Ocular Diagnostics Midterm Working Review
1/68
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
69 Terms
What is Heterophoria?
A misalignment of the visual axes in the absence of an adequate stimulus to fusion
What is Vergence?
Simultaneous movements of both eyes in opposite directions – goal is to maintain single binocular vision.
What is Von Graefe Phorias?
Subjective assessment of binocular deviations in the absence of fusion.
What is Vergence Ranges?
Subjective assessment of the eyes’ ability to perform fusional vergence movements.
What is Relative Accommodation?
Subjective assessment of the ability to decrease and increase accommodation while maintaining single vision.
What is Fused Cross Cylinder?
Subjective assessment of the accuracy of accommodation (non-presbyopes) and to find a tentative add (presbyopes).
Your Results are Distance 3 BI, what is its interpretation?
3 XP
Your results are Near 3 BU OS, what is its interpretation?
3 H’P OD
What kind of fusional vergence are you testing?
Base-in: Divergence
Base-out: Convergence
Base-down: SUPRAvergence
Base-up: INFRAvergence
What are the Direct and Indirect tests of each relative accommodation for NRA?
Direct: Relaxes accommodation
Indirect: Convergence
What are the Direct and Indirect tests of each relative accommodation for PRA?
Direct: Stimulates accommodation
Indirect: Divergence
How do you record this scenario?
Relative Accommodation: You started at +2.75 DS. The patient reports sustained blur at +0.25 DS. Record this test and findings.
PRA -2.50 D
Record this test and the findings for this scenario.
FCC: You start at the patient’s manifest refraction of +0.75 DS. The patient reports that the lines appear equal at PL DS.
-0.75 D (lead)
Record this finding in this scenario.
FCC: The patient’s manifest refraction is +0.75. You add 4 clicks of plus into the phoropter over the manifest. The patient reports that the lines appear equal at +0.50.
-0.25 D (lead)
Record this test and findings:
FCC: You start at the patient’s manifest refraction of +0.75 DS. The patient reports that the lines appear equal at +1.25 DS
+0.50 D (lag)
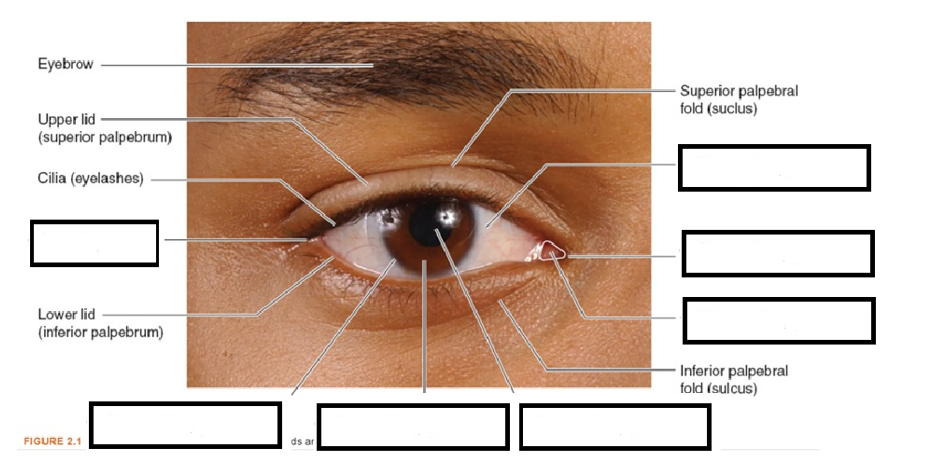
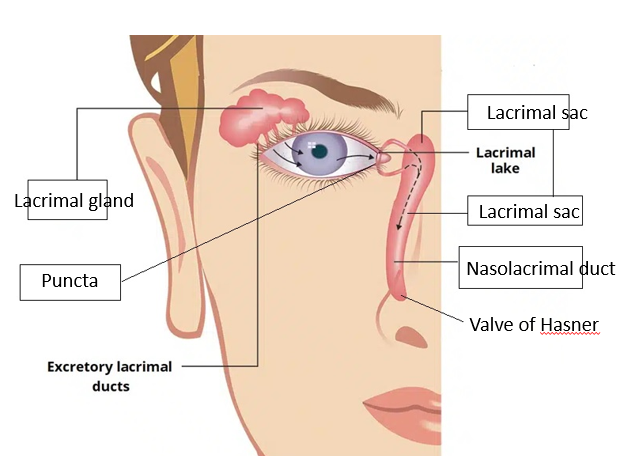
What are these parts?
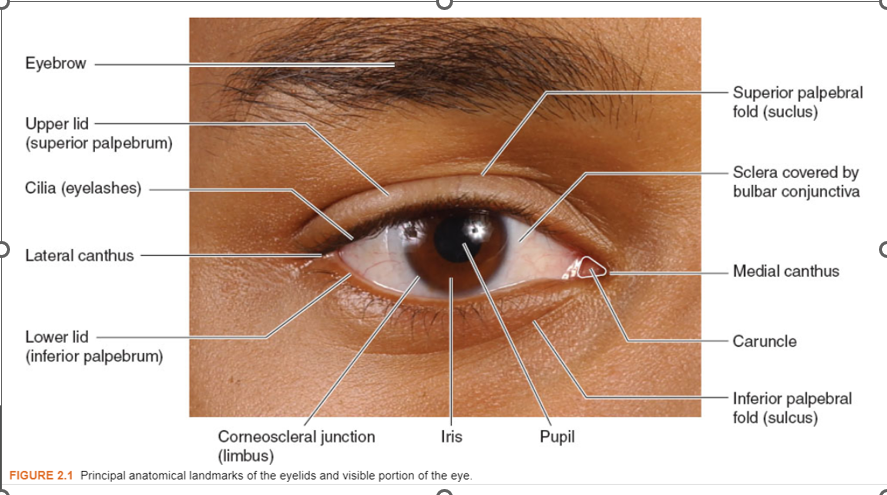
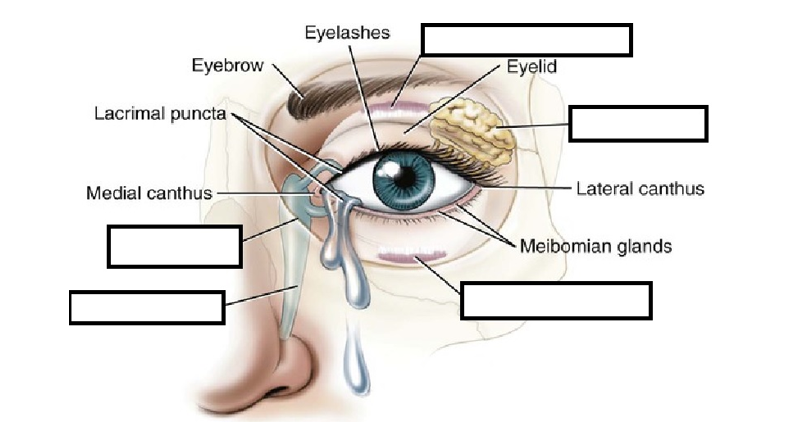
What are these parts?
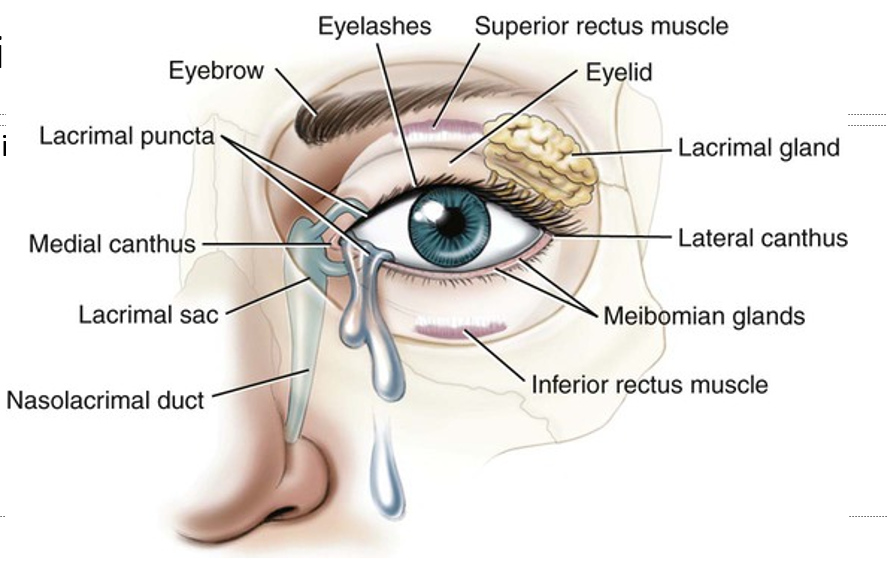
What are these parts?
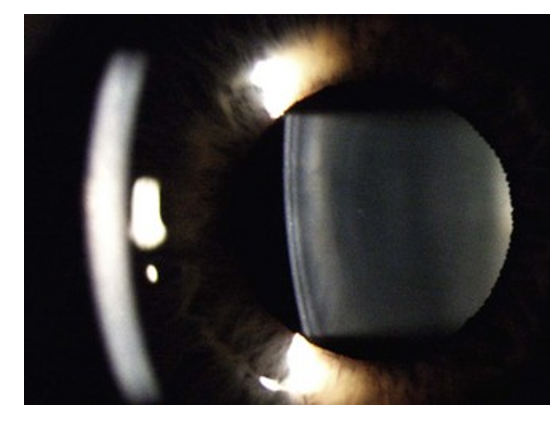
Identify lens, iris, and crystalline lens
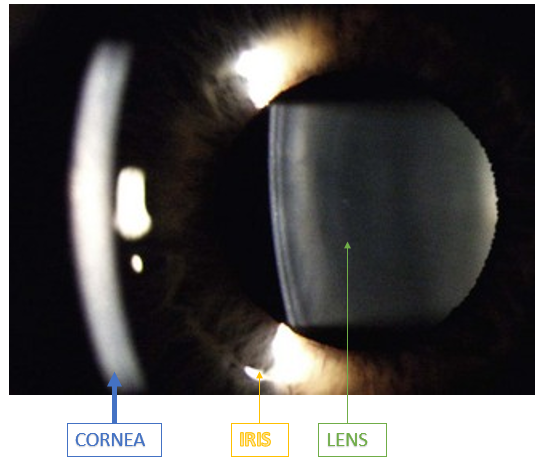
What are these parts?
How does the Zeiss Slit Lamp differ from a Haag Streit?
Illumination:
Zeiss comes from below
Haag Streit comes from above
How does the Greenough type slit lamp differ from the Galilean type?
Greenough has two mags, flipper level to change mag
Galilean has 3-5 steps on the side, (what we have)
What is the general application of direct diffuse illumination on slit lamp examination?
General gross scanning
An overview of various tissues
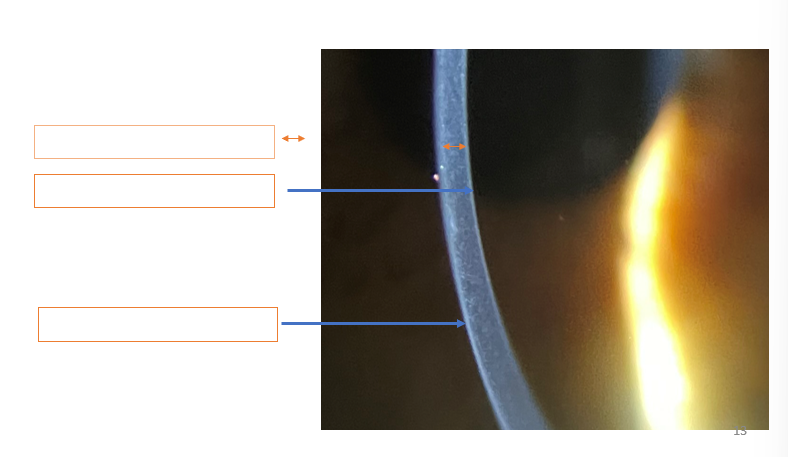
What is the appropriate beam and brightness (low/med/high)?
Van Herick
Optic section, High brightness
What is the appropriate beam and brightness (low/med/high)?
Corneal scan
Wide parallelepiped beam, Medium brightness
What is the appropriate beam and brightness (low/med/high)?
Corneal opacification
Optic section, Med-high brightness
What is the angle of the illumination arm for this tissue?
Lids
30 degrees
What is the angle of the illumination arm for this tissue?
Cornea
30-45 degrees
What is the angle of the illumination arm for this tissue?
Anterior chamber
30-45 degrees
What is the angle of the illumination arm for this tissue?
Transillumination of the iris
0 degrees
What is the angle of the illumination arm for this tissue?
Van Herick
60 degrees
What are the reasons for everting the upper lids?
Giant papillary conjunctivitis
Irritation and seasonal allergies
Removal of potentially lost contact lens
A foreign body location/removal
Evaluating the apex of internal or external hordelum
Evaluating the internal apex of chalazions
Determine the TENTATIVE add for this scenario:
Your new patient is 48 years old and has high hyperopia.
+1.75
Look at the chart from class/textbook
Determine the TENTATIVE add for this scenario:
You adjust your patient in the phoropter with the +1.00 D over their distance refraction and begin the FCC test.
With the first presentation, the patient reports that the lines are equal.
+1.00
Endpoint of FCC is the tentative add
Determine the TENTATIVE add for this scenario:
Using the push up method, you find that a patient can keep a target clear until it is 50 cm away (OD & OS). The patient prefers to work at 33.33 cm.
+2.00
Explanation: patient can use half of AA comfortably. AA=1/0.5m=2 D. AA/2=1.00 D. Patient’s preferred WD = 1/(0.3333 m)=3 D. Tentative add is what brings AA/2 up to the WD (with plus): 1.00 D+x=3 D,x=2 D
Determine the TENTATIVE add for this scenario:
After the distance refraction procedure, a patient’s near VA is 20/50 OU as measured with a traditional Snellen chart.
+1.00
Explanation: think Egger’s chart. 20/50 is 4 lines worse than 20/20, estimation is 0.25 D for each line of reduced VA. This is +1.00.
What is the REFINED add for this scenario?
A patient has the following results:
NRA = +2.50
PRA = -2.00
Tentative Add: +0.75
+1.00
Explanation: Refined Add=(NRA+PRA)/2+Tentative Add
=(+2.50+-2.00)/2+0.75=+1.00
Determine the REFINED add for this scenario?
A patient has the following results:
Tentative Add: +1.25, NVA 20/25 OU
You add another click of plus, and the patient reports clearer vision (NVA 20/20 OU).
You add another click of plus, and the patient reports clearer vision.
You add one more click of plus, and the patient reports no change.
1.75
Explanation: Leave the add at the least plus position that allowed maximum vision and was subjectively better to the patient.
What is the range of clear vision for this scenario?
The patient reports that their near vision is clear at 30 cm at the near extreme, and 45 cm at the far extreme. This is near extreme is not close enough for where the patient usually prefers to hold their reading material.
-What is the dioptric depth of field for this patient?
-What adjustment should you make to the refined add?
Dioptric depth of field is between 2.22 D and 3.33 D.
Adjust the add by adding +0.25 of plus to shift the range of clear vision closer to the patient.
Document normal for:
Adnexa
WNL or Normal OD, OS
Document normal for:
Lids
(-) crusting/flaking OD, OS
Document normal for:
Conjunctiva
(-) injection, (-) papillae, (-) follicles OD, OS
Document normal for:
Cornea
Clear OD, OS
Document normal for:
Anterior Chamber
Deep and quiet OD, OS
Document normal for:
Van Herick
OD 4×4, OS 4×4
Document normal for:
Iris
Brown, flat OD, OS
Document normal for:
Lens
Clear OD, OS

How do you describe this adnexa?
Asymmetric, Proptosis OS
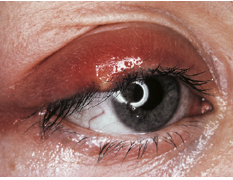
Describe these ABNORMAL findings (Assume OD)
(+) RUL lesion – tender upon touch OD
(+) RUL edema, hyperemia OD
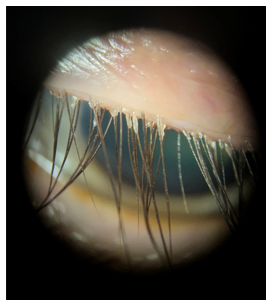
Describe these ABNORMAL findings (Assume OD)
(+) flaking RUL
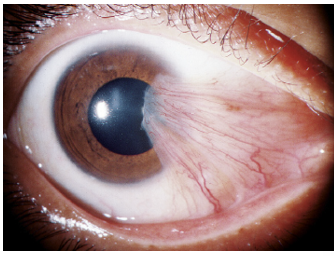
Describe these ABNORMAL findings (Assume OD)
(+) fleshy-elevated, triangular growth nasal encroaching onto cornea OD
What does NaFl stain?
Missing epithelial cells of the conjunctival and/or cornea
What does LG stain?
Dead or devitalized or epithelial cells of the conjunctival and/or cornea
What does RB stain?
Dead or devitalized epithelial cells of the conjunctival and/or cornea
What are the clinical applications of NaFl, any disadvantages?
Evaluation of ocular surface integrity
Goldmann applanation tonometry
Evaluation of the tear film (TBUT)
Evaluation of penetrating injury (Seidel’s sign)
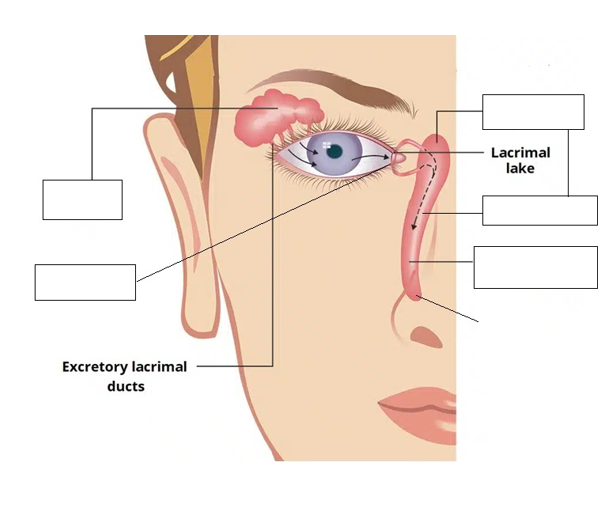
Evaluation for patency of the lacrimal system (Jones Test)
Gas permeable contact lens fitting evaluations
Fluorescein angiography
What are the clinical applications of LG, any disadvantages?
Evaluation of ocular surface integrity (bulbar conjunctiva) but can be used to evaluate the cornea too
Dry eyes, Herpes Keratitis
What are the clinical applications of RB, any disadvantages?
Evaluation of ocular surface integrity (bulbar conjunctiva) but can be used to evaluate the cornea too
Herpes keratitis, dry eyes
What is the best vital dye(s) for Tear Film Assessment?
Sodium fluorescein (NaFl)
What is the best vital dye(s) for Gas permeable fits?
Sodium fluorescein (NaFl)
What is the best vital dye(s) for Open globe?
Sodium fluorescein (NaFl)
What is the best vital dye(s) for Herpetic keratitis (dendritic)?
Lissamine green (LG)/Rose Bengal (RB) >> Sodium Fluorescein (NaFl)
What is the best vital dye(s) for Dry eyes?
Lissamine green (LG)/Rose Bengal (RB) >> Sodium Fluorescein (NaFl)
What is the light source/filter for NaFl?
Cobalt filter with Wratten filter
What is the light source/filter for LG?
White light
What is the light source/filter for RB?
White light
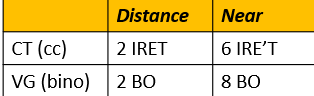
What is your Assessment and Plan for this?
Esotropia OD, Ed pt on condition. Refer to BV specialist.
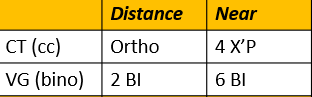
What is your Assessment and Plan for this?
Exophoria, Ed pt on condition and associated symptoms. Monitor 12 months or sooner if symptomatic
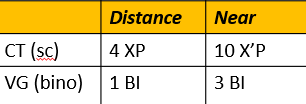
What is your Assessment and Plan for this?
Exophoria, Ed pt on condition and associated symptoms. Monitor 12 months or sooner if symptomatic

What is your Assessment and Plan for this?
Esophoria, Ed pt on condition and associated symptoms. Monitor 12 months or sooner if symptomatic