Unit 2 Lesson 3 Echo Findings and Mimickers
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
List the 6 main 2D echo findings/assessment areas for HCM.
LV size and function
LV hypertrophy in varying patterns
Apical, neutral, basal septal, and reverse curvature patterns
Characterization of mitral valve morphology and subvalvular structures
LV diastolic function
Assessment for LV outflow obstruction at rest and with provocation
Simple reminder:
For HCM echo, think: LV size/function, hypertrophy pattern, mitral valve/subvalvular anatomy, diastolic function, and LVOT obstruction.
Describe LV size and systolic function in HCM.
The LV is usually small to normal in size with normal to hyperdynamic LV systolic function.
What happens to EF in end-stage hypertrophic cardiomyopathy? how is it characterized by?
what EF % tells us there is poor prognosis?
End-stage HCM is characterized by reduced EF.
< 50% poor prognosis
Explain ASH and the septal/posterior wall ratio associated with HCM.
ASH means asymmetric septal hypertrophy. A septal-to-posterior wall ratio >1.3 cm is associated with HCM.
What septal thickness is associated with a 40% cumulative risk for sudden death?
Septal thickness >3.0 cm holds a 40% cumulative risk for sudden death.
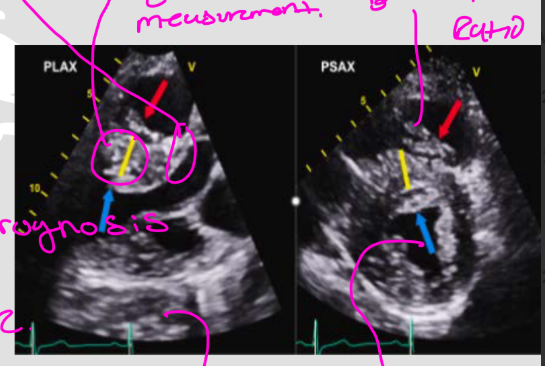
How should wall thickness be measured in HCM?
Wall thickness should be measured in multiple views. PLAX & PSAX
you take the septal wall and posterior wall and divide it to find the ratio to see is if it is associated with HCM
High-yield numbers:
Septal/posterior wall ratio: >1.3 cm
Septal thickness sudden death risk: >3.0 cm
Risk listed: 40% cumulative risk
yellow line is accurate measurement
List the 5 mitral valve/subvalvular findings associated with HCM.
Anterior and posterior mitral valve leaflets are typically elongated
Anterior leaflet may have a redundant distal segment
SAM
Papillary muscle abnormalities
Myocardial crypts
(anything that obstructes the LVOT cavity / LVOT, when they know they have HCM from gentic testing can see a young Pt MV strcustures becore thickening of the septem starts)
Anterior leaflet may have a redundant distal segment” means the front mitral valve leaflet can have extra/loose tissue near its tip.
Breakdown:
Anterior leaflet = the front leaflet of the mitral valve
Redundant = extra, floppy, or too much tissue
Distal segment = the far end/tip of the leaflet
So simple meaning:
The tip of the anterior mitral valve leaflet may be longer/floppier than normal.
Why this matters in HCM/HOCM:
If the anterior mitral leaflet has extra floppy tissue, it can get pulled or pushed into the LVOT during systole. This can contribute to SAM and worsen LVOT obstruction.
List the 2 papillary muscle/chordal abnormalities associated with HCM.
Anteriorly/apically displaced papillary muscles
Anomalous chordal attachments
(closer to the apex then where they are normally)
Simple reminder:
HCM is not only about a thick septum. The mitral valve leaflets, papillary muscles, chordae, and myocardial crypts can also be involved.
If the chordae attach abnormally, they can pull the mitral valve leaflet in a weird direction. This can make the mitral valve move toward the LVOT during systole and contribute to SAM and LVOT obstruction.
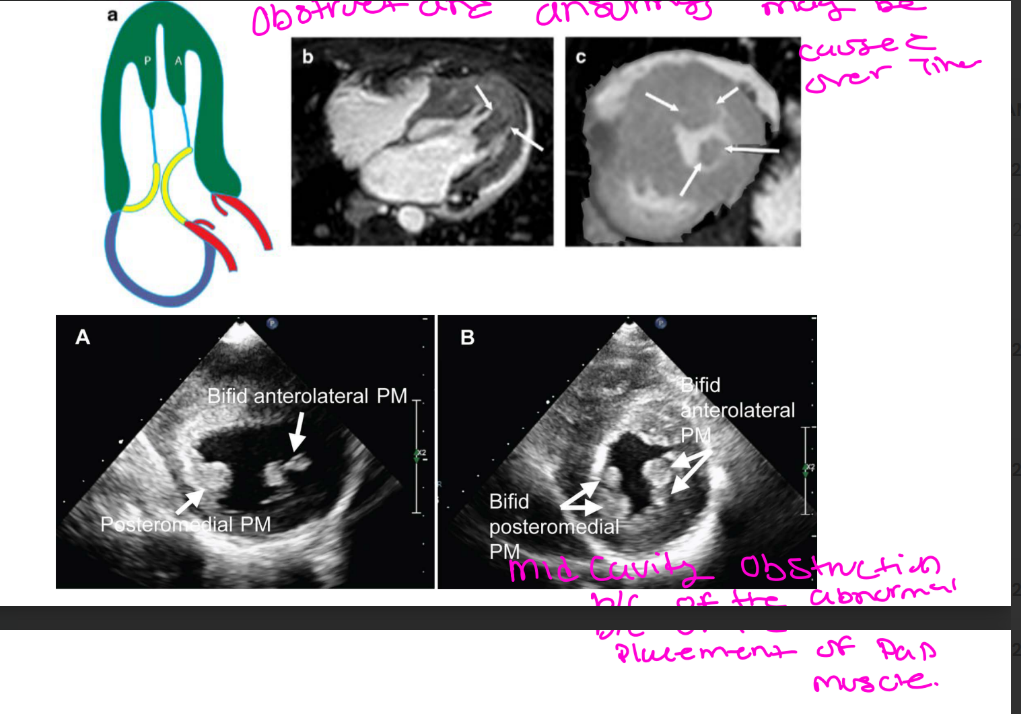
List the 3 papillary muscle findings associated with HCM.
Hypertrophied papillary muscles
Apically/anteriorly displaced papillary muscles
Bifid papillary muscles
Simple reminder:
Papillary muscle abnormalities can contribute to abnormal mitral valve motion and obstruction.
A bifid papillary muscle is a papillary muscle that has a divided or double-headed appearance.
What can SAM cause on the interventricular septum?
SAM can cause an endocardial plaque on the interventricular septum, or IVS.
(2D might see hyperechoic area / mcrio injury to the septum)
Simple reminder:
Repeated mitral valve contact with the septum can create a plaque area on the IVS.
List the 5 M-mode findings of HCM/HOCM.
ASH
SAM
Mid-systolic notching of the aortic valve
Small LV cavity dimension
B-bump
Simple reminder:
M-mode findings to remember: ASH, SAM, AV mid-systolic notching, small LV cavity, and B-bump.
List the 6 Doppler findings/assessment areas in HCM/HOCM.
Diastolic dysfunction
LA volume
LVOT obstruction
Mid-ventricular obstruction
Apical “lobster claw”
Mitral regurgitation
Explain diastolic dysfunction in HCM.
What appears before what develops, especially …..in some patients with what mutations?
diastolic dysfunction present in HCM patients regardless of what pattern?
Impaired relaxation can appear before LV hypertrophy develops, especially in some patients with gene mutations.
Diastolic dysfunction is present in HCM patients regardless of hypertrophy pattern.
If a patient with HCM is symptomatic but does not have obstruction, what is the likely cause?
Diastolic dysfunction is likely the cause.
Simple reminder:
HCM symptoms are not always from obstruction. They can also come from the stiff LV not relaxing/filling well.
Why does LA dysfunction occur in HCM? Name 3
LA dysfunction occurs because of impaired LV relaxation and increased myocyte and chamber stiffness.
List the 3 other causes of LA remodeling in HCM.
For the 3rd… LV remodeling leading to what name 2, results in what?
Prolonged exposure to MR
LVOTO
LV remodeling leading to high ventricular filling pressures and diastolic dysfunction, which increases LA afterload
Simple reminder:
The LA is affected because the stiff LV raises filling pressures, and MR/LVOTO can add more stress to the LA.
List the 4 long-term effects of LA dysfunction/remodeling in HCM.
LA dilatation
Functional deterioration
Atrial fibrillation
Increased risk for stroke
High-yield reminder:
LA remodeling can lead to AFib, and AFib increases stroke risk.
How can color flow Doppler help assess LVOT obstruction?
Color flow Doppler can help define the location of obstruction.
What color Doppler finding suggests LVOT obstruction?
Turbulent flow with aliasing.
Simple reminder:
Color Doppler helps locate the obstruction by showing turbulence/aliasing.
What can happen to the LVOT gradient after a PVC?
An increased gradient may be noted after a post-ectopic beat.
List the an events that happen after a PVC.
And list 3 events that the next beat has
Compensatory pause
The next beat has…..
Longer filling time
Increase in preload
Stronger contraction (increase gradient)
Simple reminder:
After a PVC, the next beat fills more and contracts harder, which can increase the gradient.
How is the degree of LVOT obstruction assessed - what doppler?
The degree of obstruction may be assessed with CW Doppler.
Describe the CW Doppler envelope pattern in LVOT obstruction.*******
How does the outflow velocities increase - and during what cardiac cycle, then what happens abrupty and what cardiac cycle?
results in what envelop?
Outflow velocities increase slowly in early systole, then rise abruptly and peak in mid-to-late systole, creating a dagger-shaped envelope.
Simple reminder:
HOCM LVOT obstruction has a late-peaking dagger-shaped CW Doppler profile.
What formula can be used to estimate LVOT gradient from the MR signal?
&
What alternate relationship can be used?
LVOT peak gradient = 4(MR peak velocity)² + LAP − SBP
&
MR gradient + LAP = SBP + LVOT gradient
What LAP value should be assumed?
Assume LAP = 10 mmHg.
Simple reminder:
You can use the MR signal to help estimate LVOT gradient if you know MR velocity/gradient, LAP, and SBP.
Calculate the expected LVOT gradient if the MR gradient is 211.92 mmHg, MR peak 7.28m/s, BP is 126/58, and LAP is assumed to be 10 mmHg.
MR gradient + LAP = SBP + LVOT gradient
So:
211.92 + 10 = 126 + LVOT gradient
221.92 = 126 + LVOT gradient
LVOT gradient = 95.92 mmHg
For a LVOT pe ak gradient = 4(MR pe ak gradient velocity)⇢ + LAP – SBP
4(7.28m/s)2 + 10 -126 = 96 mmHg
Final Answer:
The expected LVOT gradient is approximately 96 mmHg.
Simple reminder:
Use systolic BP, not diastolic BP, in this calculation.
Explain mid-ventricular obstruction in HCM.
Occurs in a ____ of HCM patients
what is found mid-cavitary level and unrelated to what?
Mid-ventricular obstruction occurs in a minority of HCM patients. The impedance of flow is found at the mid-cavitary level and is unrelated to SAM.
“Impedance of flow” means something is slowing down or blocking the blood from moving forward smoothly.
In this slide, it is talking about mid-ventricular obstruction. That means the blockage/resistance is happening in the middle of the left ventricle cavity, not at the LVOT.
So this sentence means:
The blood flow is being blocked in the middle of the LV, and this blockage is not caused by SAM.
A minority is a group of people that is smaller than the main population and differs in some way, such as race, culture, or religion
List the 3 causes of mid-ventricular obstruction.
Septal hypertrophy
Hyperdynamic LV wall (EF of greater then 72-74%)
Hypertrophied papillary muscle
Simple reminder:
Mid-ventricular obstruction happens in the middle of the LV cavity, not the LVOT, and it is not caused by SAM.
Explain the “lobster claw” pattern in apical HCM with mid-cavitary obstruction.
the emptying profile has an initial what of the pouch in what cardiac cycle? follwed by what signal in what cardiac cycle and why does this happen? then follwed by a second what in what cardiac cycle from what?
Mid cavitary obstruction: The emptying profile has an initial rapid emptying of the pouch in early systole, followed by a signal void in mid-to-late systole because flow stops/ cessation of flow as the neck narrows during contraction obstructing flow. Then follwed by a second outflow in diastole from incompletely emptied pouch.
(Diastolic emptying of Apical Aneurysm) ( Blue berry on top)
The “second outflow in diastole” means the apical pouch did not fully empty during systole, so some blood is still trapped/left over in that pouch. Then, when the heart relaxes in diastole, that leftover blood moves out again.
the third signal is basically showing the leftover blood trying to empty after the obstruction relaxes. The slide describes this as an initial rapid emptying, then cessation of flow when the neck narrows, then a second outflow in diastole from the incompletely emptied pouch.
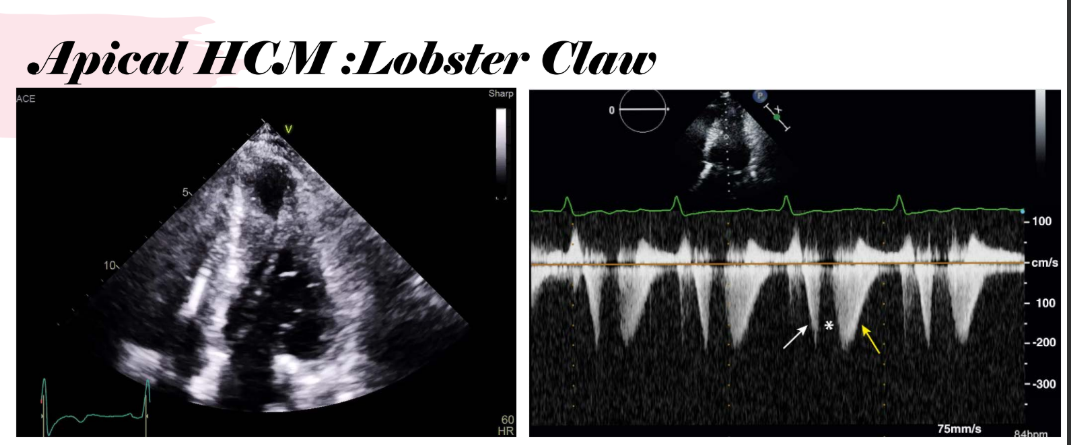
List the 3 parts of the lobster claw flow pattern.
Initial rapid emptying of the pouch in early systole
Signal void in mid-to-late systole due to cessation of flow
Second outflow in diastole from the incompletely emptied pouch
Simple reminder:
Lobster claw = early systolic emptying, mid/late systolic flow stop, then diastolic emptying.
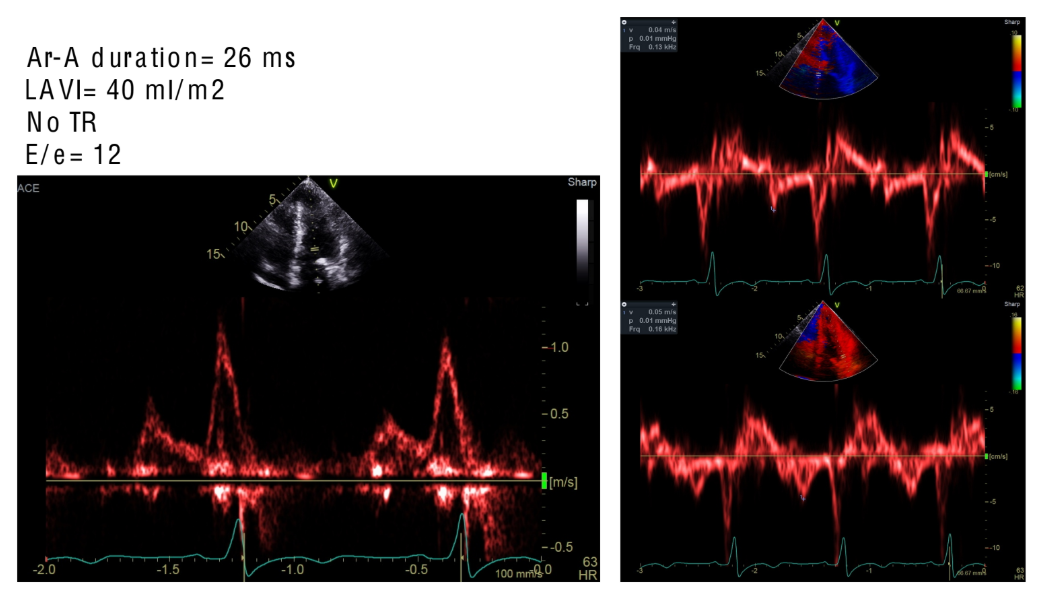
Grade the diastology you see here
Grade 1 diastolic dysfunction
signal identification. and tell me the cardiac cycle
MR (Holoystolic IVCT & IVRT)
MID (late systole)
LVOT (mid - late systole)
HCM Phenocopies / differentials:
How can pressure overload conditions mimic HCM? - _____ exposure to what induces a ……..response in the …..
Chronic exposure to high LV pressures can induce a hypertrophic response in the myocardium.
List the 3 pressure overload conditions that can mimic HCM.
Uncontrolled hypertension
Coarctation of the aorta
Obstruction to LV outflow at the subvalvular, valvular, or supravalvular level
Simple reminder:
Pressure overload can cause LVH, so it can look like HCM unless you identify the cause.
Why can athlete’s heart mimic HCM? list two similars
Athlete’s heart can cause LV hypertrophy, and LV wall thickness >13 mm can be seen in both trained athletes and HCM.
about ____ of althletes may have an _______ in LV what?
About 1/3 of athletes may have an increased LV cavity dimension.
what can help differentiate HCM from athlete’s heart? and how do we know if its true althetes heart
The athlete may need to decondition to see whether the LVH subsides. if LVH subside with deconditioning it’s althletes heart if not its HCM (should get gentic testing)
High-yield numbers:
Wall thickness overlap: >13 mm
Increased LV cavity dimension: 1/3 of athletes
List the 4 echo findings that help favor HCM over athlete’s heart.
ASH or abnormal hypertrophy patterns vs concentric hypertrophy in althlete’s heart
Small LV cavity size
LA enlargement
Diastolic dysfunction, grade 1 or greater
(Althletes heart will have enhance diastology, better diastolic function)
List the 3 other findings/tests that help support HCM over athlete’s heart.
Family history of HCM (genetic testing)
Abnormal EKG pattern
Poor VO₂ capacity
Simple reminder:
Athlete’s heart is more likely concentric and physiologic. HCM is more suspicious when there is abnormal hypertrophy pattern, small LV cavity, LA enlargement, diastolic dysfunction, family history, abnormal EKG, or poor VO₂.
Poor VO₂ capacity means the person has a low ability to use oxygen during exercise.
VO₂ = how much oxygen your body can take in and use when you are active.
So poor VO₂ capacity means:
When the patient exercises, their body/heart cannot keep up well, so their exercise ability is lower than expected.
In your slide, this is used to help tell the difference between athlete’s heart vs HCM. An athlete’s heart usually has good exercise capacity, but someone with HCM may have poor VO₂ capacity because the thick/stiff heart does not fill or pump efficiently during exercise.
List the 2 genetic phenocopies of HCM.
Fabry disease
Danon disease
Explain Fabry disease as an HCM phenocopy.
Fabry disease is an what rescessive disorder, typically manifests in what gender in what decade of life?
what history of disease does this phencopie have?
what type of cardiomyopathy is this phencopie and what disease with what buildup throughout where name two?
name 2 area that Fabry diease affects the heart
Fabry disease is an X-linked recessive disorder that typically manifests in men in the 3rd or 4th decade of life.
History of renal disease / transplant
It is a restrictive cardiomyopathy and storage disease caused by glycolipid buildup throughout the body and in the LV myocardium.
Fibrosis of LV myocardium and valves
List the 7 characteristics of Fabry disease.
How are the PR intervals ?
Presents like any ______ of HCM- no significant differences in what name 4
typically, has what walls and LV hypertrophy
name another structure in the heart that hypertrophy
what’s worse
*****LV strain pattern: typically…….*****
______ myocardium
Short PR interval
Can present like any HCM phenotype
No significant differences in LVH, EF, LAVI, or GLS
Typically concentric LVH
Papillary hypertrophy
Worse LA strain
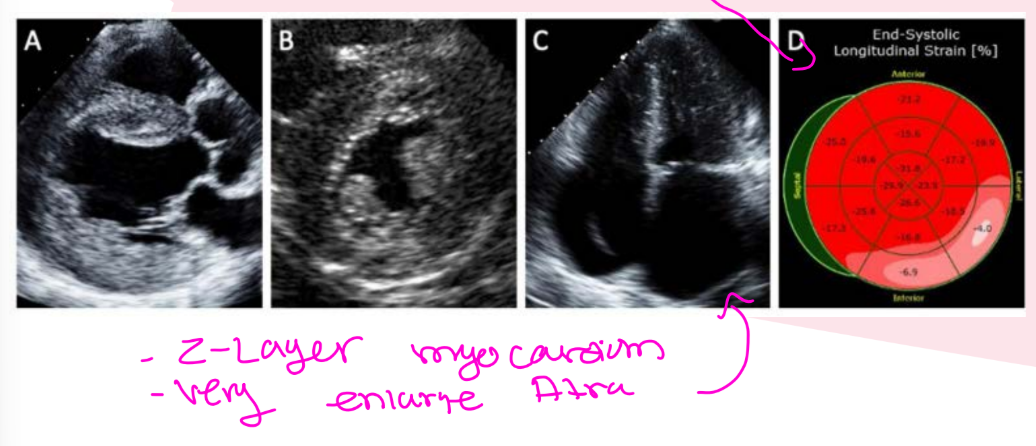
****LV strain pattern usually worse in the basal inferolateral wall**** (and the rest of the walls are normal so you know its Fabry DIsease)
Binary myocardium
Binary myocardium means the heart muscle looks like it has two different layers/textures on echo.
In Fabry disease, the myocardium can sometimes look like:
1. A bright inner layer near the endocardium
and
2. A darker outer layer of myocardium
That “two-layer look” is why they call it binary myocardium
“Presents like any HCM phenotype” means Fabry disease can look like regular HCM on echo.
A phenotype means the pattern/appearance of the disease.
So the slide is saying:
Fabry disease can show up with the same types of heart-thickening patterns that HCM can show.
For example, it may look like:
septal hypertrophy
concentric LVH
papillary muscle hypertrophy
abnormal strain patterns
That is why it is called an HCM phenocopy — it copies/mimics the appearance of HCM, even though the cause is different.
The next part, “no significant differences in LVH, EF, LAVI, GLS,” means the echo measurements may not clearly separate Fabry from regular HCM:
LVH = left ventricular hypertrophy/thick heart muscle
EF = ejection fraction/pumping function
LAVI = left atrial volume index
GLS = global longitudinal strain
Explain Danon disease as an HCM phenocopy.
Danon disease is a what condition caused by ______variants in what disorder?
That produces what and may transition from _______ cardiomyopathy to _______cardiomypathy
what gender are more severely affcted, often develop what CM by what years of age ?
Danon disease is an X-linked condition caused by pathogenic variants in LAMP2. It is a lysosomal storage disorder that produces LVH and may transition from hypertrophic cardiomyopathy to dilated cardiomyopathy.
Males are more severely affected, often develop end-stage CM by 20 years of age
List the 2 infiltrative phenocopies of HCM.
Amyloidosis
Sarcoidosis
List the 5 features that favor amyloidosis over HCM.
_______ Hypertrophy (shape of the heart)
whats the LVEF
_______hypertrophy
enlargement where
whats happening with the IAS
Concentric hypertrophy
Decreased LVEF
RV hypertrophy
Bi-atrial enlargement
Interatrial septal thickening
How does end-stage HCM with reduced EF differ from amyloidosis with reduced EF?
End- stage HCM with reduced EF is characterized by progressive ______ with wall ______
where as amyloidosis with reduced EF involves wall _____ as disease _______
End-stage HCM with reduced EF is characterized by progressive fibrosis with wall thinning, while amyloidosis with reduced EF involves wall thickening as disease progresses.
Simple reminder:
Amyloidosis can mimic HCM, but think concentric thickening, RVH, bi-atrial enlargement, interatrial septal thickening, and progressive wall thickening.
Explain sarcoidosis as an HCM phenocopy
is an what process of the what….
Sarcoidosis is an inflammatory granulomatous process of the myocardium.
List the 2 hypertrophy/thickening findings that can occur with sarcoidosis. and what involvement?
Hypertrophy of the septal myocardium
Localized thickening of the muscle, especially basal hypertrophy (this is why so many people get confused and think its HCM)
RV involvement (may see RV anurysm of the RV free wall, RV dysfunction, & TR)
Simple reminder:
Sarcoidosis can mimic HCM because it can cause septal or localized basal thickening.
Explain Friedreich’s ataxia as an HCM phenocopy. what disorder is it?
Friedreich’s ataxia is an autosomal recessive neurodegenerative disorder that can involve the heart and mimic HCM.
List the 5 key features of Friedreich’s ataxia.
the disorder
what does the nervous system causes
______ accumulation of _____
describe the walls
whats the LV function (systolic of diastolic?) - how is it affected
Autosomal recessive neurodegenerative disorder
Nervous system causes decreased mobility
Mitochondrial accumulation of iron
Concentric LV wall thickness or ASH
Decreased LV systolic function
Simple reminder:
Friedreich’s ataxia can cause LV thickening and reduced systolic function, so it can look like HCM.

what does this image show?
AMVL & PMVL are elongated

what does this image show?
Papillary muscle hypertrophy
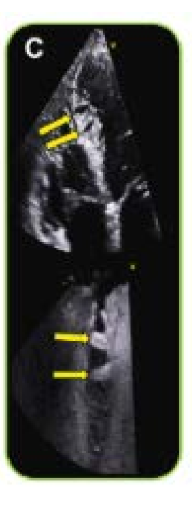
what does this image show? where are the found? and are more common in pt with what?
Myocardial crypts, deep cavities within the myocardium they are typically in the IVS and inferior basal wall, when you see Myocardial crypts more common in pt with HCM

what does this image show?
showing an abbranet muscle band that we dont measure in the septum measurement
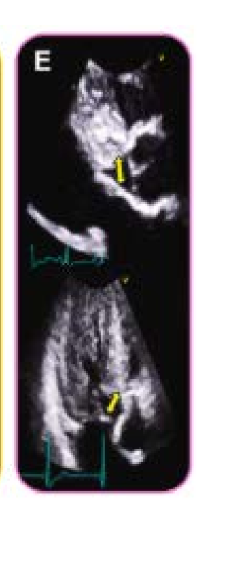
what does this image show
showing shorten septal to MV distance, measure the gap
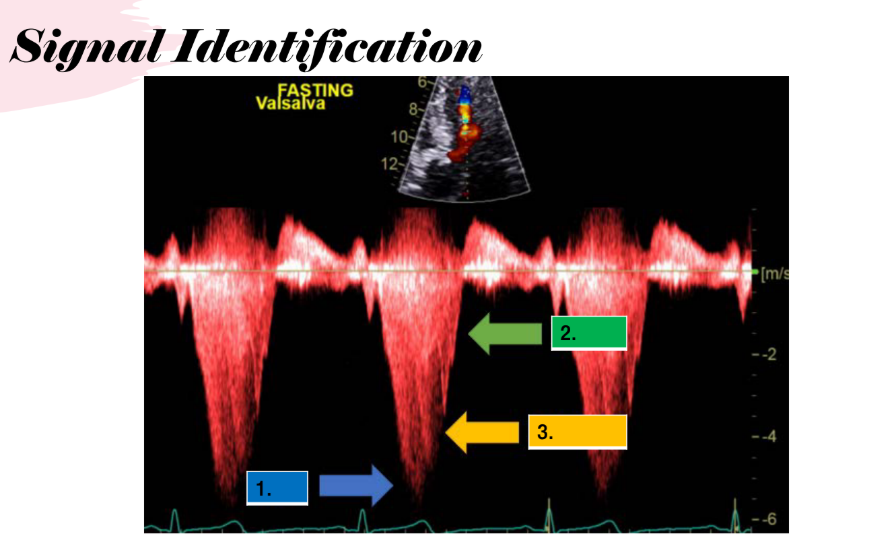
does fasting or eating cause a increase in gradients?
easting causes increase in gradients
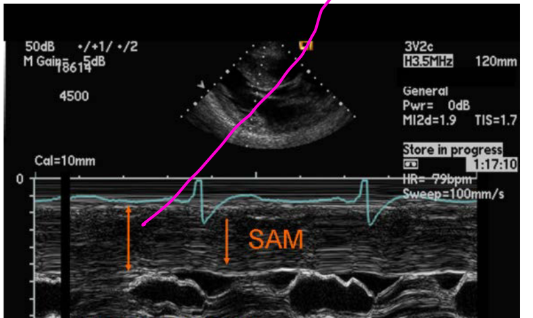
what does this image tell you, list 3
ASYMMETRIC SEPTAL Hypertrophy (ASH)
Massive IVS and Massive septal hypertrophy
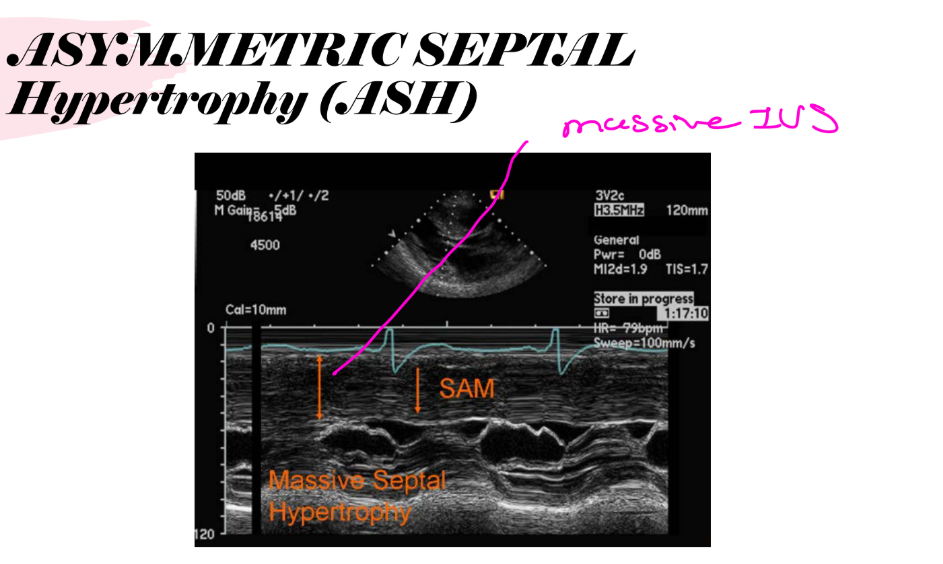
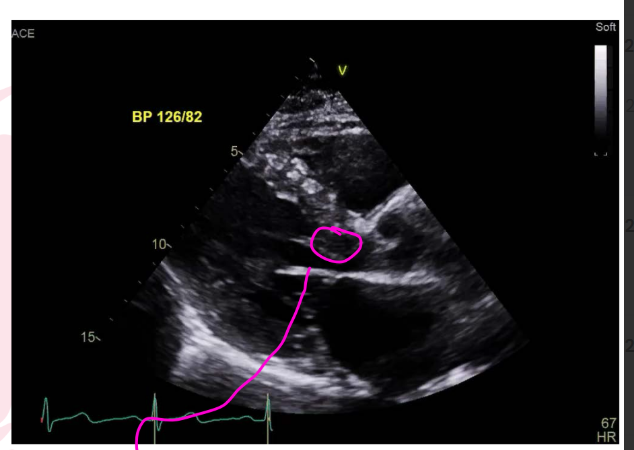
what does this image show you list 3
ASH, SAM, small Cavity Dimension
(very small LV and thicken walls)
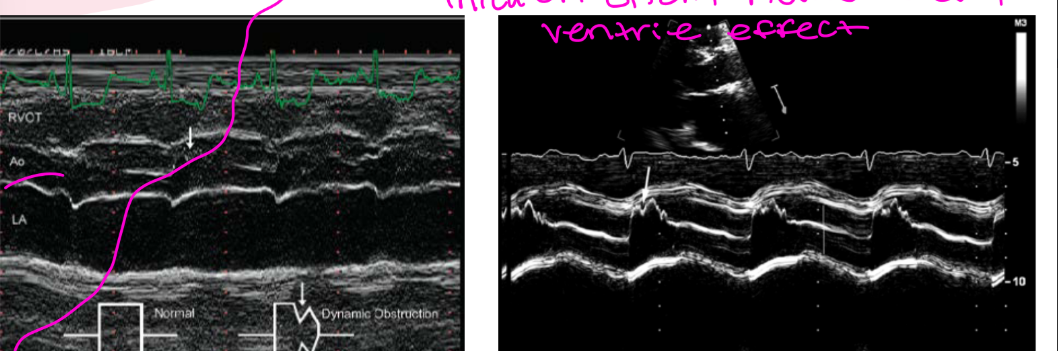
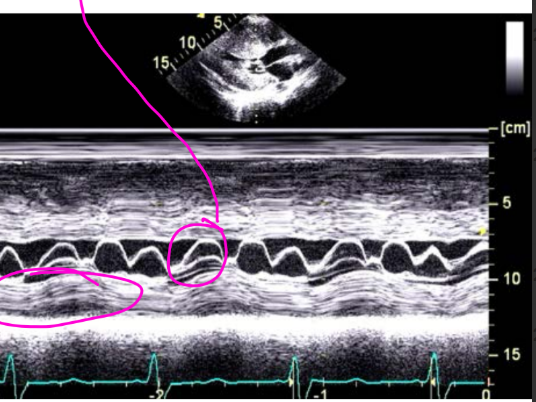
what does this image tell you and during what cardiac cycle?
The aortic valve opens normally, but when LVOT obstruction suddenly worsens in what cardiac cycle , forward flow ____, so the valve partially _____early and creates a ______on M-mode.
Mid-sysolic notching of AV
that mid systolic notching we are going to get that thicken septum that narrow the LVOT, blood acclerates throw the narrow portion ventri effect
the LVOT obstruction sudden increases during systole
then they systolic notching comes in where forward flow breifly drops and causes a reduced pressure across the AV
then the AV cusp paratily drifts towards closure which leads the notch on m-mode
and mid systolic notching is due to the ventri effect
so the valve normally open at first and then at mid systole the cusp paratially closes or notch (during mid systole) and then after they may re open slightly before final close again
Mid-systolic notching of the aortic valve means the aortic valve starts to close a little in the middle of systole, even though systole is not finished yet.
Normally:
LV contracts → aortic valve opens → blood leaves LV smoothly → valve closes at end systole
But in HOCM/LVOT obstruction, this happens:
1. The LV starts squeezing.
At first, blood moves out through the LVOT and the aortic valve opens normally.
2. The thick septum narrows the LVOT.
Because the pathway is narrow, blood has to speed up as it passes through.
3. The obstruction suddenly gets worse during systole.
As the LV squeezes harder and the cavity gets smaller, the LVOT becomes even more narrowed. SAM can also worsen the obstruction.
4. Forward flow briefly drops.
Even though the LV is still contracting, less blood is getting through the LVOT for a moment.
5. The aortic valve cusp partially drifts toward closing.
Because forward flow drops, there is less force holding the aortic valve fully open. So on M-mode, the valve looks like it makes a small “dip” or “notch” in the middle of systole.
6. Then it may reopen slightly before closing fully at the end.
So it can look like:
open → partial mid-systolic closure/notch → slight reopening → final closure
Your slide lists mid-systolic notching of the AV as an M-mode finding in HCM/HOCM.
A really simple way to remember it:
The aortic valve opens normally, but when LVOT obstruction suddenly worsens in mid-systole, forward flow drops, so the valve partially closes early and creates a notch on M-mode.
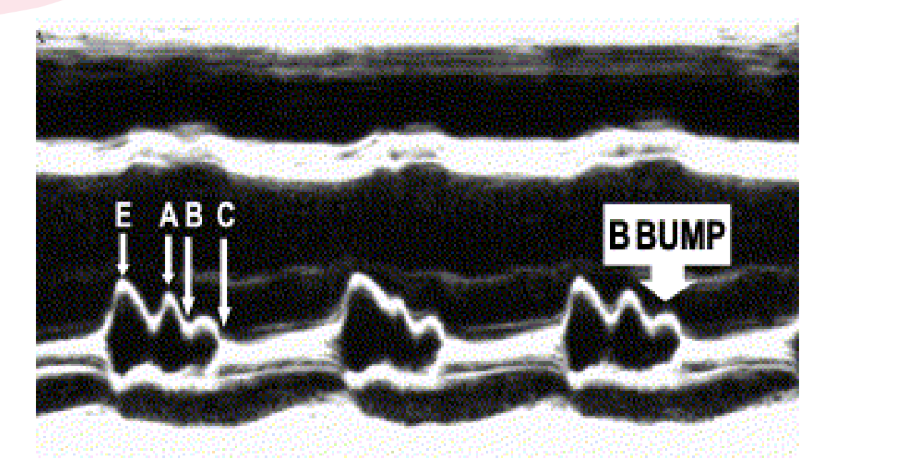
what does this image tell you, why does in HCM? explain how it happens ?
Happens because the in HCM the ventricle is thick and stiff, during diastole / relaxtion phase the LV fills poorly (doesnt fill well) and pressure increase and because of the LVEDP increase we get the B-Bump
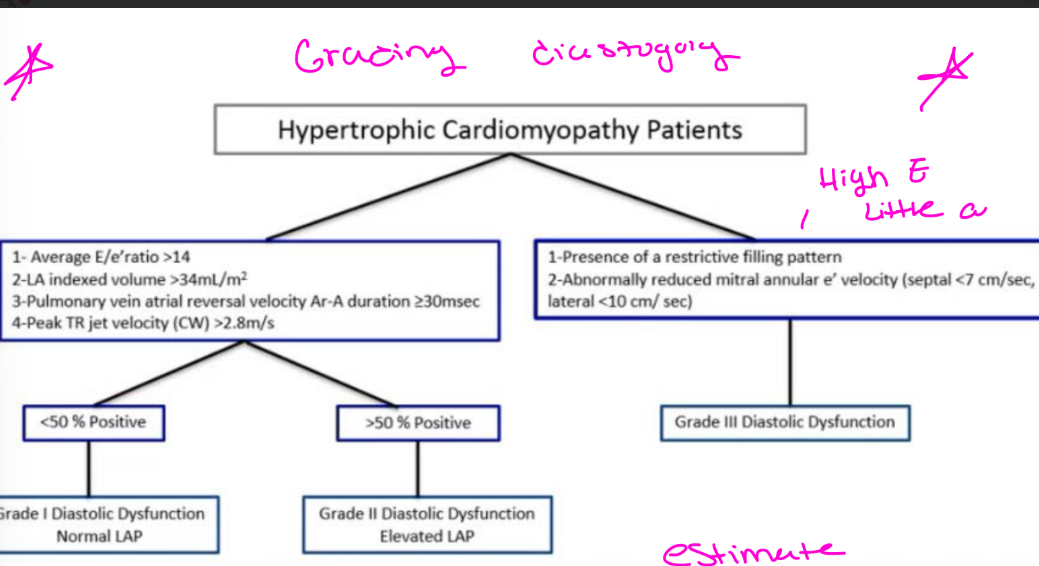
For Grading diastology, HCM Pt, why do we use a different grading chart instead of the tradtional diastology chart
abnoromal myocardium relaxtion is present in HCM, filling pressures is increase in HCM, LA enlargemnet, dynamic LVOTO it can alter that trans MV inflow pattern (PW at the MV tips) wont follow the typically progression that we see in other diastolic dysfunction, MR is common which alter the LA pressure, main goal estimate LV filling pressures and symptom burden
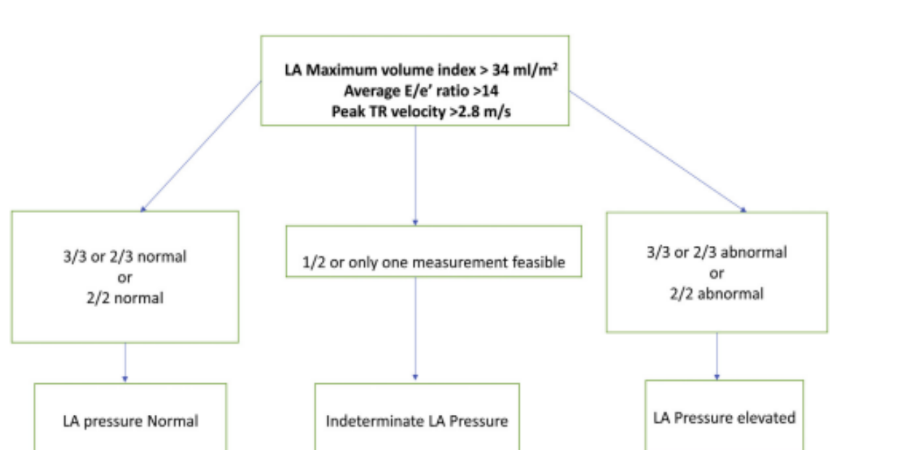
what is this chart used for?
Alogoirthm for estimation of mean LA pressure in HCM pt without significant MR
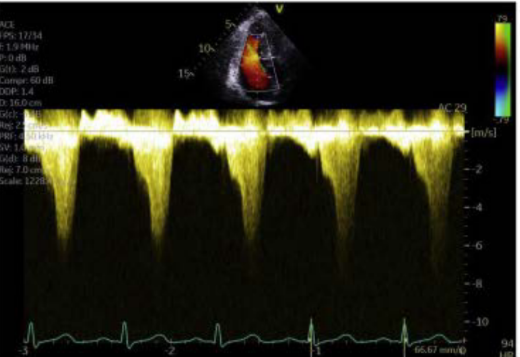
explain what you see the shape dont forget the cardiac cycle when does it peak and wht kind of raising is this
Dagger- shaped LVOT velocity
Late peaking concave LVOT signle demonstrates dagger shape signle =LVOTO (LVOTO mid -to - late systole)
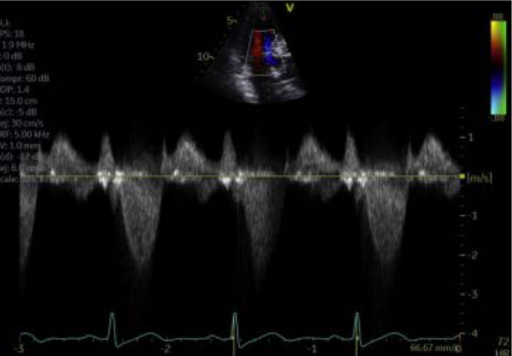
explain what you see the shape dont forget the cardiac cycle when does it peak and wht kind of raising is this
symmetric LVOT velocity
slows rasing , peaks at mid systole (instead of that later systole)
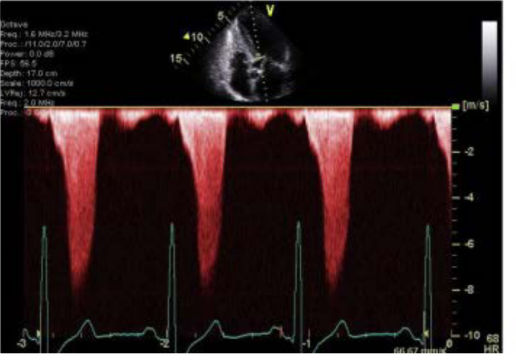
explain what you see
Late -peaking LVOTO velocity
concave dagger shaped signle
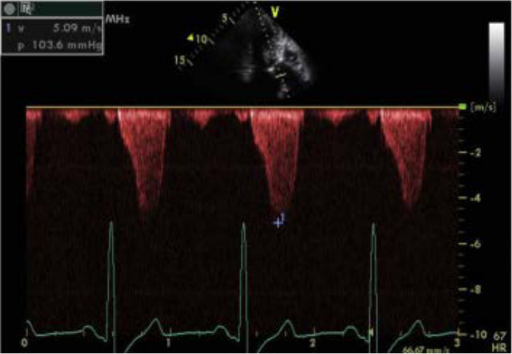
explain what you see
LVOTO velocity and superimposed MR velocity
The MR over rides the LVOTO, can make it seem like the gradient is higher then what it is (should use off axis views to separte the MR vs the LVOTO)
both MR and LVOTO occur at systole, MR is more rounded and parabolic shape
****if the signle is presented during IVCT or IVRT its more likely MR****
(Holoystolic)
****If it is limited to the ejection period and shows late systolic peak it is LVOTO****
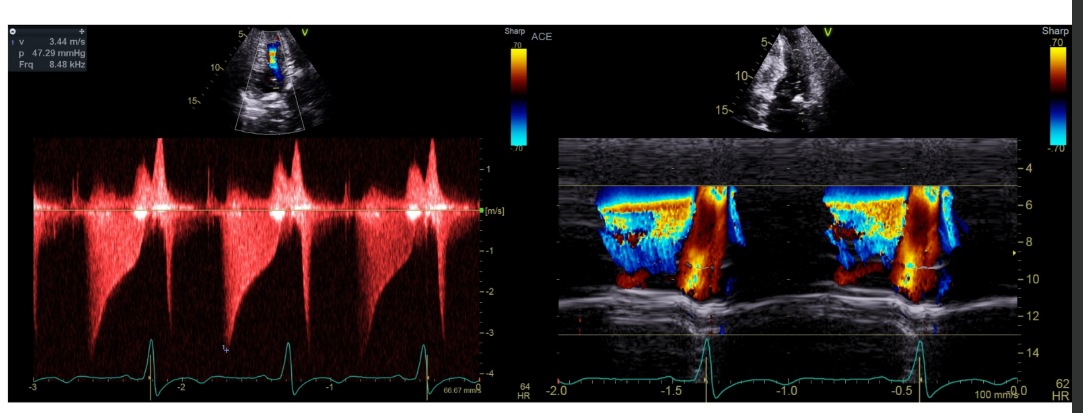
explain what the m-mode is showing
Apical Lobster claw
blue shows that rapid empty of pouch in early systole
and the red shows empty in diastole
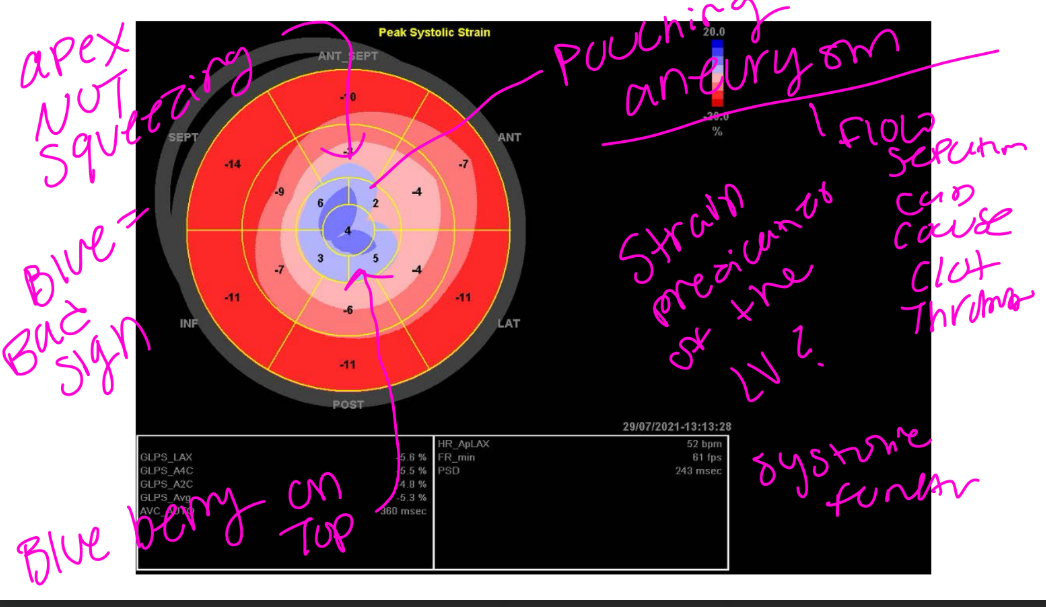
what does strain predict?
Strain is a predictor of the LV dysfunction greater then -18 is normal
blue is that anerusymal site - blue is bad, apical ansurysm, called the blue berry on top
HCM Phenocopies, what are ways we can do to differenite things?
Genetic testing, testing panal, biopsy