MSK LEC_ SHOULDER
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
70 Terms
is a multiaxial, ball-and-socket, synovial joint that depends primarily on the muscles and ligaments rather than bones for its support, stability, and integrity (3 DOF)
_____ is a ring of fibrocartilage, surrounds and deepens the glenoid cavity of the scapula about 50% ( Only part of the humeral head is in contact with the glenoid at any one time.
What is the RP and CPP of this joint? What is its Capsular Pattern?
GH joint
Labrum
55° abduction, 30° Horizontal adduction ; CPP: Full ABER
ERabIR
The glenoid in the resting position has a 5° superior tilt or inclination and a 7° retrover- sion (slight medial rotation). The angle between the humeral neck and shaft is about _____, and the humeral head is retroverted 30° to 40° relative to the line joining the epicondyle
130°
The rotator cuff controls osteokinematic and arthrokinematic motion of the humeral head in the glenoid and along with the biceps depresses the humeral head during movements into elevation.
Ligaments of GH joint:
_______ - limits inferior translation in adduction. It also restrains anterior translation and ER up to 45° abduction.
______ - limits ER between 45° and 90° abduction.
______ - The most important ligament. It supports the humeral head above 90° abduction, limiting inferior translation while the _______ band tightens on ER and the posterior band tightens on ______
SGHL
MGHL
IGHL - anterior band , medial rotation
Excessive lateral rotation, as seen in throwing, may lead to stretching of the anterior portion of the ligament (and capsule), thereby increasing glenohumeral laxity.
Ligaments of GH joint:
______ - limits inferior translation and helps limit lateral rotation below 60° abduction.This ligament is found in the rotator interval between the anterior border of the supraspinatus tendon and the superior border of the subscapularis tendon, thus the ligament unites the two tendons anteriorly.
The rotator interval consists of ___________
Injury to these structures can lead to contractures, _______ instability, and _______ instability
CHL
CHL, SGHL, GH joint capsule & tendons of subscapularis & supraspinatus
biceps tendon & anterior glenohumeral
The _______ ligament forms an arch over the humeral head, acting as a block to superior translation.
______ ligaments holds the long head of biceps tendon within the groove.
GH JOINT: Branches of the posterior cord of the brachial plexus and the suprascapular, axillary, and lateral pectoral nerves innervate the joint.
coraco-acromial
Transverse humeral Ligament
______ - is a plane synovial joint that augments the ROM of the humerus in the glenoid (3 DOF). This joint depends on ligaments for its strength. The ______ ligaments surround the joint and control horizontal motion of the clavicle. ( 1ST LIGAMENT INJURED when stressed)This joint is innervated by branches of the suprascapular and lateral pectoral nerve.
Types:
1:
2:
3:
4:
About 70% of _______ are associated with a hooked acromion.
The________ ligament is the primary support of the AC joint.
AC joint → acromioclavicular ligament
flat → curved → hooked → convex (uptured)
rotator cuff tears
coracoclavicular ligament
AC JOINT : Coracoclavicular ligament
2 portions: _______ & _____ control the vertical motion of the clavicle.
If a ______ occurs, this ligament has been torn
CPP:
RP:
Capsular Pattern:
Conoid & Trapezoid
step deformity
90° Abduction, Arm resting at side , Pain at Extreme Rom in Full elevation & Horizontal adduction
The _________ joint, along with the AC joint, enables the humerus in the glenoid to move through a full 180° of abduction ( saddle shape w/ 3 DOF). It joins the appendicular skeleton to the axial skeleton.
_____ & _______ , which support the joint anteriorly and posteriorly
________ the main ligament maintaining the integrity of the SC joint
RP:
CPP:
Capsular Pattern:
SC joint ( medial end of clavicle, manubrium sternum & cartilage of 1st rib; also depends on ligaments for it strength)
Ant & Post ligaments
Interclavicular & costoclavicular ligament ( rhomboid ligament)
Arm resting by side in normal physiologic position
Full elevation & protraction
Pain at extremes ROM in horizontal adduction & full elevation
_________ It consists of the body of the scapula and the muscles covering the posterior chest wall and must be considered in any assessment because a stable scapula enables the rest of the shoulder to function correctly.
T or F: When assessing the shoulder, it is important to look not only the shoulder but also the whole kinetic chain ( linkage of multiple segments of the body that allows transfer of forces and motion starting at the feet)
Scapulothoracic joint ( No CPP & Capsular pattern)
True
Rotator Cuff Lesions
Hx:
O:
Active movement:
Passive movement:
MMT:
Special Test:
Sensory Function:
Palpation:
Diagnostic Imaging:
30 to 50 years, Pain and weakness after
eccentric load
Normal bone & soft tissue outlines, protective shoulder hike may be seen
Weakness of EXABIR (any) , crepitus may be present
Pain if impingement occurs
Pain & weakness on ABER
Drop Arm & Empty can test +
Not affected
Tenderness over rotator cuff
MRI & Xray: acromial spurring, upward displacement of humeral head
Frozen Shoulder
Hx:
O:
Active movement:
Passive movement:
MMT:
Special Test:
Sensory Function:
Palpation:
Diagnostic Imaging:
45+ ( insidious), after trauma or surgery, restricts EXABIR
Normal bone and soft tissue outlines
Restricted ROM & Shoulder hiking
Limited ROM in EXABIR
Normal when arm by side
None
Not affected
Not painful unless capsule is stretched
X ray : (-) , Arthrography: DEC capsular size
Atraumatic Instability
Hx:
O:
Active movement:
Passive movement:
MMT:
Special Test:
Sensory Function:
Palpation:
Diagnostic Imaging:
10-35, pain and instability c activity, No hx of trauma
Normal bone and soft tissue outlines
Full of excessive ROM
Normal or Excessive ROM
Normal
Apprehension, Relocation & Augmentation test: (+); Load & shift test : (-)
Not affected
Ant or Post pain
(-)
Cervical Spondylosis
Hx:
O:
Active movement:
Passive movement:
MMT:
Special Test:
Sensory Function:
Palpation:
Diagnostic Imaging:
50+ years ( acute/chronic)
Torticollis may be present, Minimal or no cervical spine movement
Limited ROM c pain
Limited ROM ( symptoms may be exacerbated)
Normal unless nerve root compressed = myotome
Spurling, Distraction, ULNT & Shoulder abduction test : (+)
Dermatomes & reflexes affected
Tender over appropriated vertebra or facet
X - ray : narrow osteophytes
Patient History
A fall on out-stretched hand (FOOSH), which could indicate a _________
A blow to the tip of the shoulder, or land on the elbow, driving the humerus up against the acromion may indicate an ___________
T or F: Patients with instability may appear normal on clinical examination, especially if shoulder muscles are not fatigued.
Persons who had recurrent dislocations/instability of the shoulder may find that any movement involving______ bothers them, because this movement is involved in anterior dislocations of the shoulder.
fracture or dislocation of shoulder
acromioclavicular dislocation or subluxation.
True
ER
Patient History
Long head of biceps pathology causes pain that moves ____________
Excessive ________ may lead to dead-arm syndrome - sudden paralyzing pain and weak- ness in the shoulder.
This finding often indicates altered shoulder mechanics commonly involving a tight posterior capsule, altered arthrokinematics of the glenohumeral joint, and scapular dyskinesia. In throwers, the condition may be referred to as a ______
If the patient complains of pain during specific phases of pitching (for example, during the late cocking and acceleration phases),______ should be considered even in the presence of minimal clinical signs.
ER & IR of the shoulder
ABIR
“SICK” scapula
anterior instability
SICK Scapula is?
Malpositioned Scapula
Inferior medial border of scapula prominence
Coracoid pain & malposition
Scapular dysKinesia
Cause of Primary Impingement Syndrome
Inflammation in subacromial space
Rotator cuff tendon degeneration
Osteophytes under AC joint
Hooked acromion
Glenohumeral joint hypermobility
impingement or pinching is the primary cause of the pain
>40 , degenerative
Cause of Secondary Impingement Syndrome
Abnormal glenohumeral arthrokinematics
Abnormal scapulothoracic arthrokinematics
“Slouched” posture
Muscle weakness or fatigue
Muscle hypomobility
Capsule tightness especially posterior
implies that although impingement signs are present, they result from a primary problem somewhere else, commonly in the scapular or humeral control or stabilizer muscles.
15-35 yrs old
scapula dyskinesia & altered muscle dynamics
Impingement
_______ In the older patients, this impingement occurs due to degenerative changes to the rotator cuff, acromion & coracoid process, anterior tissues from stress overload
______ In 15-35 y/o , anterior shoulder pain is primarily caused by muscle imbalances and abnormal movement patterns
______ a type of impingement found posteriorly mostly in overhead athletes and involves contact of rotator cuff ( Supra & Infra) with the posterosuperior glenoid labrum when arm is abducted to 90° and ER fully.
Primary Impingement
occur anteriorly
Secondary Impingement
presents instability of scapula or GH joint
occur anteriorly
Internal/Non-outlet impingement
occur posteriorly
T or F: Stability of the shoulder depends on both dynamic stabilizers (the muscles) only
False, Stability of the shoulder depends on both dynamic stabilizers (the muscles) and static stabilizers (e.g., the capsule, labrum)
Patient History
Night pain and resting pain are often related to _____ and, on occasion, to ___; activity-related pain usually signifies _______. _____ commonly shows, at least initially, at the extremes of motion.
Acromioclavicular pain is especially evident at _______and tends to be localized to the joint. Similarly, sternoclavicular pain is localized to the joint and increases on ______
rotator cuff tears or tumors
paratenonitis
Arthritis pain
> 90° abduction
horizontal adduction
Patient History
deep, boring, toothache-like pain in the neck, shoulder region, or both may indicate ______ OR _____
Strains of the ______ usually cause dull, toothache-like pain that is worse at night, whereas ________ usually causes a hot, burning type of pain.
_________ are often seen in skiers and may result from holding on to a ski tow; in cross-country skiing, it may result from poling . Paratenonitis is inflammation of the paratenon of the tendon (outer covering of the tendon whether or not it is lined with synovium) Tendinosis is actual degeneration of the tendon itself. With chronic overuse,________ is more likely to be present
thoracic outlet syndrome or acute brachial plexus neuropathy
Rotator Cuff strains
acute calcific tendinitis
bicipital paratenonitis or tendinosis
tendinosis is more likely than paratenonitis
Patient History
Patients with nerve root pain may find that ________ relieves symptoms.
For a patient with instability or inflammatory conditions, _________ usually exacerbates shoulder problems
If the limb tires easily, it may indicate _______. Pressure maybe applied in 3 locations : scalene triangle, at the costoclavicular space, and under the pectoralis minor and the coracoid process.
elevating the arm over the head
lifting the arm over the head
vascular problem ( TOC - can be caused by excessive repetitive demands placed on shoulder)
Patient History
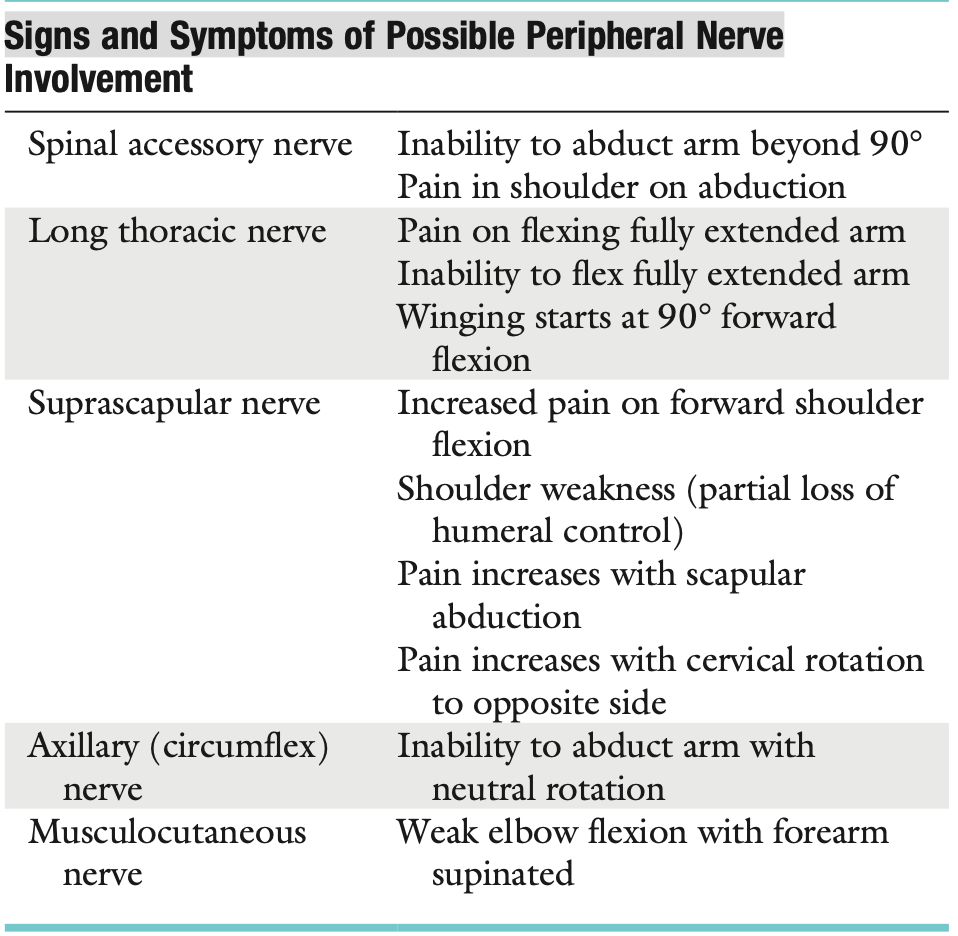
If there is atrophy and paralysis of the supraspinatus and infraspinatus muscles → _______ nerve affected or _______
Dislocation of GH joint could affect ________ → atrophy/paralysis of _______
Fracture to humeral shaft can affect → _______ ( extensors of the elbow, wrist, and fingers are affected and sensation distribution)
Suprascapular nerve or 3rd degree rupture of supraspinatus tendon
Musculocutaneous nerve or axillary nerve → deltoid & teres minor
Radial nerve
Observation
T or F: As part of the observation, noting whether the patient can assume a “neutral pelvis” position is important, because an abnormal pelvic position can lead to an abnormal scapulothoracic, glenohumeral, and cervical spine position and abnormal kinematics in these joints.
True
Observation: Ant View
Ensure ____ & ____ are in midline
Forward Head posture is often associated with _____ shoulders, a medially rotated humerus and a protracted scapula resulting in the humeral head translating _____, a tight ____ capsule, tightness of the ____ ,_____, and _____, and weakness of the lower scapular stabilizers and deep neck flexors.
________ a deformity may be caused by an acromioclavicular dislocation with the distal end of the clavicle lying superior to the acromion process
both the ______ & _____ ligaments have been torn.
_____ is evident anterior to AC joint
______ indicates that degeneration has caused communication between the acromioclavicular joint and swollen subacromial bursa underneath
If a ______ appears when traction is applied to the arm, it may be caused by multidirectional instability or loss of muscle control due to nerve injury or a stroke, leading to inferior subluxation of the GH joint ( deformity is lateral to acromion)
Flattening of the normally round deltoid muscle area may indicate an ___________ or _____ of the deltoid muscle
head and neck
rounded shoulders, humeral anterior translation, posterior capsule; tightness of pectoral, upper trapezius, and levator scapulae
Step deformity → acromioclavicular and coracoclavicular ligaments torn ( can be check in IR and bring hand up or horizontal adduction )
swelling → Fountain sign
sulcus deformity
anterior dislocation of the glenohumeral joint or paralysis
Observation: Ant View
In anterior dislocation, If the examiner palpated in the ____, he or she would feel the head of the humerus.
If the patient is protective of the shoulder, however, it may appear that the injured shoulder, whether dominant or nondominant, is _____ than the normal side
Assume normal functional position of shoulder _________
In this position, or with the arm abducted to 90°, rupture or congenital absence of the_______ may be evident
Rupture of the _______ is often accompanied by a tearing sensation and pop along with weakness, painful LOM and ecchymosis ( bruising).
If the patient’s arm is in IR from this position to bring the hand into midline, the biceps tendon is forced against the lesser tuberosity of the medial wall of the bicipital groove. If this position is maintained for long periods, there may be increased wear of the biceps tendon, which can lead to ____________
If the arm is horizontally adducted while it is medially rotated, anterior pain indicates ______
Wider grooves allow the tendon too much lateral movement, leading to ___________ , the deep grooves tend to be too narrow, compressing the tendon, especially if it becomes _______.
axilla
higher
60° of abduction and the arm in neutral or no rotation
pectoralis major
bicipital tendinitis or paratenonitis
impingement symptoms ( Hawkins Kennedy Test)
Paratenonitis; tendinitis
Observation: Post View
Atrophy of the upper trapezius may indicate ________, whereas atrophy of supraspinatus or infraspinatus may indicate _________ palsy
Test used to measure scapular position ______. Measuring from the spinous processes horizontally to 3 scapular positions: the medial aspect of the most superior point (superior angle), the root of the spine of the scapula, and the infe- rior angle
If the scapula is sitting lower than normal against the chest wall, the superior medial border of the scapula may “washboard” over the ribs, causing a ________ during_________
_________ can lead to altered GH joint angulation, abnormal stress on shoulder liga- ments, altered subacromial space, overload of the AC joint, INC strain on the scapular stabilizing muscles, altered muscle activation, and modified arm position and motion
These alterations are commonly the result of an excessively _______ scapula during arm motion.
spinal accessory nerve palsy; supraspinous nerve
Lennie’s Test
snap during ABAD
Scapular dyskinesia
protracted
Observation: Post View
Scapular Dyskinesia Types:
Type 1: shows the________ being prominent at rest and the inferior angle tilts _____ with movement (scapular tilt), while the acromion tilts ____ over the top of the thorax.
If the inferior border tilts away from the chest wall, it may indicate the presence of _______,____, & _____ or tight _____
2: classic winging of the scapula with the _______ of the scapula being prominent and lifting away
May indicate presence of ______ to _____ lesion & weakness of
3: _______ of the scapula being elevated at rest and during movement; . This deformity is seen with active movement and may result from overactivity of the ______ & _____ along with imbalance of the upper and lower trapezius force couple. Associated with impingement and rotator cuff lesions
4: both scapulae are ______ at rest and movement. they rotate symmetrically upward with the inferior angles rotating laterally away from midline . It is seen during movement and may indicate that the scapular control muscles are not stabilizing the scapula.
inferior medial border prominent, dorsally , anteriorly ( Scapular Tilt & Maybe seen during concentric/eccentric movement)
Weak L traps, Lats & SA or tight Pecs Minor
whole medial border prominent ( Maybe seen during concentric/eccentric movement)
SLAP lesion to biceps lesion & weakness of SA, Rhomboids, TRAPS, Long thoracic nerve or tight humeral rotator
Superior border → Levator & traps( minimal winging in shoulder shrug)
symmetrical scapulae
Observation: Post View
_________ - winging is the result of muscle weakness of one of the scapular muscle stabilizers that, in turn, disrupts the normal muscle force couple balance of the scapulothoracic complex.
_________ - implies that the normal movement of the scapula is altered because of pathology in the glenohumeral joint.
________ - (winging by movement) can be cause by a lesion of long thoracic nerve affecting serratus anterior, trapezius palsy (spinal accessory nerve), rhomboid weakness, multidirectional instability, voluntary action, or a painful shoulder resulting in splinting of the glenohumeral joint, which in turn causes reverse scapulohumeral rhythm.
________ - causes the scapula to depress and move laterally with the inferior angle rotated laterally. If the trapezius is weak or paralyzed, the winging of the scapula occurs before 90° abduction, and there is little winging on forward flexion
________- causes the scapula to elevate and move medially with the inferior angle rotating medially
Winging of the scapula occurs on abduction and forward flexion
Primary scapular winging
Secondary Scapular winging
Dynamic scapular winging
Spinal accessory nerve palsy
Long thoracic nerve palsy
Observation: Post View
________ - (winging occurring at rest) is usually caused by a structural deformity of the scapula, clavicle, spine, or ribs
_________ - developmental condition leading to a high or undescended scapula, most common congenital deformity of the shoulder complex. (uni or bilat.)
Dec abduction
_______ - wasting of supraspinatus & infraspinatus can lead to winging of scapula
Static winging
Sprengel’s deformity
Suprascapular nerve palsy
Examination : T or F
If If the examiner has any doubt as to the location of the lesion, a cervical spine assessment should be done
Scapular instability may be evident in open kinetic chain when the arm is fixed and the rotator cuff muscles work in reverse order (reverse origin- insertion)
In open kinetic chain, the scapula acts as the base or origin of the muscles, whereas the insertion into the humerus is more mobile
True
False, evident in CKC
True
Differential Diagnosis of Shoulder Pathology
Pathology → Symptoms
________ → >35 with Intermittent mild pain with overhead activities
__________ → Mild to moderate pain with overhead activities or strenuous activities
______ → Pain at rest or with activities , Night pain may occur & Scapular or rotator cuff weakness
Rotator cuff tear (full thickness) - ____ pain → Weakness of ____ & _____ and
Loss of _____
Adhesive Capsulitis (idiopathic frozen) → Inability to perform ___ (LOM maybe perceived as weakness)
Anterior instability (with or without external secondary impingement) → ______ to mechanical shifting limits activities ( ____ capsular pattern), _______ may present as instability , ________ pain may be present & Weak scapular stabilizers
Stage 1 External primary impingement
Stage 2
Stage 3
Classic night pain ; Weakness in abduction and lateral rotators & Loss of motion
Inability to perform ADLs owing to loss of motion
Loss of motion may be perceived as weakness
Apprehension to mechanical shifting limits activities usually in HORABER
Slipping, popping, or sliding may present as suitable instability rotation
Anterior or posterior pain may be present
Weak scapular stabilizers
Differential Diagnosis of Shoulder Pathology
Pathology → Symptoms
Posterior instability → _______ of the humerus out the back, associated with ______ & _____ while shoulder is under a compressive load
Multidirectional instability → Looseness of _____ in all directions, most pronounced while _______ or _______ & Pain _______
Slipping or popping of the humerus out the back
This may be associated with forward flexion and medial rotation
Looseness of shoulder in all directions, most pronounced while carrying luggage or turning over while asleep & Pain may or may not be present
AROM
T or F : Shoulder movements may also involve the thoracic spine and ribs.
True
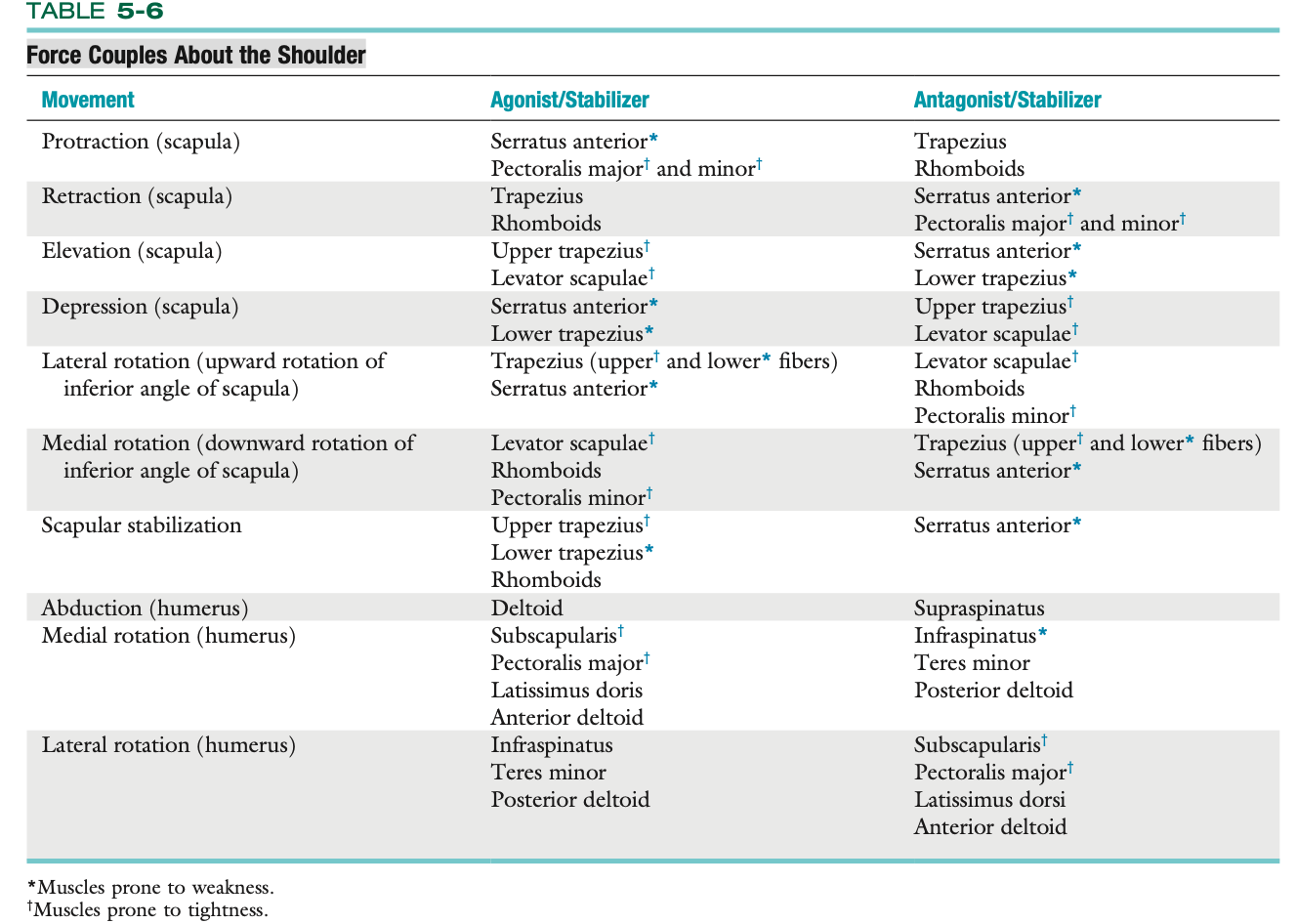
Force Couples About the Shoulder
AROM : Painful Arc
most commonly by _______
45-60° : abduct arm with little difficulty
60-120° : ______ is impinge ( glenohumeral painful arc )
120-160° : painless
170- 180° : _______ or ____
an unstable scapula
subacromial bursa, rotator cuff tendon insertions, especially supraspinatus
acromioclavicular painful arc(localized ) or impingement syndrome (ant shoulder region)
Classification of Glenohumeral Painful Arcs
Anterior
Night Pain
Age
Sex
Aggravated By
Tenderness
AC joint involvement
Calcification
3rd degree strain biceps (long head)
Porgnosis
Yes
50+
Female
ABER
lesser tuberosity
No
calcification SI_S muscles
No
Good
Classification of Glenohumeral Painful Arcs
Posterior
Night Pain
Age
Sex
Aggravated By
Tenderness
AC joint involvement
Calcification
3rd degree strain biceps (long head)
Porgnosis
Yes
50+
Female
ABIR
Posterior aspect of greater tuberosity
No
Supra / Infraspinatus
No
Very GOOD
Classification of Glenohumeral Painful Arcs
Superior ( most common)
Night Pain
Age
Sex
Aggravated By
Tenderness
AC joint involvement
Calcification
3rd degree strain biceps (long head)
Porgnosis
Maybe
40+
Male
Abduction
Greater tuberosity
Often
Supraspinatus and subscapularis
Occasional
Poor (without surgery)
Scapulohumeral Rhythm
Phase 1: No 2:1 ratio yet
Humerus :
Scapula :
Clavicle :
This setting phase means that the scapula may rotate slightly in, rotate slightly out, or not move at all.
30° abduction
minimal movemet (setting phase)
0-5° elevation
Scapulohumeral Rhythm
Phase 2:
Humerus :
Scapula :
Clavicle :
Thus, there is a 2:1 ratio of scapulohumeral movement.
40° abduction
20° rotation, minimal protaction or elevation
15° elevation
Scapulohumeral Rhythm
Phase 3:
Humerus :
Scapula :
Clavicle :
the angle between the scapular spine and the clavicle increases an additional 10°. Thus, the scapula continues to rotate and now begins to elevate.
during this final stage, the humerus finishes its lateral rotation to 90° so that the greater tuberosity of the humerus avoids the acromion process.
60° abduction, 90° lateral rotation
30° rotation
30-50° posterior rotation , 15° elevation
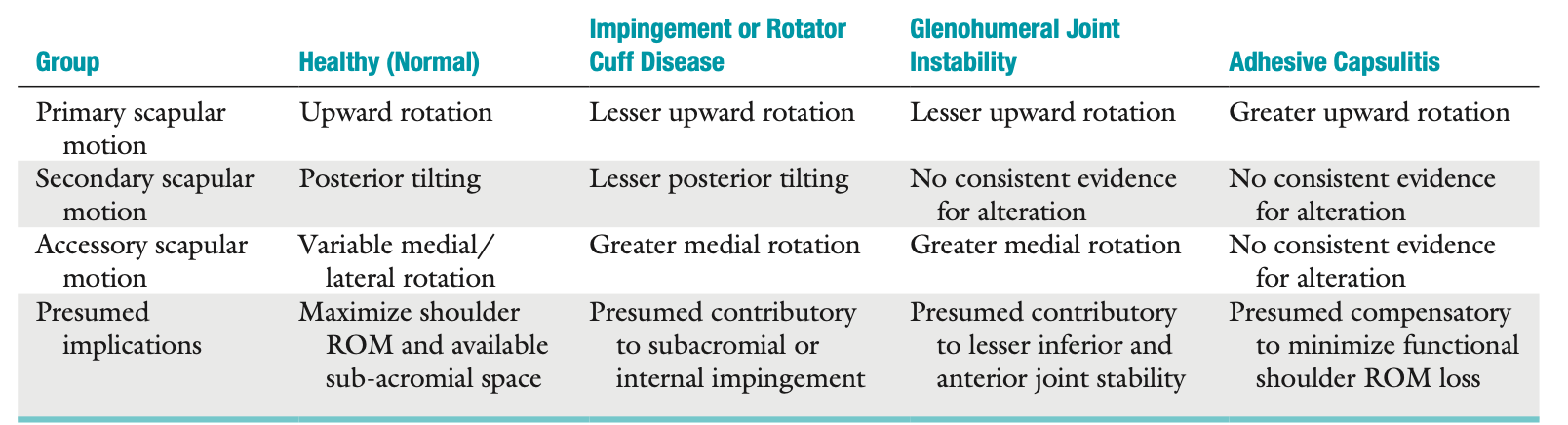
Summary of Scapular Kinematics During Arm Elevation in Healthy and Pathologic States
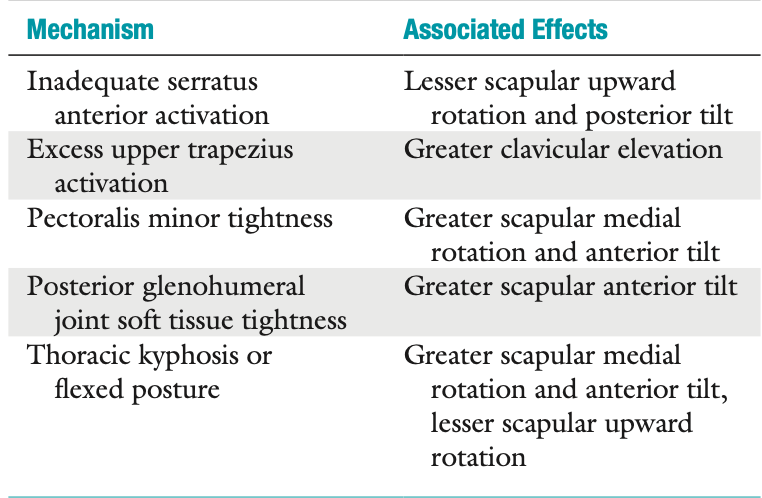
Mechanisms of Scapular Dyskinesia
If the clavicle does not rotate and elevate, elevation through abduction at the glenohumeral joint is limited to ____
If the glenohumeral joint does not move, elevation through abduction is limited to ___
If there is no lateral rotation of the humerus during abduction, the total movement available is ____, 60° of which occurs at the glenohumeral joint and 60° of which occurs at the scapulothoracic articulation.
120°
60°
120°
_________ means that the scapula moves more than the humerus. This occurs in conditions like the frozen shoulder. The patient appears to “hike” the entire shoulder complex rather than produce a smooth coordinated abduction movement.
Reverse Scapulohumeral rhythm
Active elevation (170° to 180°) through the plane of the scapula (30° to 45° of forward flexion), termed scaption, is the most natural and functional motion of elevation
Doing the rotation testing in 90° abduction (if the patient can achieve this position) will give a clearer indication of true glenohumeral joint medial and lateral rotation, which are measured when the scapula starts to move .
If rotation is tested in 90° abduction and crepitus is present on rotation, it indicates abrasion of torn tendon margins against the coracoacromial arch and is called the “______
abrasion sign.
Normally, any gain in lateral rotation is commonly accompanied by a comparable loss in medial rotation.
A GIRD can lead to → ______ →
GERD → ________
______ caused by scapula rubbing over the underlying ribs
Posteroinferior capsule → SLAP lesion
shoulder problem
Snapping scapula
Functional ROM Combined Test
_______ combines medial rotation with adduction and lateral rotation with abduction
Note: Often, the dominant shoulder shows greater restriction than the non-dominant shoulder, even in normal people. An exception would be patients who continually use their arms at the extremes of motion
Muscles that are tight in ant shoulder instability : _______ while ______ weak
Apley’s scratch test (scratch at back)
subscapularis, pectoralis minor and major, LATS , upper trapezius, levator scapulae, SCM, scalenes, and rectus capitus.
serratus anterior, middle and lower trapezius, infraspinatus, teres minor, posterior deltoid, rhomboids, longus colli, and longus capitus.
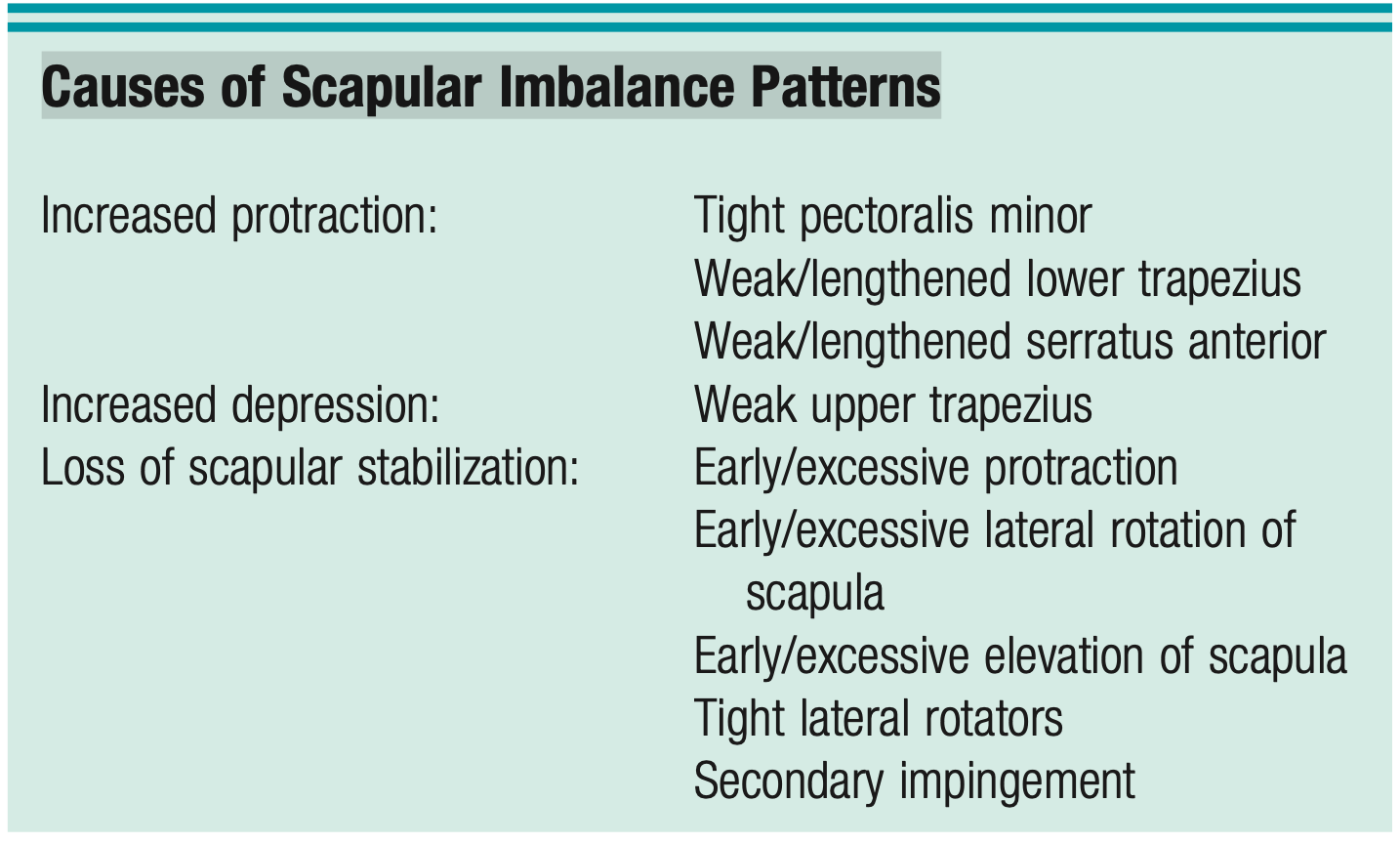
Causes of Scapular Imbalance Patterns
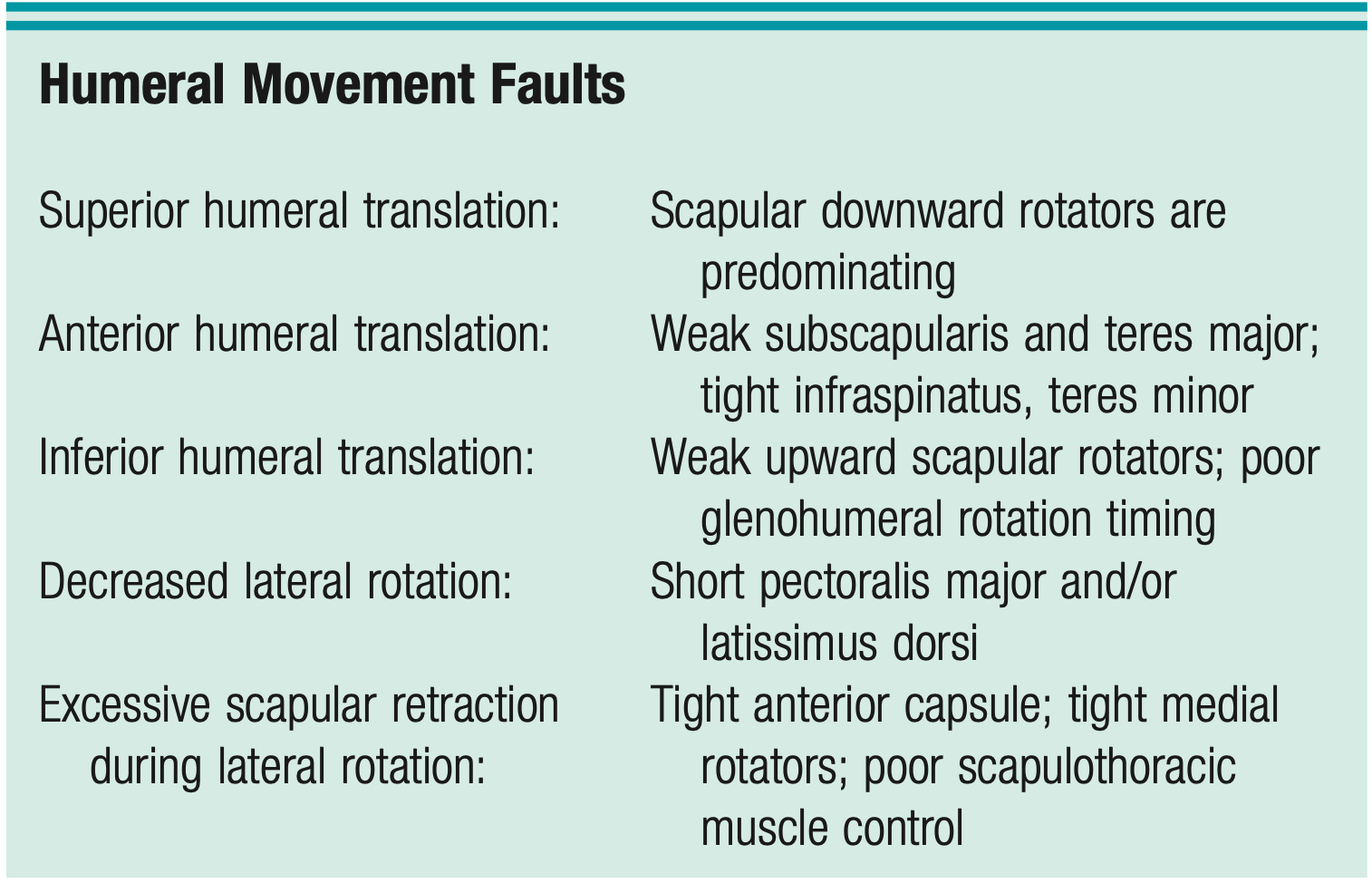
Humeral Movement Faults
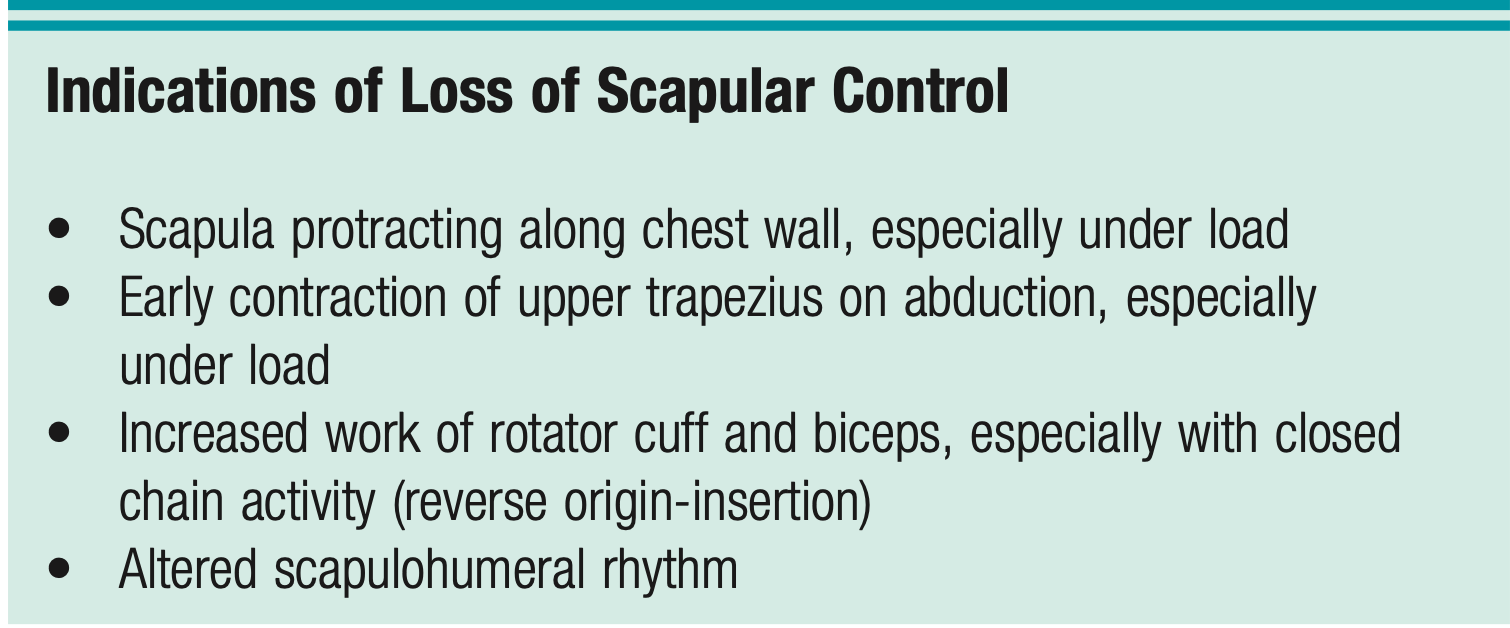
Indications of Loss of Scapular Control
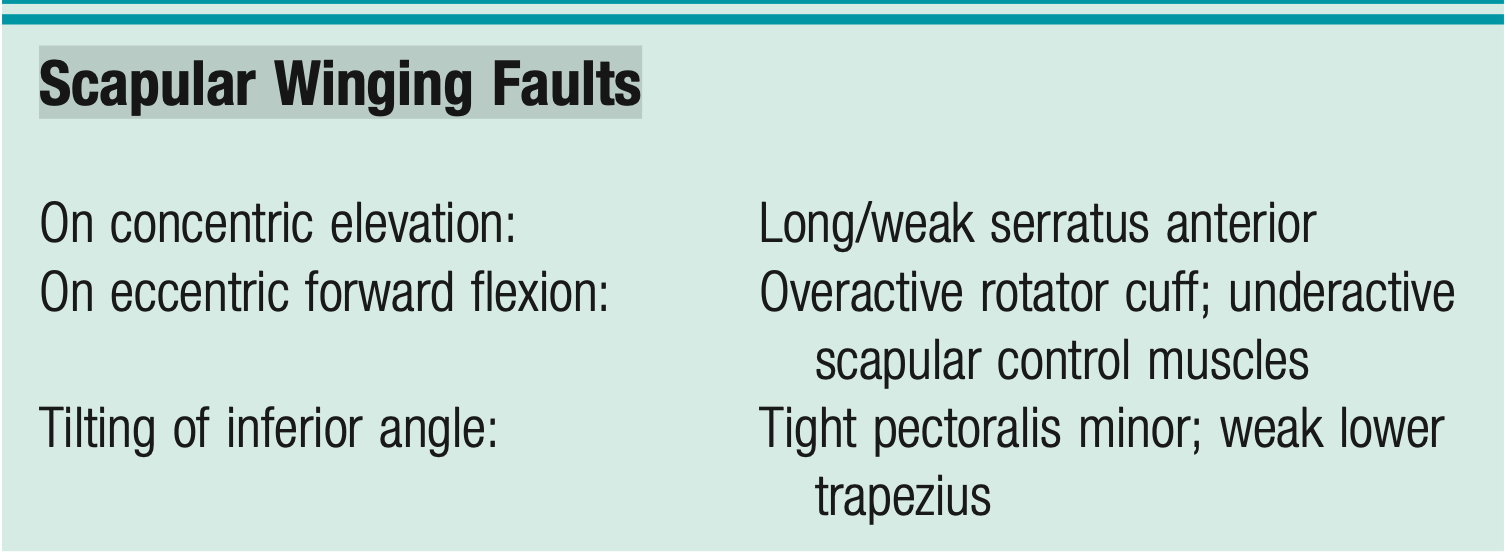
Scapular Winging Faults
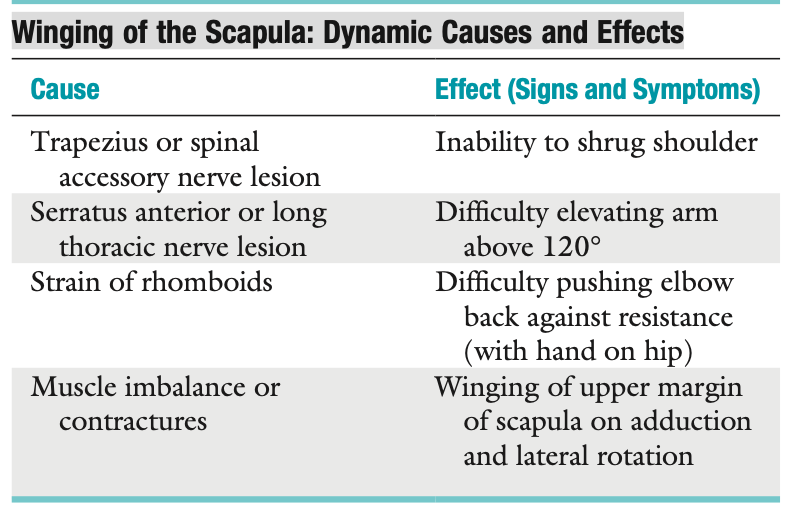
Winging of the Scapula: Dynamic Causes and Effects
Signs and Symptoms of Possible Peripheral Nerve Involvement
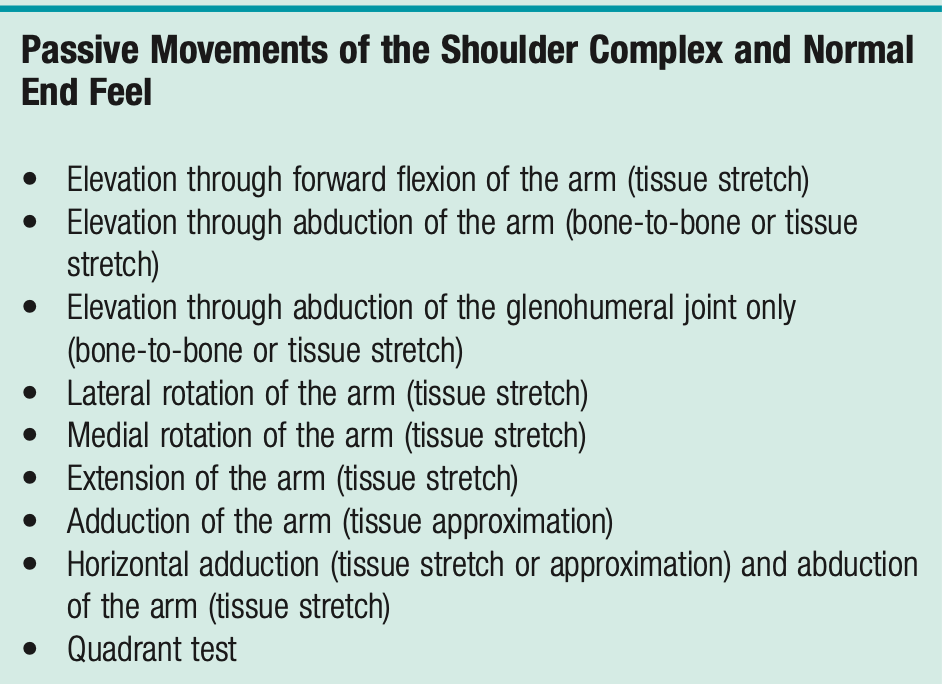
Passive Movements of the Shoulder Complex and Normal End Feel
Subcoracoid bursitis may limit full lateral rotation, and subacromial bursitis may limit full abduction because of compression or pinching of these structures.
Resisted Isometric Movements
T or F: The scapula should not move during isometric testing. Scapular protraction, winging, or tilting during isometric testing indicates weakness of the scapular control muscles.
3rd degree strain (rupture) of the long head of biceps tendon presents ______ sign when testing isometric elbow flexion
True
Pop-eye sign
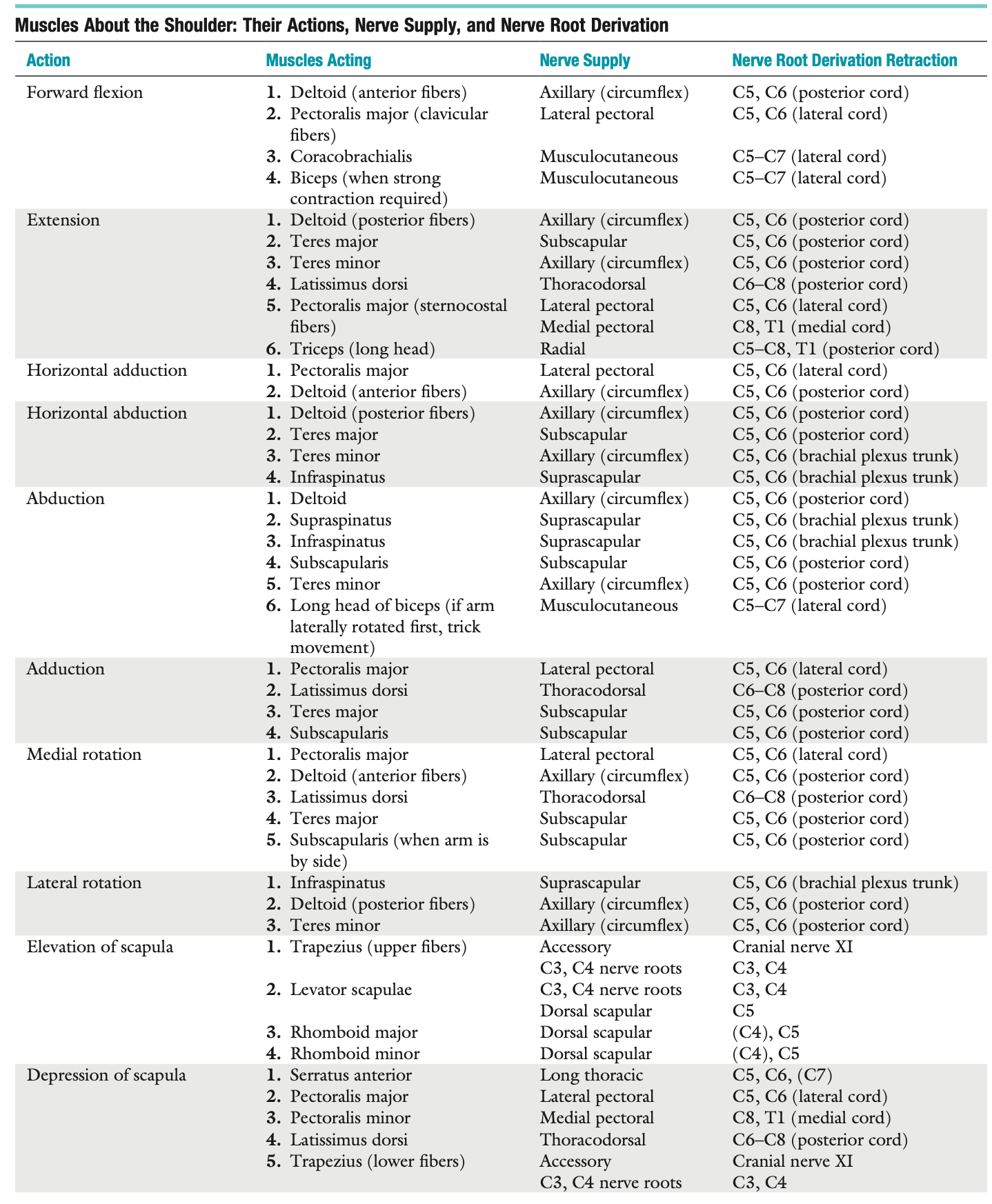
Muscles About the Shoulder: Their Actions, Nerve Supply, and Nerve Root Derivation
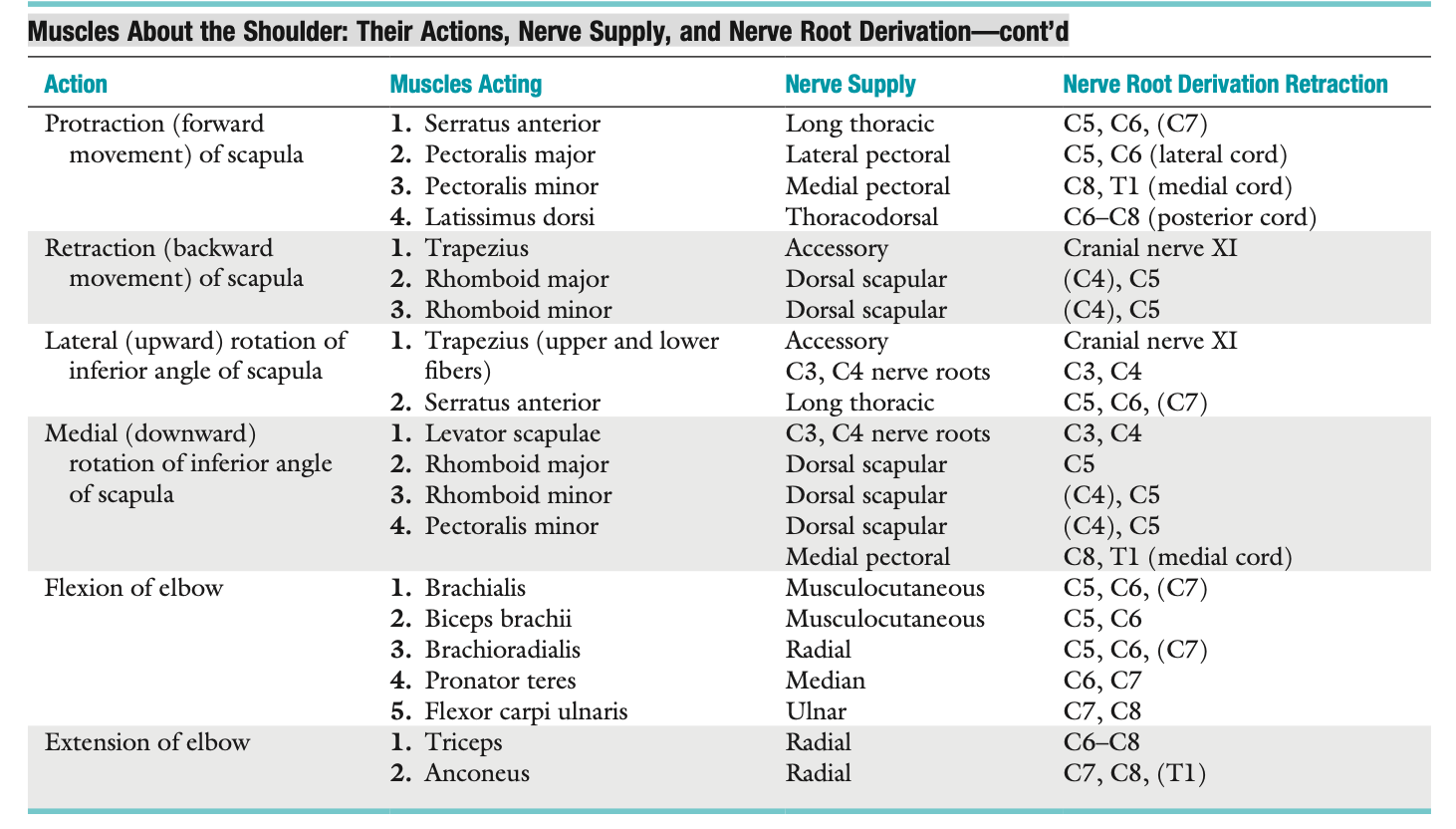
Muscles About the Shoulder: Their Actions, Nerve Supply, and Nerve Root Derivation—cont’d
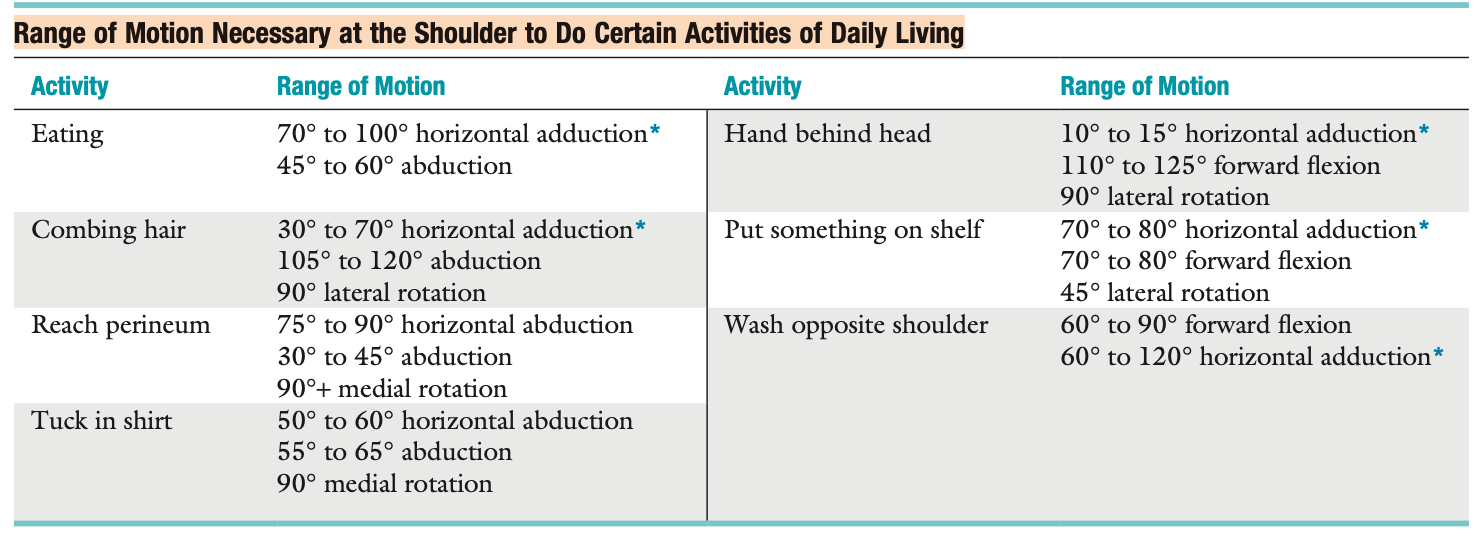
Range of Motion Necessary at the Shoulder to Do Certain Activities of Daily Living
:)
Palpation : Anterior
Clavicle - make sure it is in its resting position in injured side.
SC joint - also palpate the ligaments & SCM
AC joint - ligaments, muscles ( traps, deltoid, subclavius)
Coracoid Process: In ______ syndrome is very tender
Sternum
Ribs & Costal Cartilage
Humerus & SITS
Axilla
SICK scapula syndrome
Palpation : Posterior
Spine of scapula
Scapula
Spinous processes of lower cervical & thoracic spine - trapezius
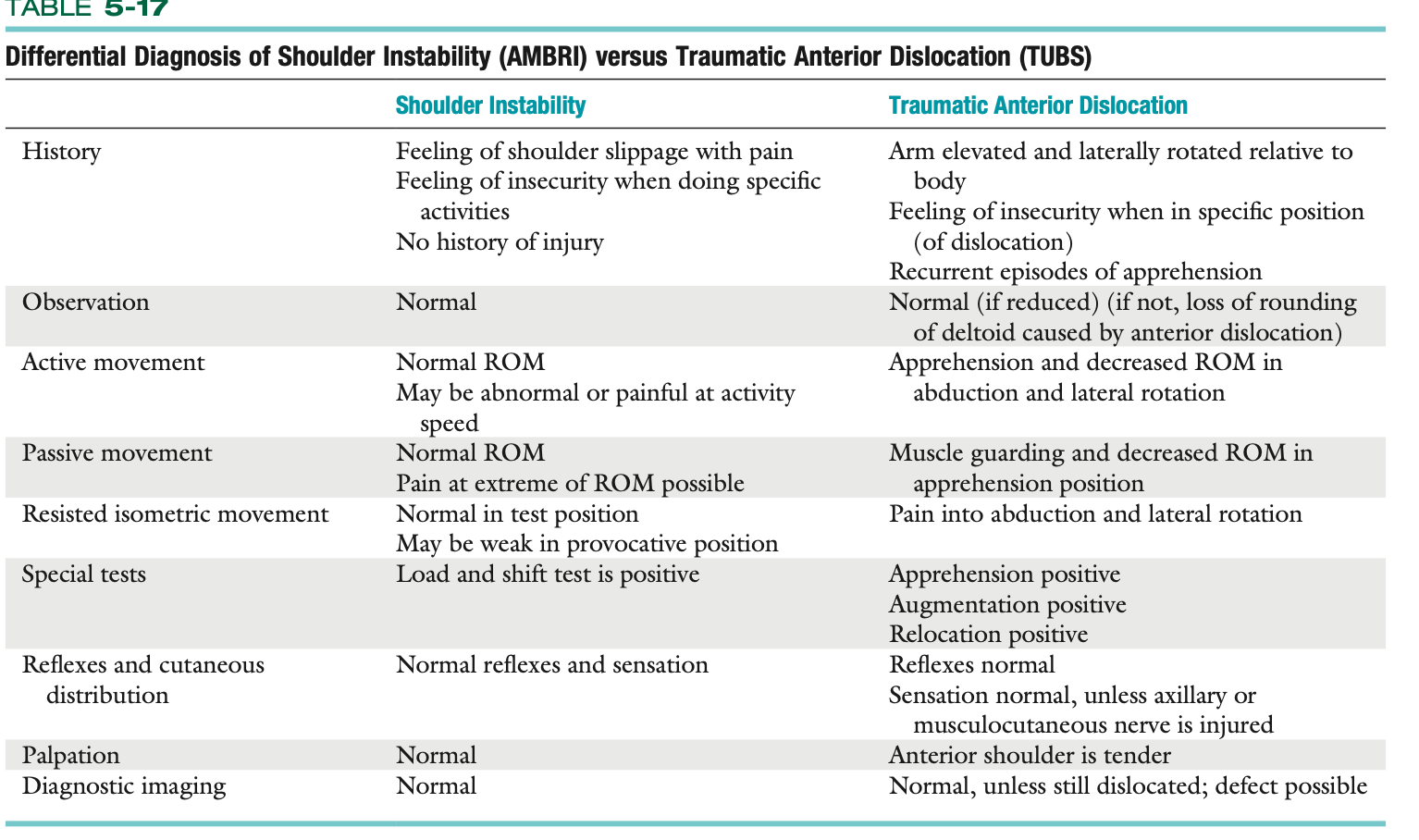
Differential Diagnosis of Shoulder Instability (AMBRI) versus Traumatic Anterior Dislocation (TUBS)
T or F: A hypermobile or lax joint does not imply instability.
True
Instability and Pseudolaxity Impingement
_______ - In the older patient (40-years-old or older), mechanical impingement occurs because of degenerative changes to the rotator cuff, the acromion process, the coracoid process, and the anterior tissues from stress overload resulting in impingement.
_______ - In the young patient (15 to 35-years-old), anterior shoulder pain is primarily caused by problems with muscle dynamics with an upset in the normal force couple action leading to muscle imbalance and abnormal movement patterns at both the glenohumeral joint and the scapulo- thoracic articulation.
_______ - This type of impingement is found posteriorly rather than anteriorly, mostly in overhead athletes. It involves contact of the undersurface of the rotator cuff (primarily supraspinatus and infraspinatus) with the posterosuperior glenoid labrum when the arm is abducted to 90° and laterally rotated fully.
primary impingement
Secondary impingement
Internal impingement
T or F:
If a patient exhibits posterior instability , multidirectional instability is also present
ERABIR results to posterosuperior impingement
True
False, ABER
Labral Tear
In young, _____ stress when applied to GH joint results to injury
Tear maybe ______ where anteroinferior labrum is torn or _______ when superior labrum is affected
_____ lesion occurs commonly with a traumatic anterior dislocation leading to anterior instability
anterior
BANKART lesion → IGHL stability lost
SLAP
BANKART ( 3-7 O CLOCK)
Labral Tear
______ Occurs when the poster GH dislocation occurs and results in labrum detached from 6-9 o clock
_____ lesion that occurs in 10-2 O clock position,caused by FOOSH, decceleration when throwing or when sudden traction is applied in bicpes
Reverse Bankart lesion
SLAP lesion
Types of SLAP LESION
1
2 (Most Common)
3
4
A _____ mechanism results in a posterior TYPE 2 SLAP lesion in overhead athletes, INC ER, DEC IR and tight posterior capsule = tear in posterosuperior labrum
Superior Labrum strained but intact
Small tear in SL + instability of labrum-biceps complex
Bucket handle tear of labrum that displace into joint; labral biceps attachment intact
Bucket handle tear of labrum that extends to the biceps tendon, allowing tendon to sublux into joint
REFLEX
often assessed reflex are 😀
C5-C6 → Pecs major and clavicular portion; biceps
C7,C8,T1 → sternocostal
C7-C8 → triceps
Peripheral Nerve Injuries of the Shoulder
_______- MOST COMMONLY INJURED nerve in the shoulder.
MOI : _______
Muscle: _____,______
Axillary nerve
Anterior dislocation/ fracture of humeral neck
Deltoid & Teres Minor
Peripheral Nerve Injuries of the Shoulder
_______ -Injury from a fall on posterior shoulder, stretching, repeated microtrauma or fracture of scapula
Muscle: ______,______
Suprascapular nerve
Supraspinatus & infraspiantus
Peripheral Nerve Injuries of the Shoulder
______ - Injured due to humeral dislocation, fracture
Muscle : ____,______
Musculocutaneous nerve
biceps,brachialis,coracobrachialis
Peripheral Nerve Injuries of the Shoulder
_______ - Injury from repeated microtrauamtic activities
Symtpoms: _____,_______,______
Long thoracic nerve
SA weakness, medial winging of scapula and weakness on forward flexion
Peripheral Nerve Injuries of the Shoulder
_______ - traumatic injury
Symptoms: affect trapezius, shoulder drooping and lateral scapular winging
Spinal accessory nerve
Once all struggle is grasped, miracles are possible
Break a 🦵 !!!