Muscular Strength & Endurance Testing & Rx: Clinical Scenarios
1/11
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
12 Terms
top 10 chronic conditions for adults 65+ + what others can you think of
*lot of CV
*80% of at least 1 chronic condition; 68% of 2 or more
-Neuro control issues: ex: Parkinson’s; could use stationary machines
-Autoimmune diseases: RT impact on immune system, but prob worse w/ aerobic
-Cancer: bone mineral density, osteoperosis
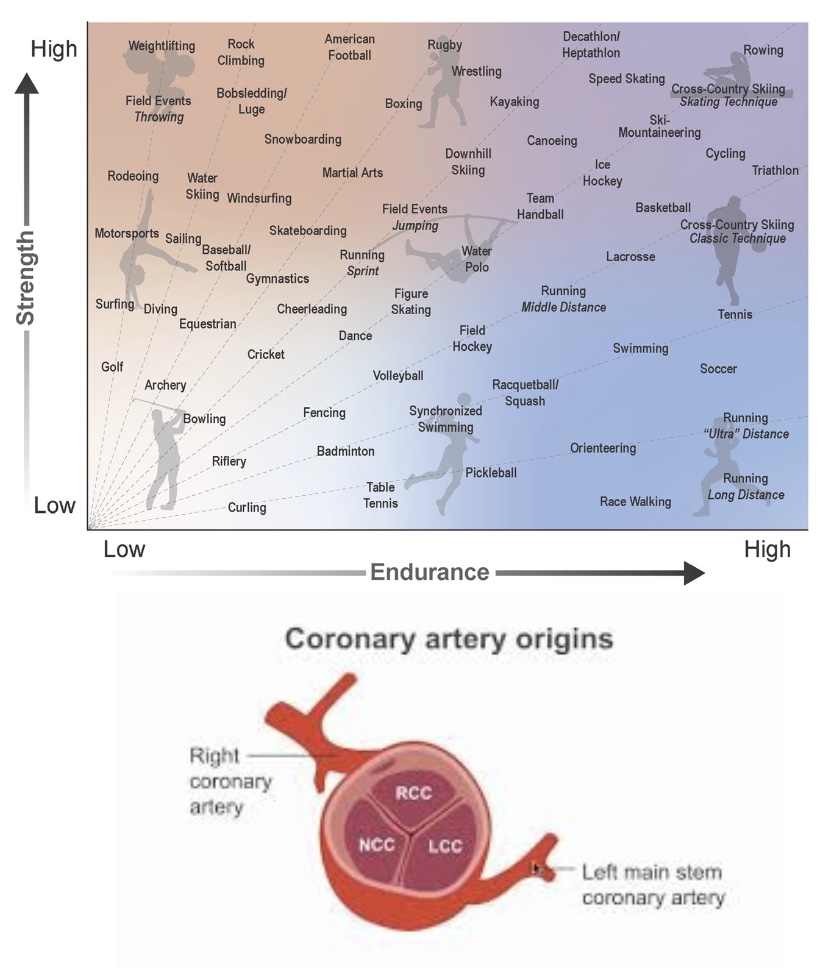
Cardiovascular Disease
-RT is effective; but don’t do 1RM or isometric (valsulva/high pressure; so do 5-10RM to assess)
-Coronary artery disease, heart failure, hypertension, hypercholestermia, valve disease (atherosclerosis)
Is strength assessment and training safe or appropriate?
-CAD and Heart Failure: used to say don’t push; now know RT increases P but decreases HR, so really effective bc CA get lots of blood; little risk if done right (higher reps and low volume)
*CA: off aortic valve, higher HR=more systole and less filling of CA → heart attack (fill cusps when relaxes/dystole)
-Hypertension: RT helps control or lower BP
-Hypercholesteremia: no great data for RT, know RT increases muscle mass=increase metabolic activity; aerobic better to lower LDL
-Heart Valve Disease: RT distorts valves quicker, so not good
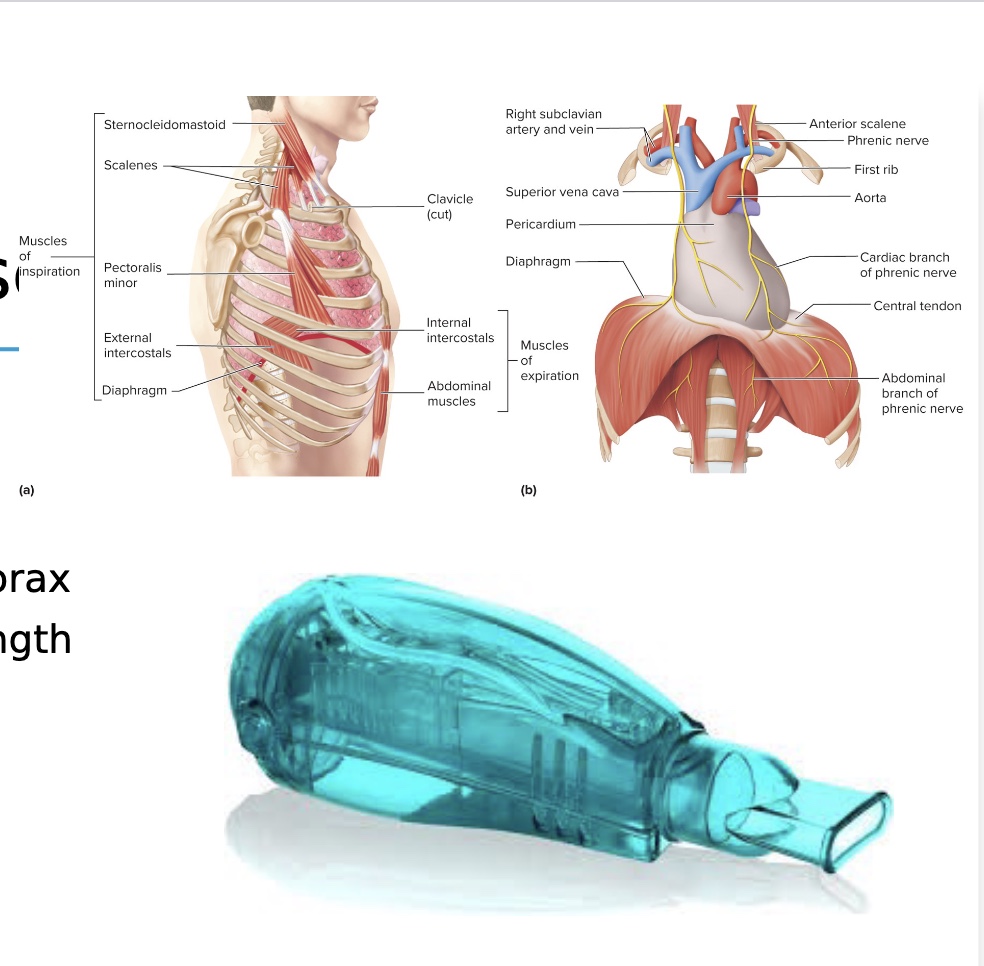
Pulmonary Disease
-COPD, asthma, CF, Pneumothorax
*maybe 1RM, yes, maybe, definitely not
Is strength assessment and training safe or appropriate?
-yes they can
-could test w/ spirometry
-Respiratory muscle training
Mean Inspiratory and Expiratory Pressure: activate accessory muscle and more diaphragm; suck in or blow out as much as can
Acapale Devise: sets resistance(also incentive spirometer where ball goes up)
*valsulva could crease spontaneous pneumothorax (small risk)
Hypertension/Valve Disease
*HT could be bc of valve disease?
-long-debated topic
-upper body RT: no benefit BP; lower body RT: mild decrease BP
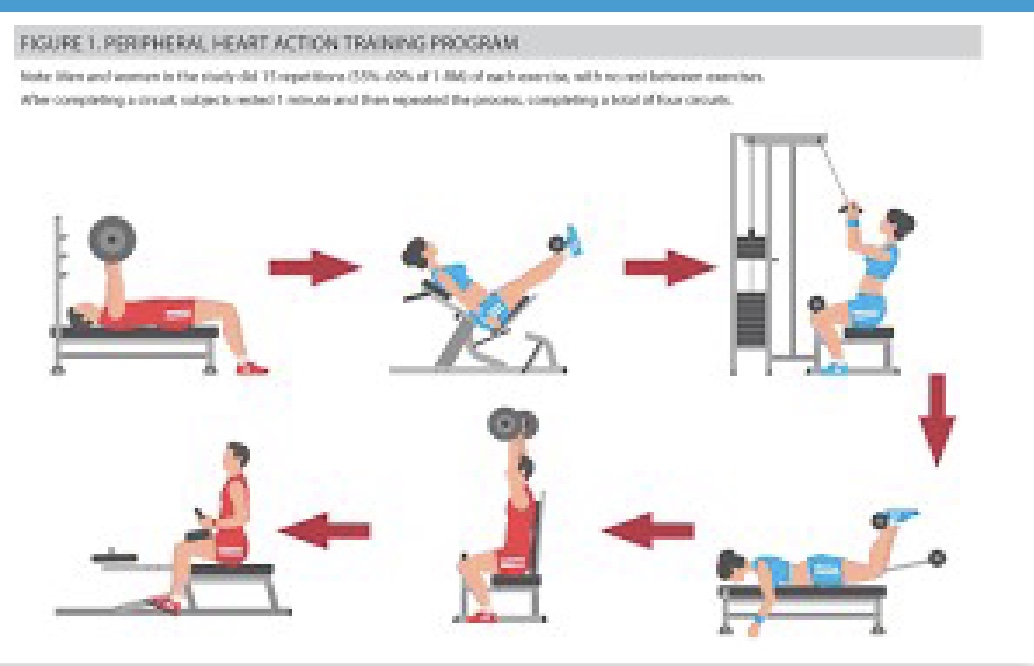
Hypertension
-Peripheral Heart Training: similar to high intensity; alternate UB and LB exercises so confused body and make it good at fine tuning VD/VC; use relatively large muscle groups
Valve Disease
-make sure it’s resolved before do RT
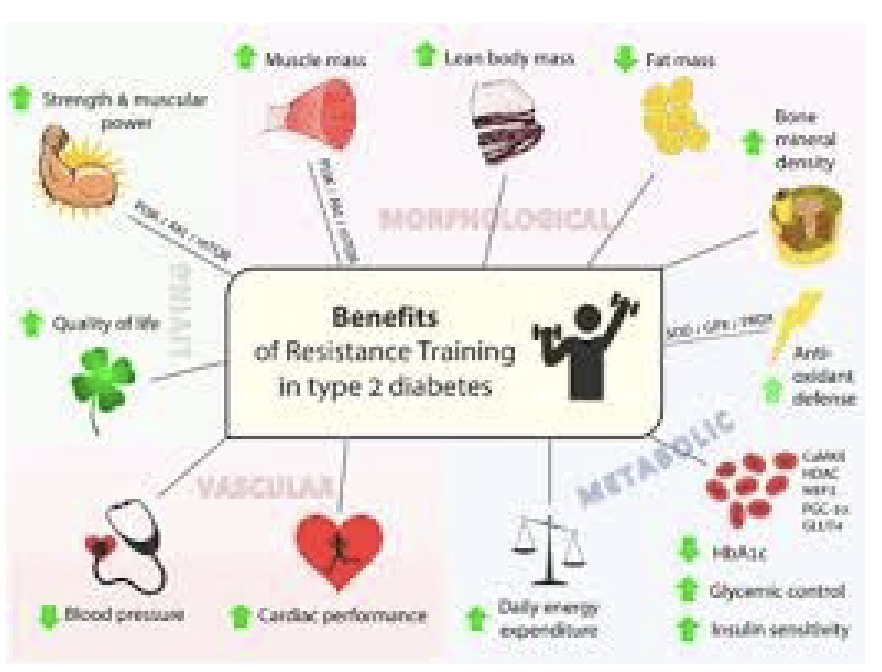
Diabetes
-Type I and Type II
-RT benefits in Type II: all increase glucose sensitivity and insulin control
-Ask: is there kidney disease present? peripheral neuropathy (lack of sensation)?
-Aerobic all good, but RT increases muscle mass so better glucose control
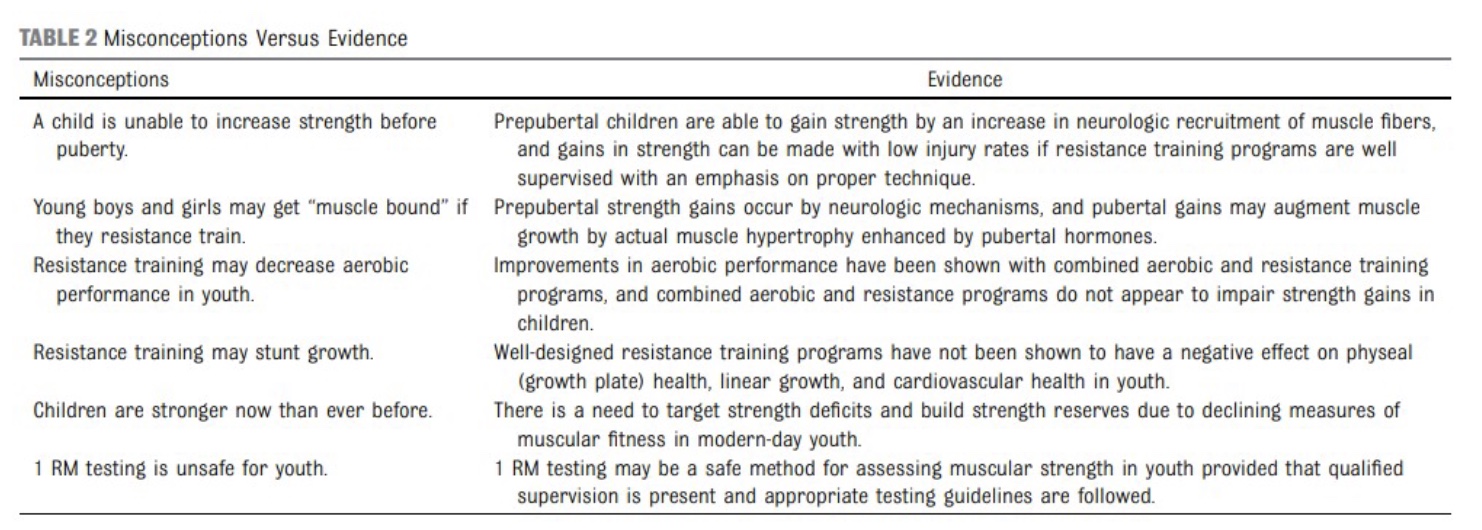
Children and RT: American Academy of Pediatrics
-big debate!
*prepubertal: can do weights but be careful
*rare will get a ton of muscle hypertrophy
*higher muscle mass=higher overall performance
*rare; if inappropriate
*understand more now, but not necessarily stronger; more accessible diets
*Mike: but what gain?
What did Michael teach you?
-FMS
-1,3,5, and 10 RM
-Sit-up, push-up, YMCA bench test
Non-Traditional Strength Assessments: List
-Manual Muscle testing
-Handheld dynamometry
-30 second Sit to Stand
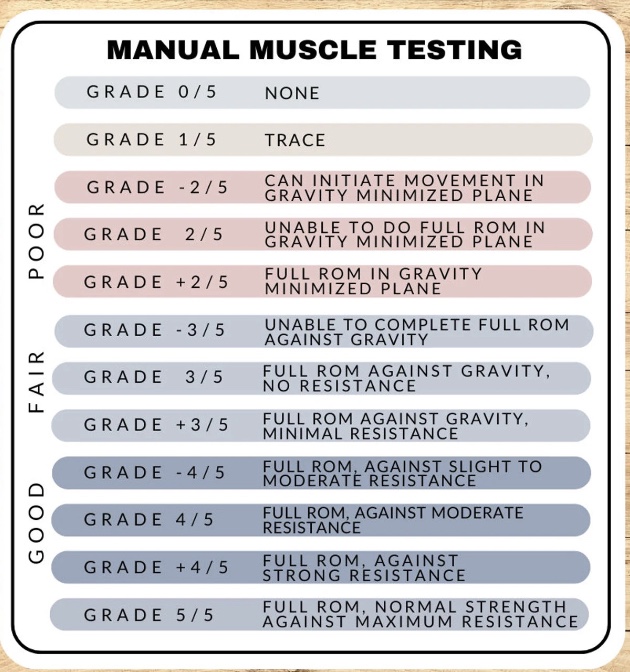
Manual Muscle Testing
-push against patient
-Benefits: clinical populations, an option
-Limitations: very subjective, different ratings between practitioners; lot of athletes=5
Hand Held Dynamometry
-Quantify (get #’s) manual muscle testing (go hand in hand; get more data)
-F in lb
-like a bathroom scale; hand held; hold against wall/stationary structure; can do many movements; do 6 sec effort; can also do balance
-can see peak and fatigue curve; tracking lines while dong could add some neuromuscular trainging
-can Rx off of/give an exercise Rx based off results

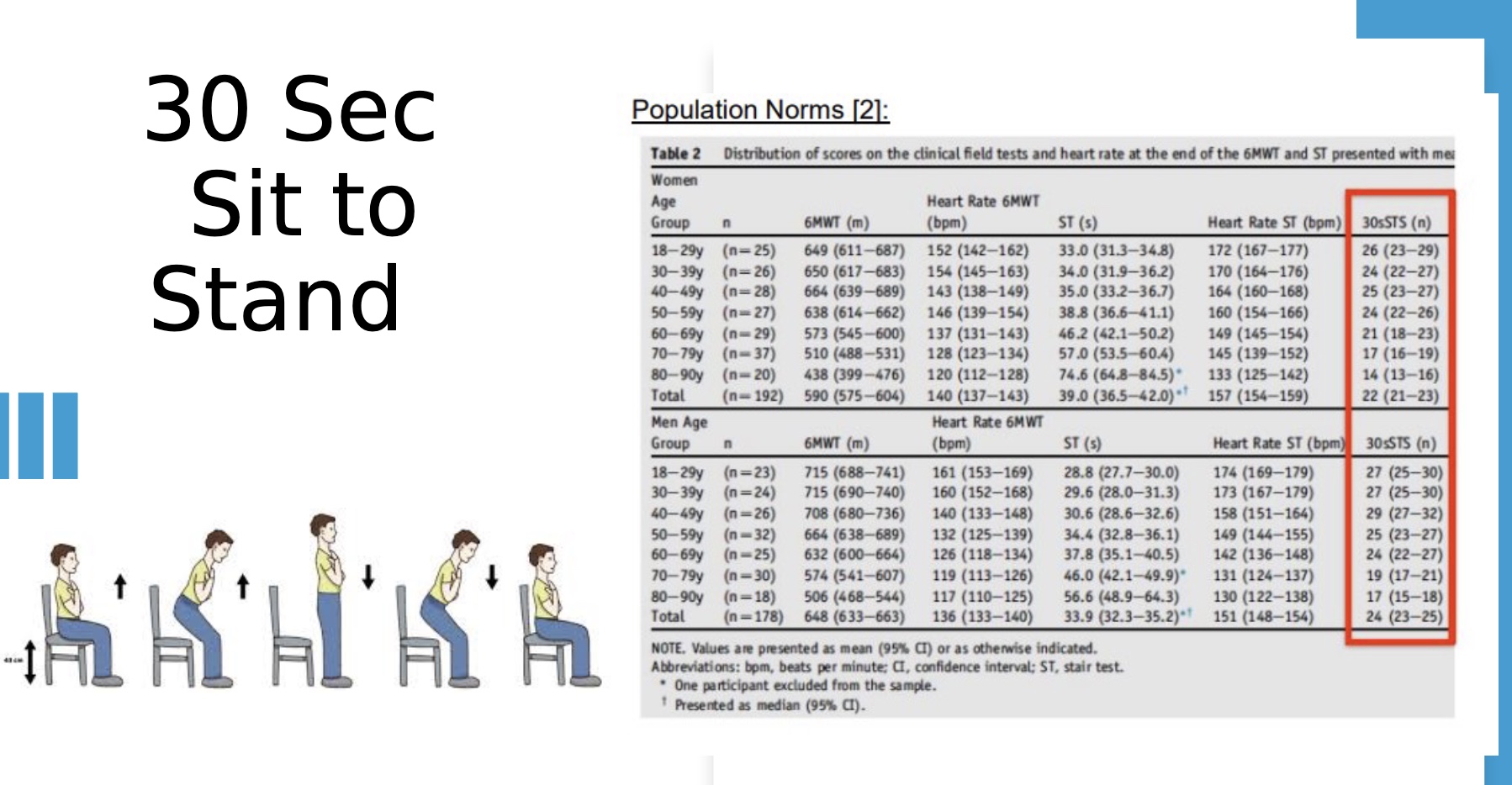
30 Second Sit to Stand
-age groups (for people are age=26/27)
-when can’t do it is when you get the greatest info (ex: if poor LB strength; older person might not be able to even get out of the chair)
who absolute should NOT do RT?
-post stroke
-risk of an annarhrism (=bubbling vessel, could bleed out; in eye, BV, etc.; pressure sensitive)
-aortic stenosis/any sever valve disease
-phenumothorax/sever lung disease
-injury prohibits a safe form
-HD: severe heart failure
-cancer: can do, but don’t decrease BMD
-osteoporosis/penia: be careful; if in spine don’t do back squats, etc.