Comprehensive Study Guide on Esophagus, Stomach, and Nutrition in Surgery
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
88 Terms
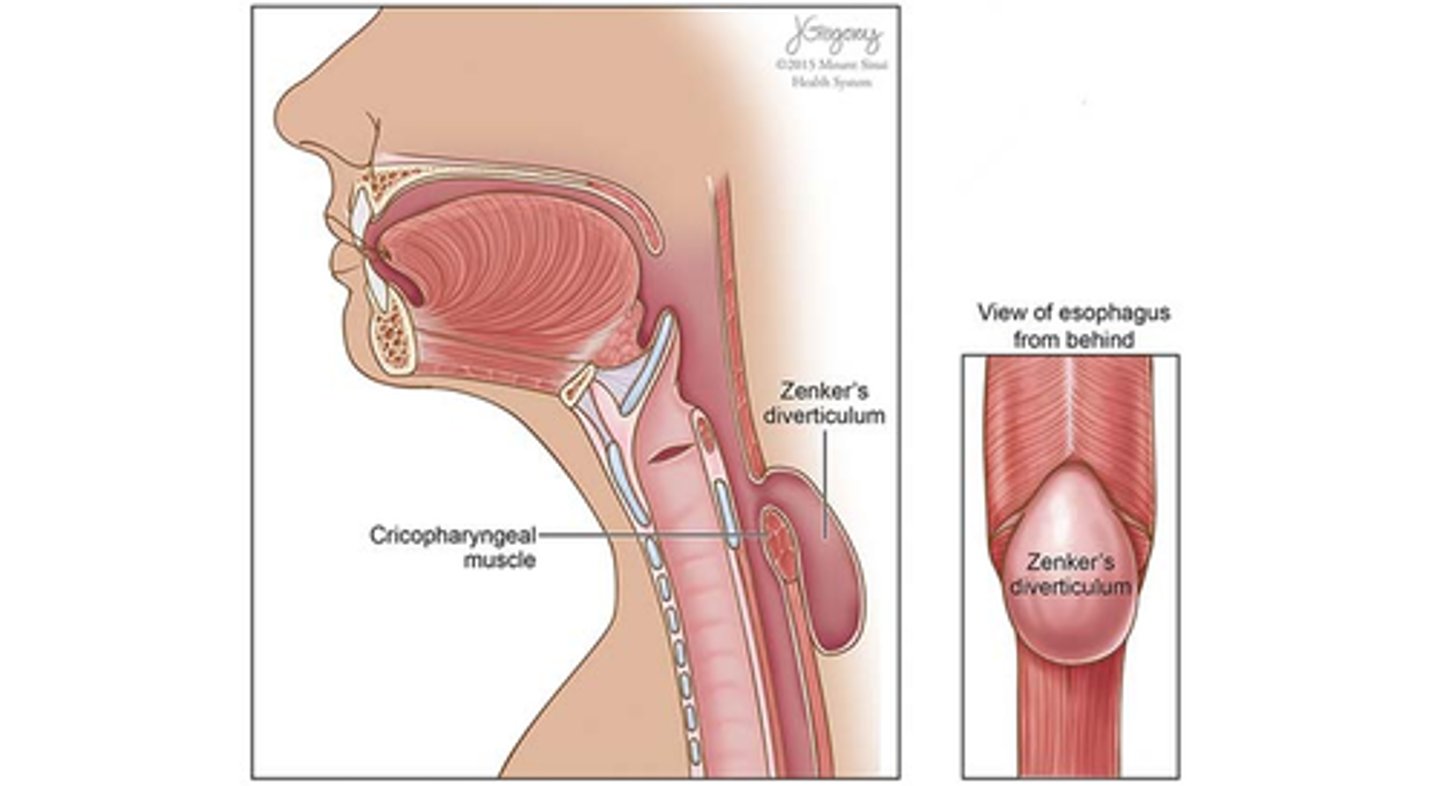
Between what muscles do Zenker's diverticulum develop?
esophagus & cricopharyngeus muscle
MC location perforation in Boerhaave's syndrome
lower thoracic esophagus
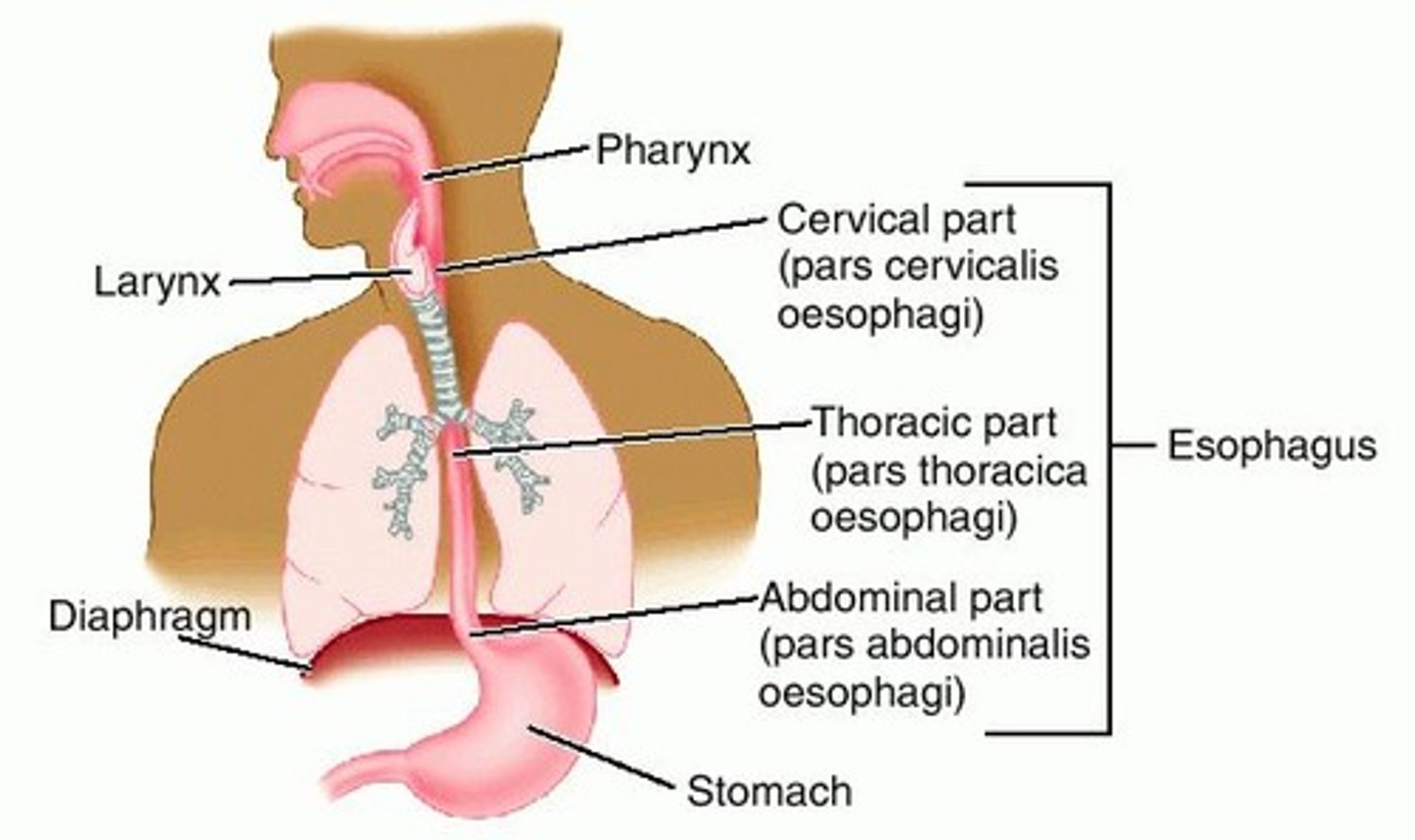
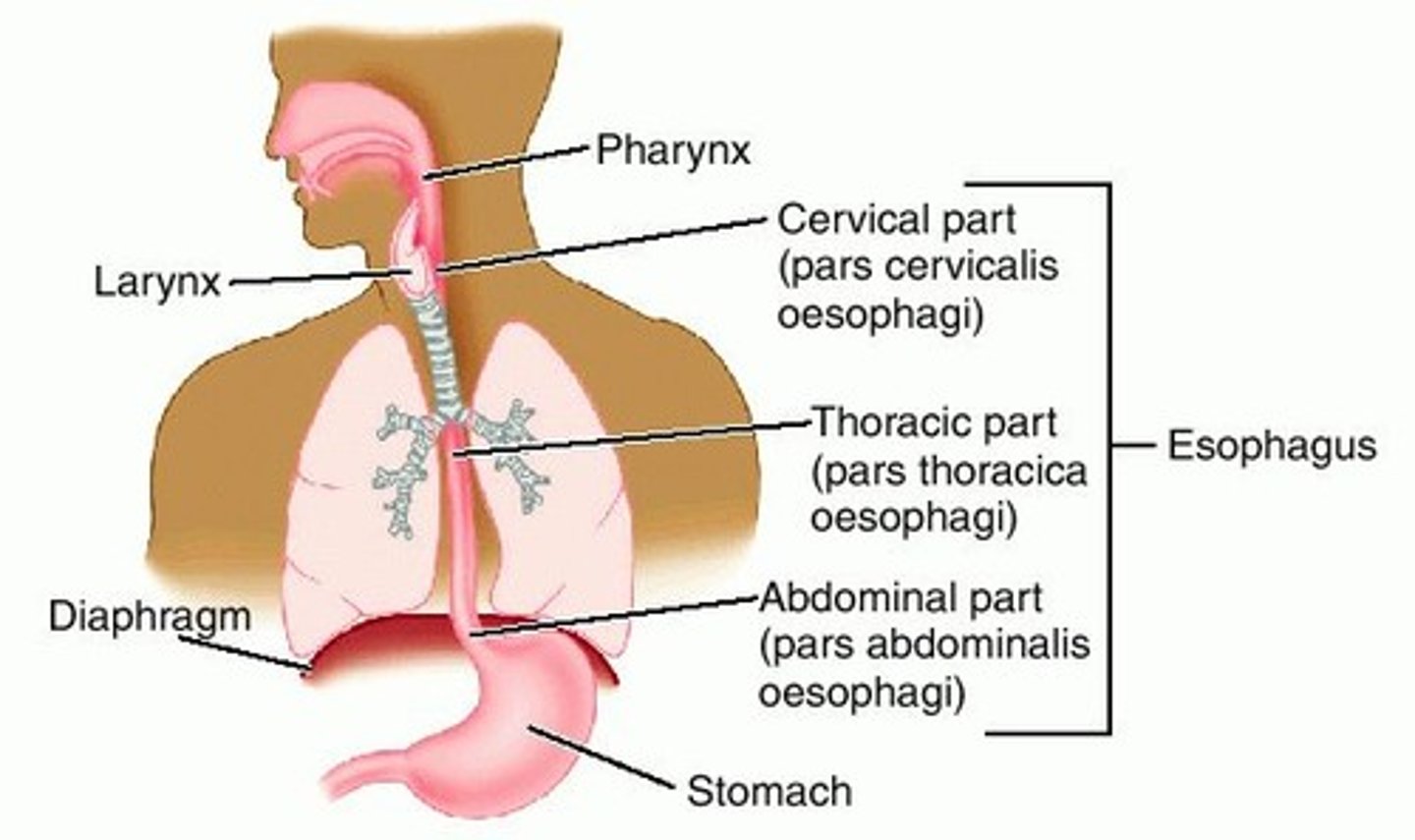
parts of esophagus
cervical, thoracic, abdominal
The LES is a zone of high
pressure
Early sign of carotid hematoma is
dysphagia followed by hoarseness
Substernal burning discomfort may radiate to epigastrium or sternal notch
pain occurs 1-2 hrs AFTER eating
worse when pt lies down at night or after meal
GERD
Medical tx GERD
PPIs and H2 blockers
When may surgery be indicated for GERD?
pts dependent on medical tx for sx relief
Dx GERD (3)
endoscopy
24 hr pH monitoring
measurement of LES pressure/Manometry
Gold standard dx GERD
24 hour pH monitoring
Condition in which tubular esophagus is lined with columnar rather than squamous epithelium
intestinal metaplasia within sphincter-- loss of LES function --> free reflux & progressive mucosal injury
Barrett's esophagus
Complications of GERD (3)
erosive esophagitis, stricture, Barrett's
Tx of high-grade dysplasia in Barrett's esophagus
Esophagectomy
(40-50% pts will have invasive CA)
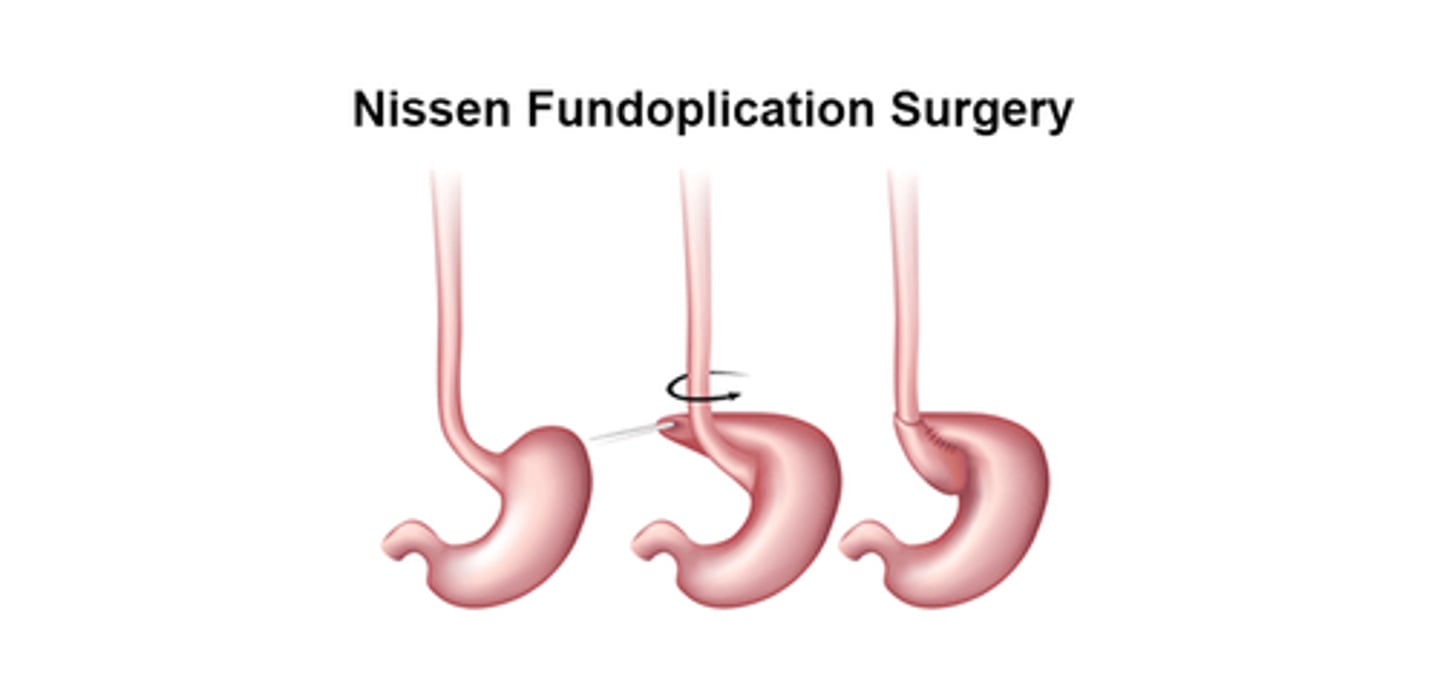
Surgery of choice GERD
laparoscopic Nissen Fundoplication
Benign esophageal tumors (2)
Leiomyoma & Hemangioma
MC benign esophageal tumor
Leiomyoma
MC malignant esophageal tumor
SCC
2 types of malignant esophageal tumors
SCC (MC) & adenocarcinoma
MC symptom esophageal carcinoma
dysphagia
Test of choice esophageal carcinoma
barium swallow & endoscopic evaluation
Definitive dx Esophageal Carcinoma
endoscopy with bx
If lymphadenopathy for esophageal carcinoma exists, what should be performed?
If nodes are positive, what is the prognosis?
FNA
6-9 month survival
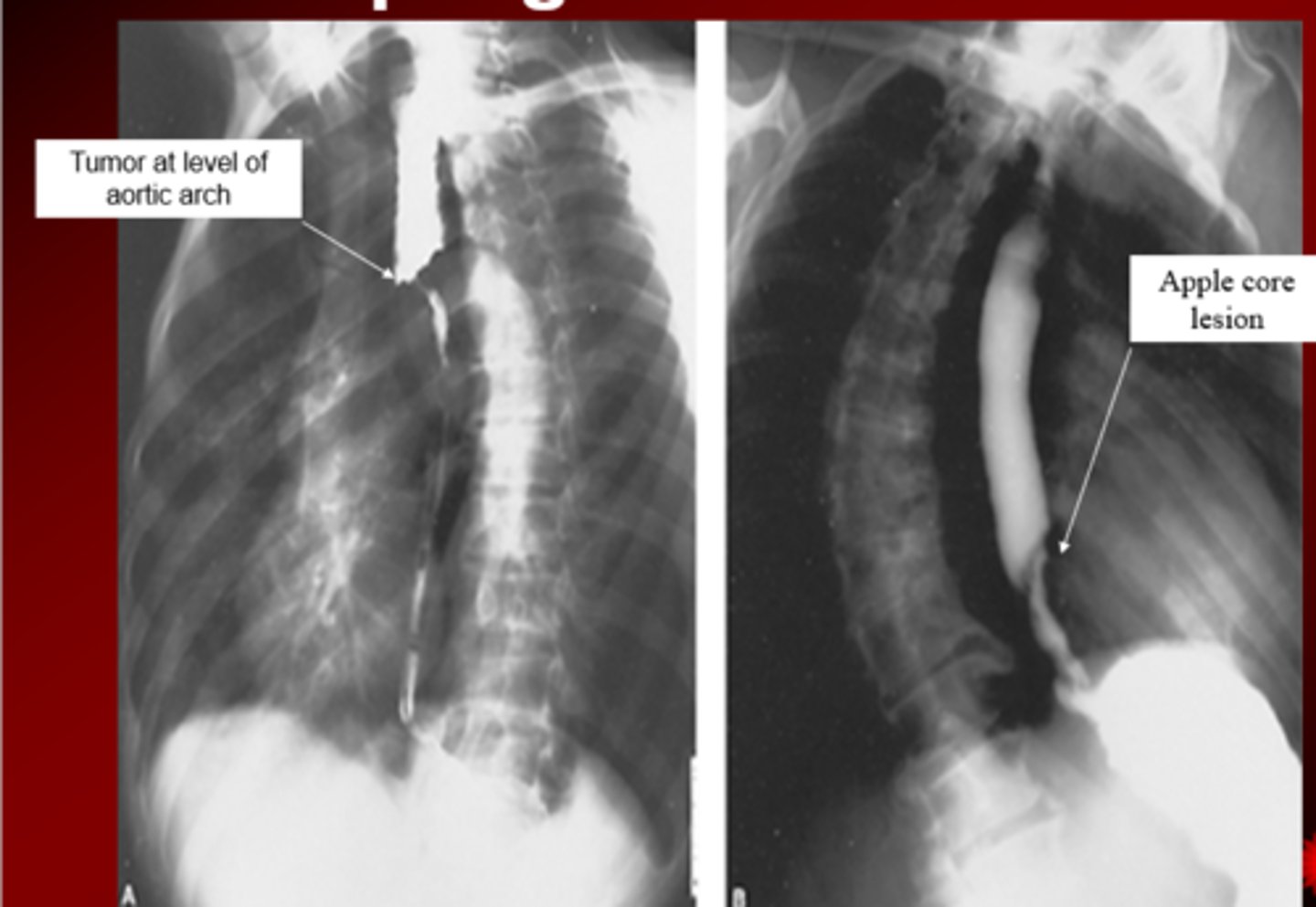
Mucosal irregularity & shelf of tumor is consistent with (SCC/adenocarcinoma)
SCC
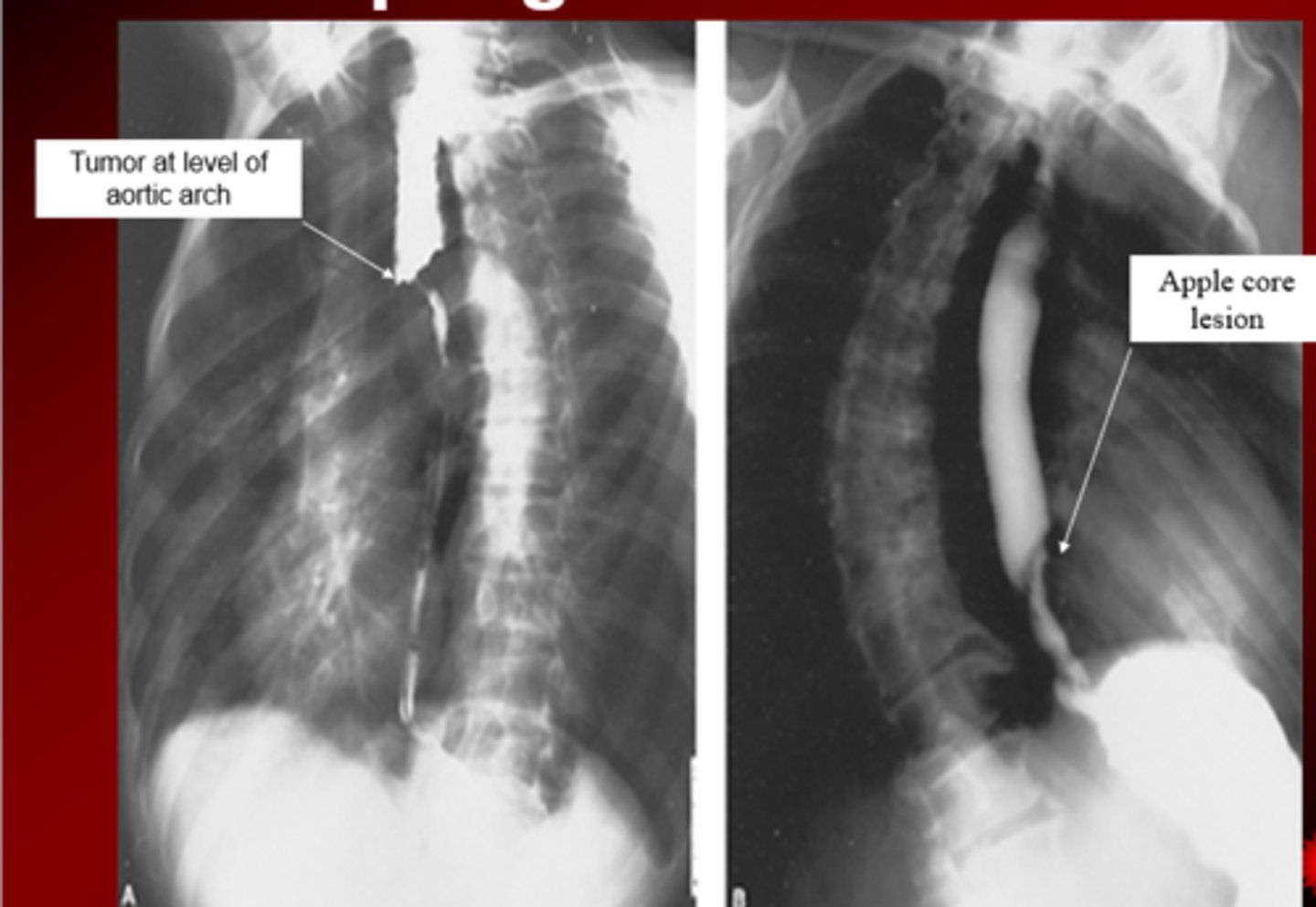
Lesion at GE junction is consistent with (SCC/adenocarcinoma)
adenocarcinoma
Esophageal carcinoma palliative tx
- Radiation
- intubation & stenting (<6 months to live)
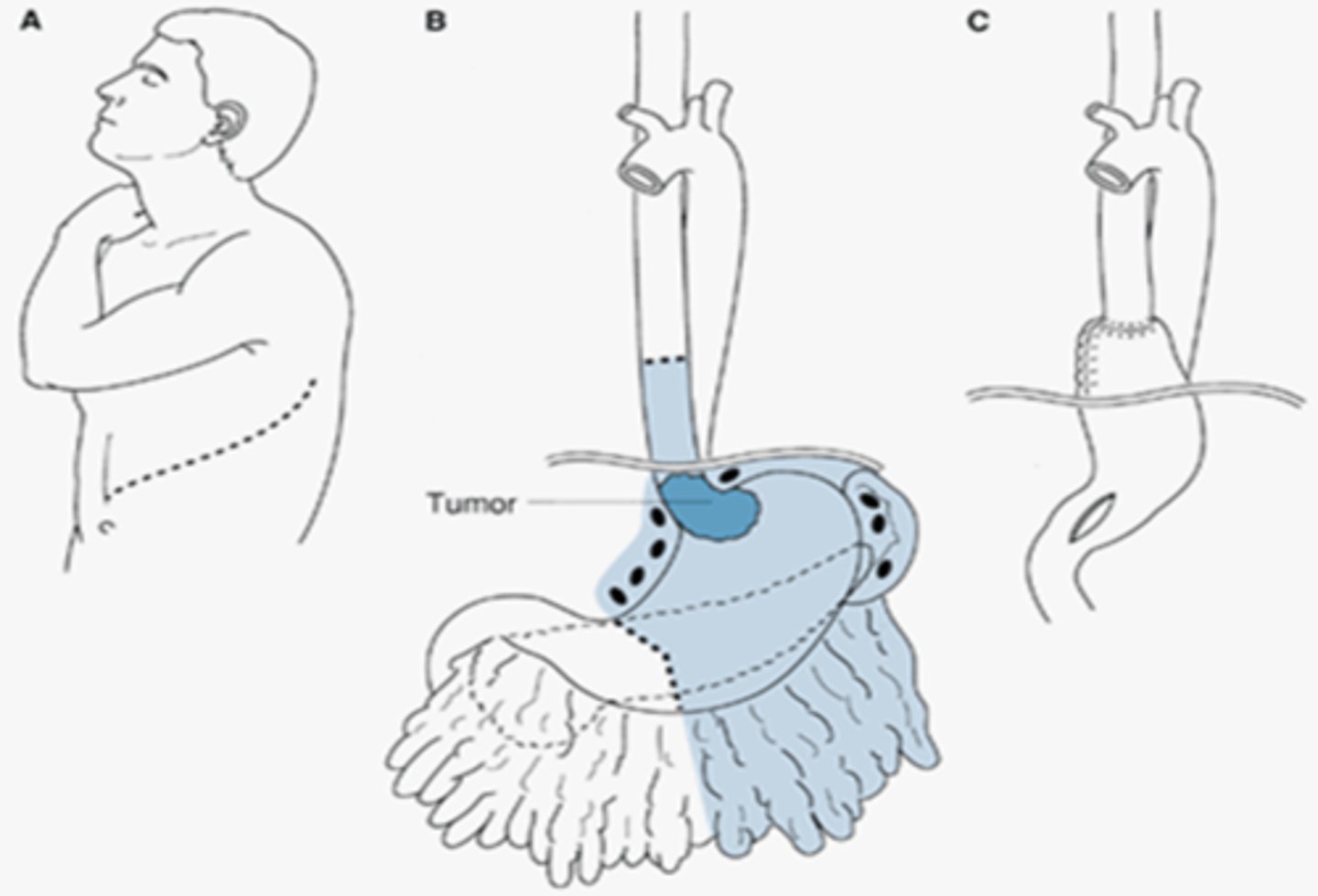
- transthoracic resection
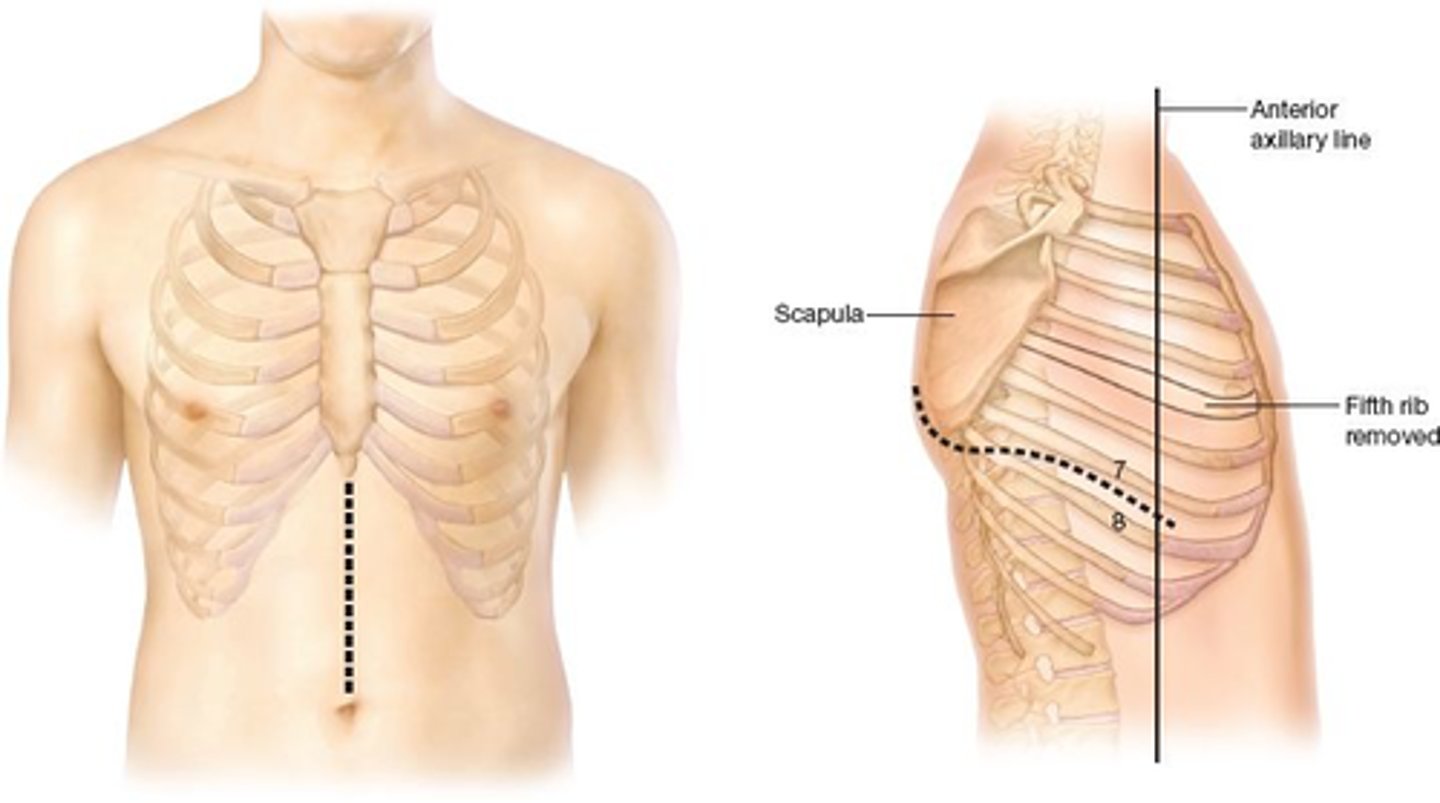
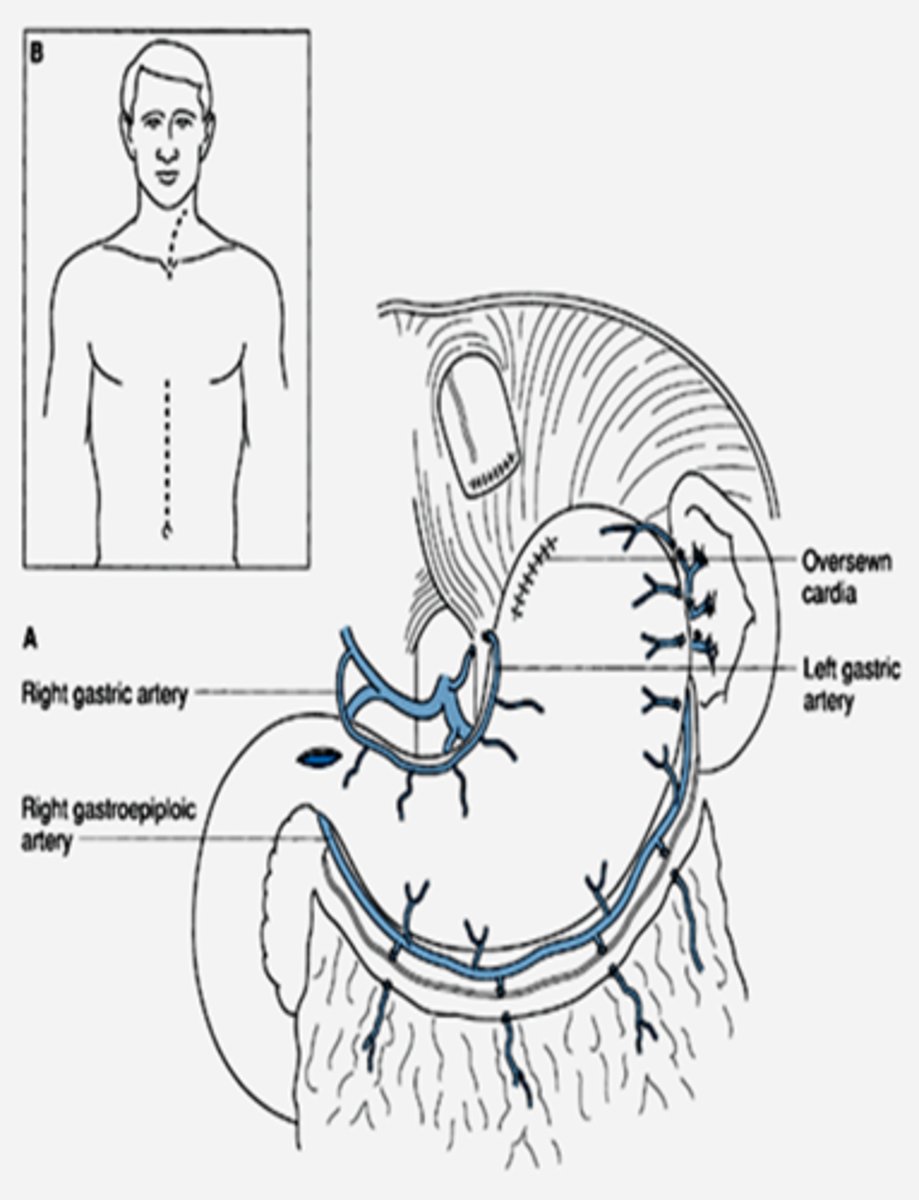
Transthoracic resection
(distal lesions- CA of distal esophagus & cardia)
pull stomach up & use as conduit more so than digestive organ--> add chest tube or pigtail catheter--> re-expand lung and ensure no leak from anastomoses--> swallow study (no leak- can remove tube)
removal is of blue pt in picture
Transthoracic resection
(proximal lesions-- middle or upper 1/3 esophagus tumors)
aka Ivor Lewis Esophagectomy
Pull stomach into chest, 1-2 pigtail catheters/chest tubes to re-expand lung, drainage for leak of anastomoses
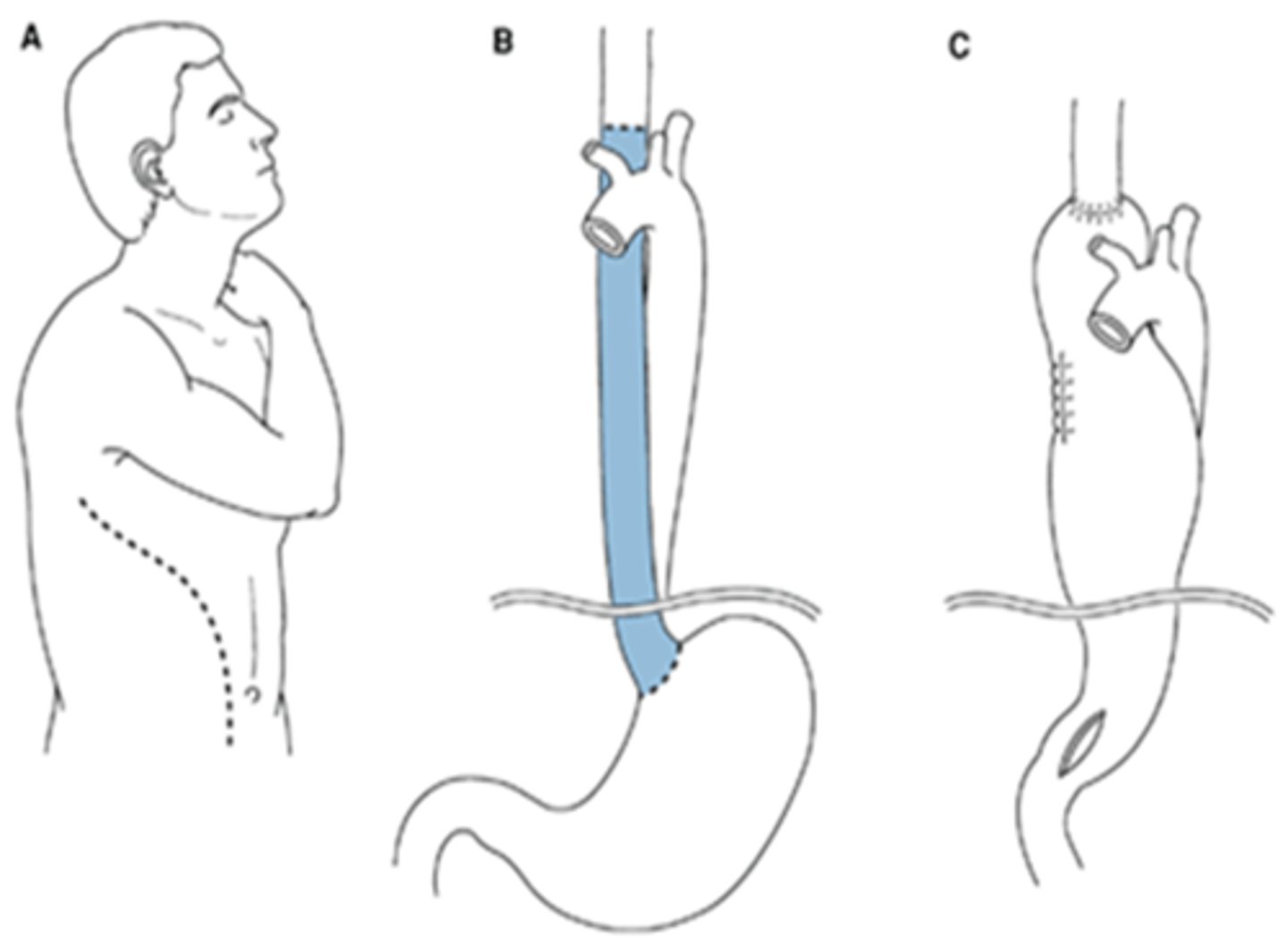
Ivor Lewis Esophagectomy aka transthoracic esophagectomy requires what two incisions
Abdominal incision & right thoracotomy
What surgical approach for esophageal carcinoma minimizes poor results associated w/ transthoracic resection
Transhiatal resection
Why are there less poor results with transhiatal resection for esophageal CA?
anastomoses in the neck are less likely to break
Unlike transthoracic resection, Transhiatal resection involves incisions of the ______________ and _______________
abdomen, neck
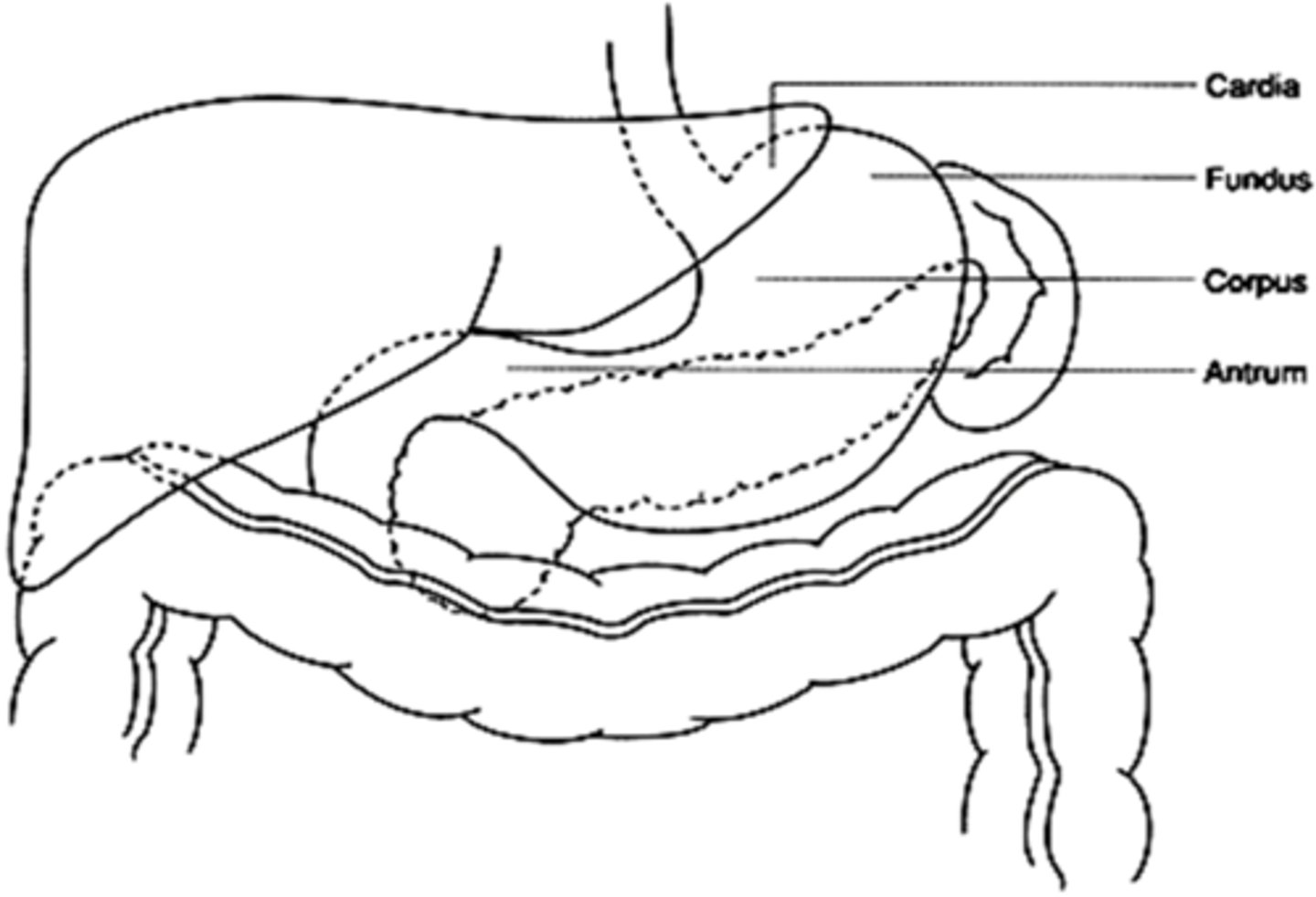
Region of stomach distal to GE junction
cardia
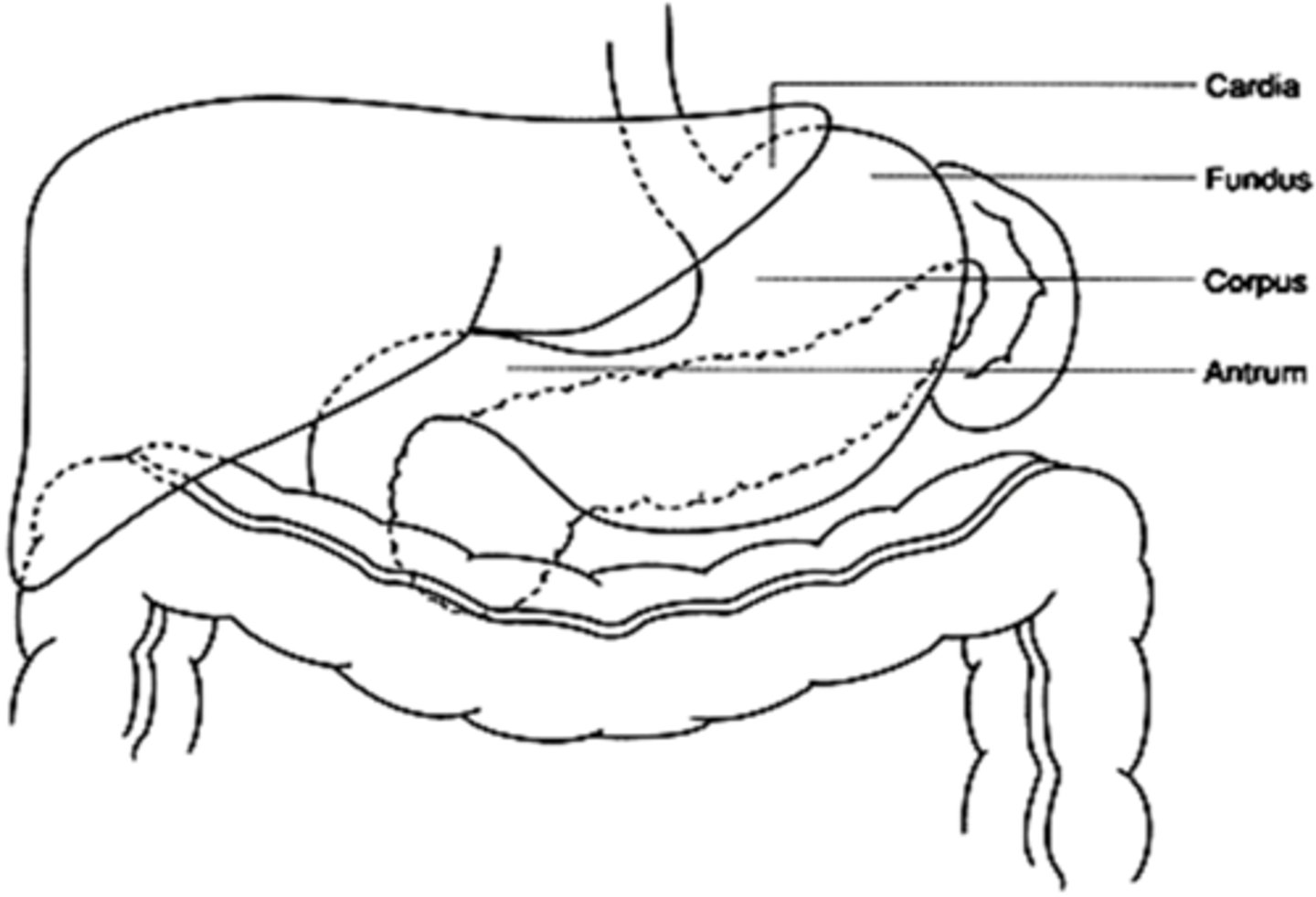
Portion of stomach above and left to GE junction
fundus
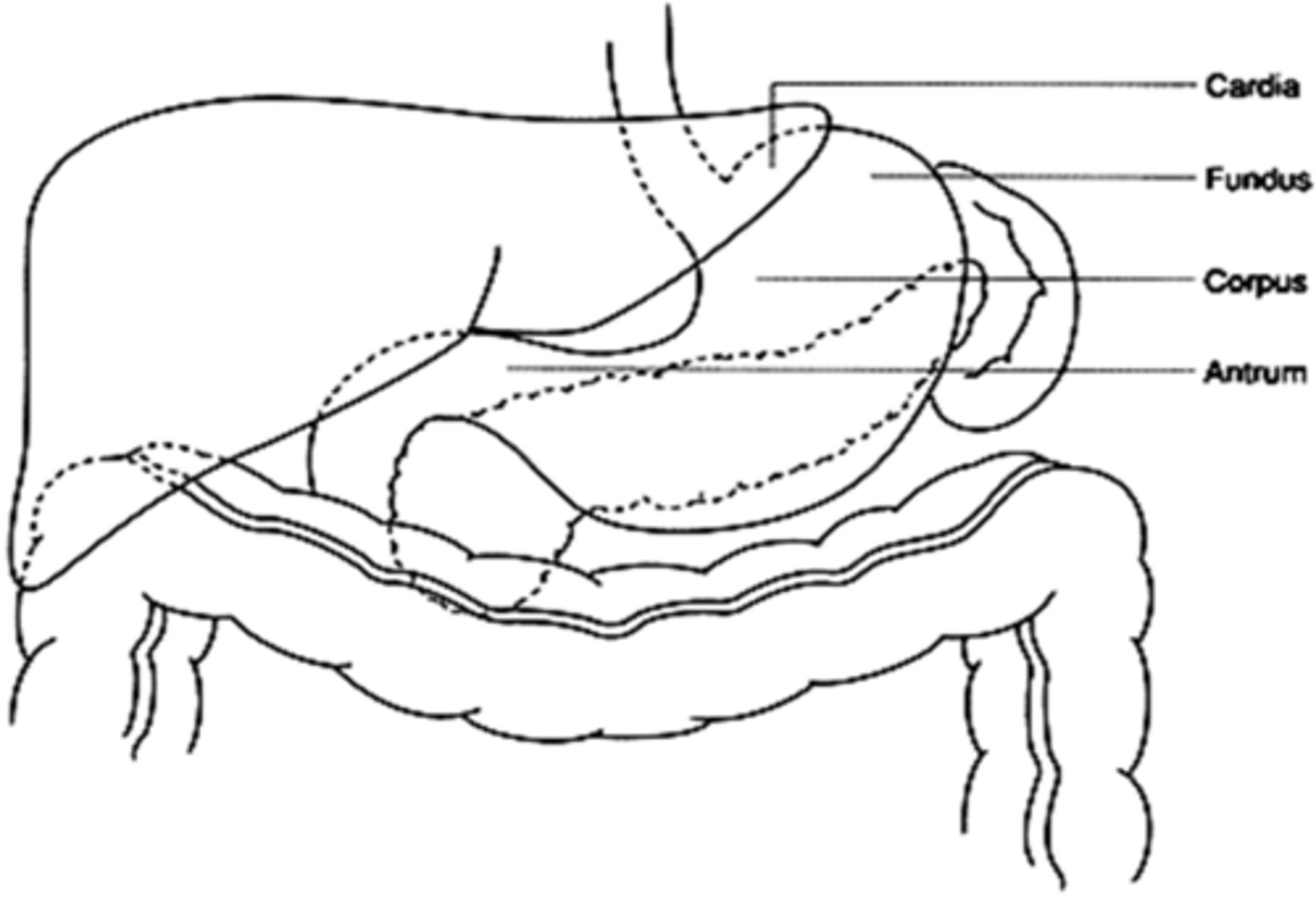
Gastric ______________ is bounded distally by the pylorus
antrum
(T/F) stomach is highly vascular
True
Lymphatic drainage of the stomach mimics ______________ supply; therefore, diseases that spread through lymphatics extend to distal ______________ ____________ quickly
blood, lymph nodes
90% of Vagus is (afferent/efferent) from GI tract to CNS
afferent
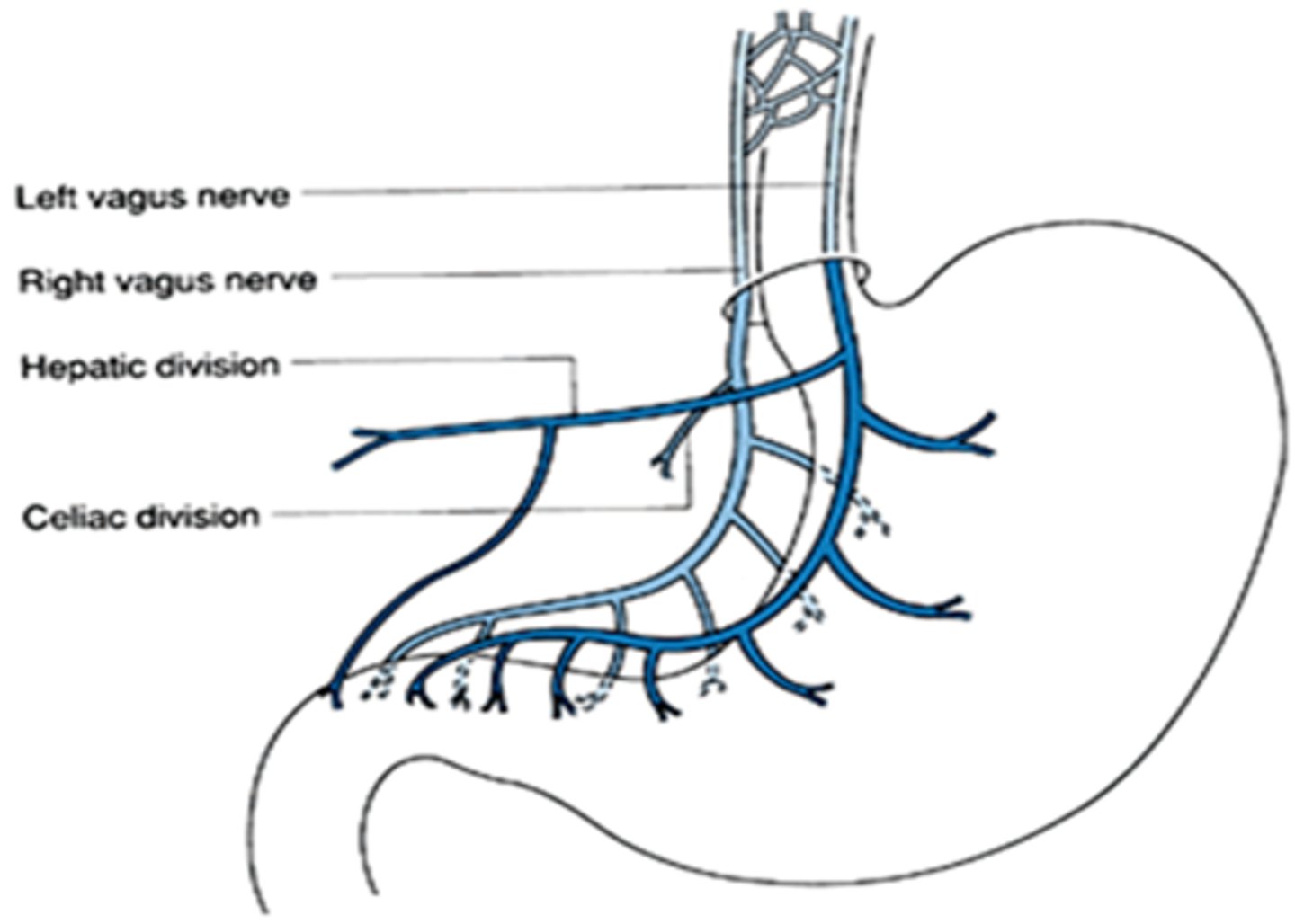
NT of efferent vagal neurons
ACh
Tx of PUD is primarily (surgical/medical)
medical
MCC PUD
H. pylori
Risk factors PUD
smoking, NSAIDs, ASA,
Pts w/ PUD complain of burning, stabbing, gnawing ____________________ pain
epigastric
Gold standard dx PUD
endoscopy
PUD medical tx
PPI + abx
PPI (omeprazole)
+ clarithromycin
+ metronidazole/ amoxicillin
x 7-14 d
H2 blockers
Sucralfate
Antacids
Surgical tx of ulcers is indicated when?
complicated ulcer DZ--> hemorrhage, perforation, obstruction
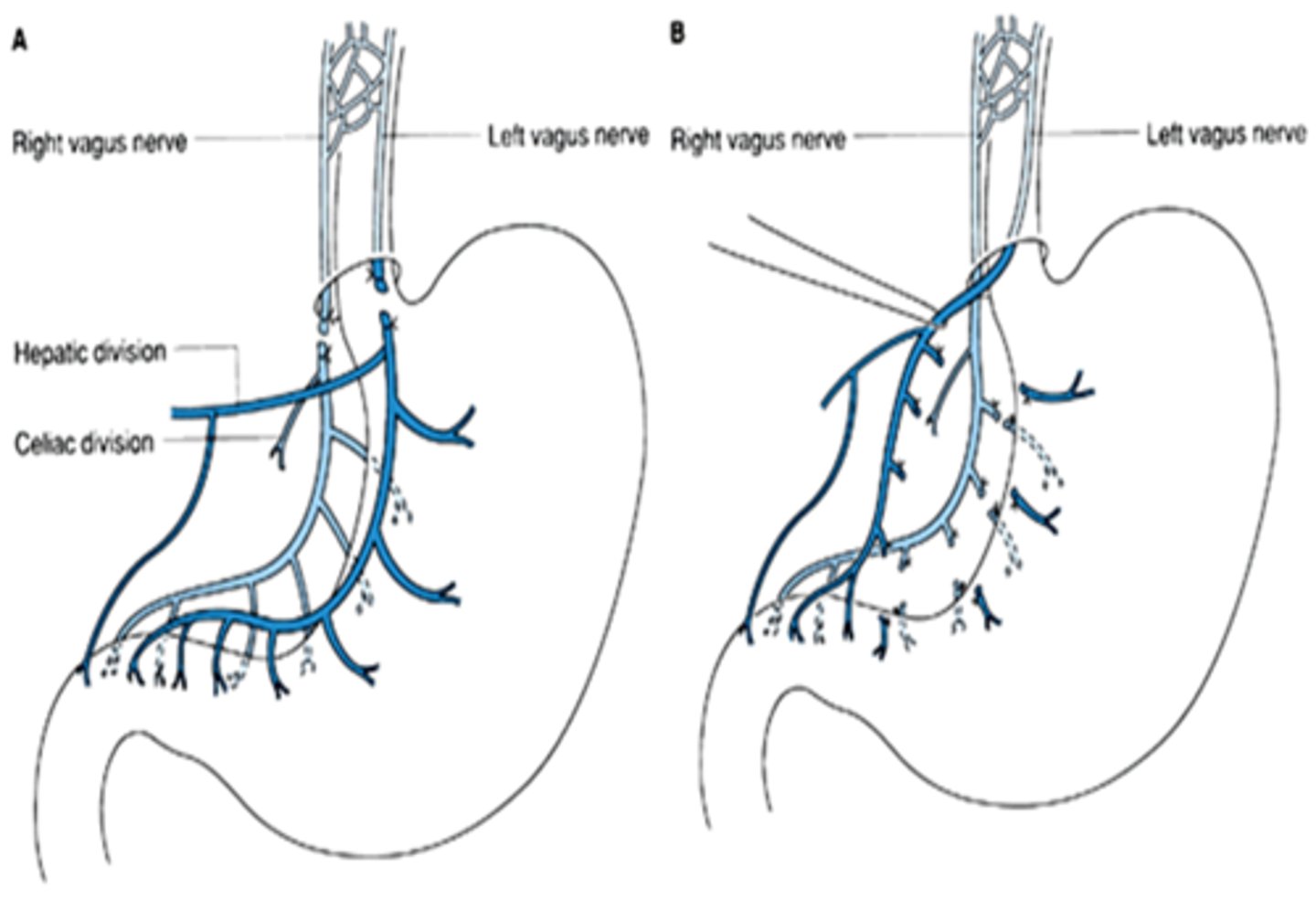
Surgical procedures ulcers (3)
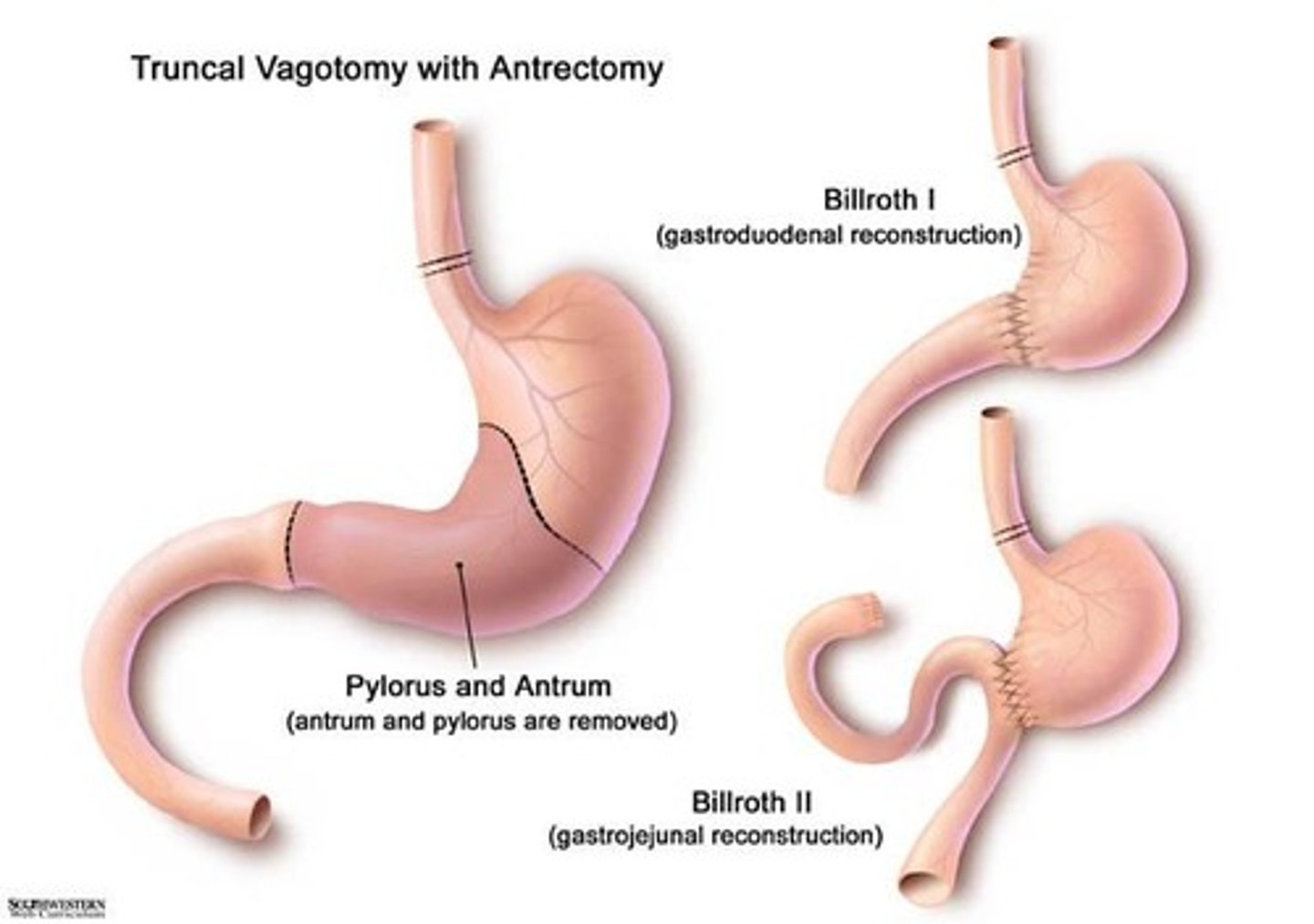
- Truncal vagotomy + drainage (pyloroplasty)
- Truncal vagotomy + antrectomy** procedure of choice!
(Billroth I and II)
- Proximal gastric vagotomy
Ulcer procedure involving denervation & elimination of sphincteric function
truncal vagotomy & drainage
Most definitive surgical tx ulcers
truncal vagotomy & antrectomy
Ulcer procedure that reduces receptive gastric relaxation (emptying of liquids faster), affects acid producing parts of stomach not the sphincter
proximal gastric vagotomy
Billroth I
Gastroduoden-ostomy
Attaches remaining stomach to the duodenum
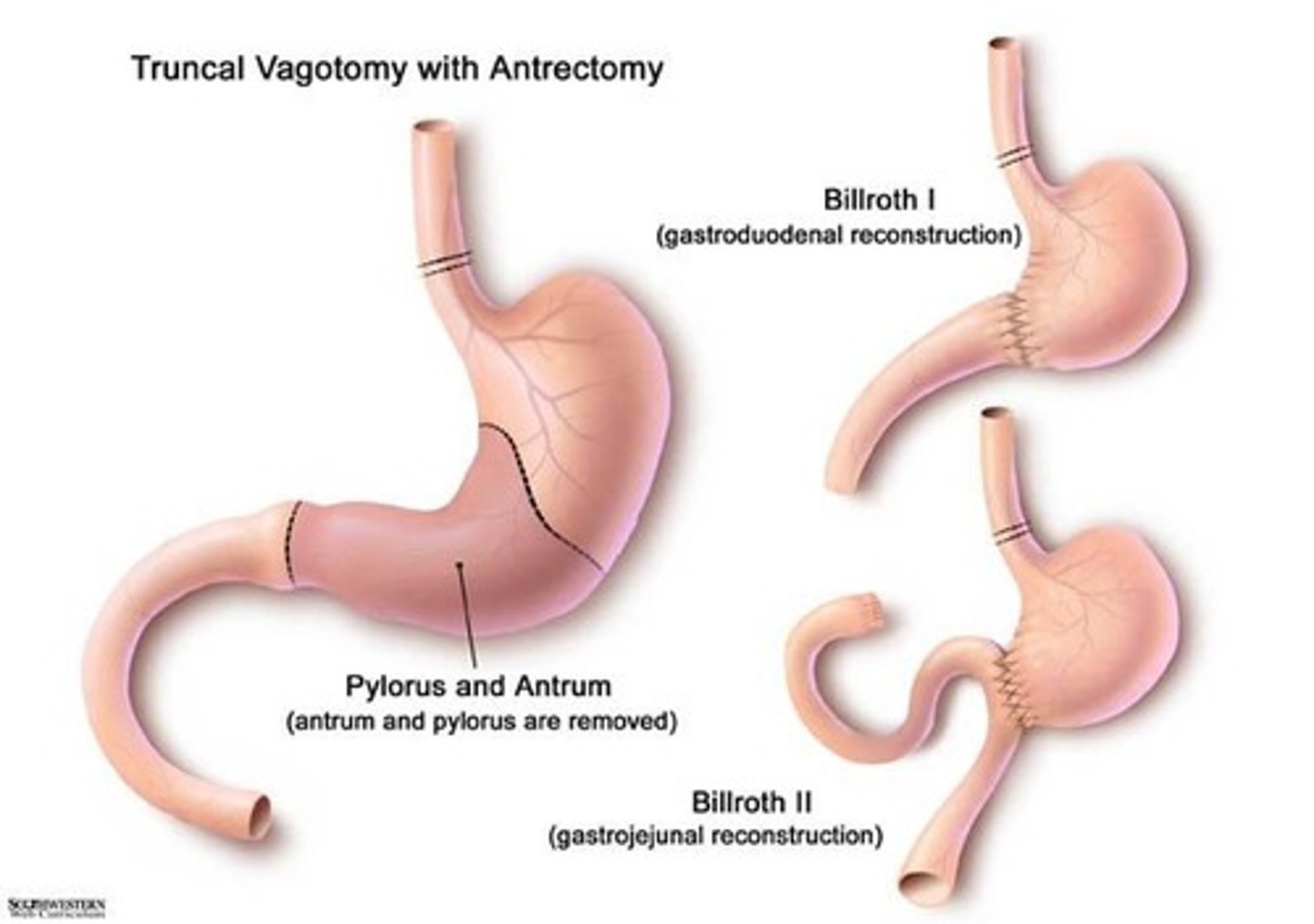
Billroth II
Gastrojejunostomy
Which is preferred- Billroth I or II?
Billroth I
...but more difficult
Which is easier- Billroth I or II?
Billroth II
Leading cause of death related to ulcer disease
upper gastrointestinal hemorrhage
What is both diagnostic and therapeutic for UGIB?
endoscopy
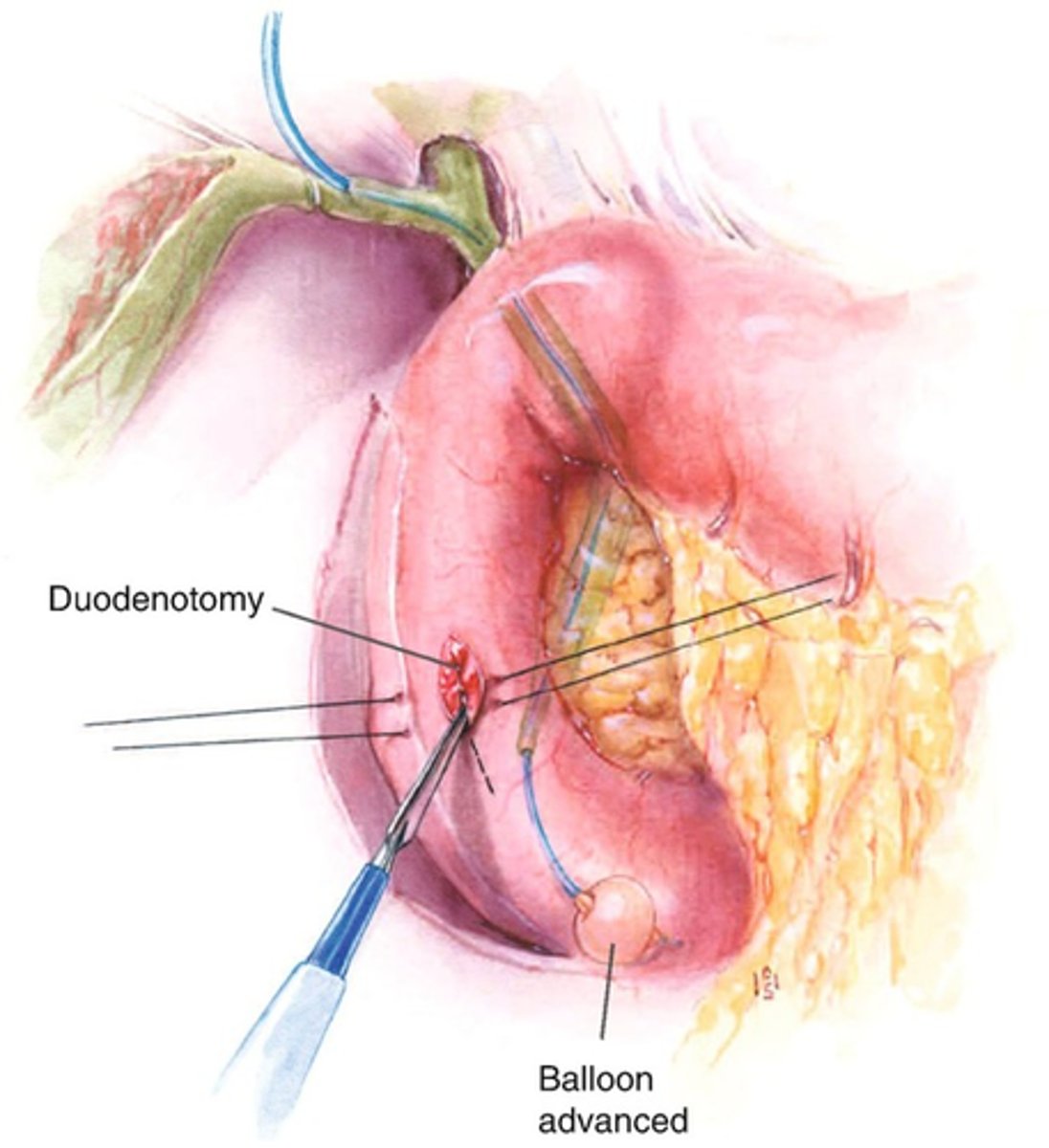
Surgical tx UGIB
duodenotomy
+ direct ligation of bleeding vessel in ulcer base
+ procedure to reduce acid production (truncal vagotomy and pyloroplasty
OR truncal vagotomy + antrectomy)
sudden severe epigastric pain, may radiate to right scapula
duodenal perforation
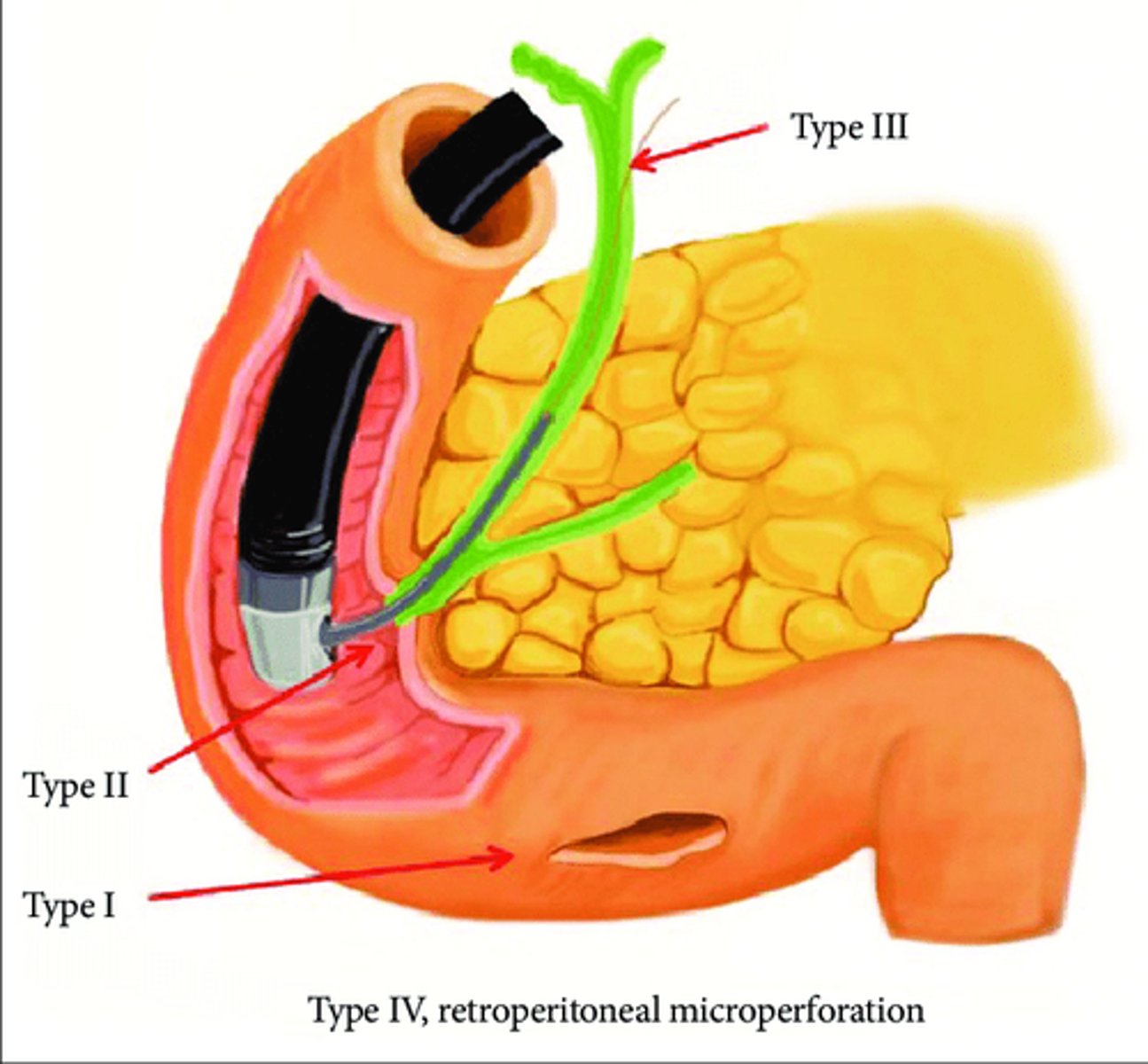
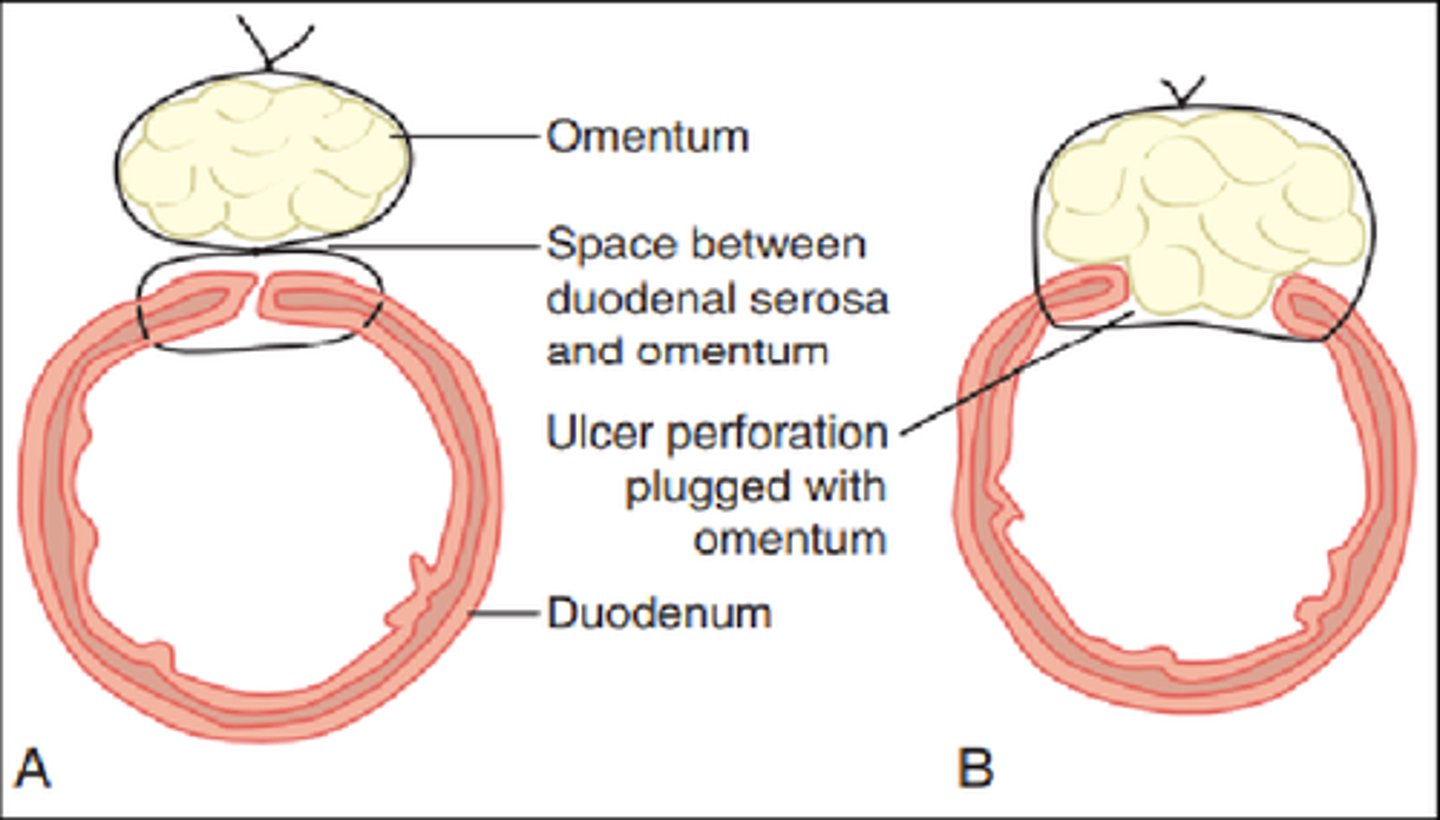
Surgical tx Duodenal Perforation
omental patch (Graham patch)
+ tx for H. pylori and secretory agents
How does Graham patch procedure heal duodenal perforation?
mesenteric stem cells are used to heal rupture
Test of choice and treatment of gastric ulcer
endoscopy w/ biopsy (r/o gastric carcinoma)
Risk factors Gastric cancer
- H-pylori
- Chronic gastritis
- Adenomatous polyps
Gastric CA diagnosis
endoscopy w/ bx
- Barium studies
- CT
What lymph nodes are usually affected in gastric CA?
virchow's
sister mary joseph's
irish
Surgical tx gastric carcinoma
Laparoscopy/ Laparotomy
- subtotal gastrectomy w/ gastrojejunal reconstruction
- total gastrectomy w/ esophagojejunostomy
- esophago-gastrectomy w/ anastomosis in cervical or thoracic position
50% of gastrointestinal lymphomas occur in the _______________________
stomach
MC organ involved in extranodal lymphoma
stomach
Dx gastric lymphoma
endoscopy + biopsy
Surgery gastric lymphoma
partial/total gastrectomy
+ radiation & chemo
MC gastric sarcoma
Leiomyosarcoma
MC performed bariatric procedure
sleeve gastrectomy
To qualify for bariatric surgery an individual's BMI needs to be >__________ or ____________ with comorbid medical conditions
40, 35-40
Bariatric procedures
Restrictive
- LAGB (laparoscopic adjustable gastric banding)
- SG (sleeve gastrectomy)
Malabsorptive
- BPD (biliopancreatic diversion)
- DS (duodenal switch)
Combination
- Roux-en-Y gastric bypass
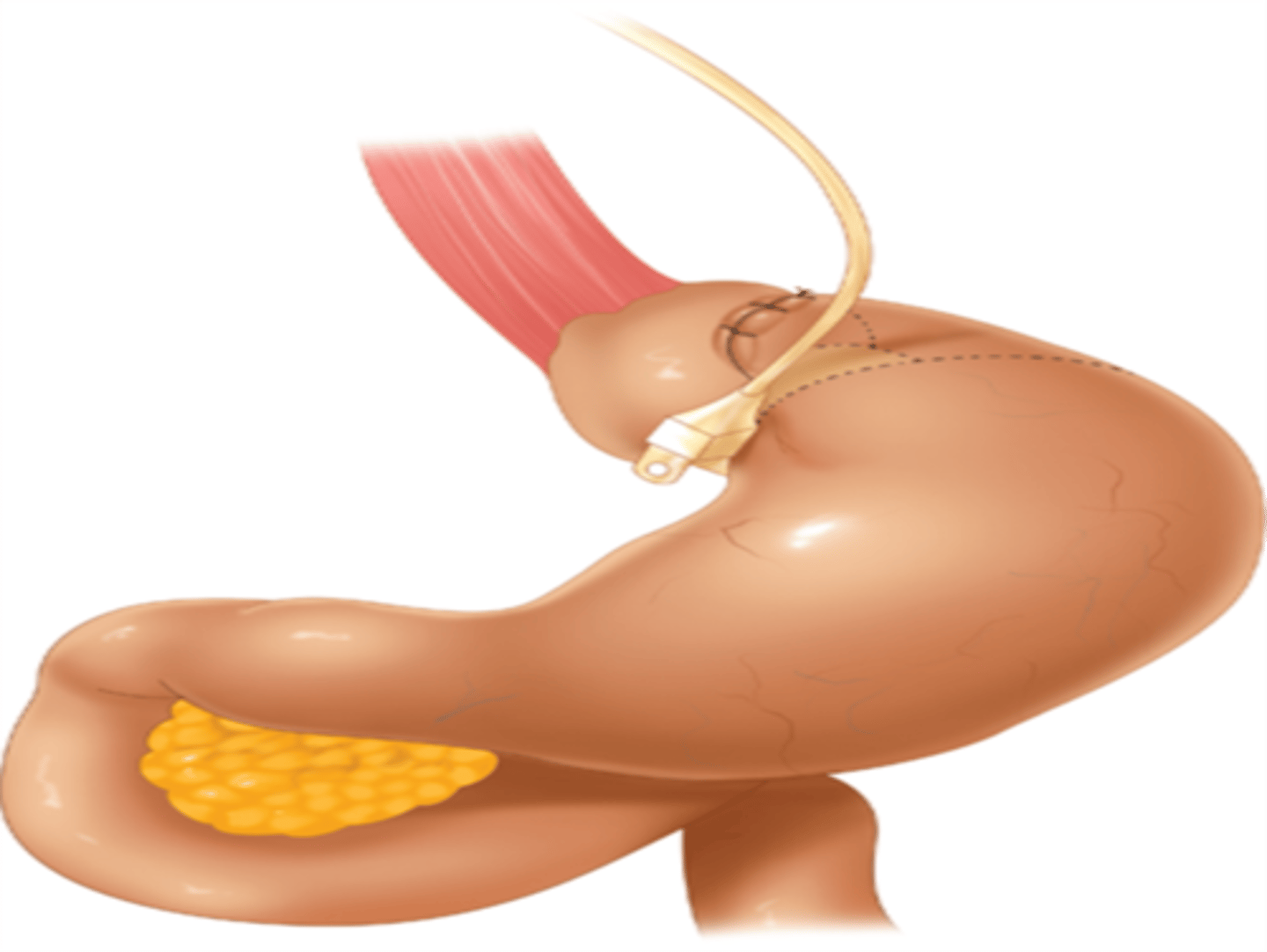
Involves placement of inflatable silicone band around proximal stomach
Band is attached to reservoir system & accessed through SQ placed port
LAGB (laparoscopic adjustable gastric band)
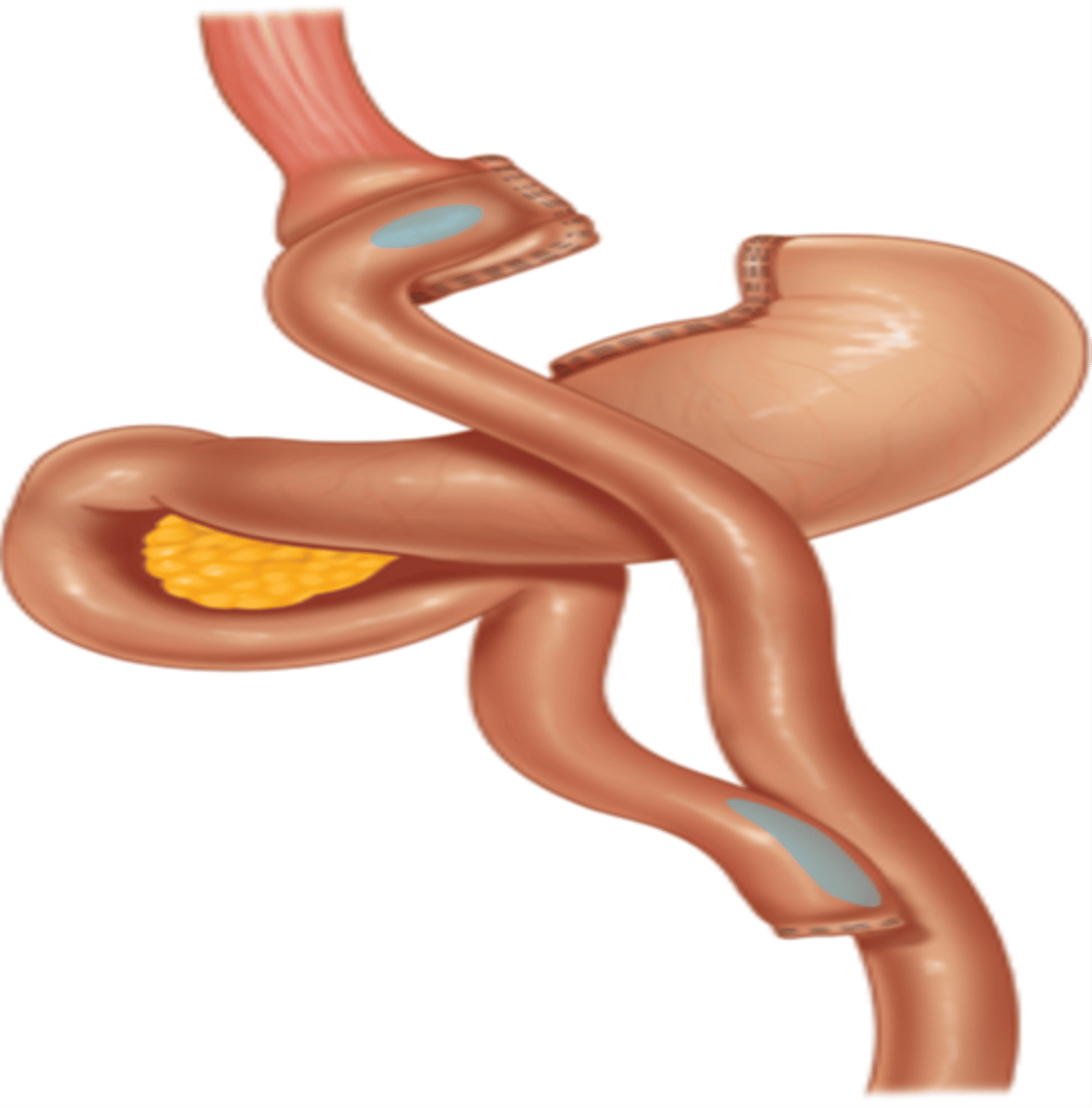
Roux-en-Y gastric bypass
Small pouch created from stomach
Part of small intestine bypassed
Restriction and malabsorption
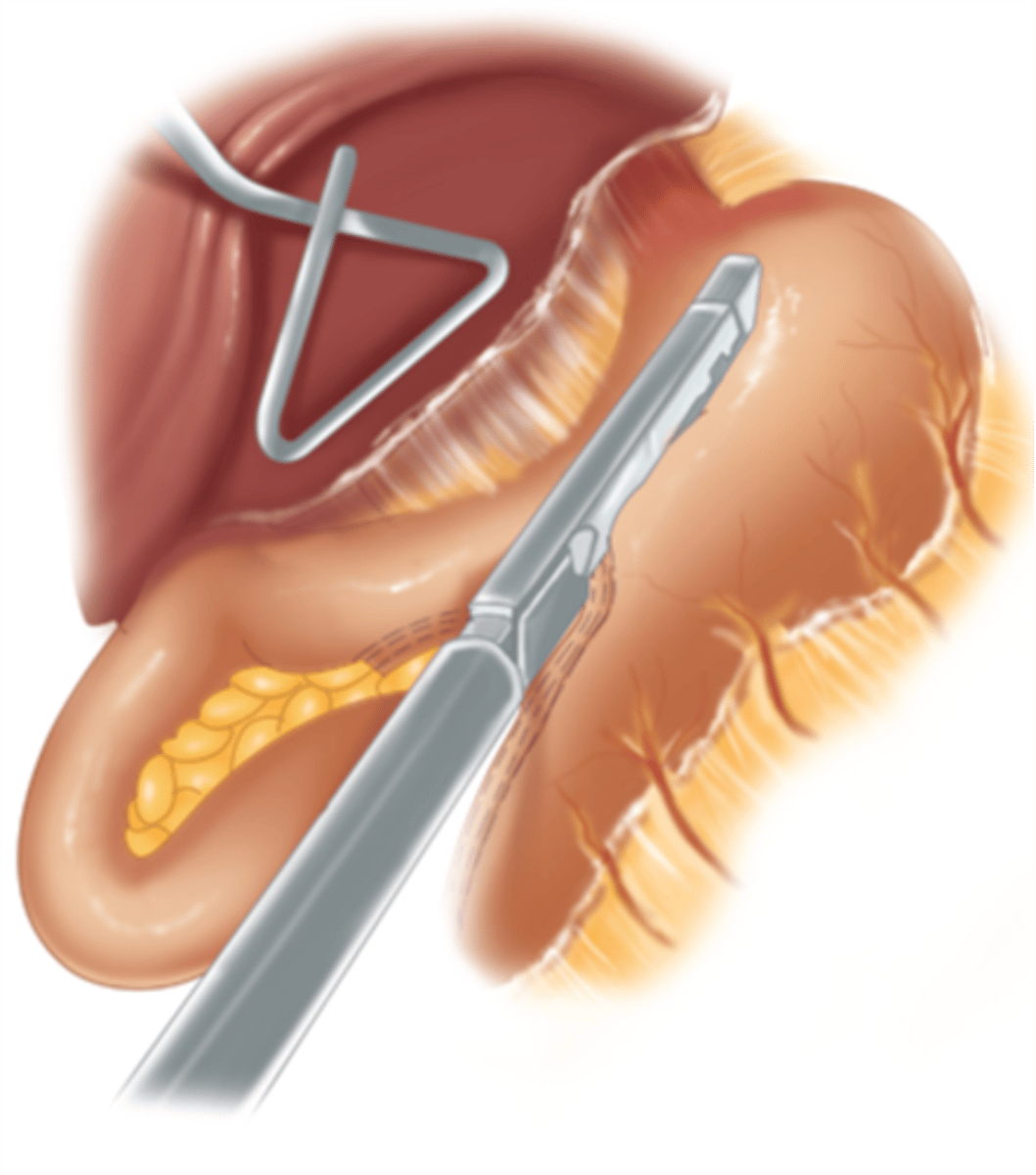
Sleeve gastrectomy
Portion of stomach is removed, leaving a banana-shaped stomach pouch
1st muscle to waste in malnutrition
temporal (jaw)
Laboratory data malntutrition
- albumin
- total lymphocyte count
- transferrin
- prealbumin
- retinol binding protein
Preferred form nutritional support
Enteral
What equation is used to assess energy expenditure?
Basal Energy Expenditure (B.E.E.)
Complications of TPN
- infection
- gut atrophy
- hyperglycemia
- fatty liver
- acalculous cholecystitis
TPN composition
Carbs, lipids, proteins, vitamins, minerals, electrolytes
NPC:Nitrogen ratio is useful in determining
severity of illness
The sicker the pt. is the (larger/smaller) the NPC:N ratio
smaller
TPN special formulations
Hepatic
- Branched chain AAs
Renal
- Low protein
Pulmonary
- Dec. carbs, inc lipids
Immune enhancing
- impact
Enteral nutrition benefits
- decreases brush border atrophy
- decreases translocation of bacteria
What enteral formulation is used as a standard tube feed preparation?
polymeric
What enteral formulation is used for septic/malnourished pts?
oligomeric
Impact vs Oxepa
(immune enhancing formula)
Oxepa lacks Arginine