GW BGZ 2025 Practical - Indirect calorimetry/CPET
1/10
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
11 Terms
What is VO₂max and why is it important?
VO₂max (maximal oxygen consumption) is the greatest amount of oxygen a person can take up, transport, and use during maximal exercise. It is also called aerobic power, maximal aerobic capacity, cardiorespiratory fitness, or aerobic fitness.
VO₂max reflects the integrated ability of:
The lungs to take in oxygen.
The heart and blood vessels to transport oxygen.
The blood to carry oxygen.
The skeletal muscles to extract and use oxygen for aerobic ATP production.
Because aerobic metabolism depends on oxygen availability, VO₂max provides a quantitative measure of the body's maximum capacity for aerobic ATP resynthesis.
It is considered the best single measure of aerobic fitness and the most useful indicator of the functional capacity of the oxygen transport system.
VO₂max can be expressed as:
L/min (absolute VO₂max)
mL/kg/min (relative VO₂max, allowing comparison between individuals of different body sizes)
What determines VO₂max? Explain the Fick equation.
The physiological determinants of VO₂max are described by the Fick equation:
VO2=Q×(a−vO2 difference)
where:
VO₂ = oxygen consumption
Q = cardiac output
a-vO₂ difference = arteriovenous oxygen difference
Cardiac output itself is determined by:
Q=HR×SVQ =
where:
HR = heart rate
SV = stroke volume
Therefore, VO₂max depends on:
Central factors (oxygen delivery)
Maximal heart rate
Maximal stroke volume
Maximal cardiac output
Peripheral factors (oxygen utilization)
Muscle blood flow
Capillary density
Mitochondrial content
Ability of muscles to extract oxygen (a-vO₂ difference)
A high VO₂max requires both efficient oxygen delivery and efficient oxygen extraction/utilization.
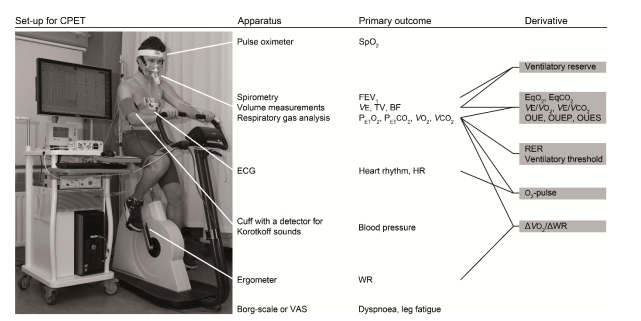
How is VO₂max measured and what is CPET?
VO₂max is usually measured during a cardiopulmonary exercise test (CPET) using indirect calorimetry.
During a CPET:
The subject exercises on a treadmill or cycle ergometer.
Exercise intensity progressively increases until voluntary exhaustion.
Respiratory gases are continuously analyzed.
Variables measured include:
VO₂ (oxygen uptake)
VCO₂ (carbon dioxide production)
VE (minute ventilation)
Heart rate
RER (respiratory exchange ratio = VCO₂/VO₂)
The ideal test duration is approximately 8–15 minutes.
If the test is too short:
Anaerobic contribution becomes too large.
If the test is too long:
Fatigue may occur before maximal physiological capacity is reached.
The purpose of CPET is to determine:
VO₂max/VO₂peak
Ventilatory threshold (VT1)
Respiratory compensation point (VT2)
Overall cardiorespiratory fitness
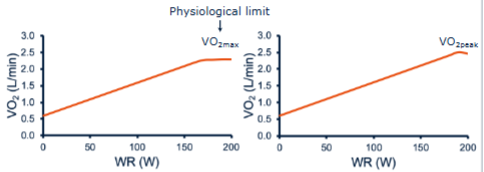
What is the difference between VO₂max and VO₂peak?
VO₂max and VO₂peak are often used interchangeably but are not identical.
VO₂max
VO₂max is achieved when oxygen uptake reaches a plateau despite increasing exercise intensity.
In other words, workload increases but VO₂ no longer increases significantly.
This indicates that the body's maximum aerobic capacity has been reached.
VO₂peak
VO₂peak is simply the highest VO₂ value measured during the test.
It is used when a clear VO₂ plateau is not observed.
Because many people stop due to fatigue before a plateau occurs, VO₂peak is often reported in practice.
To determine whether VO₂peak likely represents a maximal effort, additional criteria are used:
Objective criteria
HR ≥ 85–95% of predicted HRmax
RER ≥ 1.10
Subjective criteria
Severe fatigue
Heavy sweating
Unsteady cycling/running
Strong unwillingness to continue
Borg score ≥17
Therefore:
VO₂max = physiological maximum confirmed
VO₂peak = highest measured value, may or may not equal true VO₂max
Which factors influence VO₂max?
Several factors affect VO₂max:
Genetics
Approximately 25–50% of VO₂max is genetically determined.
Sex
Men generally have VO₂max values 15–20% higher than women due to:
Larger heart size
Greater muscle mass
Higher hemoglobin concentrations
Age
VO₂max is typically highest around age 20.
After approximately age 30, it declines by about 8% per decade, although training can reduce this decline.
Training status
Endurance training can improve VO₂max by approximately 6–25%.
Adaptations include:
Increased stroke volume
Greater capillary density
Increased mitochondrial content
Improved oxygen extraction
Exercise mode
VO₂max depends on how much muscle mass is involved.
Generally:
Running > cycling > arm exercise
because larger active muscle mass increases oxygen demand.
What is the ventilatory anaerobic threshold (VT1)?
The ventilatory anaerobic threshold (VT1) is the point during progressive exercise where anaerobic glycolysis begins to contribute significantly to energy production.
It is defined as: The highest VO₂ that can be achieved without a sustained excessive increase in ventilation relative to oxygen uptake.
At VT1:
Oxygen delivery becomes insufficient to meet all energy demands aerobically.
Anaerobic glycolysis increases.
Lactate production rises.
Hydrogen ions (H⁺) increase.
Bicarbonate buffers these H⁺ ions.
Buffering reaction:
HCO3− + H+ ↔ H2CO3 ↔ H2O+CO2
This buffering generates additional CO₂.
The increased CO₂ stimulates ventilation, causing:
Increased VE
Increased VCO₂
Rising RER
VT1 is important because it represents the highest sustainable exercise intensity without significant lactate accumulation.
For endurance athletes, VT1 is often a stronger predictor of performance than VO₂max alone.
What is the respiratory compensation point (VT2)?
The respiratory compensation point (VT2) occurs at a higher intensity than VT1 and represents the point where lactate accumulation becomes so large that buffering mechanisms can no longer fully compensate.
At VT2:
Lactate production increases rapidly.
Hydrogen ions accumulate.
Blood pH begins to fall (metabolic acidosis).
Chemoreceptors detect the fall in pH.
Hyperventilation occurs to reduce acidity.
This causes:
A disproportionate rise in VE
Excessive increase in VCO₂
Loss of the linear relationship between ventilation and carbon dioxide production
VT2 therefore marks the onset of significant metabolic acidosis and indicates that exercise can only be maintained for a relatively short period.
It is a near-maximal marker and is extremely useful for prescribing high-intensity endurance training.
Compare VO₂max, VT1, and VT2.
VO₂max
Maximal aerobic capacity.
Highest rate of oxygen consumption possible.
Requires maximal effort.
Reflects the overall capacity of the oxygen transport system.
VT1 (First Ventilatory Threshold)
Submaximal marker.
Beginning of substantial anaerobic glycolysis.
First sustained rise in lactate.
Increased ventilation due to bicarbonate buffering.
Represents the highest intensity that can be maintained largely aerobically.
VT2 (Respiratory Compensation Point)
Near-maximal marker.
Rapid lactate accumulation.
Metabolic acidosis develops.
Hyperventilation occurs.
Represents the upper limit of sustainable endurance exercise.
Relationship during increasing exercise intensity
Rest → Aerobic exercise → VT1 → Mixed aerobic/anaerobic metabolism → VT2 → Metabolic acidosis → VO₂max → Exhaustion
A useful way to remember them:
VO₂max = ceiling of aerobic capacity
VT1 = first major lactate threshold
VT2 = point where acidosis forces hyperventilation
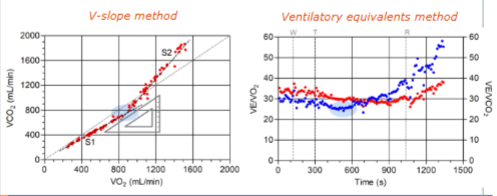
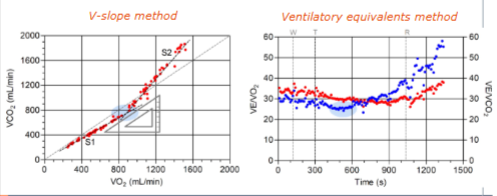
What is the V-slope method?
Principle
As exercise intensity increases:
VO₂ increases steadily.
VCO₂ initially increases proportionally with VO₂.
Once lactate begins accumulating, bicarbonate buffers H⁺ ions.
This buffering produces extra CO₂.
VCO₂ starts increasing faster than VO₂.
The V-slope method identifies the point where this change occurs.
Graph
Plot:
VO₂ on the x-axis
VCO₂ on the y-axis
Before VT1:
Relationship is approximately linear.
Slope ≈ 1.
After VT1:
VCO₂ rises disproportionately.
Slope becomes steeper.
How VT1 is determined
VT1 is the breakpoint where the VCO₂-VO₂ relationship changes slope.
Why it works
The extra CO₂ produced by bicarbonate buffering of lactate causes VCO₂ to rise faster than VO₂.
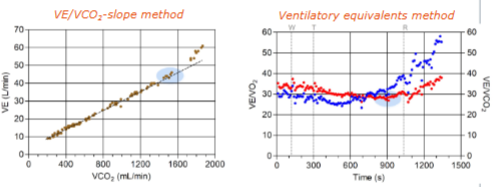
What is the ventilatory equivalents method?
Principle
The ventilatory equivalent tells us how much ventilation is required per liter of gas exchanged.
Two ratios are examined:
VE/VO₂
VE/VCO₂
Before VT1
Ventilation increases proportionally with oxygen uptake.
Therefore:
VE/VO₂ decreases or remains stable.
VE/VCO₂ remains stable.
At VT1
Additional CO₂ is produced from lactate buffering.
Ventilation increases to remove this CO₂.
Result:
VE/VO₂ begins to rise.
VE/VCO₂ remains stable.
Graph
Plot:
VE/VO₂
VE/VCO₂
against time or workload.
How VT1 is determined
VT1 is the point where:
VE/VO₂ starts increasing
while VE/VCO₂ remains unchanged
Why it works
The body must ventilate more to remove excess CO₂ generated by lactate buffering, but CO₂ elimination is still efficient, so VE/VCO₂ has not increased yet.
What is the VE-VCO2 method?
Principle
This method is more commonly used for identifying the Respiratory Compensation Point (VT2), although it can contribute to threshold analysis.
It examines the relationship between:
VE (minute ventilation)
VCO₂ (carbon dioxide production)
Before VT2
Ventilation and CO₂ production rise almost linearly.
After VT2
Metabolic acidosis develops.
The body begins hyperventilating to reduce acidity.
Ventilation now rises faster than VCO₂.
How VT2 is determined
VT2 is identified as the point where:
The VE–VCO₂ relationship loses linearity.
VE increases disproportionately relative to VCO₂.
Why it works
At VT2, lactate buffering is no longer sufficient. Blood pH falls, stimulating hyperventilation, causing VE to rise excessively.