PANCE Blueprint Dermatology - All Smarty PANCE dermatology flashcard lesson sets combined (Smarty PANCE)
1/610
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
611 Terms
A 14-year-old boy with dozens of erythematous papules, pustules, and cysts. On closer examination, he also has atrophic scars on the lateral forehead. What's the dx?
Acne vulgaris
What are four main reasons that acne happens?
1. Increased sebum production (more androgens)
2. Clogged sebaceous glands (d/t proliferation of the follicular keratinocytes)
3. Propionibacterium acne overgrowth
4. Inflammation
Bad bacteria that causes most acne?
Cutibacterium acnes (formerly known as Propionibacterium acnes)
What medications can worsen or induce acne?
Lithium, steroids, OCPs, androgens
How is acne vulgaris diagnosed?
Acne vulgaris is diagnosed by a simple physical examination examining the appearance of the skin.
Open comedones?
Blackheads
Closed comedones?
Whiteheads
What is nodular/cystic acne?
Characterized by inflammatory hard lesions found deeper in the skin at the point where the hair follicle becomes plugged w/ dead skin cells (usually PAINFUL/TENDER)

Severity of acne?
Mild: comedones, small amount of papules/pustules
Mod: comedones, large# of papules/pustules
Severe: nodular (>5 mm) or cystic acne
Topical choices for acne?
1. Salicylic acid
2. Benzoyl peroxide
3. Topical retinoids (typically these are 1st line)
4. Topical antibiotics (clindamycin common)
Systemic choices for acne?
1. Systemic antibiotics (doxycycline, minocycline, clindamycin)
2. OCPs
3. Spironolactone
4. Isotretinoin
First line treatment for mild acne is?
First line treatment for mild acne is topical benzoyl peroxide.
What is the most effective topical agent for mild to moderate comedonal acne vulgaris.
Topical retinoids are the most effective topical agent for mild to moderate comedonal acne vulgaris.
If mild acne is unresponsive to topical benzoyl peroxide, topical antibiotics such as ________ and _______ may be added.
If mild acne is unresponsive to topical benzoyl peroxide, topical antibiotics such as clindamycin or erythromycin may be added
With moderate to severe acne, oral antibiotics such as __________ and __________ can be used in addition to topical treatment.
With moderate to severe acne, oral antibiotics such as doxycycline or minocycline can be used in addition to topical treatment.
Last line for acne?
Acutane (isotretinoin)
Inconvenient side effects of benzoyl peroxide?
Bleaches everything
Method of action of topical retinoids?
Main MOA: COMEDOLYTIC. Vit A derivatives that bind to RAR or RXR receptors found in keratinocytes. They help w normalization of follicular keratinization and decreased cohesiveness of keratinocytes.
Method of action of benzoyl peroxide?
- Decrease P. acne levels (antibacterial)
- Decreases inflammation from leukocytic and monocytic attraction to follicles
- Comedolytic effect: increases epithelial cell turn over
Why are topical antibiotics often given w/ benzoyl peroxide?
To reduce resistance
Side effect of certain systemic acne medications, particularly tetracyclines?
Photosensitivity
What acne medications can cause photosensitivity?
All vitamin A derivatives and oral tetracyclines
With acne medications, what are the 4 things we are targeting?
Inflammation, bacteria, oil, or actual cells
Should topical antibiotics be used alone in acne?
Nope!
Topical acids (salicylic and azelaic) work how?
Destroy the keratin/comedones
Isotretinoin unique things to know?
BEFORE STARTING: LFTs, LP, urine/serum pregnancy test in females
BIRTH CONTROL: Take 2 forms (1 month prior to initiation and 1 month after)
Side effects of isotretinoin?
Chapped lips, cheilitis, dry skin/mucus membranes, epistaxis, photosensitivity, teratogenic, depression, increases lipids/TGs, bone pain, mood changes, GI issues
General mgmt of each type of acne?
Mild: topical retinoids, BPO, topical abx, OCPs
Mod: add PO antibiotics or spironolactone
Severe: isotretinoins
What helps you differentiate acne vs. rosacea?
Comedones
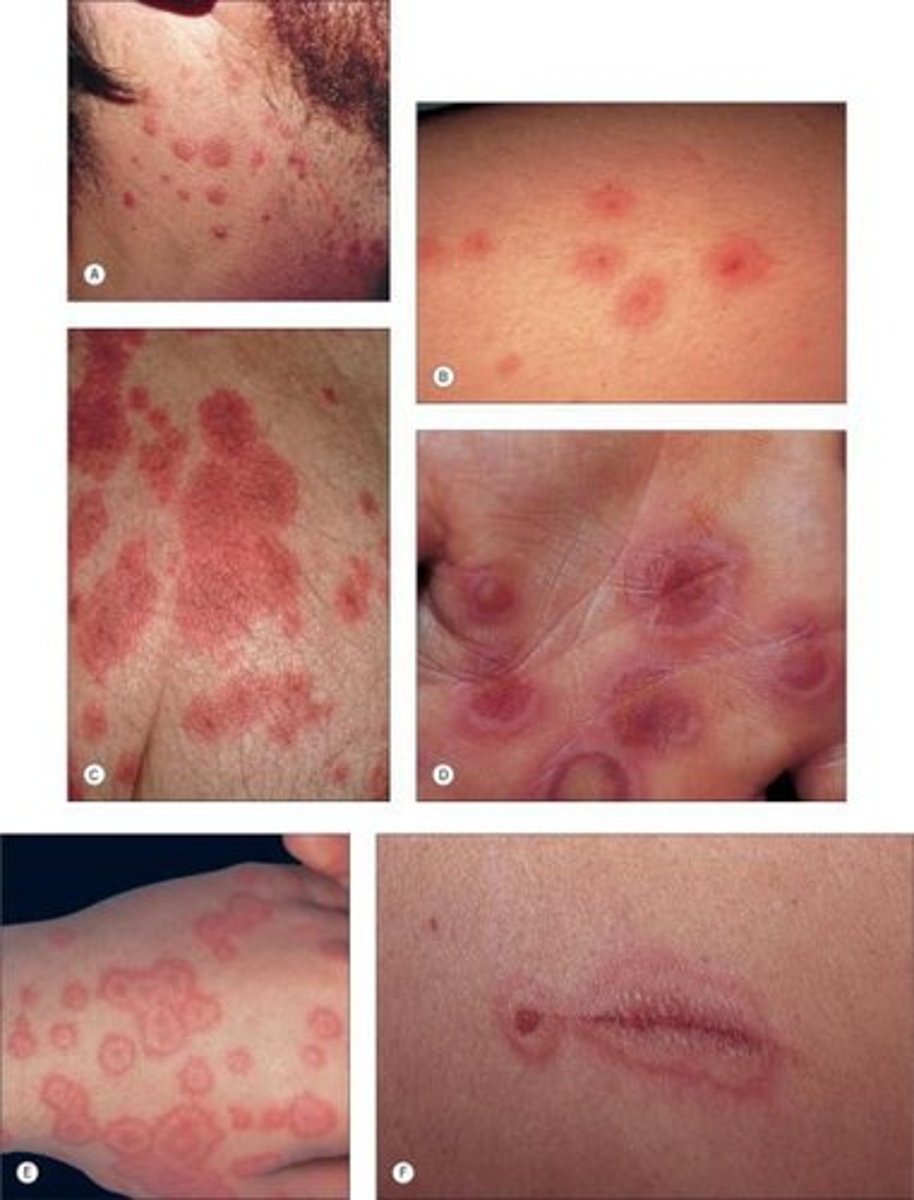
What is folliculitis?
Superficial infection of a hair follicle with small pustules/papules with surrounding erythema

What are the causes of folliculitis?
Commonly caused by S. aureus but can be caused by other organisms. Pseudomonas folliculitis is seen in hot tub users
Viral folliculitis is most commonly associated with what infections?
Viral folliculitis is most commonly associated with herpesvirus infections
What is another form of noninfectious folliculitis caused by ingrown hairs in the beard area from shaving in the direction against the grain of hair growth
Pseudofolliculitis barbae (razor bumps), is another form of noninfectious folliculitis caused by ingrown hairs in the beard area from shaving in the direction against the grain of hair growth
How is folliculitis diagnosed?
The diagnosis is usually clinical - culture for bacteria, viruses, and fungi in diseases refractory to standard therapy or if unusually severe
First line treatments for folliculitis?
Gentle cleansing with antibacterial soap and mild compresses help
Mupirocin ointment and topical benzoyl peroxide cream are first-line
Topical application of clindamycin or erythromycin works well on mild cases of infectious folliculitis
Second line treatment of folliculitis in more extensive cases?
In more extensive cases, oral antibiotics may be necessary - dicloxacillin and cephalexin. If methicillin-resistant S. aureus is suspected, patients should be treated with trimethoprim/sulfamethoxazole, clindamycin, or doxycycline
Treatment of hot tub folliculitis?
Hot tub folliculitis usually resolves without treatment; severe or recalcitrant cases may be treated with an oral fluoroquinolone
Clinical features of rosacea?
Symmetric erythema of the face
Telangiectasia
Pustules and central facial edema

Triggers for rosacea?
EtOH, high temperatures, spicy foods, hot baths
What helps you differentiate acne vs. rosacea?
Differentiate from acne by lack of comedones (blackheads)
First-line therapies in mild to moderate rosacea?
Topical metronidazole, azelaic acid, and topical ivermectin are considered first-line therapies in mild to moderate disease
Second-line therapies for rosacea in those who fail topical therapy?
Oral antibiotic therapy with tetracycline, doxycycline, and minocycline in those who fail topical therapy
Treatment for those who fail to respond to topical and oral therapy
Oral isotretinoin in patients who fail to respond to topical and oral therapy
What medication may be used for flushing in patient with rosacea?
Clonidine may be used for flushing in patient with rosacea?
What is rhinophyma?
An enlarged nose due to rosacea
What treatment has been used for the treatment of rhinophymatous skin changes?
Laser ablation has been used for the treatment of rhinophymatous skin changes
A 6-year-old male presents to the clinic with several target-looking lesions on his arms and chest and has been taking antibiotics for bronchitis. What do you suspect?
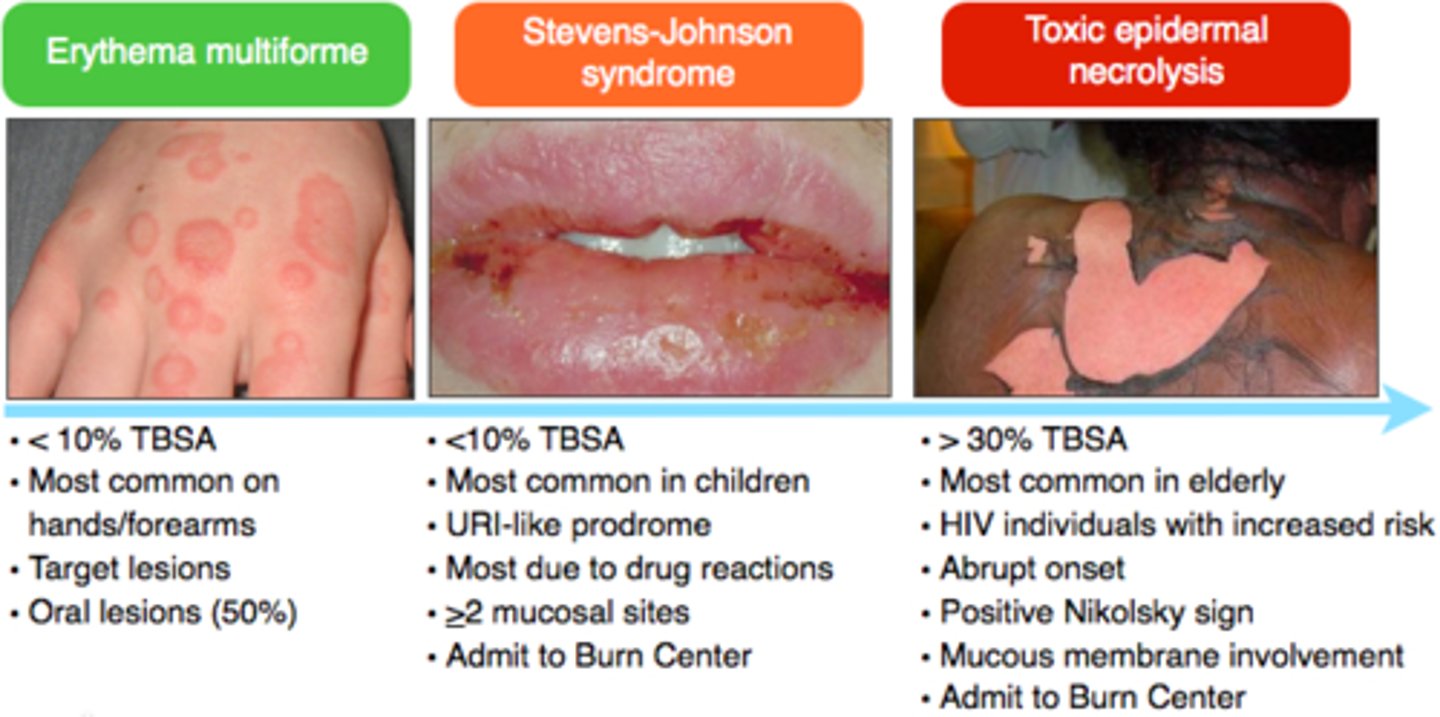
Erythema Multiforme (EM)
What is erythema multiforme?
Erythema multiforme is a target-like lesion associated with various infections - most commonly herpes simplex virus (HSV), medications (sulfa drugs), and other various triggers

Erythema multiforme is associated with which virus?
Erythema multiforme is associated with herpes simplex virus
What characterizes the rash of erythema multiforme?
Target-like shape, raised, blanching, and lack of itchiness help characterize this rash
Where are the skin lesions of erythema multiforme predominately found?
Skin lesions predominantly involve the extremities (hands, feet, and mucosa)
What are the two types of erythema multiforme?
Erythema multiforme major and minor
Describe erythema multiforme (EM) major
EM Major causes widespread skin lesions and affects 2 + mucosal sites
Describe erythema multiforme (EM) minor
EM Minor affects a limited region of the skin and 1 type of mucosa (usually oral)
How do you differentiate erythema multiforme from Steven Johnson Syndrome (SJS)?
EM may appear similar to Steven Johnson Syndrome (SJS) but SJS has a more generalized distribution of lesions; concentrated on the trunk (EM extremities and mouth), an absence of raised typical target lesions and atypical flat (not raised) target lesions or macules with the coalescence of lesions
Does erythema multiforme have a negative or positive Nikolsky sign?
Negative Nikolsky sign (as opposed to SJS/TEN)

What is the treatment for erythema multiforme?
Symptomatic treatment with oral antihistamines and topical corticosteroids for mild cases; mouthwashes or topical steroid gels for oral disease.
A 9-year-old male on antibiotics for a UTI has a cough, aching, headache, fever, a red rash across the face and trunk, and oral mucosal lesions. What is your diagnosis?
Stevens-Johnson Syndrome (SJS)
What is Stevens-Johnson syndrome?
Stevens-Johnson syndrome (SJS) is a milder form of toxic epidermal necrolysis (TEN) with LESS THAN 10% of body surface area detachment
SJS vs. TEN?
Stevens-Johnson syndrome and toxic epidermal necrolysis are considered variations of the same skin condition. If 10% of the body surface is affected, it's generally considered Stevens-Johnson syndrome; if 10-30% is affected, it's considered an overlap between Stevens-Johnson syndrome and toxic epidermal necrolysis; and if more than 30% is affected, it's considered toxic epidermal necrolysis.
SJS <10%
SJS/TEN overlap 10%-30%
TEN >30%
What is the cause of Stevens-Johnson syndrome?
Most common with drug eruptions: Over 100 medications have been implicated in causing SJS especially sulfa and anticonvulsant medications
What are two distinguishing symptoms of Stevens-Johnson syndrome and toxic epidermal necrolysis that differ from other similar conditions?
Two distinguishing symptoms of Stevens-Johnson syndrome and toxic epidermal necrolysis from other similar conditions are that both mucosal linings and skin are affected
Name two infections that can also be a trigger of SJS?
In addition, some types of infections, like Mycoplasma pneumoniae or cytomegalovirus, can also be a trigger.
How is SJS diagnosed?
A clinical diagnosis is typically made based on symptoms. But a biopsy of the affected area can help make a definitive diagnosis.
How is SJS treated?
The treatment for Stevens-Johnson syndrome is similar to the protocol for treating patients with extensive burns. Treatment includes immediately removing the trigger, followed by supportive therapy
What is the name of the separation of papillary dermis from basal layer when gentle lateral pressure is applied?
The Nikolsky sign is the separation of papillary dermis from basal layer when gentle lateral pressure is applied. Nikolsky's sign is almost always present in Stevens-Johnson syndrome/toxic epidermal necrolysis and staphylococcal scalded skin syndrome.

A patient on cephalexin presents with fever, a red rash involving 50% of the body, and generalized detachment of the skin. What do you suspect?
Toxic Epidermal Necrolysis (TEN)
What is Toxic Epidermal Necrolysis (TEN)?
Toxic epidermal necrolysis is a more severe form of Stevens-Johnson syndrome with > 30% of the body surface area affected
SJS vs TEN (Toxic Epidermal Necrolysis)
Stevens-Johnson syndrome and toxic epidermal necrolysis are considered variations of the same skin condition. If 10% of the body surface is affected, it's generally considered Stevens-Johnson syndrome; if 10-30% is affected, it's considered an overlap between Stevens-Johnson syndrome and toxic epidermal necrolysis; and if more than 30% is affected, it's considered toxic epidermal necrolysis.
SJS <10%
SJS/TEN overlap 10%-30%
TEN >30%
What's a good way to remember the body surface area affected in TEN?
A good way to remember the body surface area affected in TEN is "T hree x T en = T hirty percent in Toxic Epidermal Necrolysis
Triggers for toxic epidermal necrolysis?
Triggers for toxic epidermal necrolysis are typically certain kinds of medications!
Which medications can cause toxic epidermal necrolysis?
Medications such as lamotrigine, carbamazepine, allopurinol, sulfonamide antibiotics, and nevirapine can cause toxic epidermal necrolysis.
A virus that can cause toxic epidermal necrolysis?
A virus that can cause toxic epidermal necrolysis is cytomegalovirus.
The bacteria most-commonly associated with toxic epidermal necrolysis?
The bacteria most-commonly associated with toxic epidermal necrolysis is Mycoplasma pneumoniae.
Nearly all patients with toxic epidermal necrolysis appear with lesions where?
Nearly all patients with toxic epidermal necrolysis appear with oral, ocular, or genital mucositis, which helps to diagnose the condition
How is the diagnosis of TEN confirmed?
The diagnosis of TEN is confirmed by biopsy (showing necrotic epithelium).
What sign describes the separation of papillary dermis from basal layer when gentle lateral pressure is applied?
The Nikolsky sign is the separation of papillary dermis from basal layer when gentle lateral pressure is applied; this is a helpful diagnostic feature of toxic epidermal necrolysis.

What sign is the lateral extension of bullae with pressure and is a diagnostic feature of toxic epidermal necrolysis.
The Asboe-Hansen sign is the lateral extension of bullae with pressure and is a diagnostic feature of toxic epidermal necrolysis.

Treatment of TEN?
Treatment typically includes hospitalization, particularly in a burn or intensive care unit for severe cases.
Triggering medications should be immediately stopped
-Systemic immune modulators - like antihistamines; intravenous immunoglobulins or IVIG; or corticosteroid may be used to suppress the hypersensitivity response.
-Supportive therapy with pain medication, hydration, and sterile wound care can help to prevent further complications.
After healing, there can sometimes be scarring.
A 4-year-old female with spots of hair loss that have been progressively worsening. According to the patient's mom, her daughter lost all the hair on her head, including eyelashes and eyebrows two years ago. Her hair grew back, and now new spots of hair loss are appearing. What is the dx?
Alopecia areata
What is alopecia?
Alopecia refers to a loss of hair from part of the head or body and it can occur in a wide variety of disorders.
What is the "hair pull test?"
Assessment of activity on the scalp may be done with a hair pull test, done by gripping about 20 hairs and gently pulling upward and away from the skin
What defines a positive hair pull test?
Normally, about three hairs may fall out with each pull, while if more than 10 hairs are removed, the test is considered positive
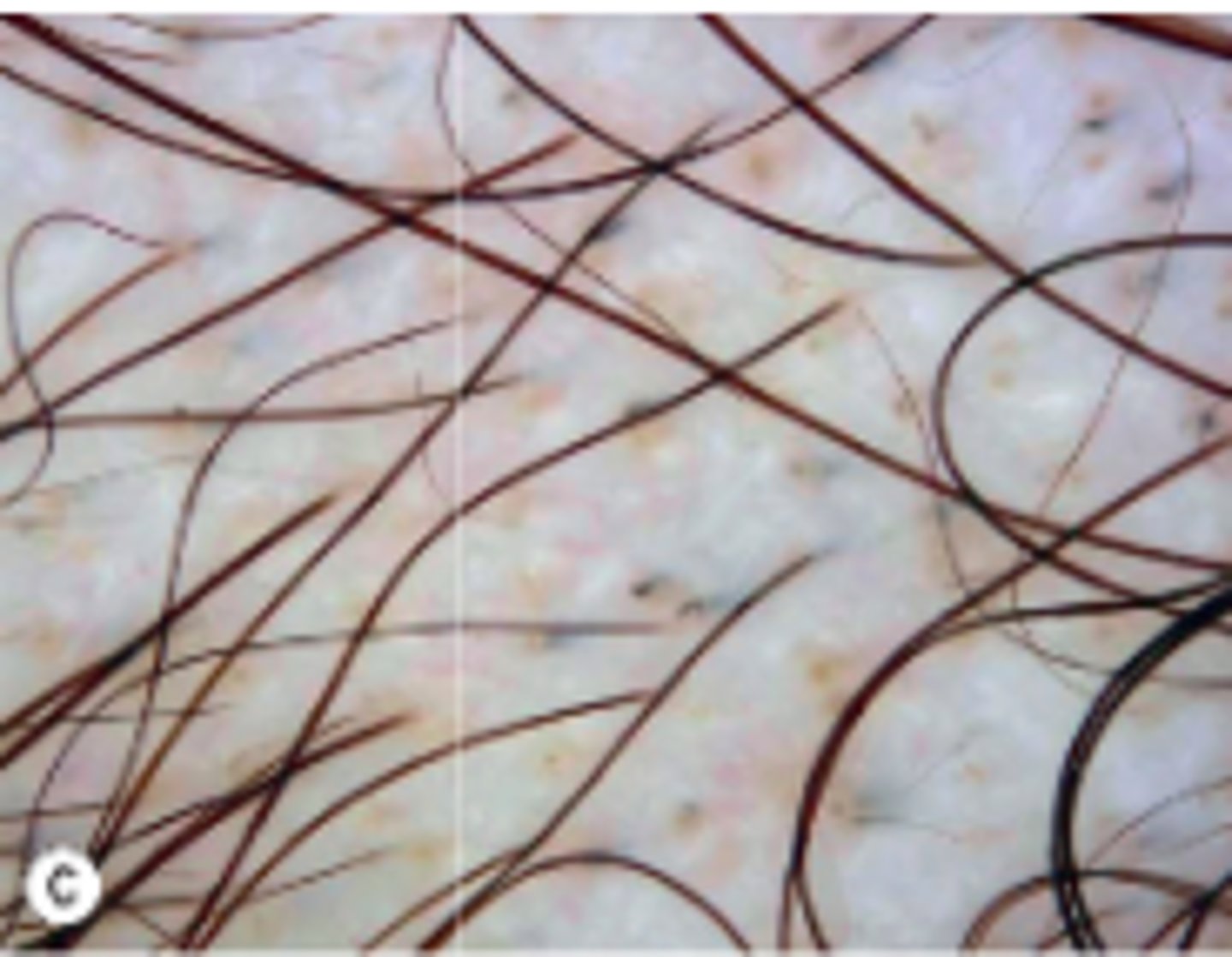
What is trichoscopy?
Trichoscopy is a noninvasive method of examining hair and scalp which is performed with the use of a dermatoscope. This traditionally consists of a magnifier, a non-polarised light source, a transparent plate, and a liquid medium between the instrument and the skin.
What is a pluck test?
The pluck test is conducted by pulling hair out by the roots. The root of the plucked hair is then examined under a microscope to determine the phase of growth, and is used to diagnose if there’s a defect of anagen or telogen.
These hairs have sheaths attached to their roots and is consistent with a long (2- to 6-year) growing phase
Anagen: A long (2- to 6-year) growing phase. Anagen hairs have sheaths attached to their roots
These hairs have tiny bulbs without sheaths at their roots and is consistent with a short (2- to 3-month) resting phase
Telogen: A short (2- to 3-month) resting phase. Telogen hairs have tiny bulbs without sheaths at their roots
Describe the three categories of alopecia?
Broadly, hair loss disorders can be divided into:
1. Cicatricial or scarring alopecias
2. Non scarring alopecias
3. Structural hair disorders
Characterized by irreversible damage to the hair follicle that results in interruption of hair cycling and permanent hair loss if not treated in time
Cicatricial alopecias are characterized by irreversible damage to the hair follicle that results in interruption of hair cycling and permanent hair loss if not treated in time. Cicatricial alopecias may be primary or secondary.
What are primary cicatricial alopecias?
Primary cicatricial alopecias are inflammatory disorders with unknown cause, which may be associated to inflammatory diseases like lupus or lichen planopilaris, and are subdivided by the type of predominant inflammatory infiltrate detected on scalp biopsy into lymphocytic, neutrophilic, and mixed primary cicatricial alopecias.
What are secondary cicatricial alopecias?
Secondary cicatricial alopecia always has a known cause. Causes include tinea capitis, radiation therapy, and surgical or injury scars.
Diagnosis of cicatricial alopecia?
A scalp biopsy is necessary to diagnose the type of cicatricial alopecia, to determine the degree of activity, and to select appropriate therapy.
Treatment of tinea capitis?
Treatment involves systemic antifungals like griseofulvin, terbinafine, fluconazole, or itraconazole. Adjunctive interventions for tinea capitis include using a shampoo with antifungal properties to reduce risk of spread of infection to other individuals.
What is alopecia areata?
Alopecia areata is a relatively common form of nonscarring alopecia in which an autoimmune process leads to the spontaneous loss of hair on the scalp or other areas.
Presentation of alopecia areata?
Most often, alopecia areata presents with smooth circular patches of complete hair loss that develop over a period of a few weeks.
Trichoscopy findings in alopecia areata?
Trichoscopy findings include yellow dots, short vellus hairs, black dots, tapering hairs, and broken hairs
Treatment of alopecia areata?
In most cases, there’s spontaneous regrowth of hair. Individuals who want additional treatment may get topical or intralesional injections of corticosteroids if alopecia is limited; while individuals with extensive alopecia may get topical immunotherapy with diphenylcyclopropenone or squaric acid dibutyl ester.
● Systemic glucocorticoids are occasionally prescribed as a temporary measure to slow hair loss in individuals with rapidly progressing and extensive hair loss.
What is traction alopecia?
Focal hair loss in traction alopecia results from prolonged pull or tension on the hair follicle, usually due to hairstyles such as tight ponytails or braids
Treatment of traction alopecia?
Treatment involves discontinuation of traction hairstyles
What is patterned alopecia?
Patterned alopecia is a common condition with increasing age, most frequently presenting as slow, progressive hair thinning and loss in a characteristic distribution on the frontal and crown areas of the scalp with relative sparing of the occipital scalp.
● The condition is mediated by the action of androgens on hair follicles in genetically susceptible individuals, and that’s why it’s called androgenetic alopecia.