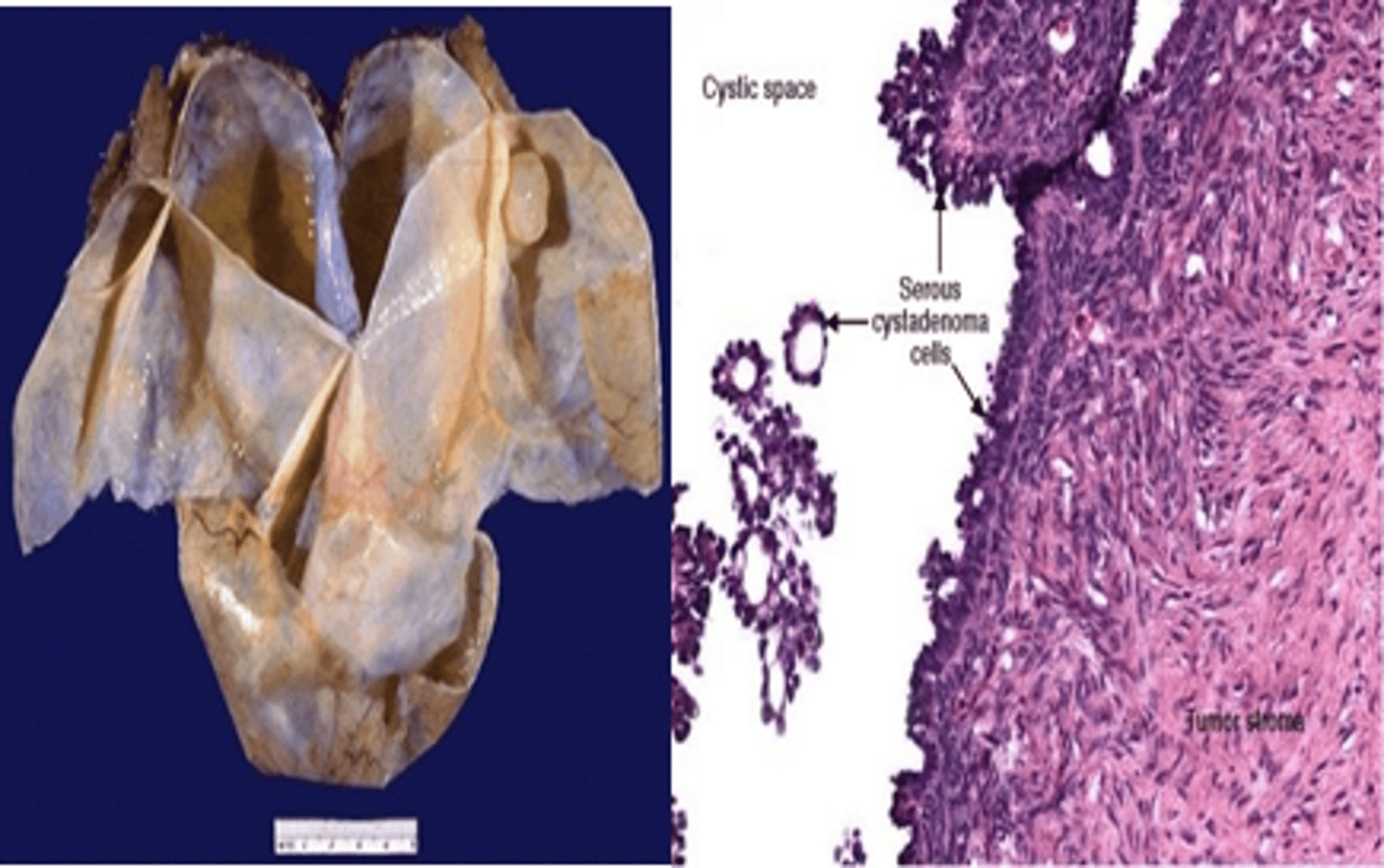
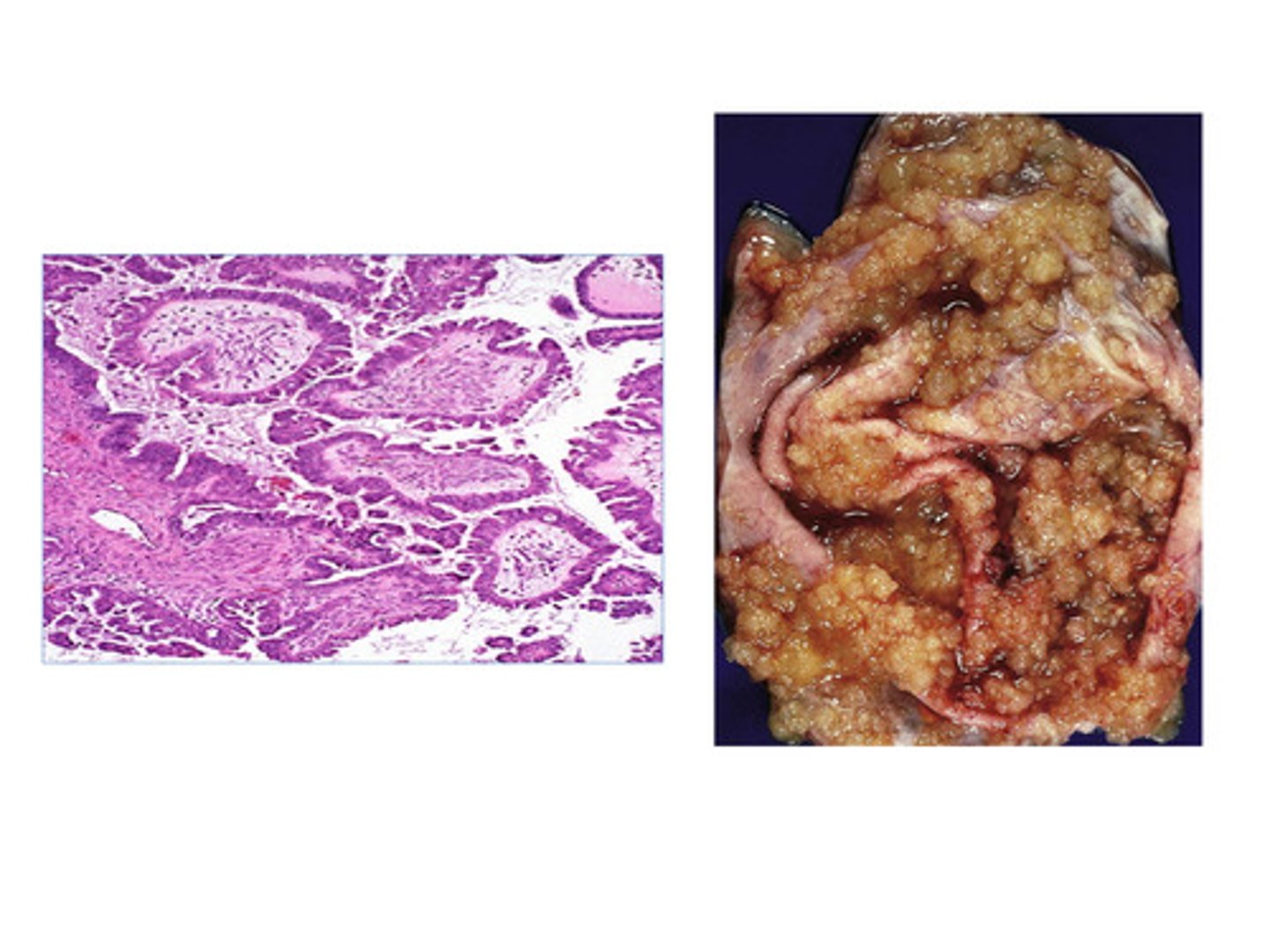
Serous Cystadenoma
Define Type of Ovarian Surface Epithelial Tumor:
MC Ovarian Neoplasm - single cyst w/ simple flat lining
-Hx:
> MC in PREMENOPAUSAL WOMEN (30-40 y/o)
> More ovulation --> More Risk
>> Advanced age
>> Early Menarche
>> Late Menopause
>> Nulliparity
>> FHx
>> BRCA mutations
>> Lynch Syndrome
> Protective Factors
>> Pregnancy
>> Breastfeeding
>> OCPs
-Path: Type 1 Carcinoma (low grade)
-Sx/PE:
> Late & Vague Abd Sx (Pain & Fullness)
> Urinary Frequency (Compression)
> Spreads LOCALLY
-Dx:
> 25% Bilateral
> Labs = CA-125 Tumor Marker (used to MONITOR TX RESPONSE & SCREEN FOR RECURRENCE)
> May see Psammoma bodies (when papillary structures calcify)
Serous Borderline Tumor
Define Type of Ovarian Surface Epithelial Tumor:
In Btwn Serous Cystadenoma and Carcinoma
-Hx:
> More ovulation --> More Risk
>> Advanced age
>> Early Menarche
>> Late Menopause
>> Nulliparity
>> FHx
>> BRCA mutations
>> Lynch Syndrome
> Protective Factors
>> Pregnancy
>> Breastfeeding
>> OCPs
-Path: Type 1 Carcinoma (low grade)
-Sx/PE:
> Late & Vague Abd Sx (Pain & Fullness)
> Urinary Frequency (Compression)
> Spreads LOCALLY
-Dx:
> Labs = CA-125 Tumor Marker (used to MONITOR TX RESPONSE & SCREEN FOR RECURRENCE)
> May see Psammoma bodies (when papillary structures calcify)
-Prog: Better prognosis than malignant tumors, but still metastatic potential
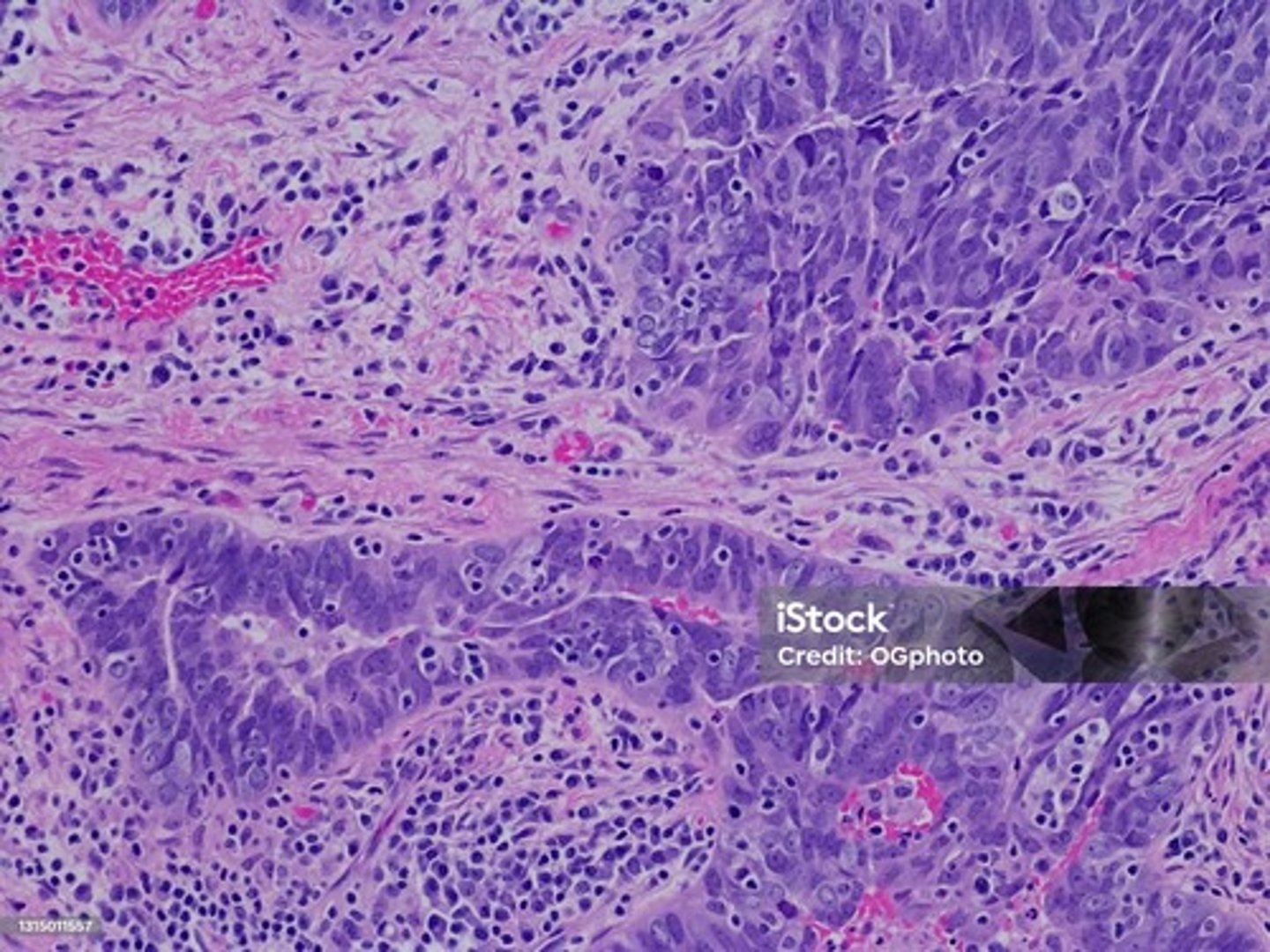
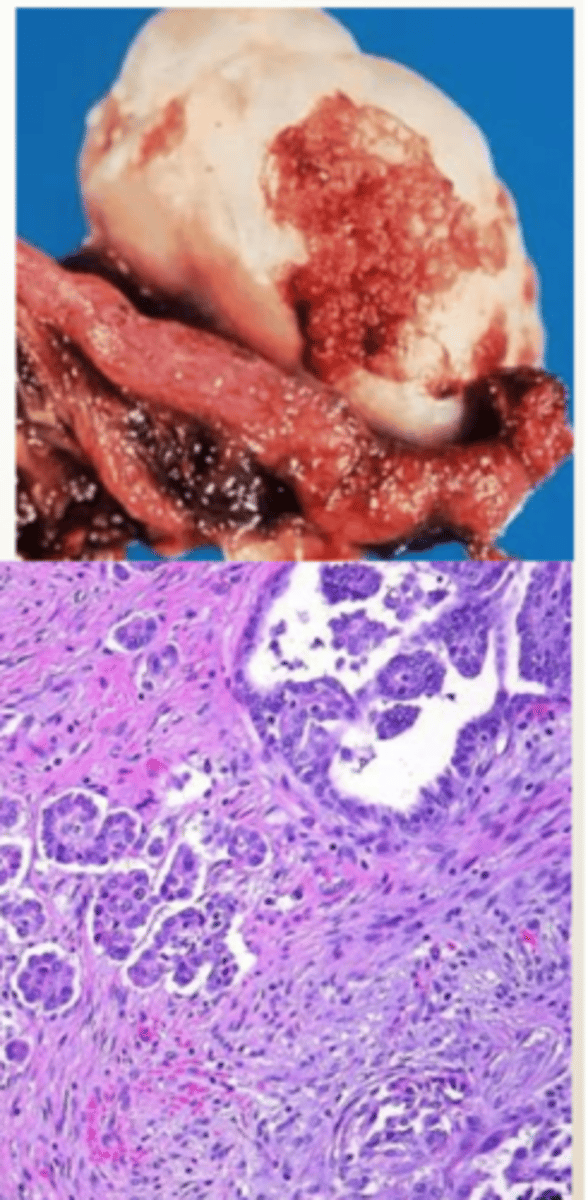
Serous Carcinoma
Define Type of Ovarian Surface Epithelial Tumor:
MC MALIGNANT Ovarian Neoplasm - Complex cysts with a thick, shaggy lining
-Hx:
> MC in POSTMENOPAUSAL WOMEN (60-70s)
> More ovulation --> More Risk
>> Advanced age
>> Early Menarche
>> Late Menopause
>> Nulliparity
>> FHx
>> BRCA mutations
>> Lynch Syndrome
> Protective Factors
>> Pregnancy
>> Breastfeeding
>> OCPs
-Path: Type 1 (low grade) OR Type 2 Carcinoma (high grade) arising from STIC
-Sx/PE:
> Late & Vague Abd Sx (Pain & Fullness)
> Urinary Frequency (Compression)
> Spreads LOCALLY
-Dx:
> Labs = CA-125 Tumor Marker (used to MONITOR TX RESPONSE & SCREEN FOR RECURRENCE)
> May see Psammoma bodies (when papillary structures calcify)
-Tx:
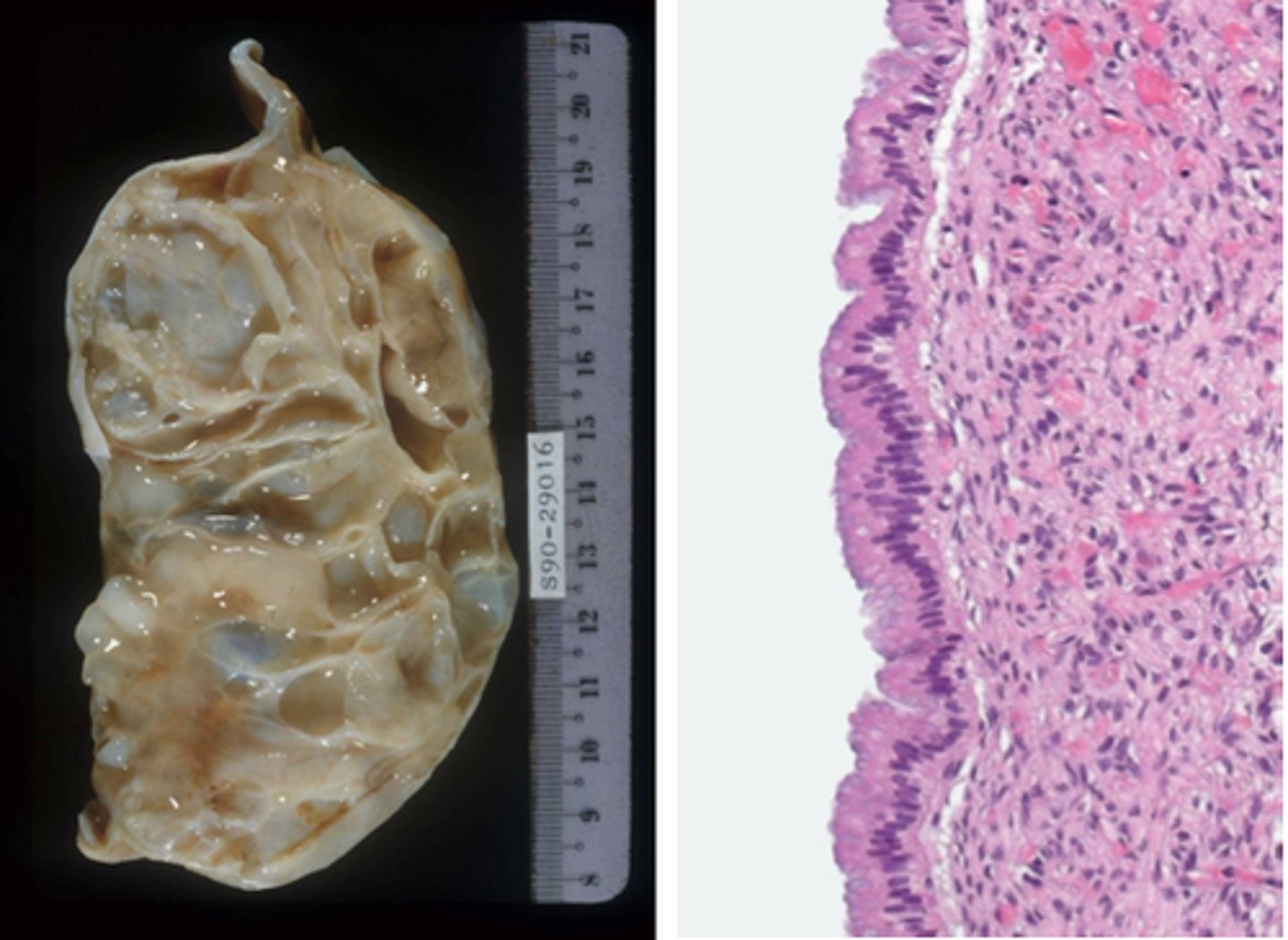
Mucinous Cystadenoma
Define Type of Ovarian Surface Epithelial Tumor:
Large & rarely bilateral BENIGN Tumor lined by mucus secreting epithelium
-Hx:
> More ovulation --> More Risk
>> Advanced age
>> Early Menarche
>> Late Menopause
>> Nulliparity
>> FHx
>> BRCA mutations
>> Lynch Syndrome
> Protective Factors
>> Pregnancy
>> Breastfeeding
>> OCPs
-Path: A/w KRAS mutations
-Sx/PE:
> Late & Vague Abd Sx (Pain & Fullness)
> Urinary Frequency (Compression)
> Spreads LOCALLY
-Dx:
> Labs = CA-125 Tumor Marker (used to MONITOR TX RESPONSE & SCREEN FOR RECURRENCE)
> Gross = Cystic multiloculated masses filled with gelatinous fluid
-Prog: Better Prog than Serous Tumors
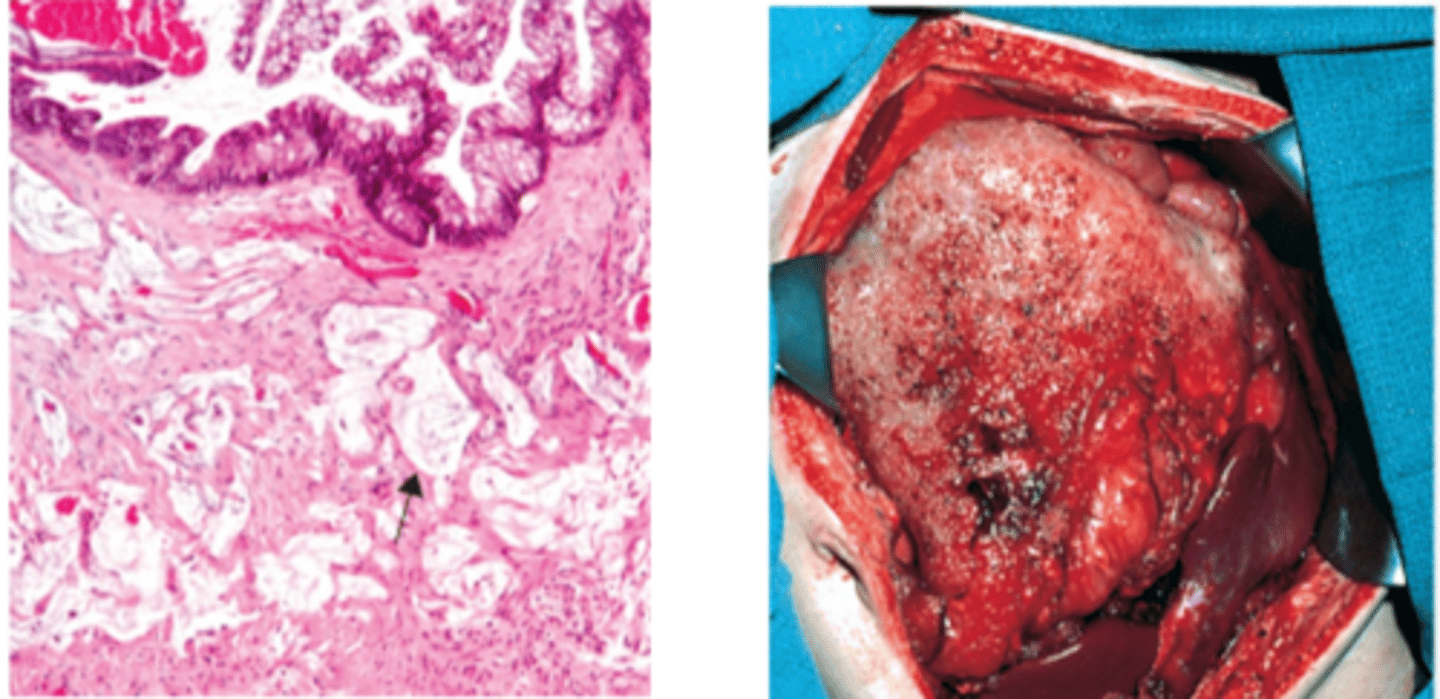
Mucinous Carcinoma
Define Type of Ovarian Surface Epithelial Tumor:
MALIGNANT & RARE Tumor w/ mucus secreting epithelium
-Hx:
> More ovulation --> More Risk
>> Advanced age
>> Early Menarche
>> Late Menopause
>> Nulliparity
>> FHx
>> BRCA mutations
>> Lynch Syndrome
> Protective Factors
>> Pregnancy
>> Breastfeeding
>> OCPs
-Path: A/w KRAS mutations
-Sx/PE:
> Late & Vague Abd Sx (Pain & Fullness)
> Urinary Frequency (Compression)
> Spreads LOCALLY
-Dx:
> Labs = CA-125 Tumor Marker (used to MONITOR TX RESPONSE & SCREEN FOR RECURRENCE)
> Gross =
>> Cystic multiloculated masses filled with gelatinous fluid
>> Sometimes cause Pseudomyxoma peritonei "JELLY BELLY"
-Prog: Better Prog than Serous Tumors
Endometrioid Carcinoma
Define Type of Ovarian Surface Epithelial Tumor:
-Hx:
> May have Hx of Endometriosis
> More ovulation --> More Risk
>> Advanced age
>> Early Menarche
>> Late Menopause
>> Nulliparity
>> FHx
>> BRCA mutations
>> Lynch Syndrome
> Protective Factors
>> Pregnancy
>> Breastfeeding
>> OCPs
-Path: MALIGNANT
> A/w PTEN mutations
> 15-30% have synchronous endometrial hyperplasia or endometrioid endometrial carcinoma
-Sx/PE:
> Late & Vague Abd Sx (Pain & Fullness)
> Urinary Frequency (Compression)
> Spreads LOCALLY
-Dx:
> Labs = CA-125 Tumor Marker (used to MONITOR TX RESPONSE & SCREEN FOR RECURRENCE)
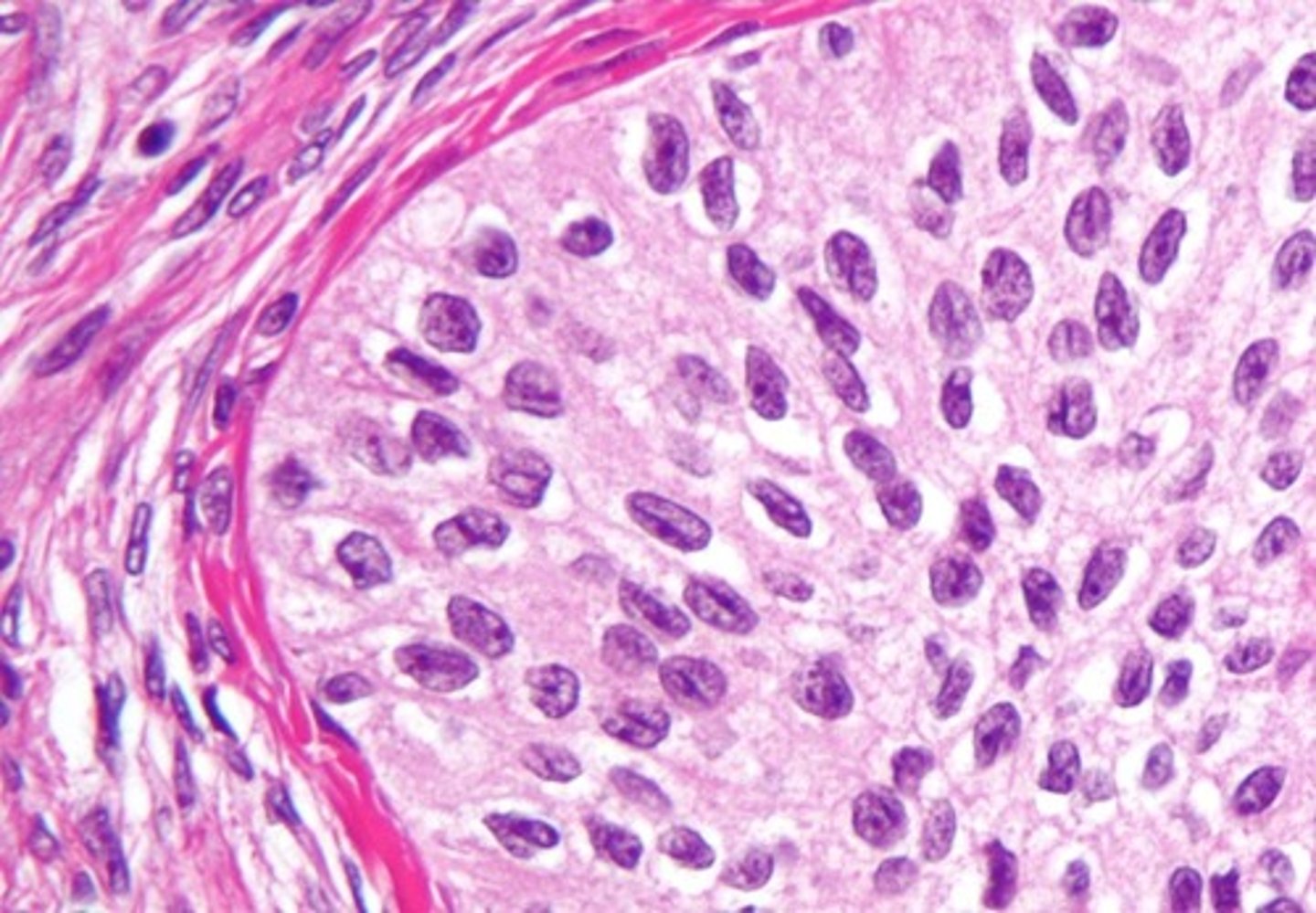
Brenner Tumor
Define Type of Ovarian Surface Epithelial Tumor:
-Hx:
> RARE (Incidental Finding)
> More ovulation --> More Risk
>> Advanced age
>> Early Menarche
>> Late Menopause
>> Nulliparity
>> FHx
>> BRCA mutations
>> Lynch Syndrome
> Protective Factors
>> Pregnancy
>> Breastfeeding
>> OCPs
-Path: BENIGN
-Sx/PE:
> Late & Vague Abd Sx (Pain & Fullness)
> Urinary Frequency (Compression)
> Spreads LOCALLY
-Dx:
> Labs = CA-125 Tumor Marker (used to MONITOR TX RESPONSE & SCREEN FOR RECURRENCE)
> Gross: Tan-yellow cut surface
> Micro: Composed of nests of bladder-like or transitional epithelium with “coffee bean” nuclei
Germ Cell Tumors
What is the SECOND most common type of Ovarian Tumor?
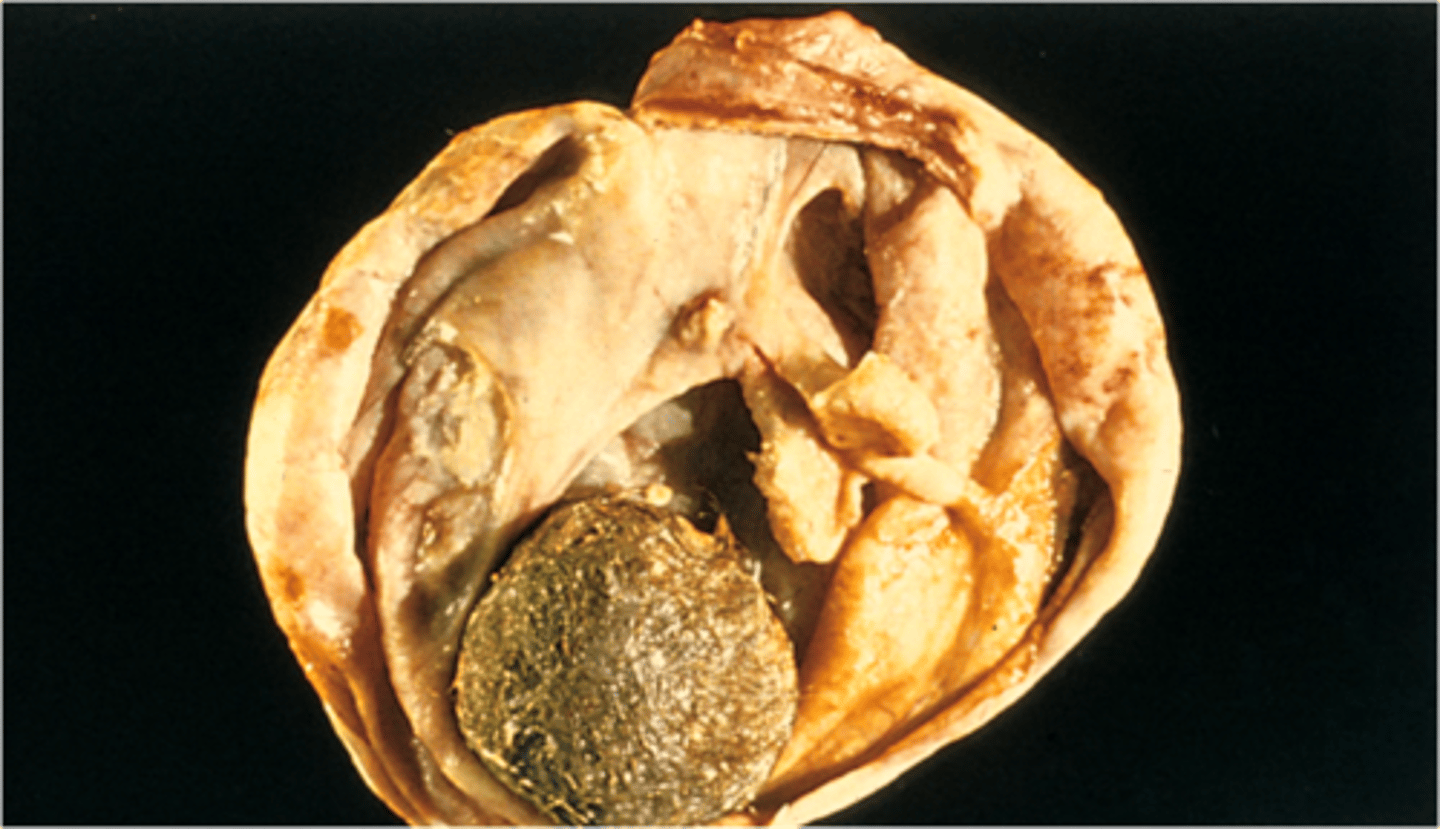
Mature Cystic Teratoma (Dermoid Cyst)
Define Type of Germ Cell Tumor:
BENIGN Germ Cell Tumor; MC Germ Cell Tumor in Young Women
-Hx: Young Women (10-30 y/o)
-Path: Mature tissue representing at least 2 embryonic layers (ectoderm, mesoderm or endoderm):
> Can contain hair, squamous cells, sebaceous (oily) material
> Walls may contain calcification, tooth-like material
-Dx:
> Labs = AFP or Beta-hCG Markers
-Prog:
> MC = Squamous Cell Carcinoma
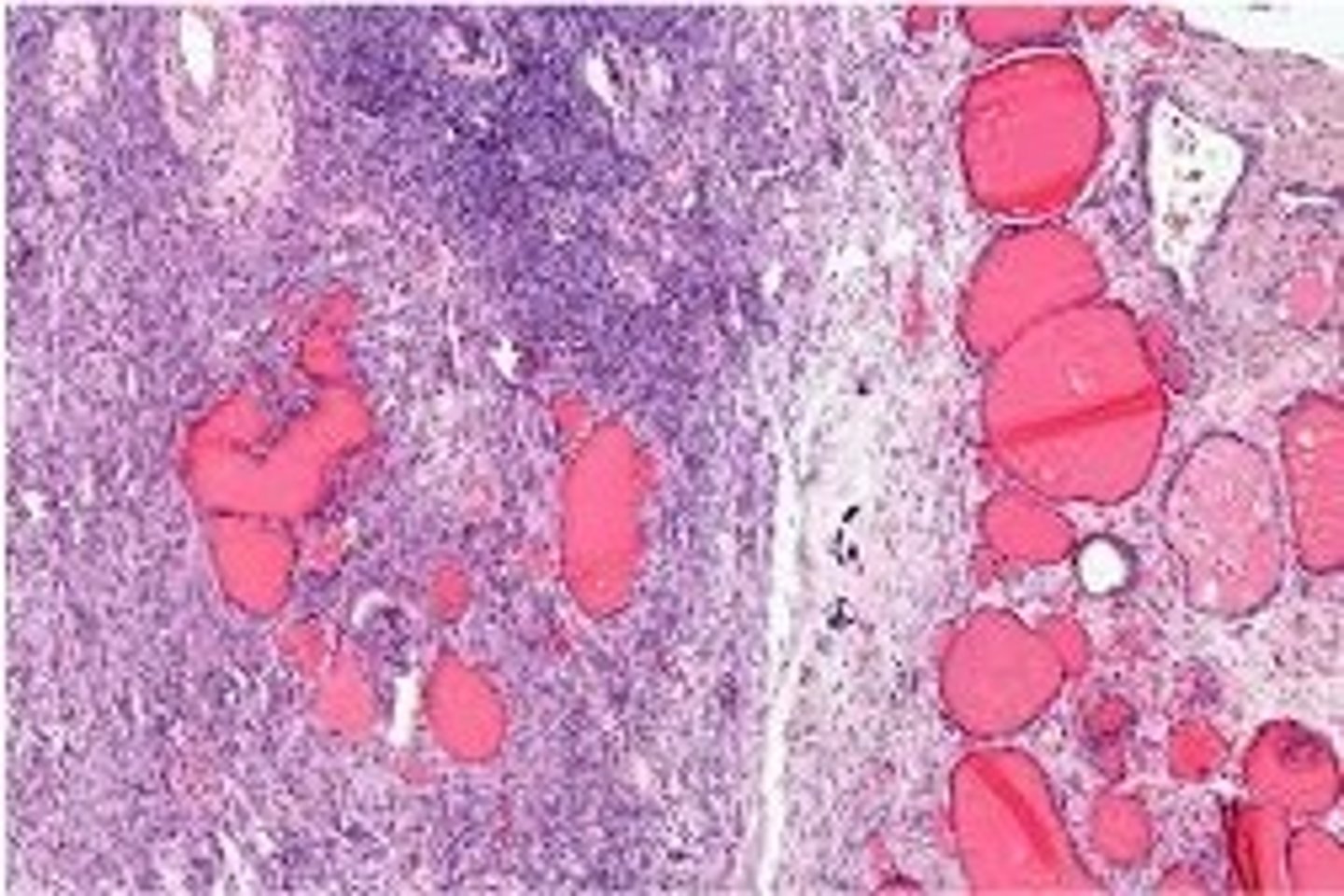
Struma Ovaril Teratoma
Define Type of Germ Cell Tumor:
Specialized Teratoma of mostly THYROID TISSUE (Monodermal)
-Hx: Young Women (10-30 y/o)
-Sx/PE: HYPOTHYROIDISM
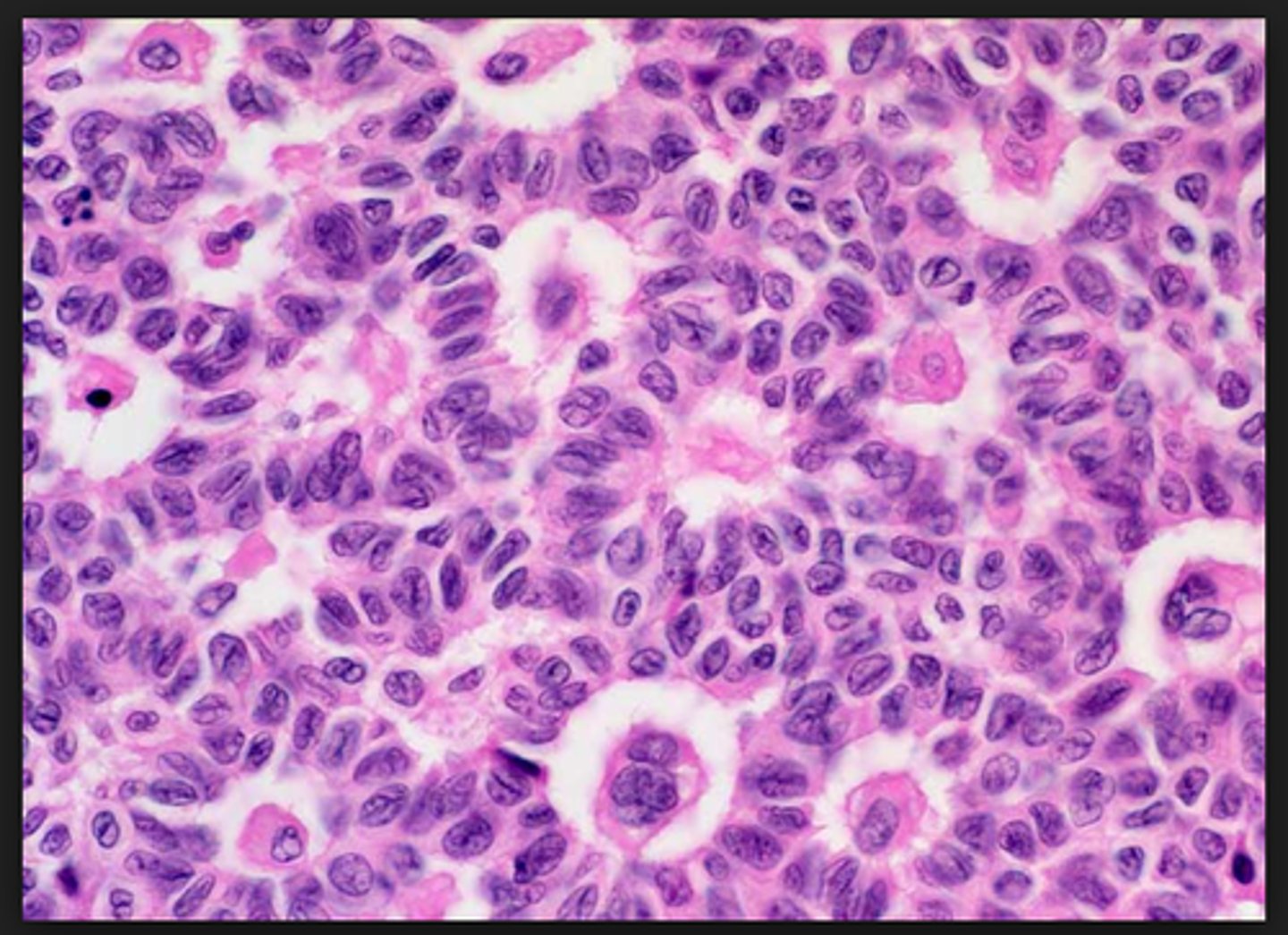
Immature Teratoma
Define Type of Germ Cell Tumor:
Solid mass of mostly neural tissue (immature fetal tissue)
-Hx: Young Women (< 20 y/o)
-Path: Has elements of all 3 germ layers
-Dx:
> Labs = AFP or Beta-hCG Markers
-Prog: Mets risk depends upon amt of immature neuroepithelium
Dysgerminoma
Define Type of Germ Cell Tumor:
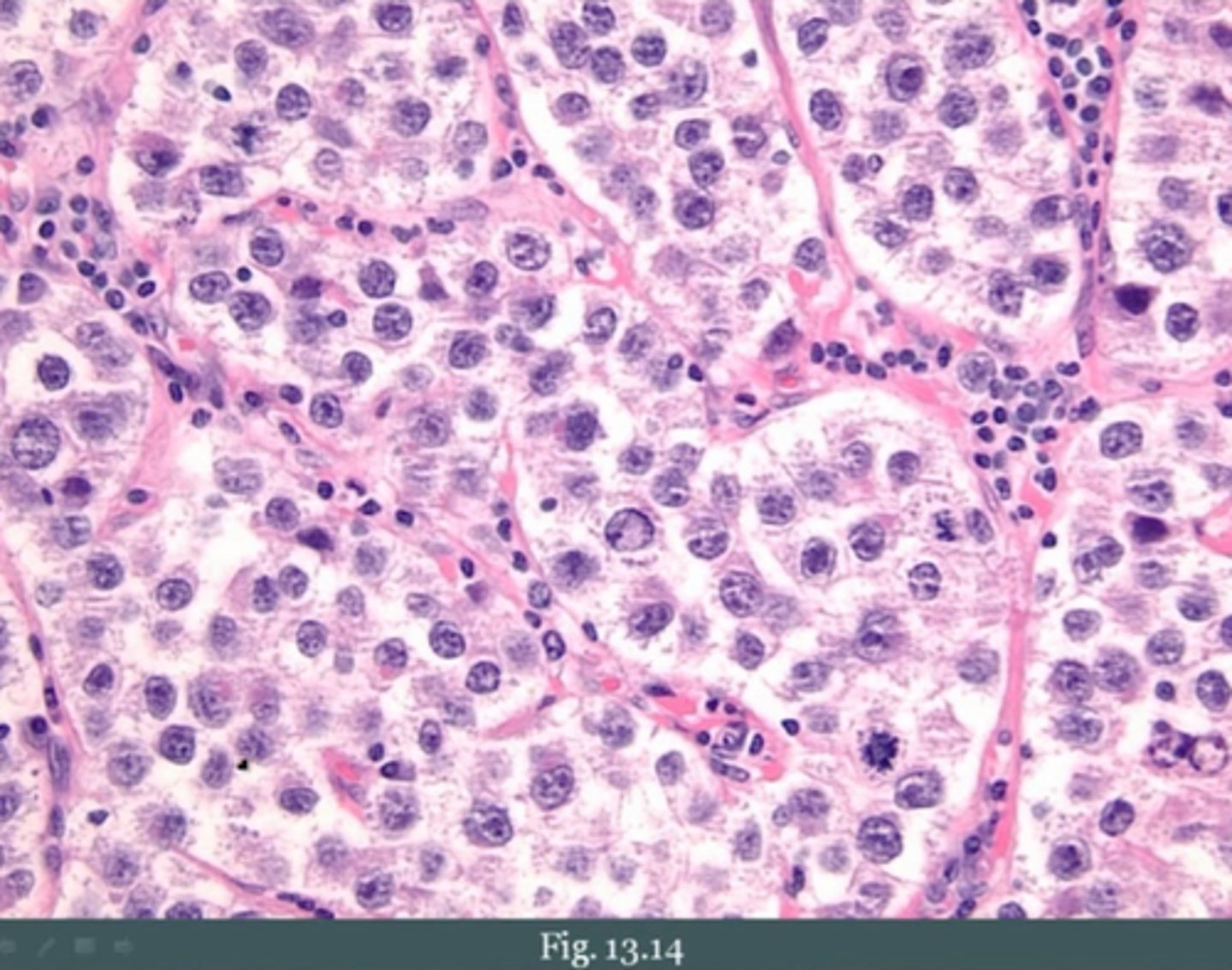
Most Common MALIGNANT Germ Cell Tumor - Ovarian counterpart to Seminoma in male testis
-Hx: Young Women (10-30 y/o)
-Sx/PE: Mostly UNILATERAL
-Dx:
> Labs = LDH or Beta-hCG or PLAP Markers
> Histo = Large cells with clear to pink cytoplasm and central nuclei (resemble oocytes, look like “fried eggs”)
-Prog:
> Only 1/3 spread
> Highly responsive to radiation and chemo
> GOOD PROGNOSIS (>80% 10 yr survival rate)
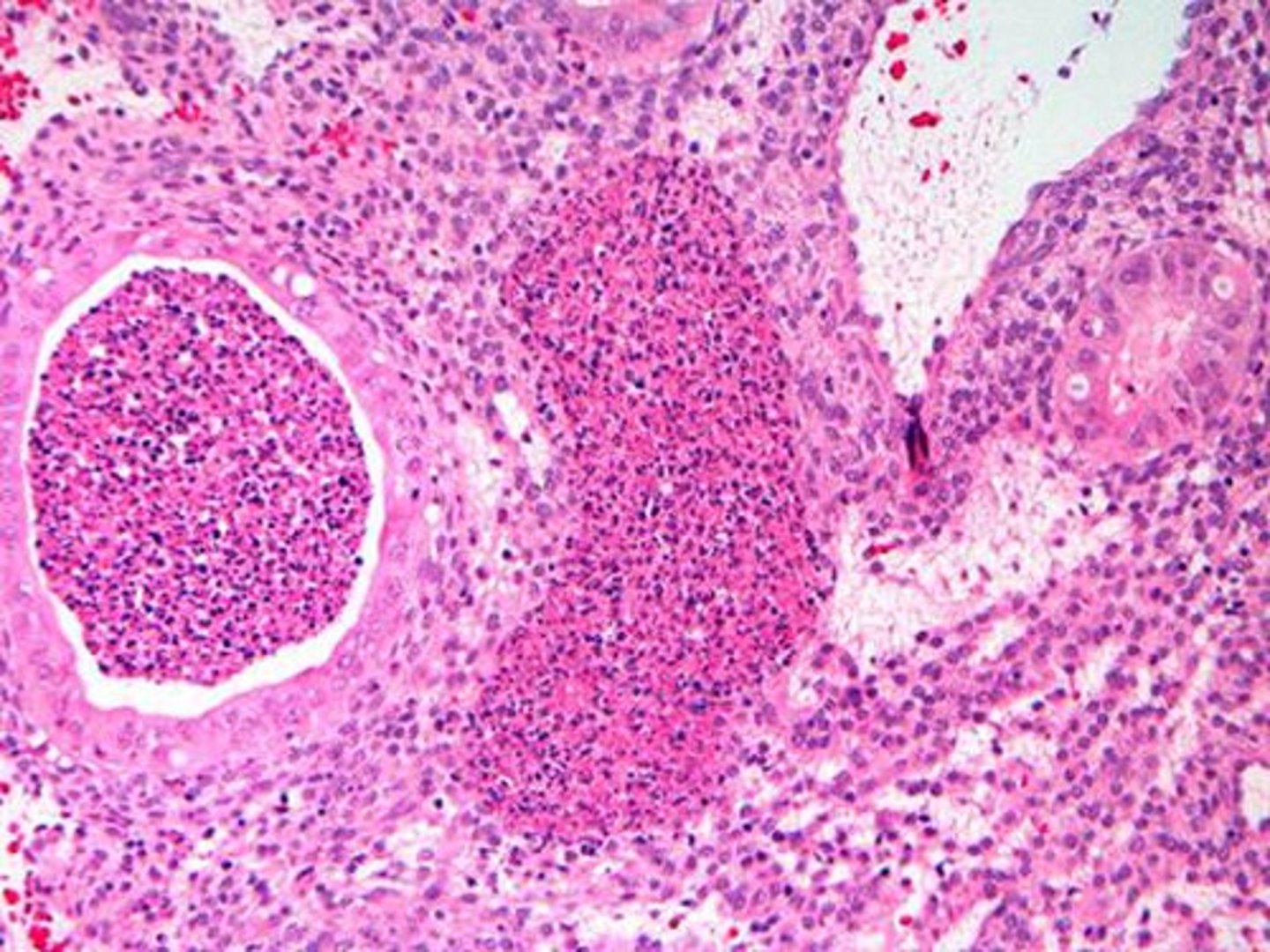
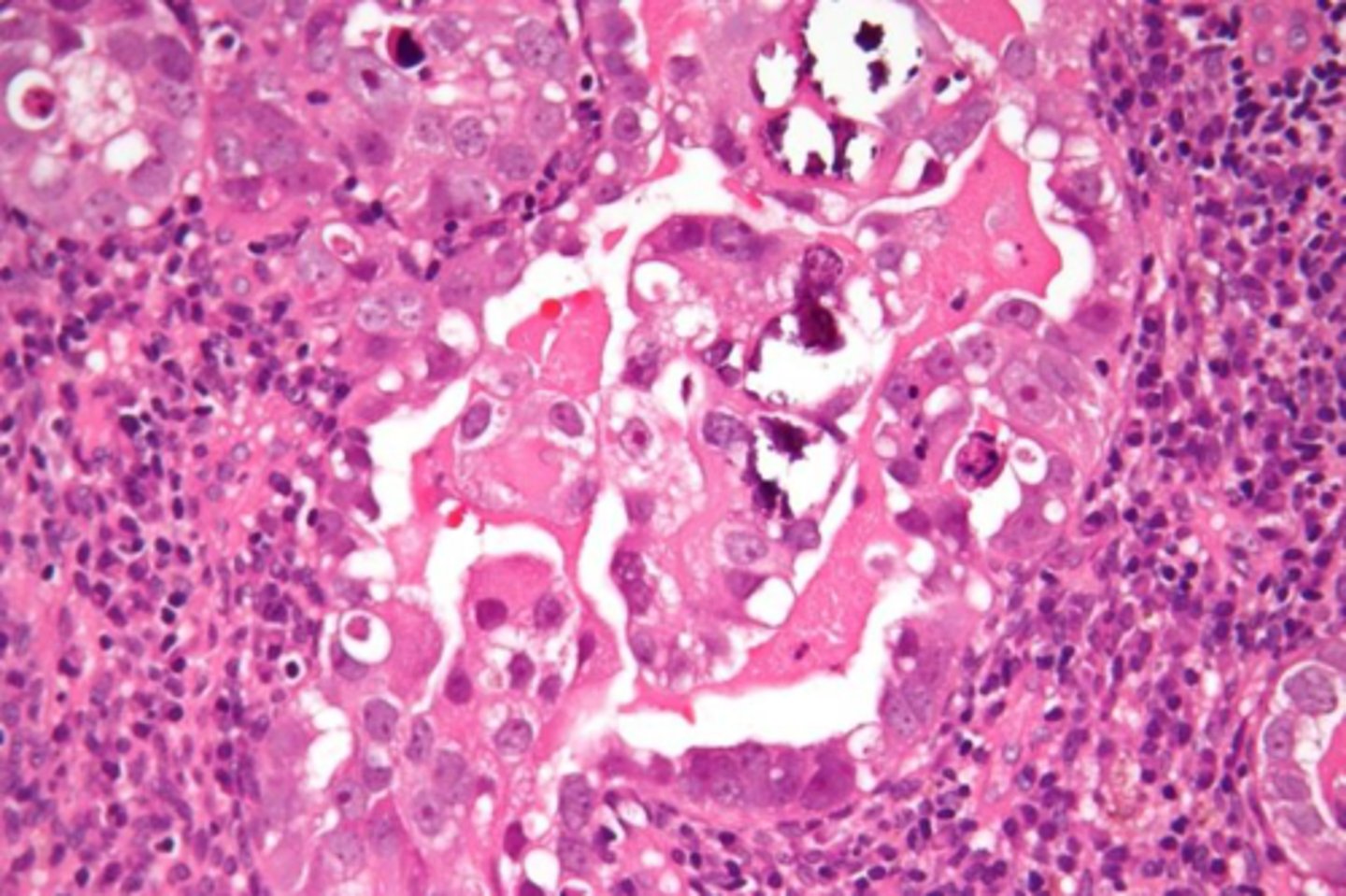
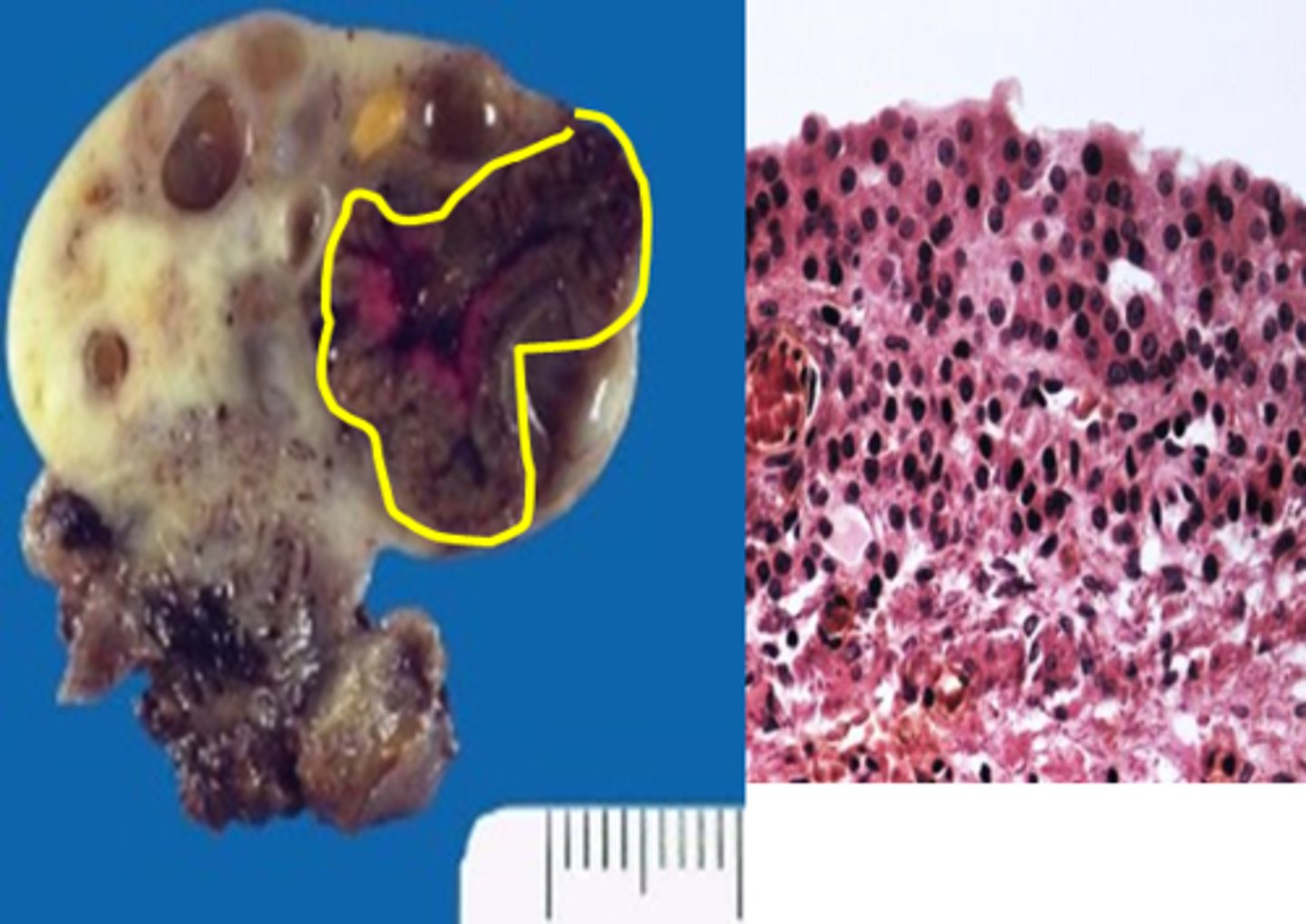
Yolk Sac Tumor (Endodermal Sinus Tumor)
Define Type of Germ Cell Tumor:
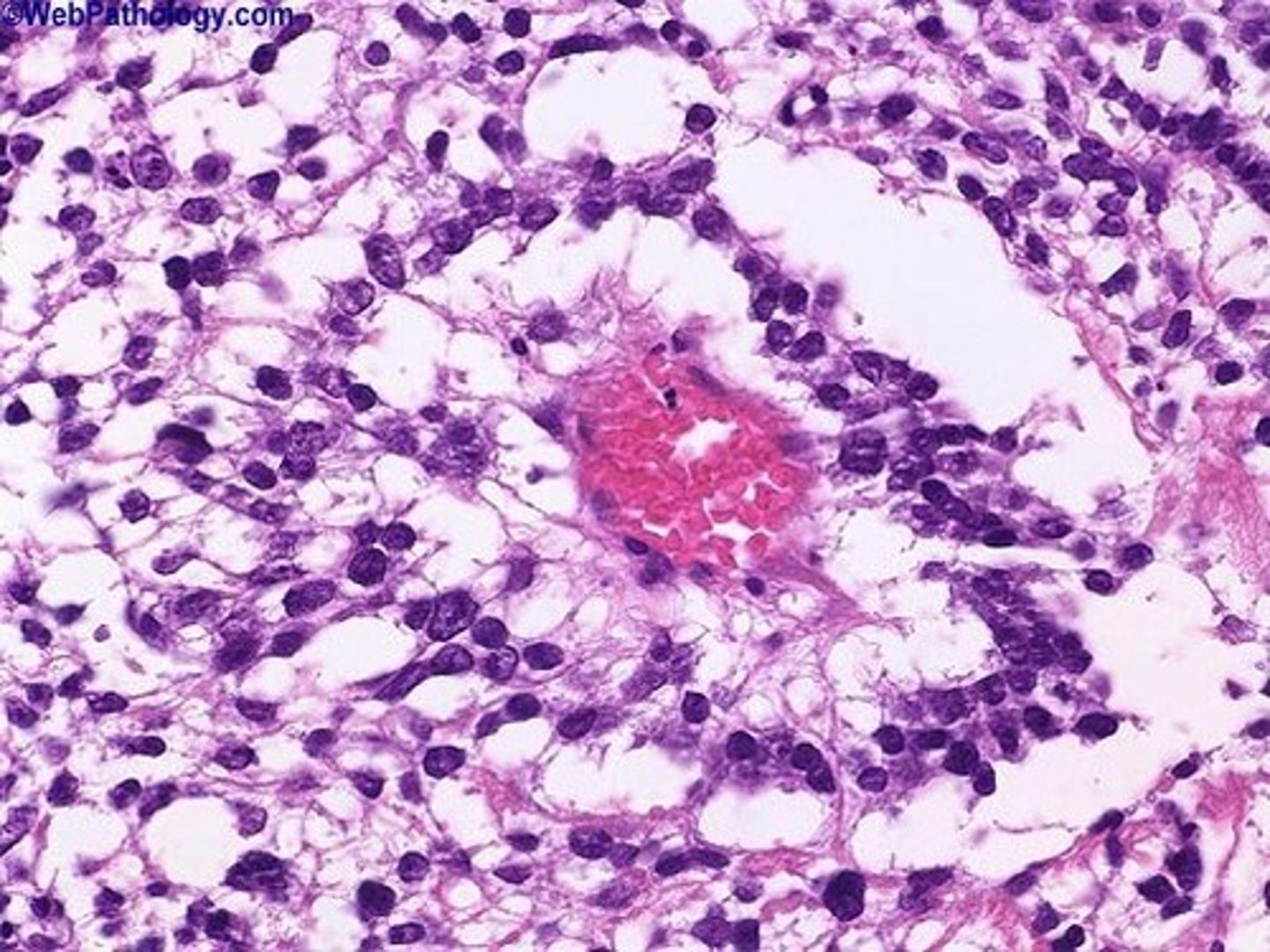
Rare, MALIGNANT, Tumor derived from extraembryonic yolk sac cells
-Hx: CHILDREN
-Dx:
> Labs = AFP Markers
> Gross = Yellow, Friable, Hemorrhagic mass
> Micro = 50% have Schiller-Duval bodies (vaguely “glomeruloid” perivascular structures) - single central vessel surrounded by several layers of tumor cells
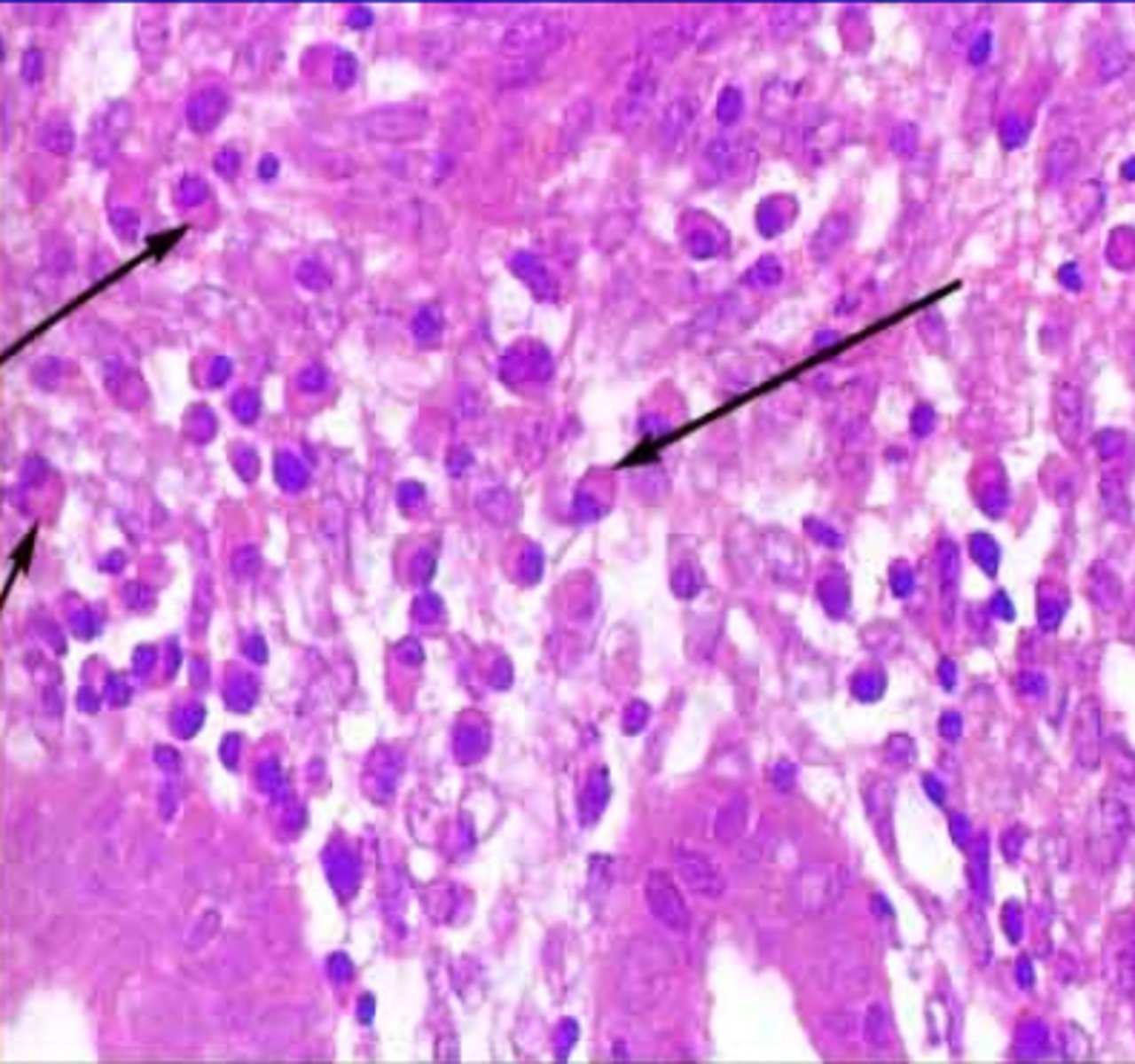
Choriocarcinoma
Define Type of Germ Cell Tumor:
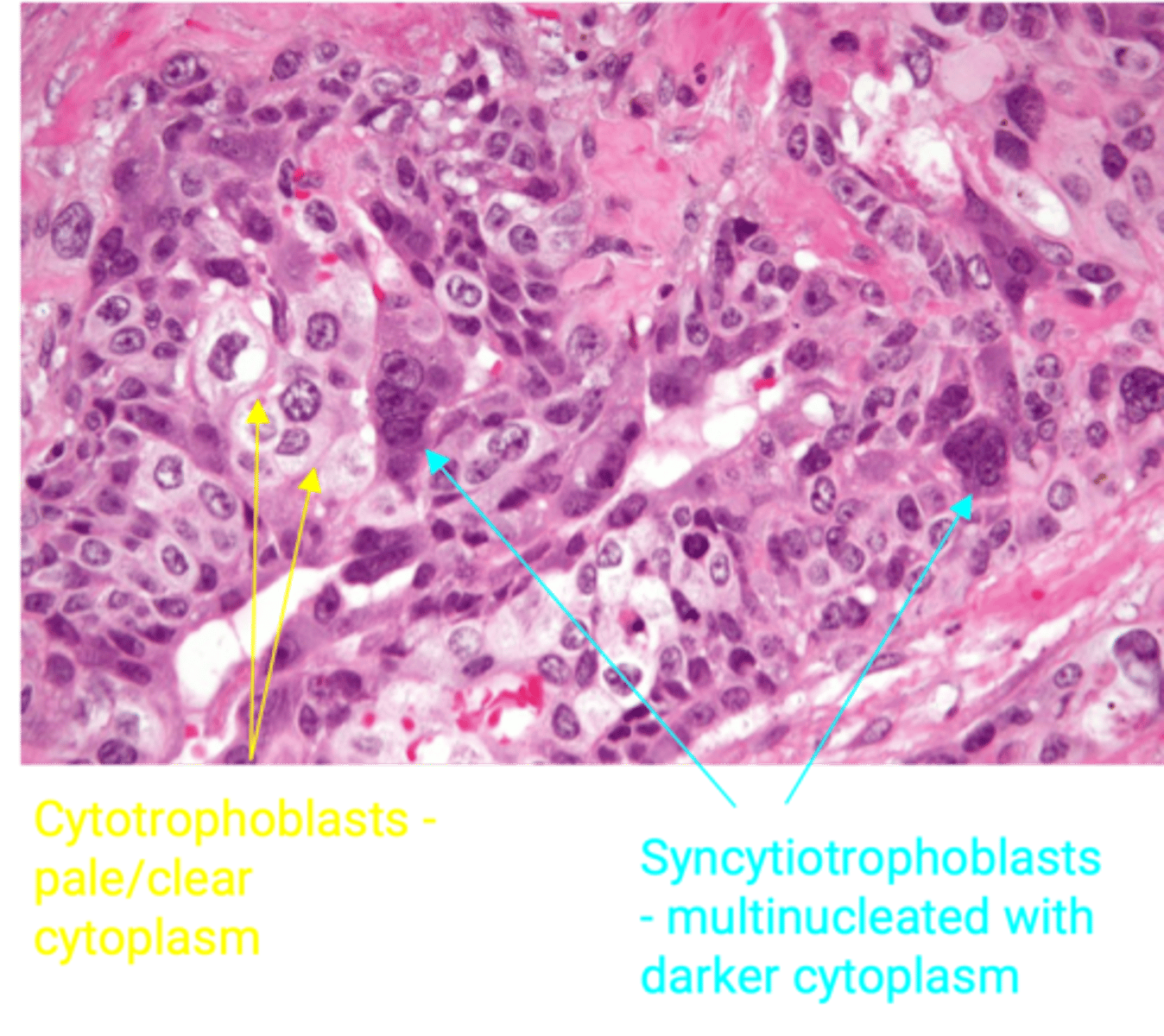
MALIGNANT tumor composed of 2 cell types: cytotrophoblasts and syncytiotrophoblasts
-Hx: Young Women (10-30 y/o)
-Path:
> Mimics placental tissue BUT villi are absent
> Small, hemorrhagic tumor with aggressive, early hematogenous spread
-Dx: Labs = Beta-hCG Markers
-Prog: Poor response to chemotherapy -> poor prognosis
Granulosa Cell Tumor
Define Type of Sex Cord Stromal Tumor:
Neoplastic proliferation of granulosa cells - MC Ovarian Sex Cord Stromal Tumor
-Hx + Types + Sx/PE:
> Adult (95%)
>> Postmenopausal bleeding
>> Endometrial Hyperplasia
>> Breast Tenderness (Estrogen)
> Juvenile (5%)
>> A/w Precocious Puberty
>> A/w endometrioid endometrial carcinoma
-Path: May contain THECA Cells --> Secretes ESTROGEN
-Dx:
> Labs = Increased INHIBIN
> Histo = Call-Exner bodies (Cells surrounding space filled with pink material resembling primitive follicles)
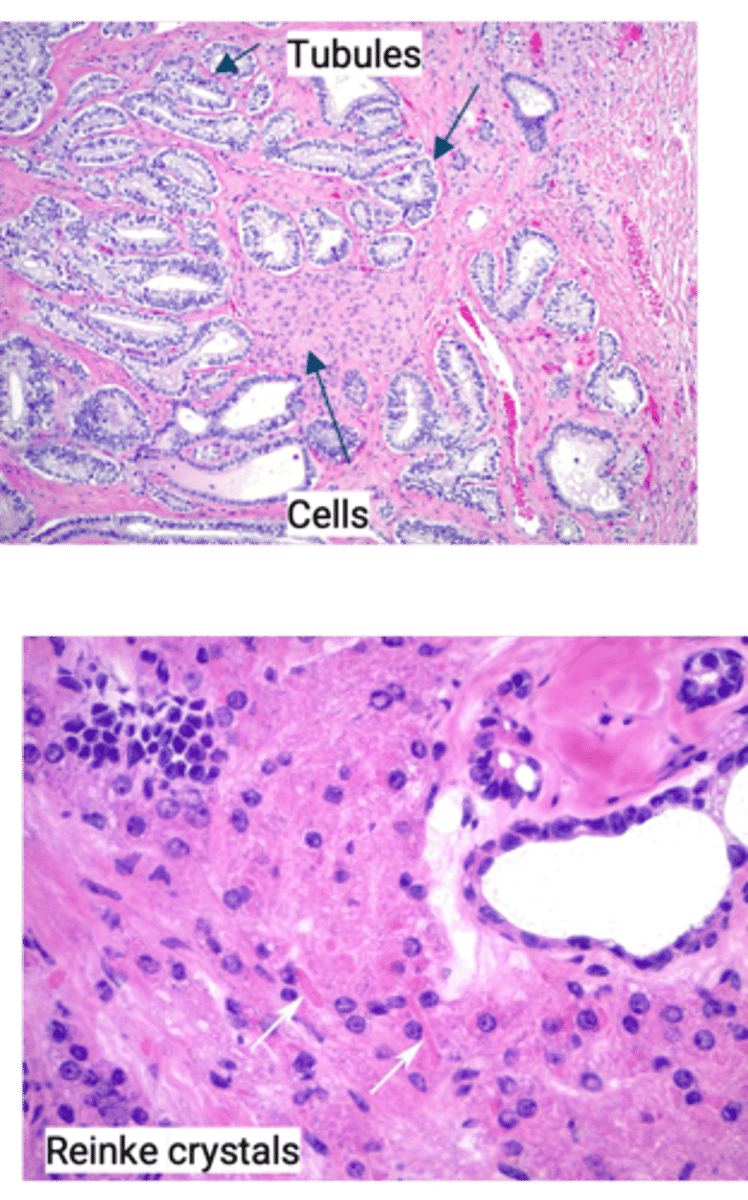
Sertoli-Leydig Cell Tumor
Define Type of Sex Cord Stromal Tumor:
-Types:
> Well-differentiated (Minimal Atypia) = BENIGN
> Poorly-differentiated (Marked Atypia) = MALIGNANT
-Path:
> Occur in males as testicular tumors, BUT can also occur in ovaries
> Produces ANDROGENS
-Sx/PE: Virilization in Females
> Hirsuitism
> Male Pattern Baldness
> Clitoral enlargement
-Dx:
> Histo = Composed of Sertoli cells that form tubules and Leydig cells (between tubules) with characteristic Reinke crystals (rod-like pink inclusions)
Fibroma
Define Type of Sex Cord Stromal Tumor:
Benign Tumor of Fibroblasts
-Hx: In POSTMENOPAUSAL WOMEN
-Path:
> Usually UNILATERAL
> No hormone activity
-Sx/PE:
> Pelvic/Adnexal Mass
> Meigs Syndrome = This + Ascites + Pleural Effusion
-Dx:
> Gross = Solid, White Tumor
-Tx: Remove Tumor & Resolve Syndrome

Thecoma
Define Type of Sex Cord Stromal Tumor:
Ovarian Stromal Neoplasm (usually benign) - made of cells resembling Theca Cells
-Hx: Postmenopausal Female
-Path: Produce Estrogen
-Sx/PE: Abnormal Bleeding
-Dx: Histo = Endometrial Hyperplasia
Metastatic Cancer from Ovaries
Define Condition:
MC Site of this in Gynecologic tract
-Hx/Path: Often from Colon & Breast
-Path/Dx: A/w Krukenburg Tumor (metastatic mucinous tumor that usually involves both ovaries)
> MC d/t metastatic gastric carcinoma (Diffuse = SIGNET RING CELLS)
> Also from metastatic breast/colon
> If BILATERAL = More Likely this (If Unilat = Primary Mucinous Carcinoma of Ovary)