Dietary Reference Intakes (DRIs): Key Concepts and Appropriate Uses
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
39 Terms
Describe the initial renditions of the RDAs.
1941 the Food and Nutrition Board was formed to review the literature and establish the first official dietary standards.
In 1943, the Recommended Dietary Allowances (RDAs) were started, and these considered gender, life stage, and activity level in their assessments. Used by nutrition professionals for dietary planning (because they included recommended food patterns) and assessment of individuals and groups.
How were the current dietary standards set?
In 1997 the Food Nutrition Board and Institute of Medicine began to release the DRIs. These were a set of nutrient reference standards for the USA and Canada that considered the distribution of nutrient requirements and the possibility of excess.
What do the Dietary Reference Intakes (DRIs) include?
- Estimated Average Requirement (EAR)
- Recommended Dietary Allowance (RDA)
- Adequate Intake (AI)
- Tolerable Upper Intake Level (UL)
Who were the DRIs intended to be used with?
Intended to be used with healthy people. They do not consider the effects of disease processes on nutrient requirements or toxicity. Additionally, they do not consider drug-nutrient interactions, and they are not appropriate to replete previously malnourished or meet increased requirements for disease.
Define parenteral feeding.
Intravenous feeding that bypasses eating/digestion
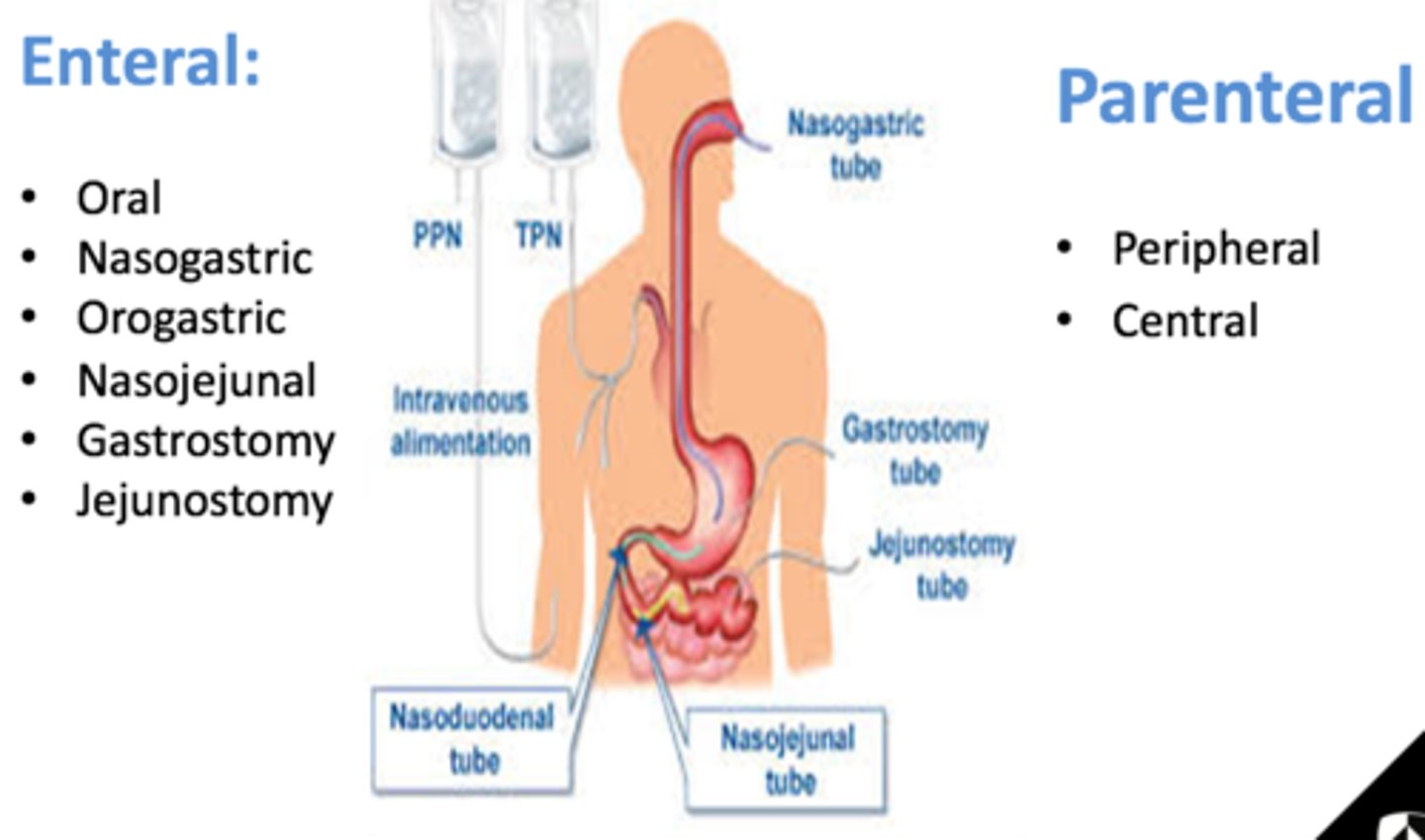
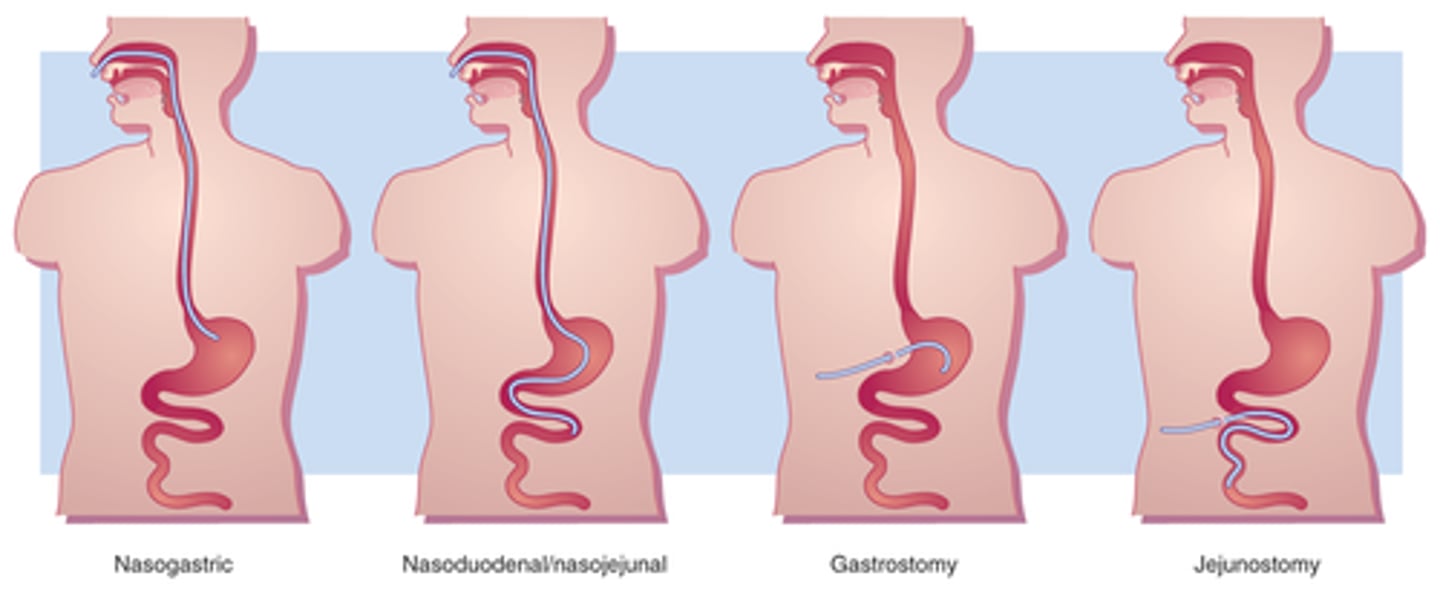
Define enteral feeding.
Feeding by mouth, or tube feeding that allows for normal digestive processes. Food enters normal.
What sources of a nutrient do the DRIs apply to?
The DRIs apply to all sources (food, beverages, supplement) of an nutrient and apply to usual intake (ongoing average intake, more narrow distribution compared to day-to-day intake)!
What are the key concepts that apply to the DRIs?
1. Intended for use with healthy people
2. Apply to all sources of a nutrient
3. Apply to usual intake
How are the DRIs established?
Standing Committee on the Scientific Evaluation of Dietary Reference Intakes commissions panels for specific components of nutrition. The Upper Reference Levels Subcommittee and Uses of DRIs Subcommittee work with these panels.
What do these DRI committees look at?
Metabolism, absorption, storage, excretion, and other components that affect nutrient bioavailability.
Does this to develop estimates of intakes: good nutrition throughout the lifespan and decreased risk of chronic disease.
What are the life stage groups in the DRIs?
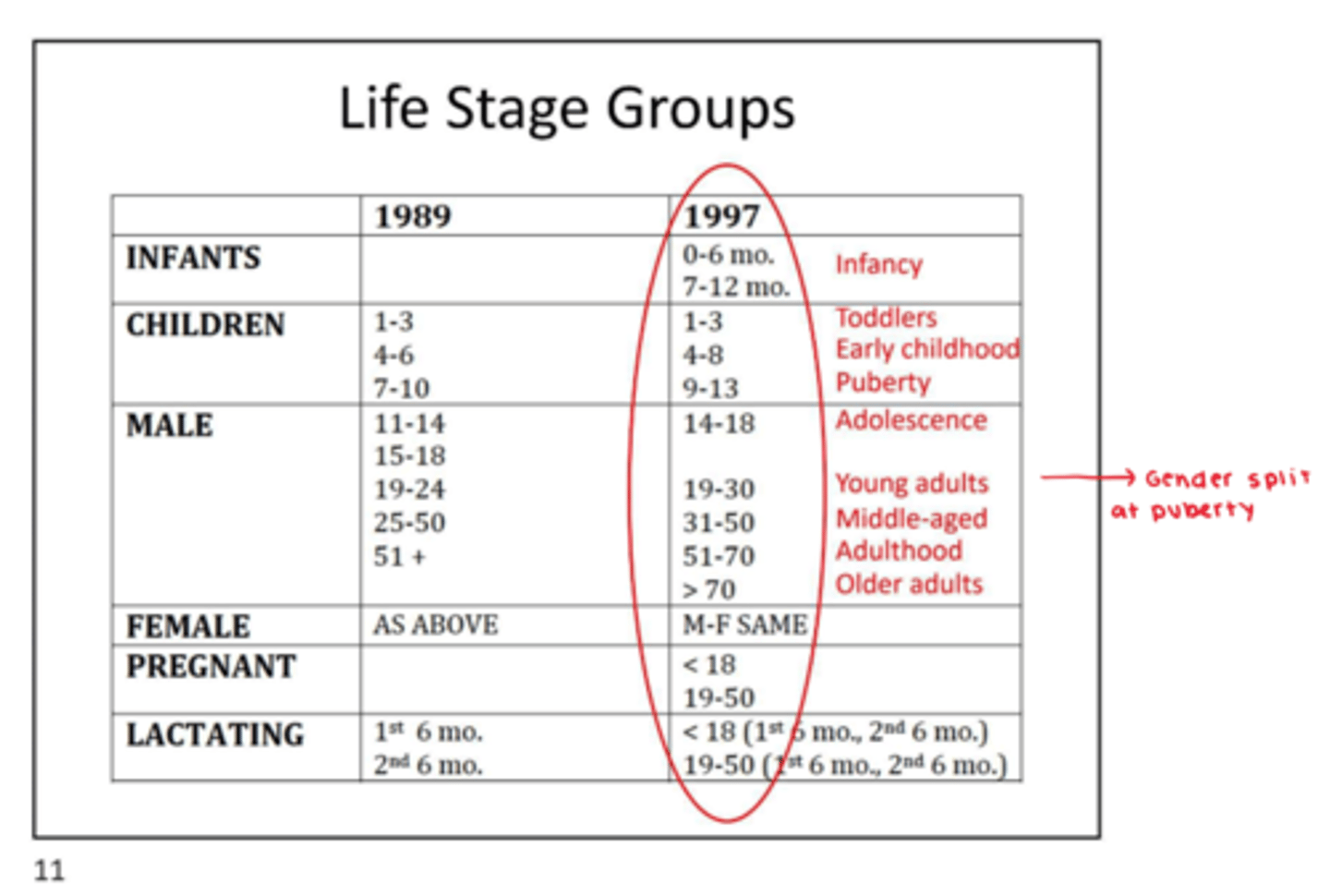
What are some examples of how the requirement of a nutrient can change based on age, gender, or life stage?
- Men older than 14 have a higher RDA for vitamin C. This means they have a higher requirement, because women have a higher plasma vitamin C content.
- Menstruating women have a higher RDA because iron lost in the blood increases the requirement
- Pregnant and lactating women have a higher vitamin C RDA and requirement than other women because of active transfer to the fetus
What is the effect of smoking on the requirement for vitamin C?
Smokers have a higher RDA for vitamin C than non-smokers. Smokers include those who are chronically exposed to environmental cigarette smoke.
Plasma [vitamin C] is significantly lower in smokers than in nonsmokers, despite similar Vitamin C intakes because vit. C is an antioxidant and smoking increase oxidative stress so there is more vit C turnover.
Smokers require an additional 35 mg/d over nonsmokers to meet the RDA.
What are some of the factors that affect the dietary requirements of nutrients in humans?
1. Dietary factors -chemical form, presence of other constituents, processing
2. Host factors - age, sex, genetic
3. Physiological states - growth, pregnancy, lactation, aging
4. Pathological states - metabolic disease, trauma, neoplasia, other stress and drugs
5. Environmental factors - physical (temperature, altitude), biological (disease), social (dietary habits, sanitation, activity, hygiene)
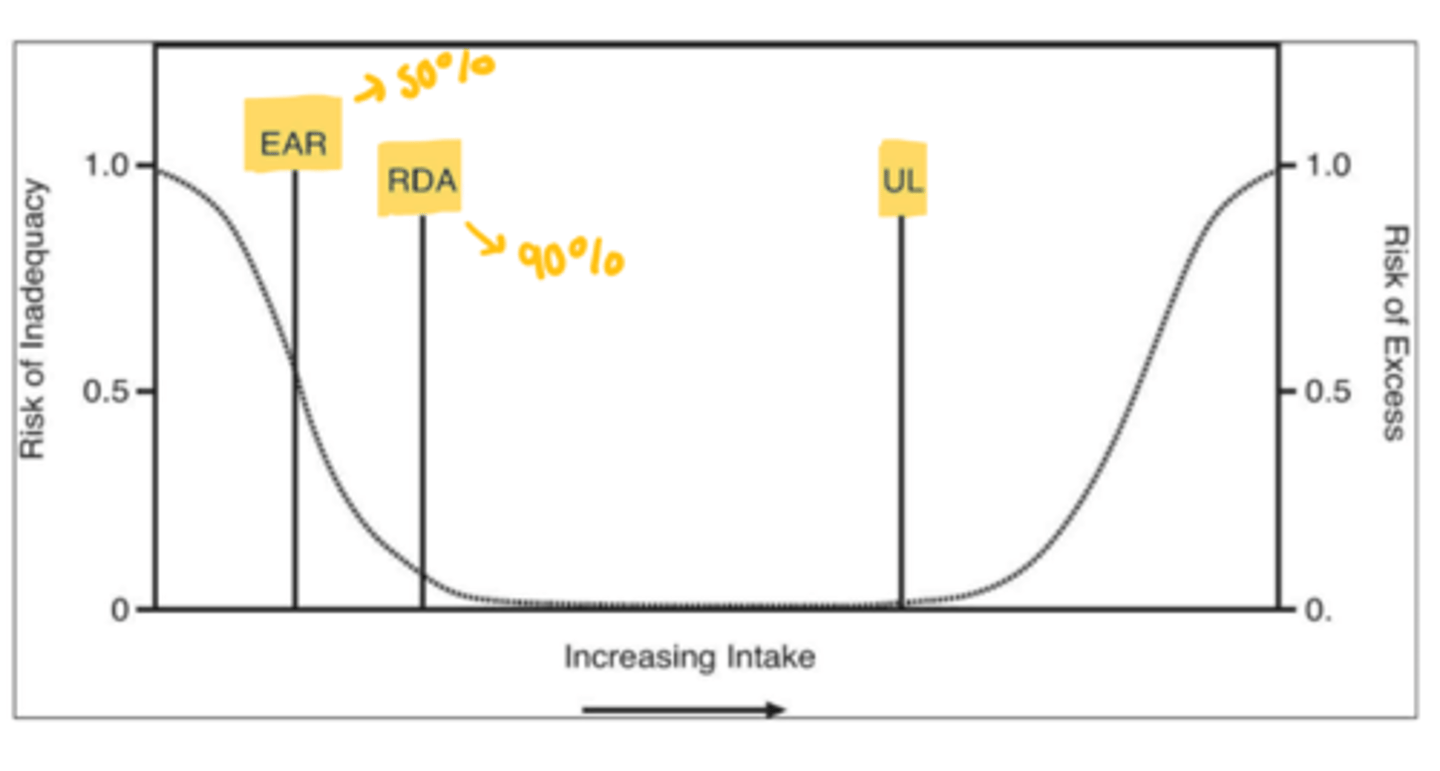
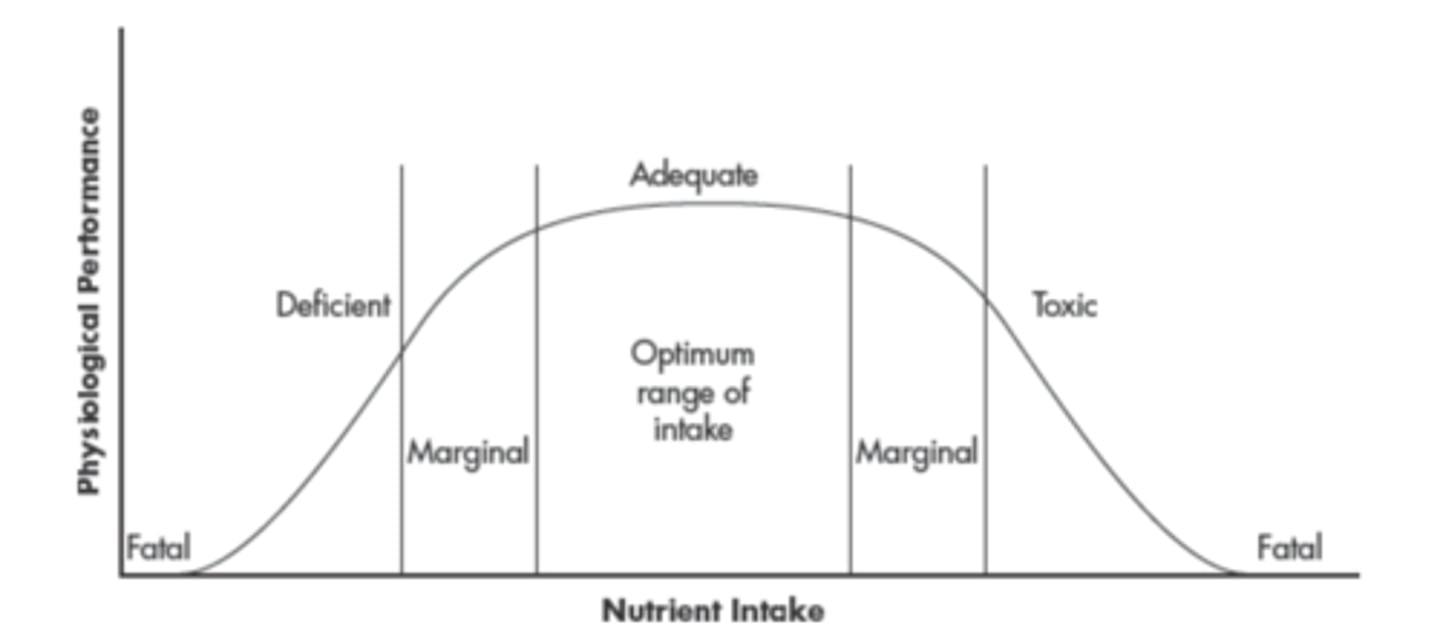
What is Bertrand's Rule?
The concept of dose. As intake increases or decreases, the curve declines from optimal to marginal and the risk for deficiency or toxicity increases.
It is the concept that describes the optimal range of intake related to optimal health.
What is a requirement?
The lowest continuing intake level that, for a specific indicator of adequacy, will maintain a defined nutriture.
Define minimum requirement.
Minimum Requirement: the least amount of nutrient needed to prevent clinical symptoms or support a defined biochemical response.
What are the indicators of adequacy?
1. Growth
2. Clinical signs + symptoms
3. Biochemical measures
4. Balance studies
What are some examples of clinical signs and symptoms of deficiency?
Vitamin C deficiency/scurvy = inflamed gums, ecchymosis on skin, pinpoint bleeding around hair follicles.
Niacin deficiency/pellagra = pigmented rash on areas exposed to sun, red, beefy tongue
Give examples of biochemical measures to determine adequacy.
1. Functional test - RBC transketolase activity as indicator of thiamin (co-factor) adequacy. In thiamin depletion, baseline activity of transketolase is low, but incremental response after addition of thiamin is enhanced
2. Testing negative balance, tissue depletion, and functional changes
What do balance studies show?
As indicators of adequacy, balance = intake - excretion products
Positive balance = intake > output
Negative balance = intake < output
Example is nitrogen balance study
What is the summary for indicators of adequacy?
1. Balance studies
2. Biochemical measures = blood levels, enzyme activity, urinary excretion
3. Clinical evaluation
Requirement refers to a specific indicator of adequacy for each nutrient. But adequate for what? What is the criteria?
Adequate enough to prevent deficiency and maintain a defined nutriture (growth in children, or level in blood, urine, or tissue).
Criteria for indicators of adequacy
- May be deemed to the most appropriate to determine the risk that an individual will become deficient.
- Relate to maintaining a desirable level of function
- **NEW Reducing the risk of chronic disease... OPTIMAL body pools/stores
What are dietary factors?
Form of a nutrient, presence or level of other nutrients or dietary components.
Nutrients can be found in different chemical forms. What are some examples?
In natural dietary sources, fortified foods, or supplements
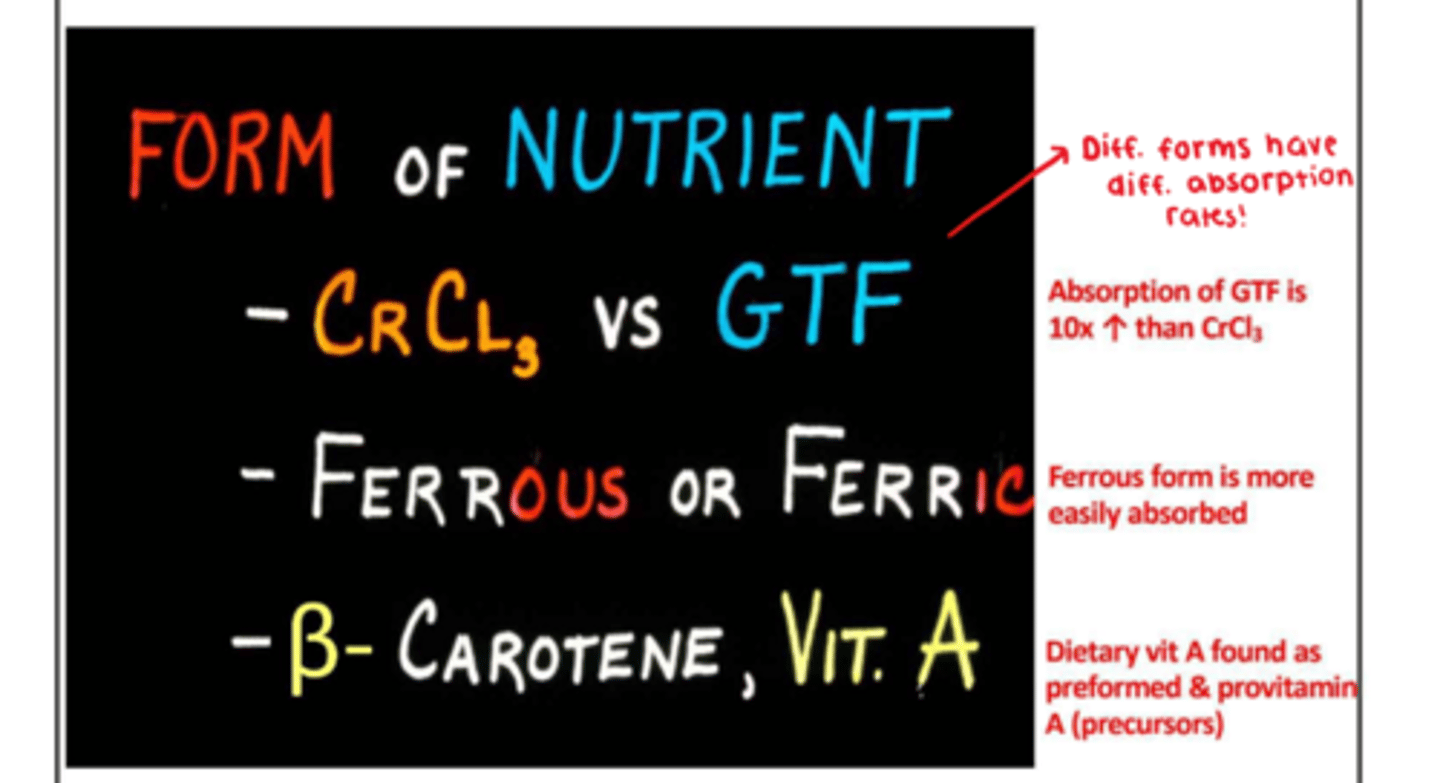
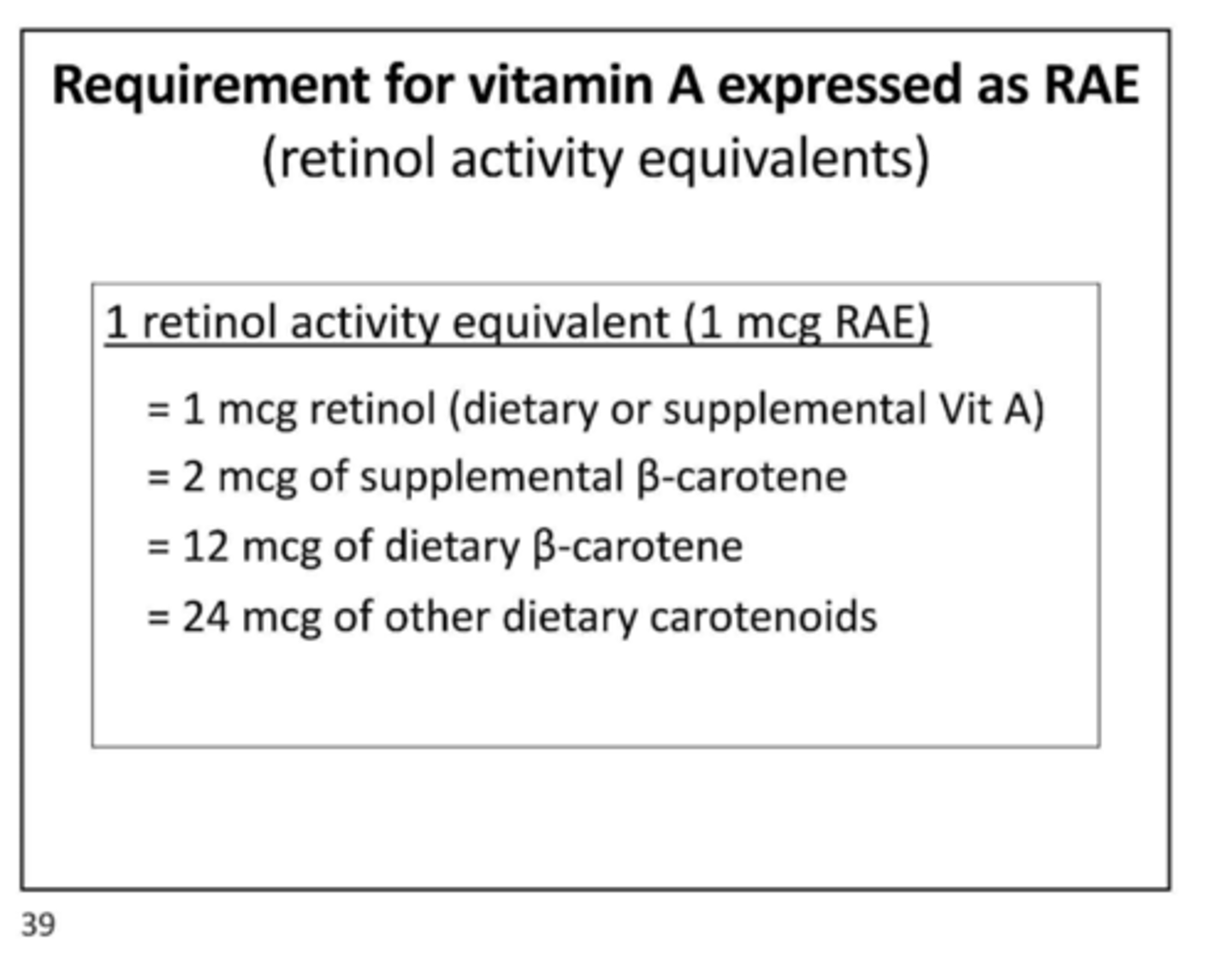
What are the different forms of vitamin A?
1. Preformed Vitamin A: retinol from supplements and diet
2. Provitamin A: carotenoids are precursors of retinol that you get from the diet and supplements
More dietary provitamin A has to be consumed to provide the same amount of retinol as dietary preformed vitamin A.
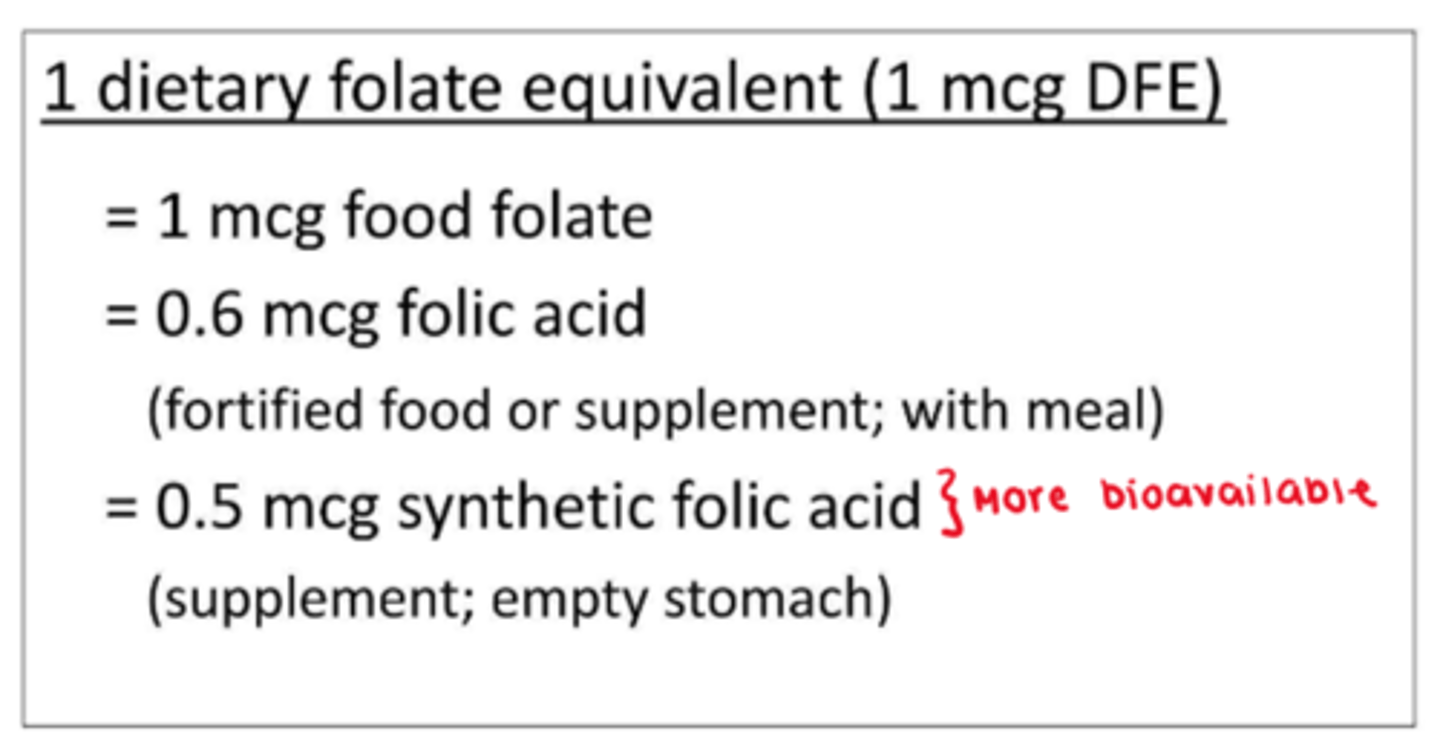
What is the requirement for folate expressed as DFE (dietary folate equivalents)?
There is a 50% decrease in bioavailability of food folate compared with that of synthetic folic acid in fortified foods/supplements.
The level of other nutrients in the diet can affect the balance of one nutrient.
For example, take nitrogen balance. Even if you control for protein intake, you cannot accurately measure nitrogen balance without considering total kcal intake.
For men, as kcal intake decreases, men have a negative nitrogen balance. As kcal intake increases, nitrogen balance reaches a positive value.
Need to consider bioavailability, absorption, and general metabolism.
What are the current dietary standards?
Dietary Reference Intakes (DRIs)
- Estimated Average Requirements (EAR)
- Recommended Dietary Allowance (RDA)
- Adequate Intake (AI)
- Tolerable upper Intake Level (UL)
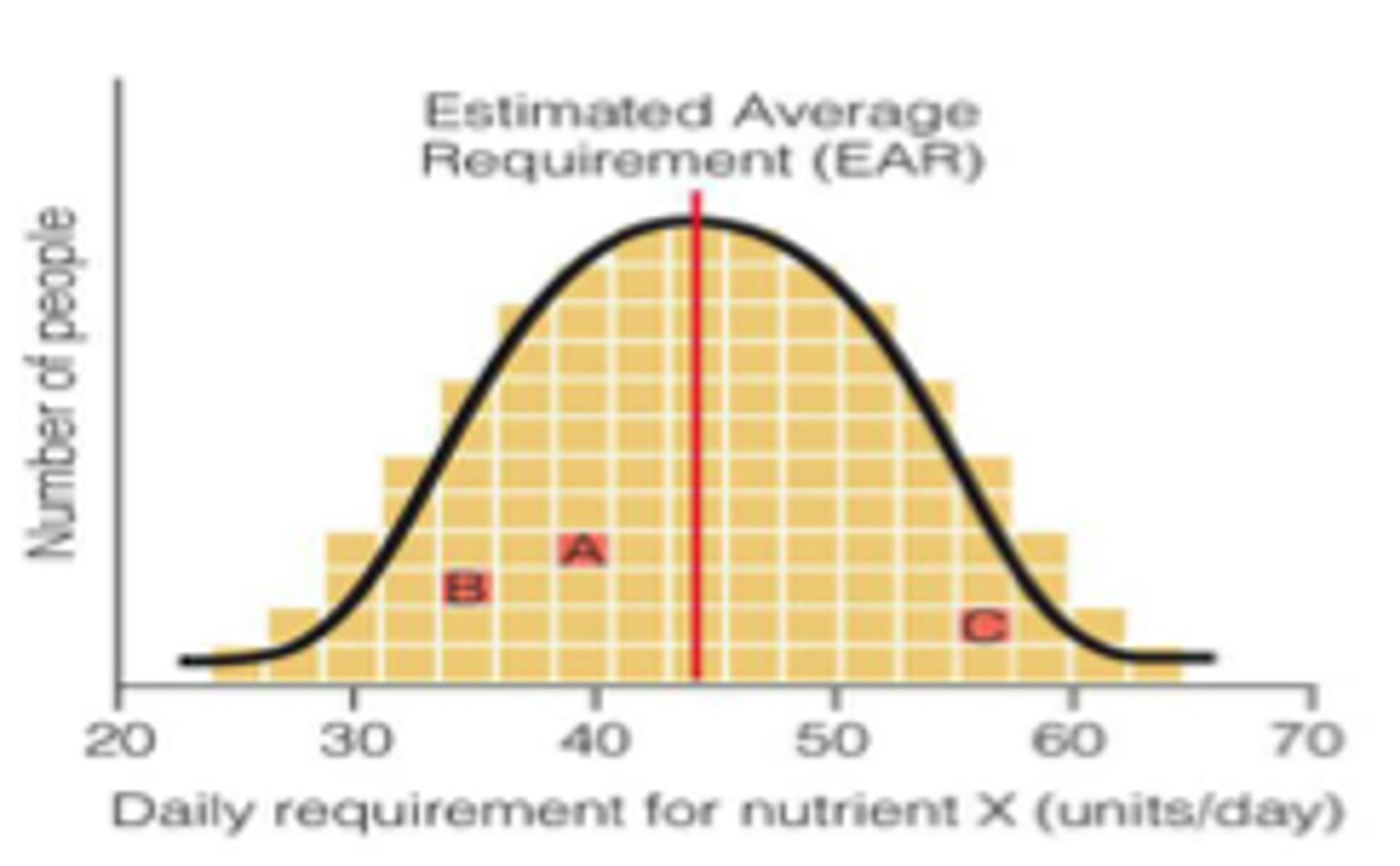
What is the estimated average requirement (EAR)?
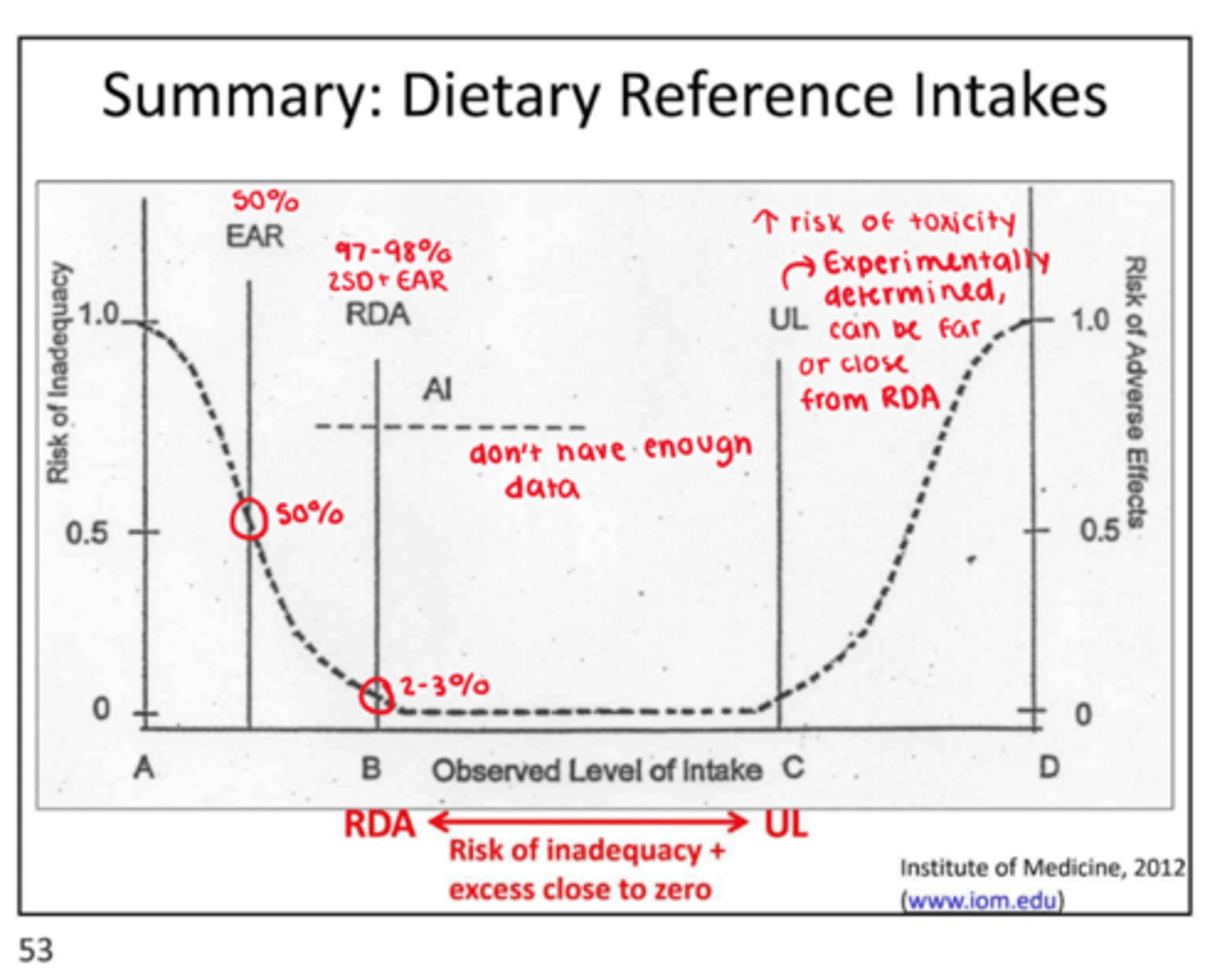
The EAR is the daily intake value estimated to meet the requirement, as defined by a specific adequacy indicator, in 50% of healthy individuals in a life stage or gender group.
It is not a recommended intake, not great for half the population.
What is the EAR used for?
Used in assessing the prevalence of nutrient inadequacy in groups + basis for the RDA
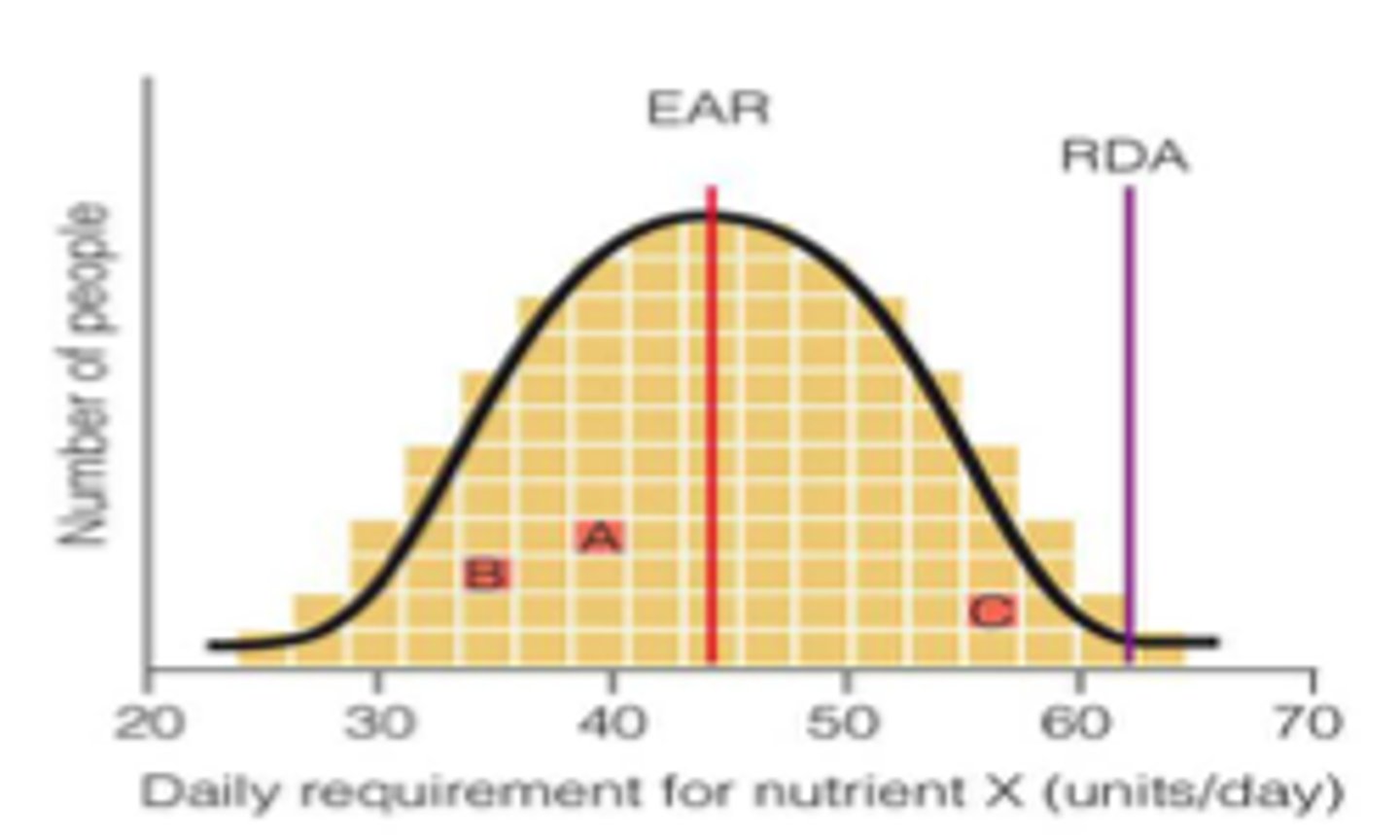
What is the Recommended Dietary Allowance (RDA)?
RDA = EAR + 2SD(EAR)
RDA is the average daily dietary intake level sufficient to meet the requirements of nearly all (97-98%) individuals in a life stage or gender group. Used as a goal for usual daily intake by individuals.
Define Adequate Intake (AI).
When there is insufficient data to establish the EAR and RDA, an adequate intake is set. It is a value based on experimental or observed estimates of the average nutrient intake that appears to maintain a defined nutriture in a group of healthy people.
The goal for people when RDA is unavailable... It should be higher than the RDA!
Arsenic, boron, nickel, silicon, and vanadium have AIs!
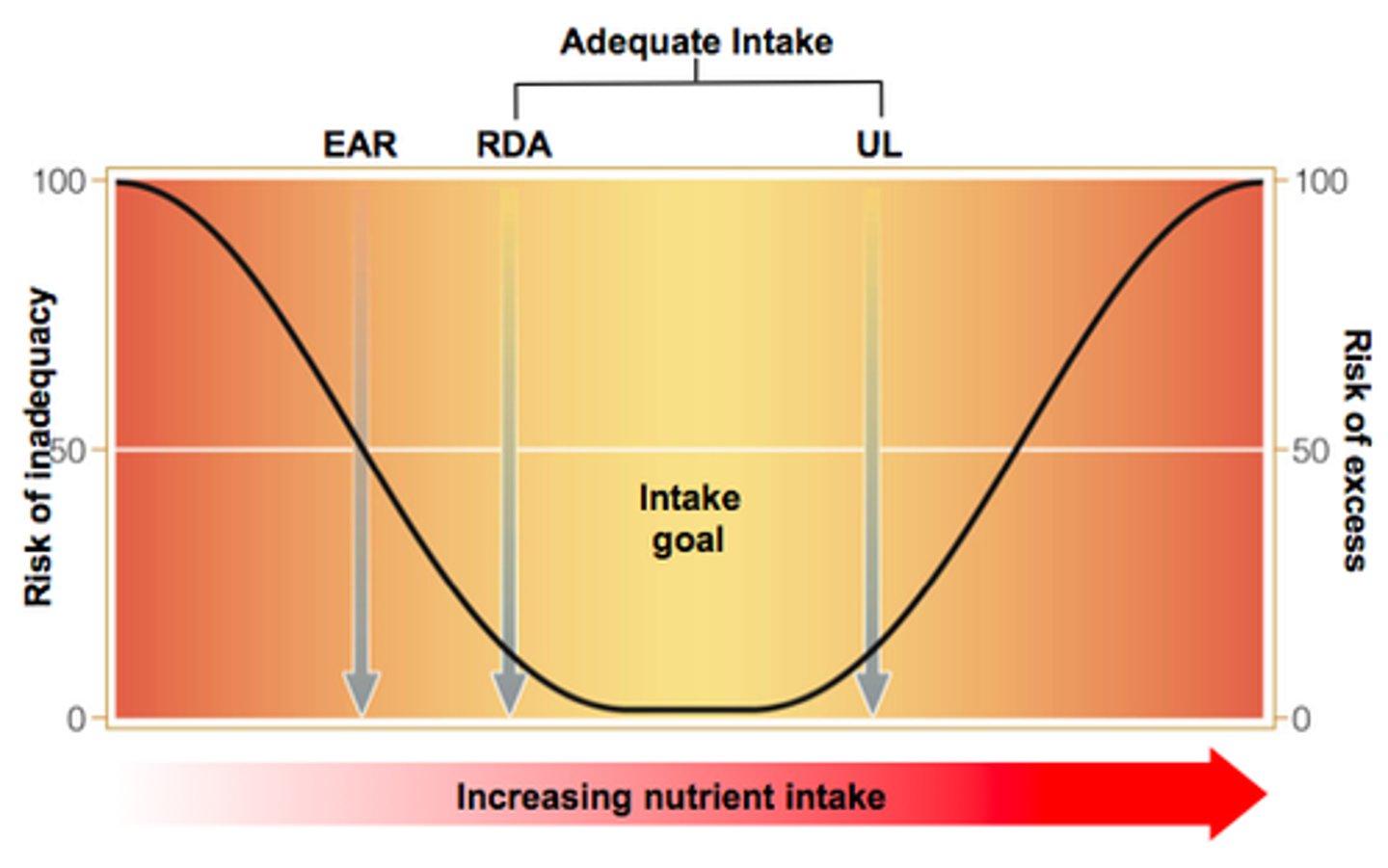
What is a tolerable upper intake level (UL)?
The UL is the maximal level of chronic daily intake unlikely to pose adverse health risks to almost all in a life stage or gender group. Chronic daily intake!
It does not apply to individuals being treated for deficiency; therapeutic doses often exceed the UL. Many nutrient's DRIs for infants will say "ND" - lack of experimental research in infants.
Can toxicity occur with foods, supplements, or both?
The UL is based on total intake from all sources of a nutrient.
The exceptions are the vitamin niacin; the mineral magnesium, zinc, and nickel. The UL only refers to non-food sources.
What is the summary image of the DRIs?
The DRIs also include the Estimated Energy Requirement (EER), what is this?
The EER is the average dietary energy intake predicted to maintain energy balance. It is based on defined age, sex, weight, height, + PA level. Used to estimate individual needs and plan appropriate energy intakes.
The DRIs also mention the Acceptable Macronutrient Distribution Range (AMDR). What is this?
The AMDR is the range of intakes for energy-yielding macronutrients with a reduced risk of chronic disease. These macronutrients include CHO, fat, protein, and n-3/6 FAs). Used as a goal for individuals and groups.
What are Daily Values (DVs)?
They are a set of nutrient standards used on nutrition facts panels developed by the FDA.
They are based on Reference Daily Intakes (RDIs) that are set for most vitamins/minerals (except Na and K) and set at the highest value required for any life stage group.
They are also based on Daily Reference Values (DRVs) that are set for energy-producing nutrients, cholesterol, Na, and K. Based on a daily caloric intake of 2000 calories.
RDI and DRV don't appear on food labels, the DV represents the combination of both.