PDA Lecture 20: Nicotinic Receptor Agonists and Antagonists
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
32 Terms
Nicotinic Receptors:
- fast or long-acting?
- how many subunits? binding sites?
- what are the 2 major types of nicotinic receptors?
- Fast acting ligand-gated ion channel
- Pentamers (5 subunits) with at least 2 binding sites
- Nicotinic Muscle (Nm) and Nicotinic Neuronal (Nn)

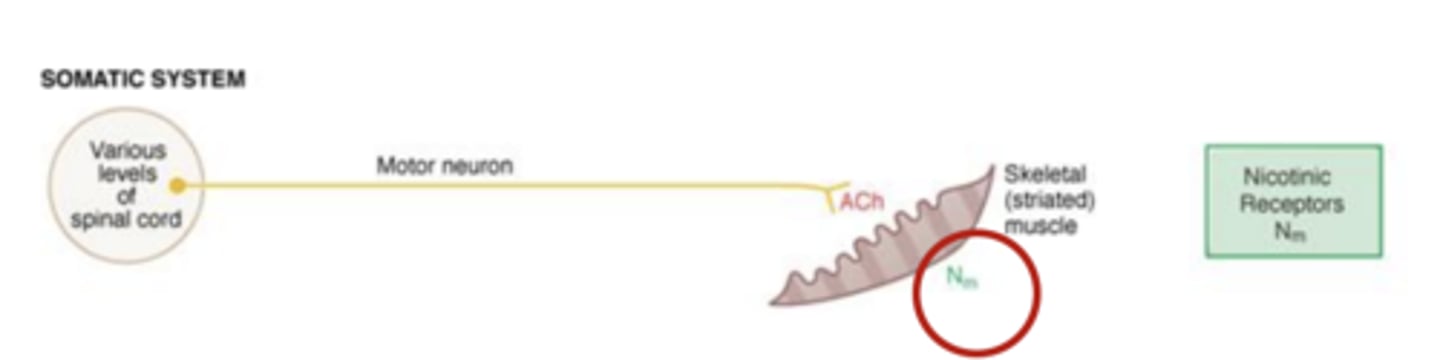
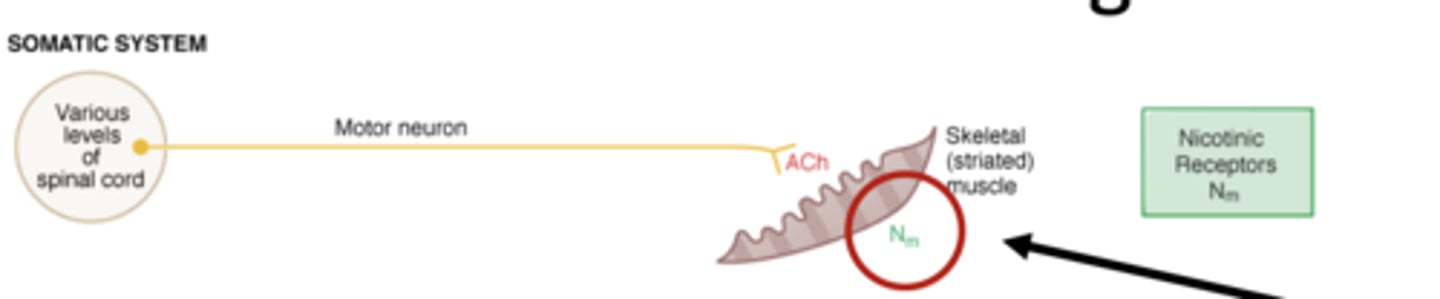
What is nicotinic muscle type involved in?
Where is it found?
- involved in somatic system
- found in skeletal muscle tissue
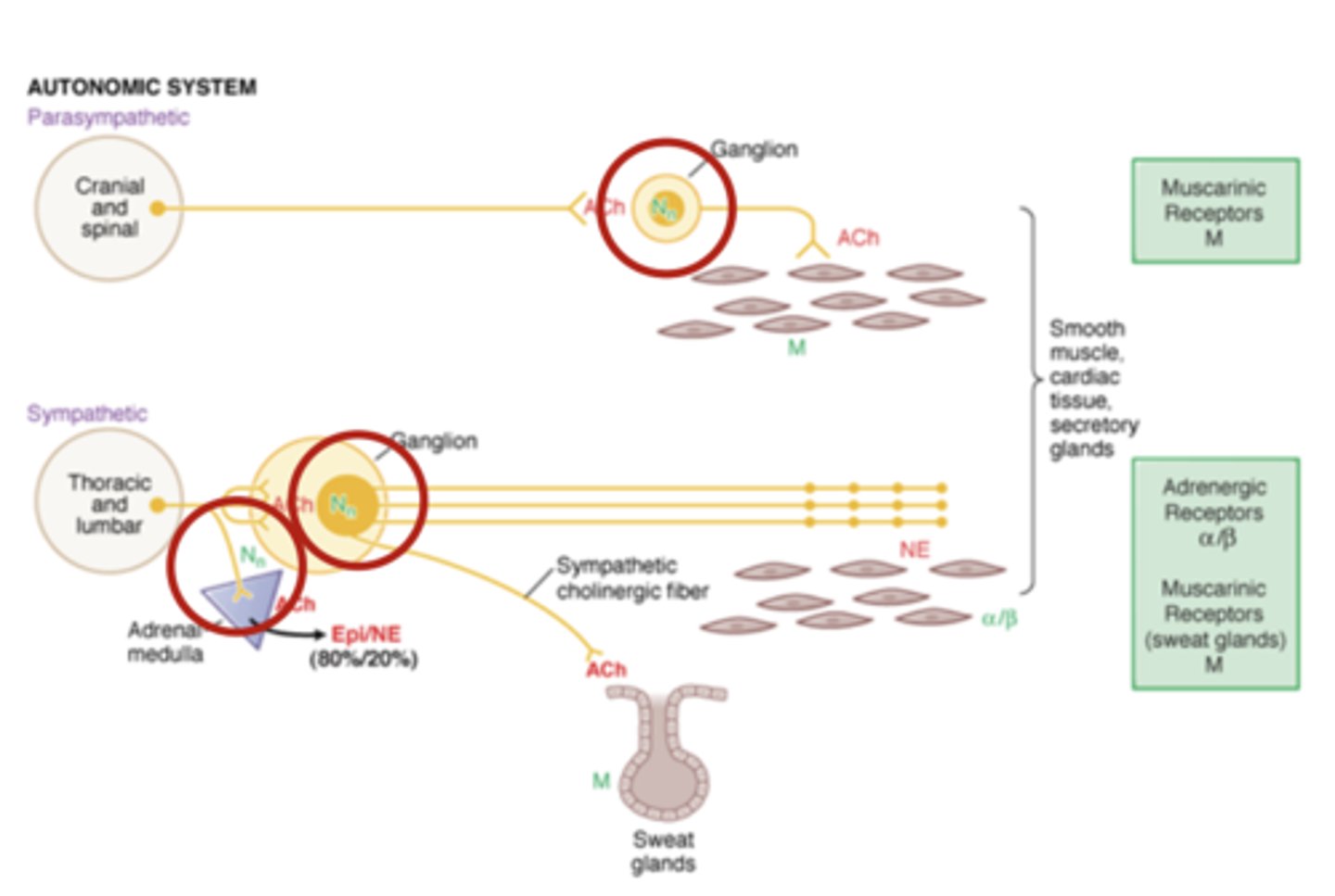
What is nicotinic neuronal type involved in?
Where is it found?
- involved in the autonomic system
- Found on ganglionic nerve bundles of sympathetic and parasympathetic systems (and activated by pre-ganglionic neurons in both systems)
- Also found on adrenal medulla, and in the CNS
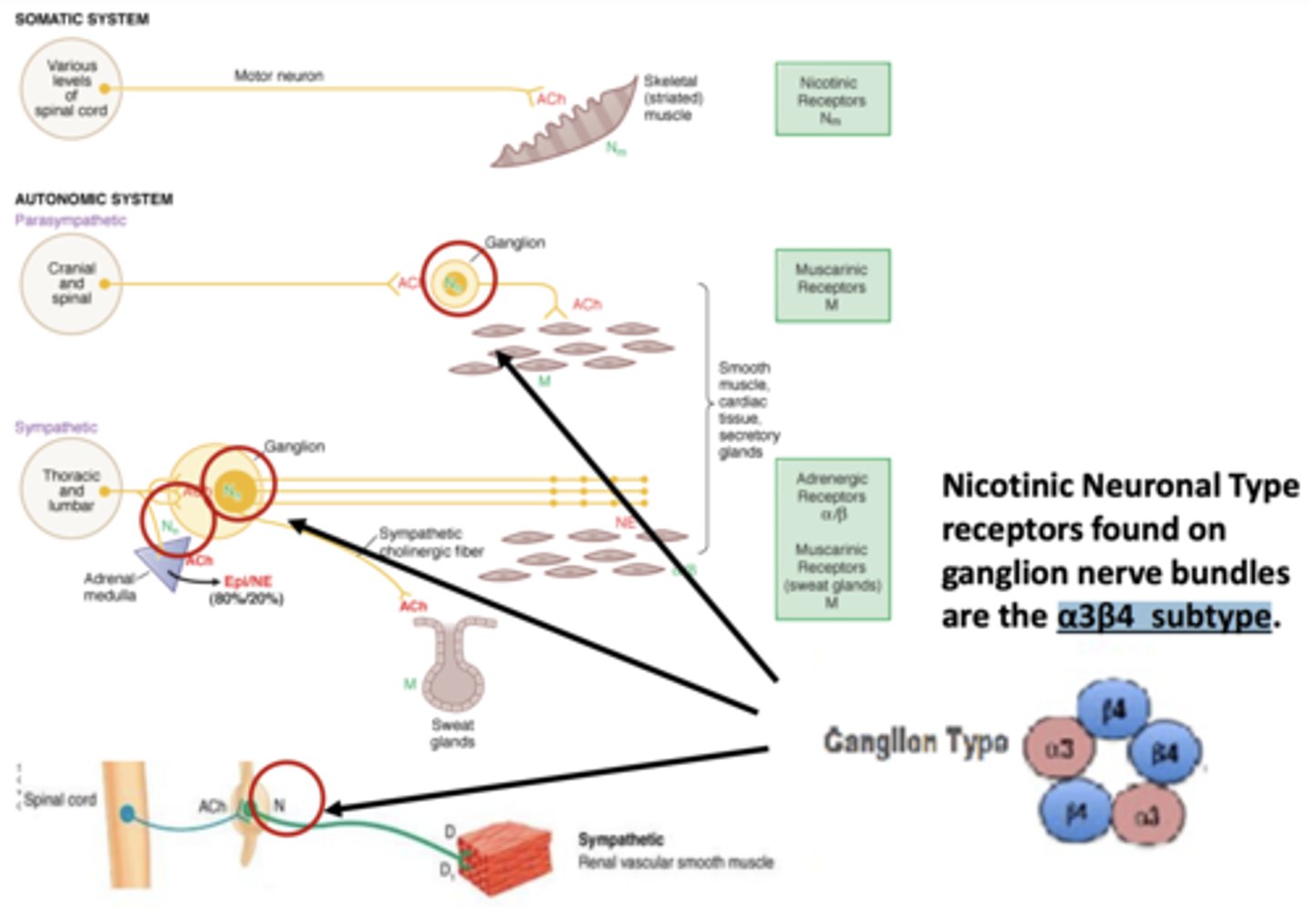
Nicotinic Neuronal Type receptors found on ganglion nerve bundles are the ____________________ subtype
α3β4 subtype
T/F: Drugs that work as nicotinic neuronal type agonists and antagonists are commonly prescribed
FALSE
they are not commonly prescribed
Why are drugs that work as nicotinic neuronal type agonists and antagonists not commonly prescribed?
- the high number, wide distribution, and diversity of nicotinic receptors in the body makes it difficult to develop effective drugs
- Interfere with too many biological and psychological processes
Example of a nicotinic neuronal type receptor agonist
Varenicline (Chantix)
− Used for smoking cessation.
Neuromuscular Blockers
- Agonist or antagonist for Nicotinic Muscle Type Receptors at the neuromuscular junction (synapse between motor neuron and skeletal muscle)
Neuromuscular Blockers: Both ___________ and ______________ work by __________ neuronal signal at the neuromuscular junction of the _____________, causing ______________________
- agonist and antagonist
- blocking
- somatic system
- muscle paralysis
What are neuromuscular blockers used for?
muscle spasms and surgical procedures
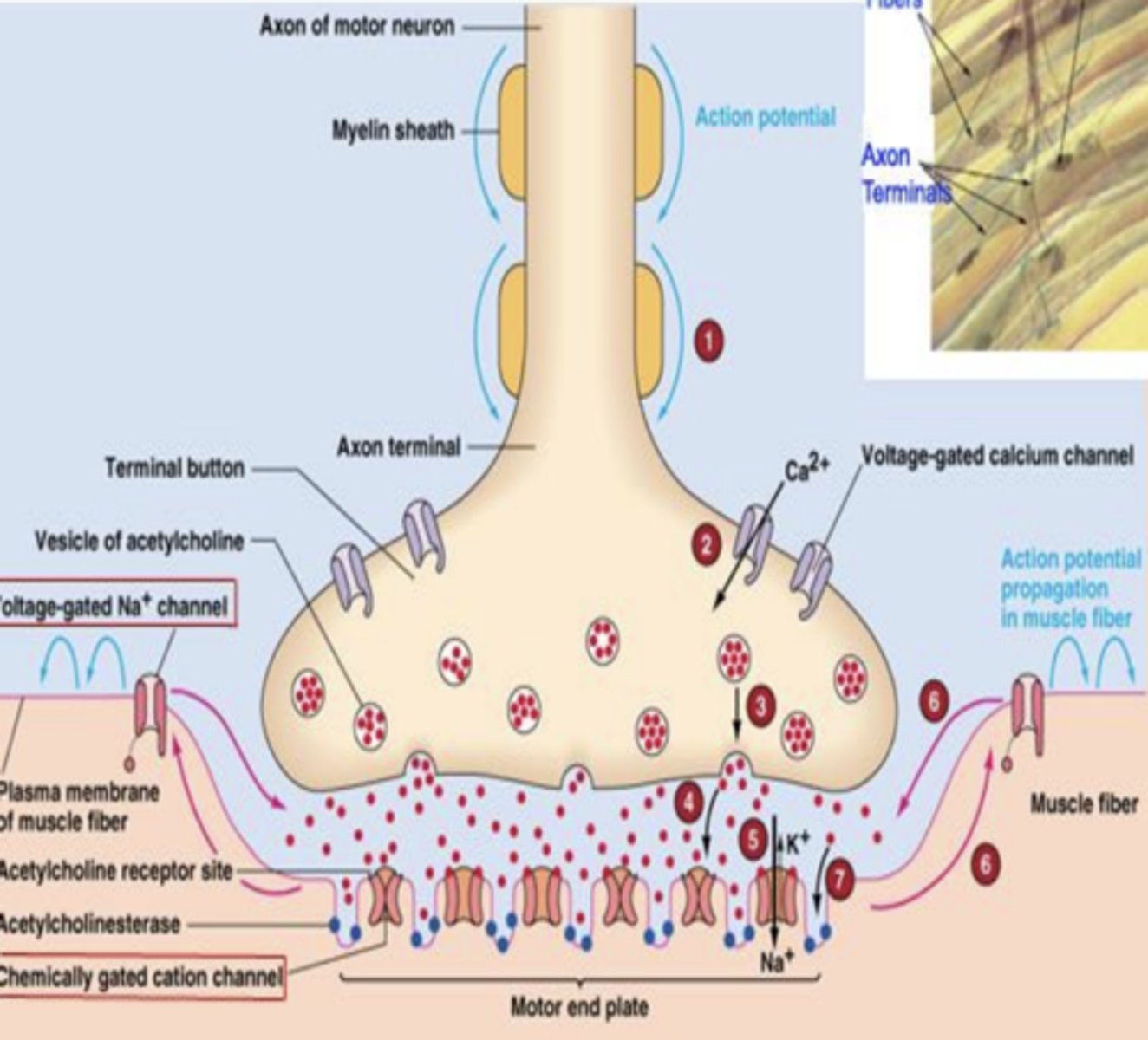
The neuromuscular junction diagram
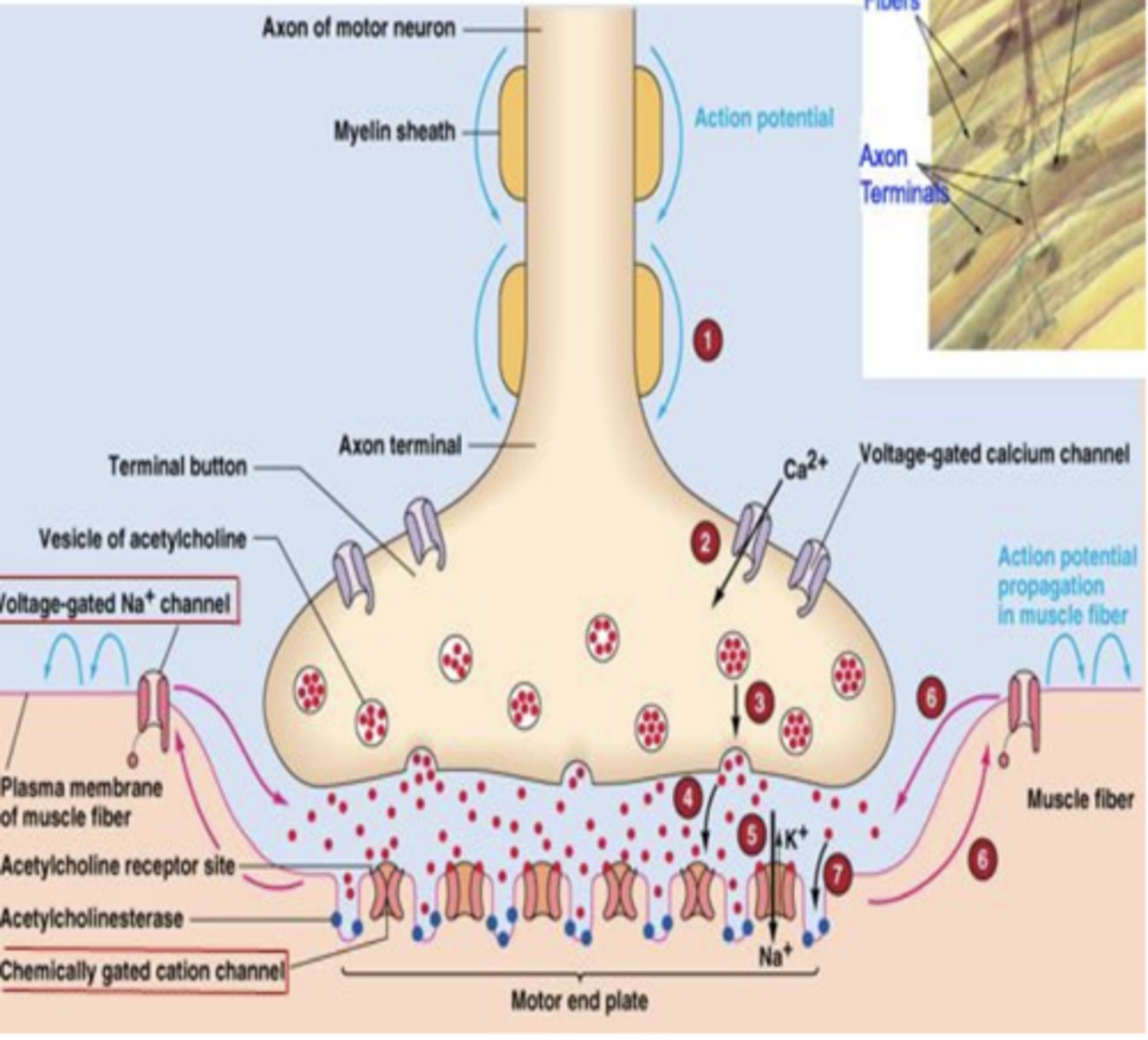
Steps of muscle contraction and the neuromuscular junction
1) Action potential (AP) travels down axon.
2) Voltage-gated Ca++ channels open with detection of AP depolarization.
3) Ca++ allows vesicles to release Ach
4) ACh crosses synapse and activates muscle-type ligand-gated nicotinic receptors with Na+ channels.
5) Na+ crosses channel, enters motor end plate, and depolarizes cells
6) Depolarization activates voltage-gated Na+ channels causing an end plate potential (EPP)
7) End Plate Potential spreads quickly across and into muscle tissue, allowing muscle to contract
The two types of Neuromuscular Blockers
- Depolarizing (agonist)
- Non-Depolarizing (antagonist)
How can a receptor agonist block an electrochemical signal?
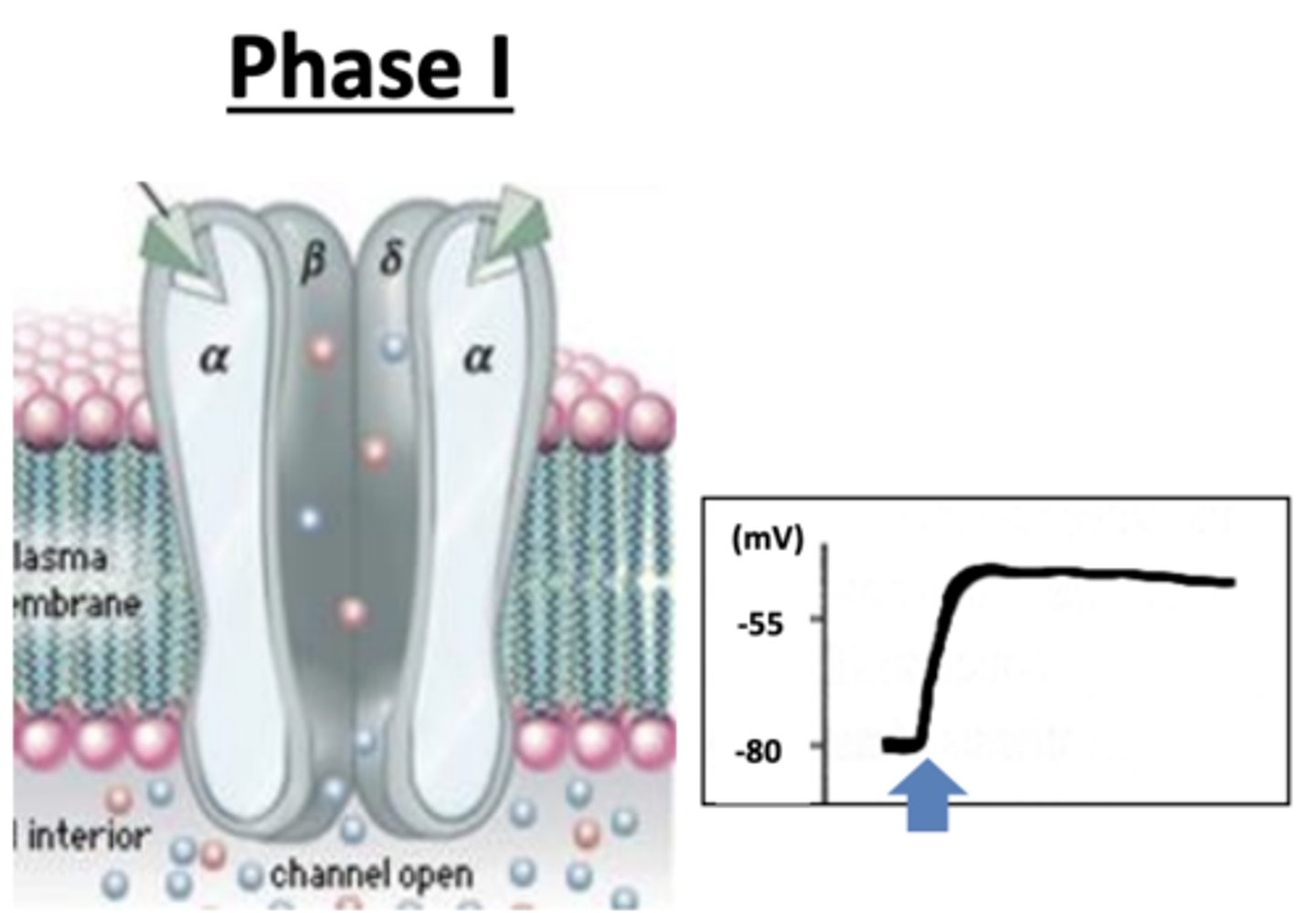
Characteristics of Depolarizing (agonist) Neuromuscular Blockers: Phase I
• Agonist (e.g. Succinylcholine) binds to receptor, remains attached, keeps channel in open state, and sustains depolarization.
• Na+ channel remains open, causing cell depolarization and excitation of muscle tissue
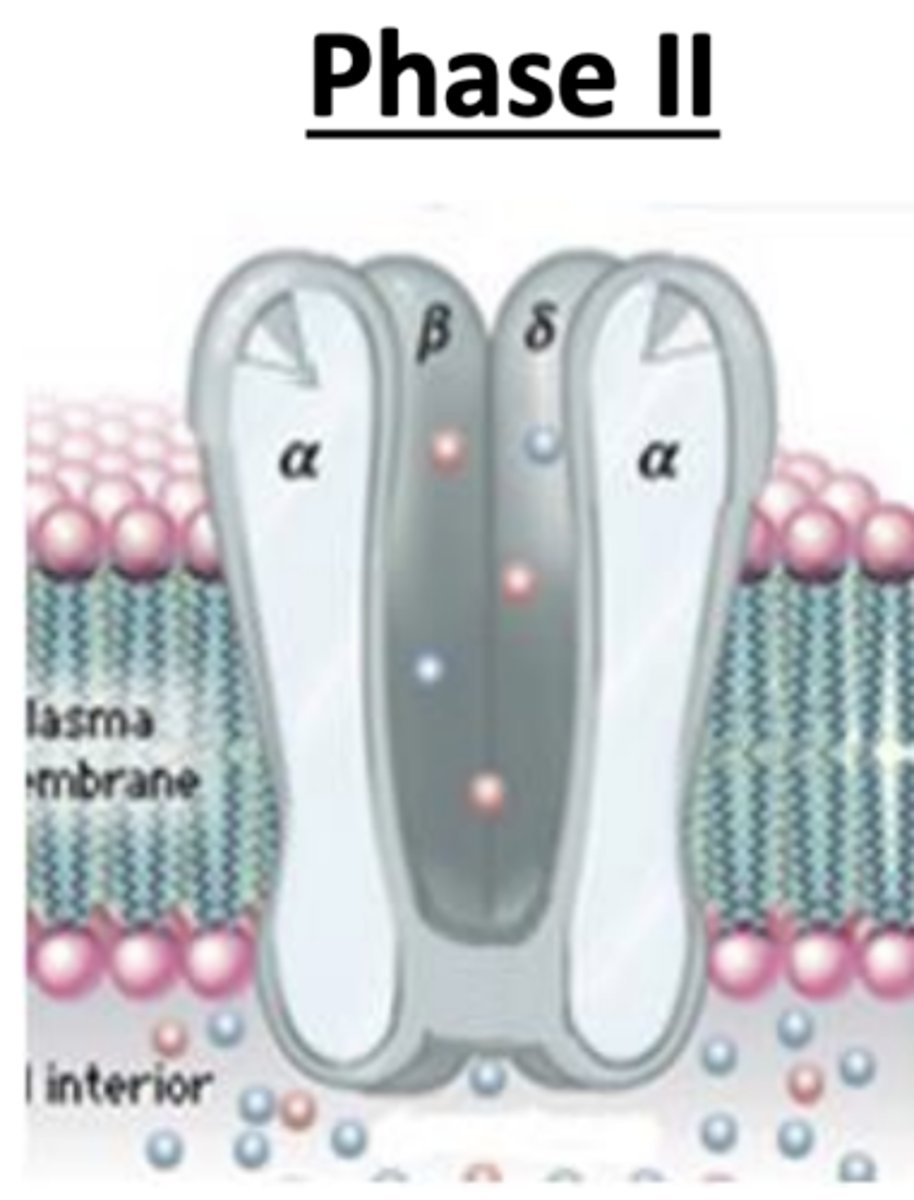
Characteristics of Depolarizing (agonist) Neuromuscular Blockers: Phase II
• Agonist remains attached, receptor becomes desensitized and reconfigures to a closed state
• Na+ influx ceases, cell repolarizes, and muscle contractions are prevented
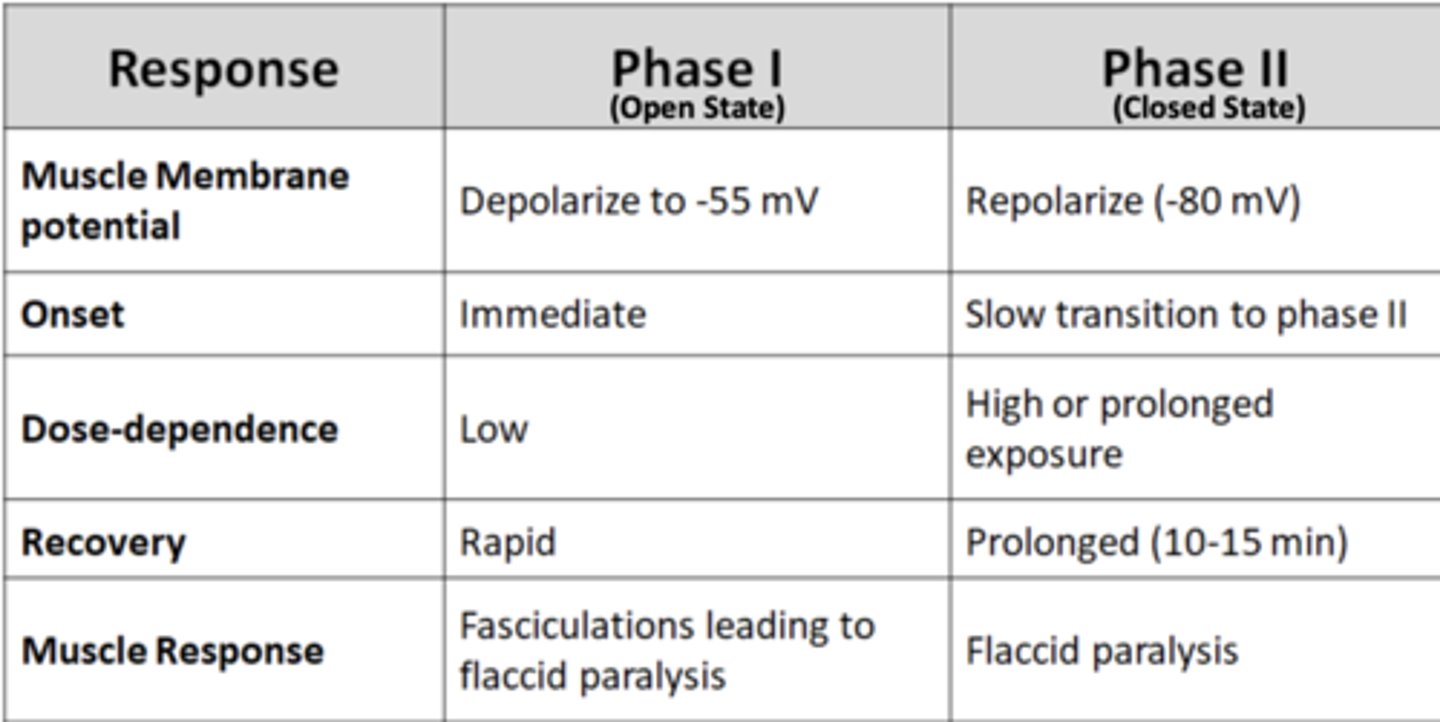
Phase I vs. Phase II comparison table
- Muscle membrane potential:
- Onset:
- Dose-dependence:
- Recovery:
- Muscle Response:
Phase I
- Muscle membrane potential: depolarize to -55 mV
- Onset: Immediate
- Dose-dependence: Low
- Recovery: Rapid
- Muscle Response: Fasciculations leading to flaccid paralysis
Phase II
- Muscle membrane potential: Repolarize (-80 mV)
- Onset: Slow transition to phase II
- Dose-dependence: High or prolonged exposure
- Recovery: Prolonged (10-15 min)
- Muscle Response: Flaccid paralysis
Characteristics of Non-Depolarizing (antagonist) Neuromuscular Blockers:
What do competitive antagonists of muscle-type nicotinic receptors at neuromuscular junction do?
Block end plate potential and muscle contraction
Do Non-Depolarizing (antagonist) Neuromuscular Blockers cause muscle paralysis slowly or rapidly?
Muscle paralysis occurs gradually (slower onset, than depolarizing blocker)
Non-Depolarizing (antagonist) Neuromuscular Blockers can cause _____________________ of antagonist blocking by ____________________ levels
- rapid reversal
- increasing acetylcholine levels
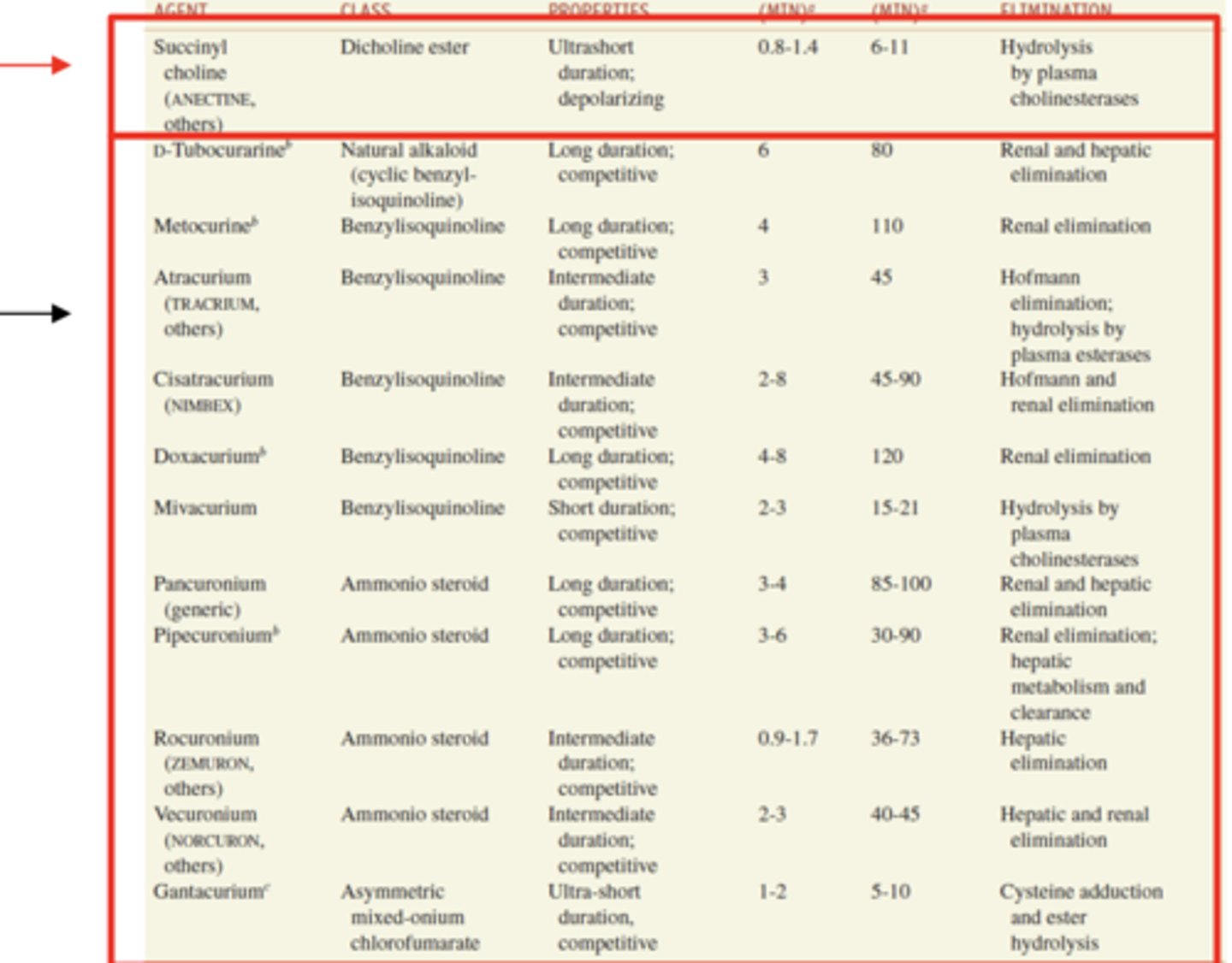
Two Types of Non-Depolarizing Neuromuscular Blockers
- Steroid Derivatives
- Isoquinoline Derivatives
Steroid derivatives and isoquinoline derivatives chart
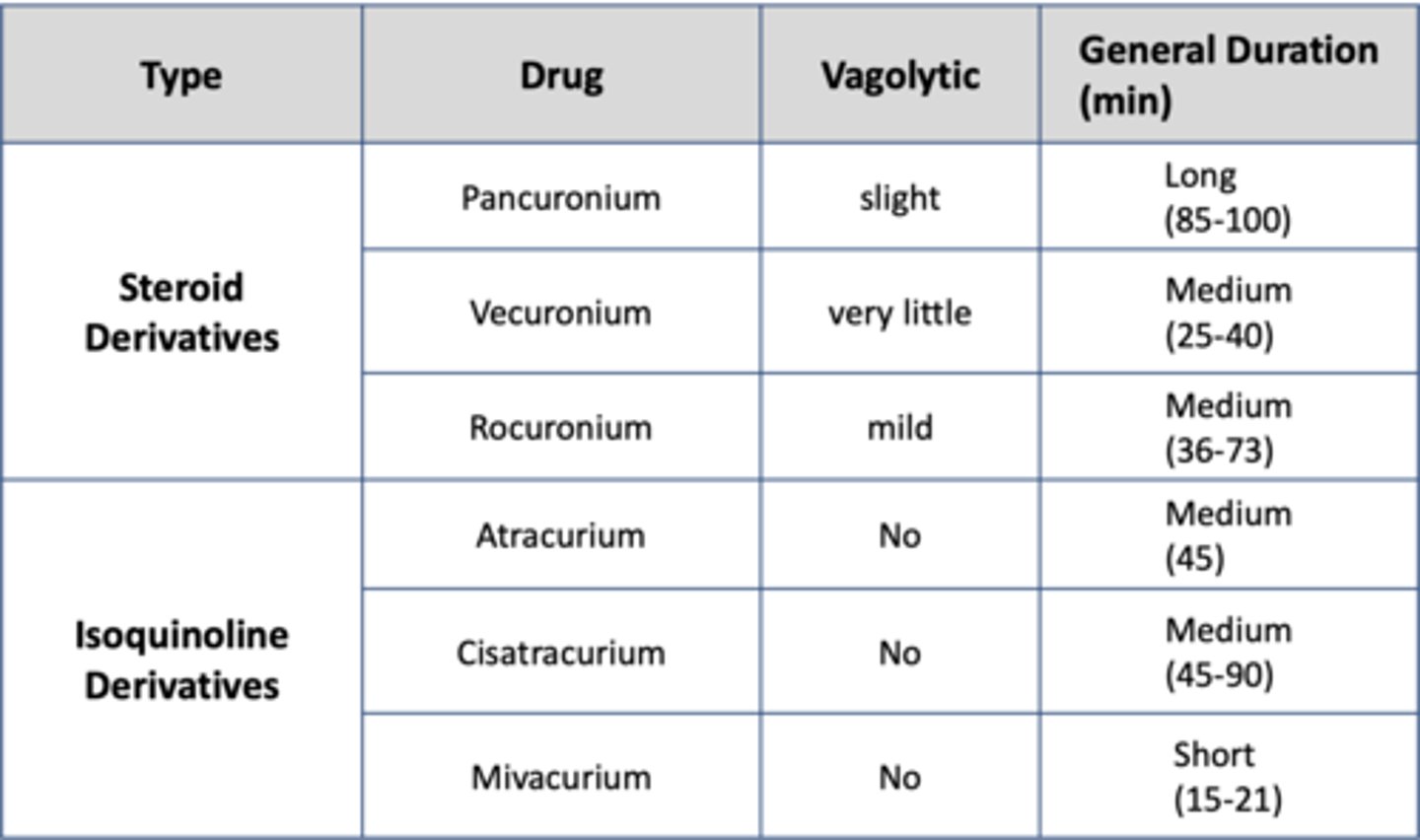
Vagolytic meaning
Inhibitory effect on the Vagus nerve regulation of heart (we don't want this)
Example of a Non-Depolarizing Neuromuscular Blocker: Tubocurarine (curare) (4)
- Used as arrow poison to hunt for large animals by paralyzing respiratory system
- Large molecule, so does not enter blood stream when eaten
- Griffith and Johnson (1942) use curare to develop standard of use for clinically “balanced” anesthesia
- Prompted synthesis of many useful nondepolarizing blockers
Drugs with very rapid onset of action (~1 min) but short duration (5-10 min) are ideal for…
tracheal intubation and require continuous infusion
Drugs with rapid onset (2-4 min) and intermediate duration (20-90 min) are ideal for…
short surgical procedures
Drugs with relatively slower onset (>3-4 min) and long duration of action are ideal for…
major surgery
Possible adverse side effects of Neuromuscular Blockers used for intubation and surgery
• Prolonged apnea (cessation of breathing)
• Cardiovascular collapse
• Histamine release (inflammatory response)
• Hypothermia
Botulinum toxin (Botox): A Nicotinic Muscle Type Receptor Indirect Antagonist (2)
- Toxin is produced by bacteria (Clostridium botulinum)
- Decreases nicotinic muscle type receptor activation without directly targeting nicotinic receptor
Botulinum Toxin (3)
• Toxin can cause paralytic illness (botulism)
• Can enter through wound , inhalations, consumption of contaminated food or water (lead to improvements in food safety)
• Treatable soon after exposure with emetics or enemas or later with antitoxin Heptavalent
Botox
- Used cosmetically today to relax facial muscles and reduce wrinkles
- Only a part of the toxin is used in microdoses
- Clinically used for tension headaches
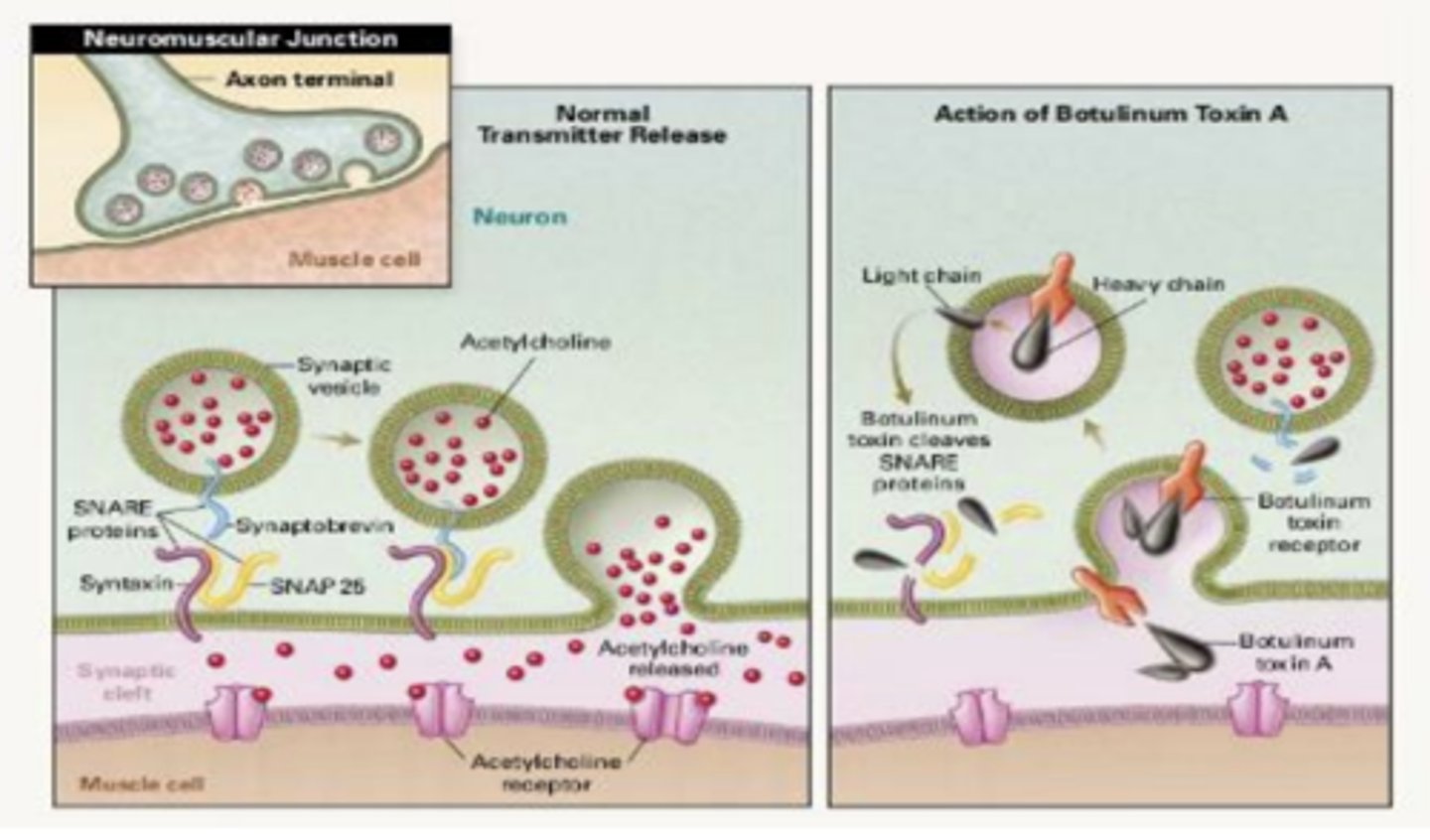
Botulinum Toxin Mechanism of Action
• Toxin heavy chain binds to receptors on membrane of presynaptic neuron
• Toxin subunit enters neuron via endocytosis. Initially found only in new, empty vesicles
• Light chain of toxin escapes acetylcholine vesicles, enters cytoplasm and destroys SNARE complex. SNARE complex is necessary for vesicular release of acetylcholine, allowing toxin works as an indirect antagonist, by interfering with vesicular release of acetylcholine