Leadership Final
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
98 Terms
what is the first step of the crucial conversation model?
introduction:
-express your intention to have a productive conversation
-use a calm and friendly tone
-(ex): "I'd like to talk with you about something that has been bothering me. I hope we can have an open and constructive conversation to resolve this issue"
what is the second step of the crucial conversation model?
express your concern:
-state the problem: "the issue I would like to address is..."
-share your feelings: "when this happened, I felt...
-describe the impact: "this has impacted me..."
what is the third step of the crucial conversation model?
seek understanding:
-ask for their perspective: "I'd like to understand your perspective better. Can you tell me how you see this situation?"
-listen actively : "I hear you, and I appreciate your viewpoint"
-ask clarifying questions: "could you elaborate on..."
what is the fourth step of the crucial conversation model?
finding common ground:
-identify shared goals: "it seems like we both want..."
-brainstorm solutions: "what do you think we could do to address this problem together?"
-evaluate solutions: "let's consider the advantages and disadvantages of each option"
what is the fifth step of the crucial conversation model?
agree on next steps:
-propose a resolution: "I propose that we..."
-seek agreement: "do you agree with this plan, or is there something else you'd like to suggest?"
-set a follow up: "let's check in [specify when] to see how things are going and make any necessary adjustments"
what is laissez-faire leadership?
-takes a hands-off approach
-permissive with little or no control
-provides little direction
-does not criticize
what is situational/contingency leadership?
-suggests that no one leadership style is ideal for every situation; leader assesses the situation and group members, and selects the style or blending of styles best for the situation
-interrelationships between the group's leader and its members are influenced by the manager's ability to be a good leader
-determinants of leadership style include nature of the situation, skills of the manager, and abilities of the group members
-power associated with leadership and the task to be accomplished also influences it
what is servant leadership?
-puts serving others (including employees, customers, and the community) as the number one priority
-focuses on increased service to others rather than to oneself and the betterment of subordinates
what is authentic leadership?
-suggests that to lead, leaders must be true to themselves and their values and act accordingly
-people come to have faith and trust in these leaders
what is transactional leadership?
-clarifies roles and responsibilities
-uses rewards and punishments to achieve goals
-results orientated
what is transformational leadership?
-focuses on vision and empowering individuals to do and be the best they can be
-known to be caretakers and have long term vision
what is the difference between a manager and a leader?
-manager: the person who brings things about; the one who accomplishes, has the responsibility, and conducts
-leader: the person who influences and guides direction, opinion, and course of action; leadership is more dynamic than management
what is followership?
-the process whereby an individual accepts the influence of others to accomplish a common goal; a choice, not a must
-the capacity and willingness to follow a leader
-important skills include motivation, courage, service, dedication, work ethic, good judgement, and honesty
what are the types of hospital budgets?
-personnel budget
-operating budget
-capital budget
personnel budget
-developed for the number of people needed to produce the product, any costs of training them, their pay and benefits, and other factors involved
-largest of the budget expenditures in most hospitals; healthcare is labor intensive
operating budget
-budget for day-to-day expenses: reflects expenses that flex up or down in a predetermined manner to reflect variation in volume of service provided
-examples: rent or property purchase costs, advertising and marketing fees, licensing fees, utility costs, vehicle maintenance, direct materials (supply) cost
capital budget
-aid in decisions related to the purchase of long-term (> 5 years) assets that usually involve high-dollar expenditures (buildings, major equipment)
-equipment that is not used daily, more expensive than operating supplies
what is revenue?
source of income or the reward for providing a service to the patient
what are sources of revenue for hospitals?
-operating revenue = the money earned directly by providing health care services to patients; largest and most important source of hospital revenue
-grants, donations, sale of assets
define the following terms:
-deductible
-copay
-coinsurance
-out-of-pocket maximum
-deductible: the amount you pay out-of-pocket before your insurance kicks in
-copay: a set fee you pay upfront before a covered medical service or procedure
-coinsurance: the percentage you pay for a service or procedure once you've met the deductible (ex: once you reach your $2000 deductible, you pay 20% for services and insurance pays 80%).
-out-of-pocket maximum: the most you will pay for covered services in a rolling year; once met, your insurance company will pay 100% of covered expenses for the rest of the year
who is covered under medicare?
-most adults age 65 and older
-some people with disabilities younger than age 65
-people who have end stage renal disease
what are the different parts of medicare and what is covered under each?
-part A: hospital insurance; inpatient hospital, inpatient skilled nursing facility, hospice, and some home health services
-part B: medical insurance; physician services, outpatient care, durable Medical Equipment (DME), lab and X-ray services, home health services, and many preventive services
-part C: medicare advantage; medicare-approved private insurance companies who provide all Part A and Part B services and may provide prescription drug coverage and other supplemental benefits (dental, vision, hearing)
-part D: prescription drug benefit: medicare-approved private insurance companies provide outpatient prescription drug coverage
who is covered under medicaid?
-people with disabilities
-low income adults
-elderly people
-children
-pregnant women
-eligibility, scope of services, and payment set by each state
what is managed care? what is the most common type?
-variety of healthcare plans designed to contain the cost of health care services delivered to members while maintaining the quality of care
-managed care = price for specific procedure or service
-HMO = one of most common types; network of providers who have agreed to accept payment at a certain level for any services they provide; keeps monthly premiums and coinsurance more affordable, but does not cover out-of-network care
what are the 5 rights of delegation?
1. right task (can the task be delegated?)
2. right person
3. right circumstances (appropriate patient setting, available resources, consider relevant factors)
4. right directions/communication (clear/concise description)
5. right evaluation/supervision (appropriate monitoring, evaluation, intervention, and feedback)
what does SBAR stand for and what information should be included in each area?
-begins with the exact reason you are calling; usually for a change in patient status
S: situation (situation you want to discuss, what is happening right now, introduce self)
B: background (admitting diagnosis, list of current meds/allergies, most recent vitals, labs, synopsis of tx to date, code status)
A: assessment (any changes from prior assessments, patient condition unstable or worsening)
R: recommendation/request (specific treatments, tests needed, patient needs to be seen now)
what is the CURE method for clinical decision making?
-critical: patient situations that need immediate attention
-urgent: patient situations that must be addressed within a couple of hours
-routine: basic cares and tasks that must be performed on patients but only need to be completed by the end of the shift
-extra: extra cares or tasks that would be nice to do for the patient or family but are not necessary
-what is critical to do first? what is urgent for you to do next? what is basic or routine for you to do? what are some extra things about your unit or population that you should do?
what are the 10 things listed under the ANA scope of practice for RNs?
-assessment
-nursing diagnosis
-outcomes identification
-planning
-implementation
-coordination of care
-health teaching and health promotion
-consultation
-prescriptive authority and treatment (advanced practice)
-evaluation
how and when do nurses delegate?
-RN scope of practice & delegation guidelines determined by nurse practice act
-RN must determine the needs of the patient and whether those needs are matched by the knowledge, skills and abilities of the delegatee & can be performed safely; RN cannot delegate any activity that requires clinical reasoning, nursing judgment or critical decision making
-RN must ultimately make the final decision whether an activity is appropriate to delegate to the delegatee based on the 5 rights
-RN is giving the responsibility, but maintains accountability
what tasks may the RN delegate to a UAP (CNA, HHA, client care technician, surgical tech)?
tasks that are considered routine, that do not require substantial scientific knowledge/technical skill, that are considered safe for the client, and that have a predictable outcome
-taking vital signs
-measuring I & O
-client transfers
-ambulation
-bathing, feeding, gastrostomy feedings
-attending to safety
-weighing
-simple dressing changes
-suctioning of chronic tracheostomies
-basic life support (CPR)
what cannot be delegated to UAPs?
-assessment
-interpreting data
-making a nursing diagnosis
-creating a nursing care plan
-evaluating care effectiveness
-care of invasive lines
-administering parenteral medications
-inserting NG tubes
-client education
-performing triage
-giving telephone advice
what tasks may the RN delegate to an LPN?
-administering PO medications
-inserting a urinary catheter
-administering enteral tube feedings
-dressing changes, trach care, suctioning
-reinforcing RN's teaching
what tasks cannot be delegated to an LPN?
-independent assessment or client education
-administering high-risk medications
-administering IV push medications, titrating medications
-client admission or discharge
what is a nursing care delivery model?
-the method used to provide care to patients
-determines who does what, who knows what, who has the authority to make decisions (like delegation), who is the team leader
what are the 4 main types of nursing care delivery models?
-total patient care
-functional nursing
-team nursing
-primary nursing
what is total patient care nursing? (what are the pros/cons, where is this model commonly seen?)
-oldest method of nursing; model in which the nurse plans, organizes and performs all care
-common areas = ICU, PACU
-provides highest degree of autonomy for nurses, but is arguably not cost effective
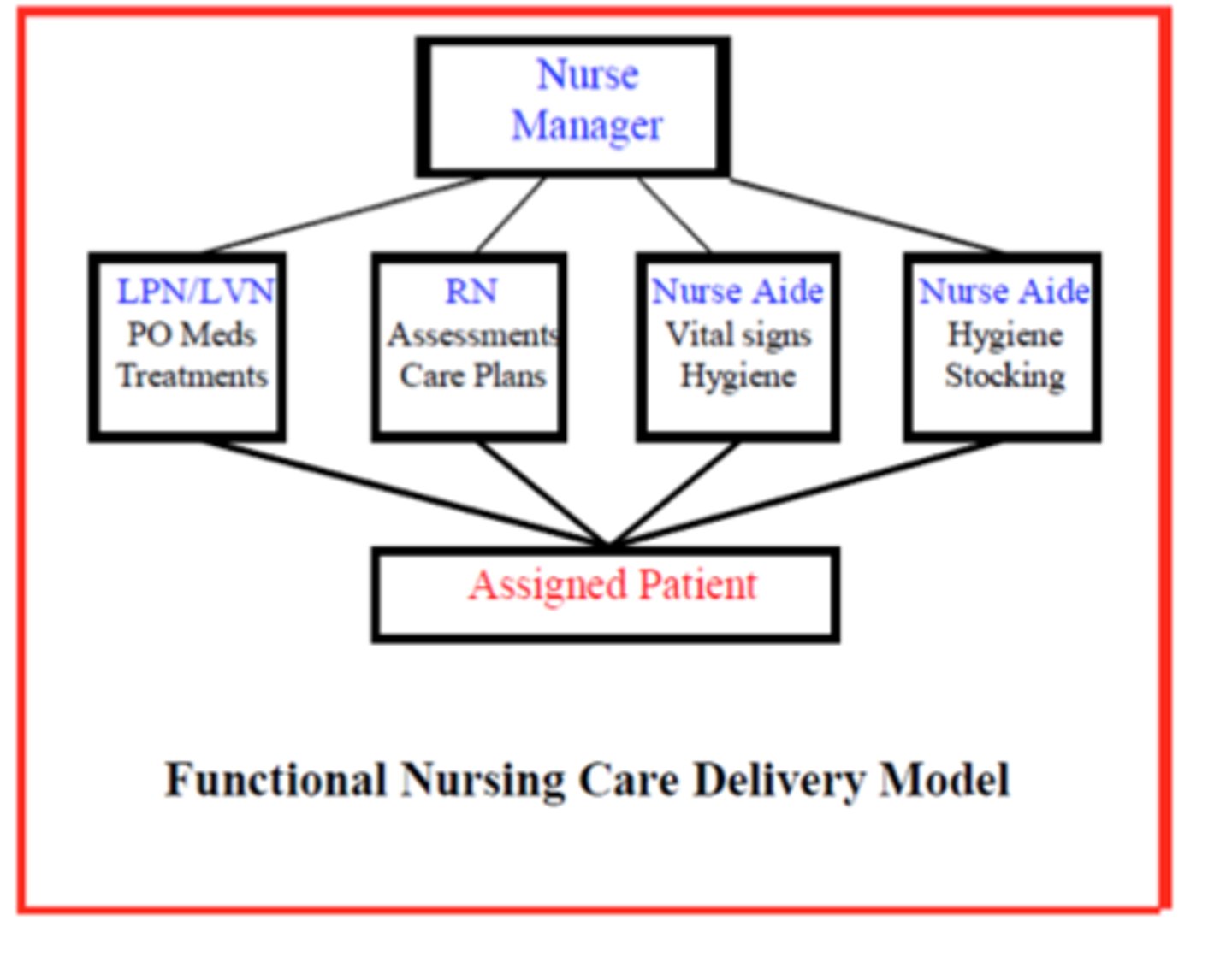
what is functional nursing? (what are the pros/cons, where is this model commonly seen?)
-staff members are assigned to complete certain tasks for a group of patients rather than perform all cares for a specific patient; broken up by tasks; (ex) UAPs attend to hygiene needs, LPNs administer all oral meds, RNs responsible for resident admissions/transfers/discharges
-more common in long-term care
-charge nurse makes assignments, coordinates care, and delegates some care
-pros: accounts for nursing shortage, utilizes special teams (IV team, wound care team)
-cons: patients get confused with so many providers, gets complicated because nurse needs to ensure their own tasks are completed PLUS the other staff members' tasks, can be hard to create a personalized experience
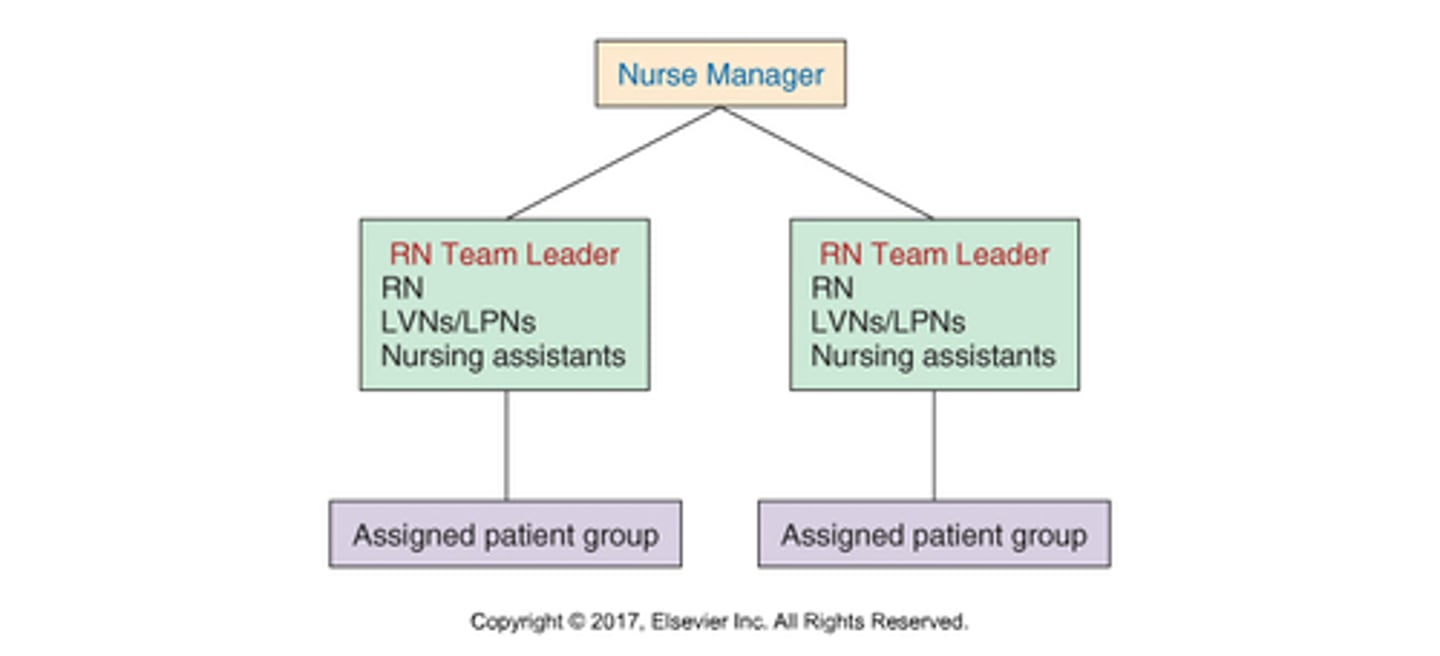
what is team nursing? (what are the pros/cons, where is this model commonly seen?)
-a variation of functional nursing
-charge nurse delegates cares to a group of patients (not broken down by tasks); multiple team leaders
-(ex): RN, LPN, and UAP team up to provide care to a group of patients
-pros: multiple team RNs coordinating care for a group of patients, hope to improve patient satisfaction
-cons: RN has to have good leadership skills
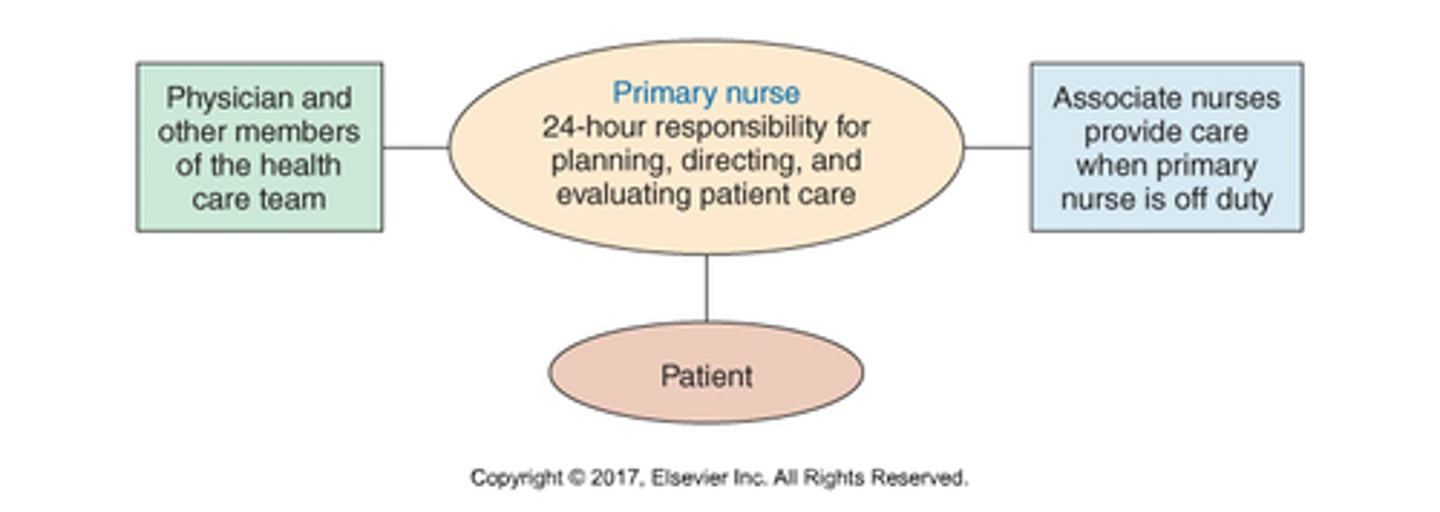
what is primary nursing?
-RN "primary" nurse assumes 24-hour responsibility for planning, directing, and evaluating the patient's care from admission through discharge; provides total patient care while on duty
-while off duty, an associate nurse provides care; follows the care plan established by the primary nurse
-requires cooperative environment and clear communication among team members
-pros: high quality care, holistic
-cons: RN practices with high degree of responsibility, expensive
-often seen in home home health, hospice, long-term care (oncology, brain injury, rehab)
what influences the types of care delivery models?
-health care setting: acute care, long-term care, ambulatory, home care, and hospice
-organizational structure and resources: management, staffing, supplies, urban or rural, and physical layout
-patient needs: acute, long-term, and chronic
what is an organizational chart?
visual representation of an organization's structure; defines positions and relationships between them
differentiate between first, middle, and top levels of management (examples, scope of responsibility, primary planning focus, communication flow)
top
-consists of an organization's board of directors and the chief executive or managing director (ex: chief nursing officer, chief executive officer, chief financial officer)
-look at organization as a whole as well as external influences
-ultimate source of power and authority since it oversees the goals, policies, and procedures of a company
-main priority is on the strategic planning and execution of the overall business success
middle
-unit supervisors, department head, director
-focus is on integrating unit-level day-to-day needs with organizational needs
-combination of long and short-range planning
-upward and downward communication with great centrality
first
-charge nurse, team leader, primary nurse
-focus primarily on day-to-day needs at unit level
-short-range, operational planning
-more often upward communication; generally relies on middle-level managers to transmit communication to top-level managers
what is centrality?
-the extent to which an employee communicates or interacts with others
-determined by distance on the organization chart
-middle manager tends to have greatest centrality because they receive information upward, downward, and horizontally
what is span of control?
-refers to the number of people directly reporting to any one manager and determines the number of interactions expected of them
-if too many people are reporting to a single manager → delays decision making; if too few are reporting → inefficient, top-heavy organization
what is centralized staffing?
-staffing decisions are made by a central office or staffing center
-manager's role limited to making minor adjustments and providing input
what is decentralized staffing?
-each department is responsible for its own staffing
-unit manager is often responsible for covering all scheduled staff absences, reducing staff during periods of decreased patient census/acuity, adding staff during high periods patient census/acuity, preparing monthly unit schedules, and preparing holiday and vacation schedules
what are the strengths and weaknesses of centralized staffing?
strengths:
-provides organization-wide view of staffing needs → encourages optimal utilization of staffing resources
-staffing policies tend to be employed more consistently and impartially; fairer
-more cost-effective
-frees the middle-level manager to complete other management functions
limitations:
-less flexibility for the worker, may not account for a specific worker's desires or special needs
-managers may be less responsive to personnel budget control in scheduling/staffing matters
what are the strengths and weaknesses of decentralized staffing
strengths
-unit manager understands the needs of the unit and staff intimately
-manager retains greater control over unit staffing
-staff can take requests directly to their manager; staff feels more in control of their work environment
-provides greater autonomy and flexibility for the individual staff member
limitations
-more special pleading, arbitrary treatment of employees; may be viewed as granting rewards or punishments through staffing
-may not be cost-effective
-more time-consuming for the unit manager
-difficulty ensuring high-quality staffing decisions throughout the organization
hospital organizational structures: shared governance
-builds on the foundation of an inclusive decision-making structure; nurses at every level play a role in the decisions that affect nursing activity throughout the system
-empowers staff nurses to work with a high level of autonomy, managing their clinical practice and working environment
-all councils led or co-led by staff nurses
-usually defined by a structure of rules or by laws
what is a magnet-designated healthcare organization?
-a Magnet-designated hospital is a medical facility considered to be the gold standard for nursing practice and innovation
-certified by the American Nurses' Credentialing Center (ANCC) as institutions that are able to attract and retain professional nurses
-only 570 institutions worldwide that are recognized as magnet status
what does it take to achieve magnet status? (5 components)
1) transformational leadership
-strong leadership that intends to transform organizations to meet the future
2) structural empowerment
-organization's personnel policies and practices
-professional development programs
-collaboration among the medical team and with community organizations
3) exemplary professional practice
-nursing staff must demonstrate a clear understanding of the role of nursing and how it applies to working with patients, families, communities and an interdisciplinary teams
4) new knowledge, innovations, and improvements
-should display a commitment to evolving the future of patient care and nursing practice
-evidence-based best practices and institutional advancements
5) empirical quality results
-studies demonstrating better patient outcomes and a higher standard of patient care
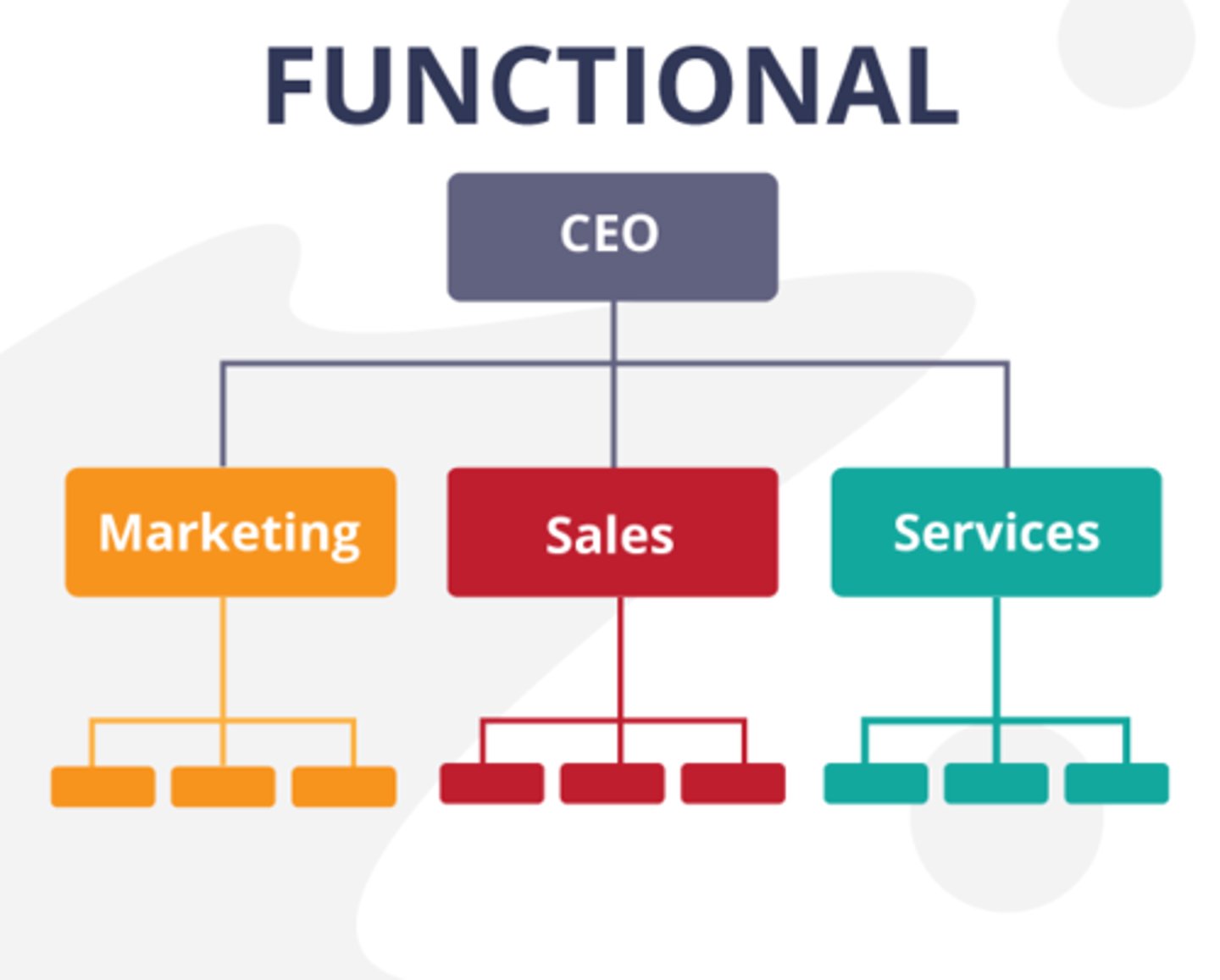
hospital organizational structures: functional
-organized by function or specialty provided to patients within the hospital
-departments providing similar functions in the hospital report to one manager or executive
-decisions made by one manager or executive for individual major functions w/in the hospital (nursing, finance, HR, IT)
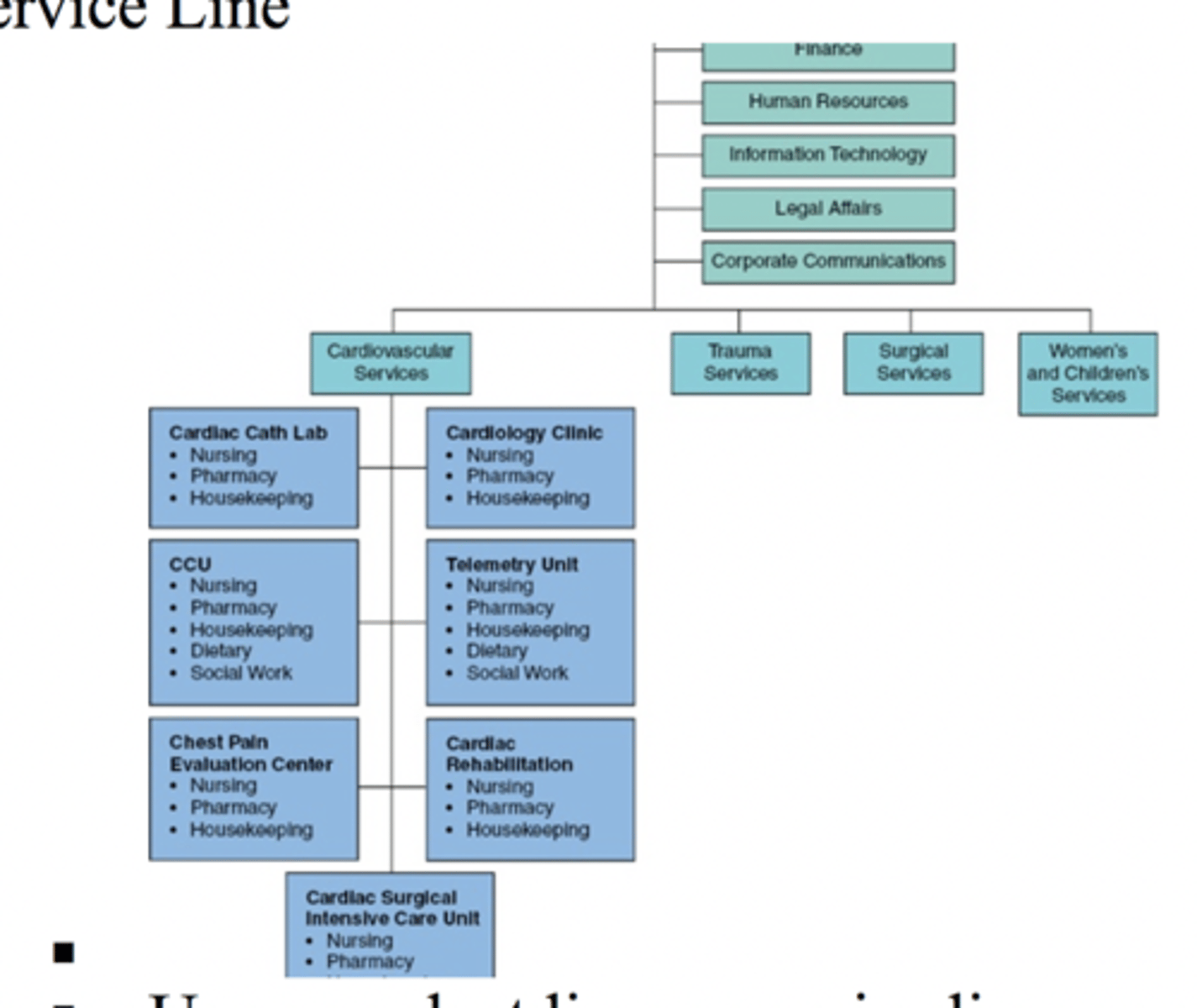
hospital organizational structures: service-line
-smaller in scale than large bureaucratic system
-overall goals determined by the larger organization, but the service line would decide on the processes to be used to achieve the goals
hospital organizational structures: matrix
-designed to focus on both product and function
-function: all the tasks required to produce the product
-product: end result of the function
-(ex): good patient outcomes are the product, and staff education and adequate staffing are the necessary functions
-vertical and horizontal chain of command
-fewer formal rules and fewer levels in the hierarchy, but decision making can be slow and often produces confusion/frustration; complicated communication required
what is telehealth?
-the delivery of health-related services and information via telecommunications technologies
-broad category; encompasses patient care, administrative activities, and health education
what is telemedicine?
-the diagnosis and treatment of patients through telecommunications technologies
-more specific; falls under the broader umbrella of telehealth
what is synchronous versus asynchronous telehealth?
-synchronous: care that happens in live, real-time settings where the patient interacts directly with a clinician, usually via phone or video; this is the most common form of real-time, virtual, direct-to-patient appointment
-asynchronous: care that does not happen in real time, but still allows the exchange of important information; for example, a patient may submit a photo of their wound through an online care portal, and the provider may review that photo several hours later and prescribe a medication or other treatment through the online care portal (AKA store-and-forward)
what is meant by "store and forward?"
An asynchronous telehealth technology that obtains and stores data at the source site, then transfers, or forwards the data to the remote intended site
what is remote patient monitoring (aka remote therapeutic monitoring)?
refer to "the use of connected electronic tools to record personal health and medical data in one location for review by a provider in another location, usually at a different time"
what are e-consults? what are tele-assessments?
-e-consult: typically asynchronous, store-and-forward clinician to clinician consults, including patient case information as well as other assessment data, such as photographs or pathology reports
-tele-assessments: patient, community, or student assessment (asynchronous or synchronous) performed at a distance
what is digital redlining?
technology policies, practices, and investments that reinforce class and race boundaries
what is digital inclusion?
technologies, clinical practices, policies, and programs that promote and support access to and use of the internet.
what is the relationship between telehealth and each of the social determinants of health?
-economic stability: may help create job opportunities
-education: increase prevention education through digital health education
-health care access and quality: can help triage patients, increase efficiency of appointments, increase prenatal care/mental health services/substance abuse treatment
-neighborhood and built environment: lack of access to wifi (rural and low income patients) may prevent individuals from using telehealth services
-social and community context: can help increase communication with providers, allows individuals to better track their healthcare data
what are unintended consequences related to telehealth?
-negative, unintended outcomes of telehealth that tend to contribute to ethical debates surrounding its use
-(ex): cardiac monitoring patch that patients wear 24 hrs a day for up to two weeks; can be helpful in catching/treating dangerous heart rhythms, but unintended consequences include over-treatment of heart rhythms (abnormalities may be benign), excess amounts of data collection, and possible legal consequences/burnout
staffing/scheduling: ten/twelve hour shift (what is it, pros/cons)
-commonplace in acute care hospitals
-continued debate about whether the length of these shifts contribute to increased judgement errors (from lack of sleep & fatigue) and exposures to hazards
-however, many nurses are satisfied with this model of scheduling because they have more days/consecutive time off
staffing/scheduling: agency and travel nurses (what is it, pros/cons)
-nurses who are employed by an external broker and work for premium pay without benefits
-provides scheduling relief (ex: during Covid-19), but are expensive and can result in poor continuity of nursing care
-nurses must also ensure their licenses allow them to practice in whatever jurisdiction they are seeking employment in
staffing/scheduling: per diem employment and float pools (what is it, pros/cons)
internal supplemental staff
-per diem: generally have flexibility to choose when they want to work; receive higher rate of pay but no benefits; may increase risks to patient safety because they are less likely to be familiar with organizational policies and procedures
-float pools: generally composed of employees who agree to cross-train on multiple units so they can work additional hours during periods of high patient census/worker shortages; help with filling gaps in staffing, but not adequate for staff continuity; staff may also feel uncomfortable floating if they have not been adequately oriented to the new unit
staffing/scheduling: flextime scheduling (what is it, pros/cons)
-a system that allows employees to select the time schedules that best meet their personal needs while still meeting work responsibilities
-variable start times may be used to schedule shifts longer or shorter than normal 8 hr workday
-when used, unit has employees coming and leaving the unit at many different times
-creates greater employee choices, but may be difficult for manager to coordinate and could easily result in over/understaffing
staffing/scheduling: self-scheduling (what is it, pros/cons)
-allows nurses in a unit to work together to construct their own schedules rather than have schedules created by management
-employees typically given 4-6 week schedule worksheets to fill out over several weeks in advance; nurse-manager then reviews the worksheet to make sure that all guidelines/requirements have been met
-offers staff greater control over work environment, but is not easy to implement; success depends on leadership skills of the manager to support the staff
staffing/scheduling: shift bidding (what is it, pros/cons)
-organization sets the opening price for a shift (ex: higher rate of hourly pay, nurses may bid down to be assigned the overtime shift)
-in general, organization chooses the nurse with the lowest bid to work the shift, but some organizations may deny bids to nurses who work too much overtime
what are nursing care hours per patient day? how is it calculated?
-way to determine requirements for staffing
-all nursing and ancillary staff are treated equally for determining hours of nursing care; no differentiation made for differing acuity levels of patients
-calculation: nursing hours worked in 24 hours divided by patient census (census: current number of individuals a facility is providing care for at that time)
what adverse patient outcomes increase as RN hours decrease in nursing care hours?
-medication errors
-patient falls
-patient satisfaction with pain management
what is a patient classification system?
-AKA "workload management" or "patient acuity tools"
-groups patients according to specific characteristics that measure acuity of illness; helps determine both the number and mix of the staff needed to adequately care for those patients
-used in staffing by acuity model: ongoing review is critical, utilize mandated ratios, hours of nursing care are assigned for each patient classification
-required by Medicare and The Joint Commission for certification
what are the 8 types of critical indicators in the patient classification system?
-eating
-grooming
-excretion
-comfort
-general health
-treatments
-medications
-teaching and emotional support
what is nurse-patient ratio staffing?
staffing model based on the number of patients on a unit
what is cyclical staffing?
-set staffing pattern is repeated every few weeks
-allows long term knowledge of future work schedules
what are mandated staffing ratios?
-defines the number of patients nurses may oversee in each hospital unit
-tend to vary depending on the unit/acuity level
-ensures nurses have enough time to properly care for their patients and avoid overworking anyone
-California is currently the only state with mandated nurse-to-patient ratios (ex: pediatric 1:4, labor and delivery 1:2, ICU 1:2)
what is mandatory overtime?
-staffing tool in which employees are forced to work additional shifts, often under the threat of patient abandonment
-neither efficient nor effective in the long-term, but devastating short-term impact on the mood, motivation, and productivity of employees
what are hours per patient day?
RN and UAP hours
3 categories:
-caregiving HPPD
-worked HPPD (education, shared governance activities (any hours worked that aren't caregiving)
-paid HPPD
what is an FTE and why is it important for nurse managers to understand this number?
-number of hours of work for which a full-time employee is scheduled for a weekly period
-1.0 FTE = 40 hrs (five, 8-hour days)
-can be divided in different ways: (ex) 2 employees each working 20 hrs per week (0.5 FTE) can make up one FTE
-3 12 hour shifts = 0.9 FTE
-FTE = 2080 hours/year, 80 hrs/2 week period
-importance: tells how many nurses/CNAs/LPNs you will need to cover the number of patients you have; if you are only budgeted a certain amount of hours, the nurse manager has to think about how many FTEs they need and how many nurses to hire
-also helps determine vacation time, disability
how are nursing FTE needs calculated?
-multiply RN nursing hours per patient day (HPPD) by 365; then divide by FTE hours in a year (2080)
-(ex): in 24 hours, we need 92 nursing hours; multiply by 365 = 33,580 hours; to translate to FTEs, divide 33580/2080 (FTE hours in a year) → 16.14 FTEs
what is a skill mix? how is it calculated?
-number of RN's, LPN's, CNA's required per shift
-calculation: of the total caregiver hours, what percent is contributed by RNs
-(ex): 140 total caregiving hours, 92 contributed by RNs = 65%
what is the work week?
-determines day the work week starts and ends (ex: Sunday to Saturday, Monday-Friday)
-helps define overtime
what is the average daily census?
-describes patient volume on a work unit
-the average number of patients that are in beds at midnight
-look at average to determine patient care needs for that unit
-when multiplied by 365 = annual patient days budget
how do you calculate nursing resource need in terms of hours per patient day?
total caregiving hours divided by average daily census
(ex): 140 total caregiving hours divided by average daily census of 16 = 8.75 hours needed per one patient day
what is a nursing sensitive indicator?
-patient outcomes determined by nursing interventions
-ex: falls, pressure injuries, CAUTI/CLABSI
what are the categories of advanced practice RNs?
1) nurse practitioners (MSN)
2) certified nurse midwives (CNM)
3) clinical nurse specialists (CNS)
4) certified registered nurse anesthetists (CRNAs)
what is a nurse practitioner? how does an individual become an NP?
-medical professional taking advanced care of children or adults within different settings; can diagnose, prescribe write orders, care management
-can become an NP with a master's of science in nursing (type of APRN)
-can also take the route of obtaining DNP (doctor of nursing practice); highest level, look at information systems and research
how does DNP differ from PhD in nursing?
-PhD in nursing are researchers; create new knowledge, determine "is this a problem?" and research how to get rid of it
-DNPs implement and apply the research
what is a post-graduate certificate?
-requires MSN or DNP
-allows someone to become certified in some area (kind of like mini masters degree)
States of Learning
• Conscious incompetence Beginner
driver
• Conscious competence Just passed
drivers test
• Unconscious competence Driver who
gets to work without remembering the
drive
Kramer’s Reality Shock
honeymoon
Elated to be finished with school
and starting a new job
• Perceive clinical setting and co-
workers in a positive light
• “Everything is great!”
• Actively focused on making new
friends
• Highly focused on developing
skills, mastering routines
• High motivation/commitment
• But...Low confidence
Kramer’s Reality Shock
reality shock
Preceptee encounters
practice differences from
what was learned in school
• Encounters obstacles to
providing quality care
• Witnesses inconsistencies in
professional behavior
• May ask self “Is this what
being a real nurse is like?
Transition stages model- doing,being, knowing
Process of Becoming (transitioning to professional nursing sttuuent)
Adjusting to changing personal and
professional roles
Benner’s Stages of Clinical
Competence
• “Novice-Expert Model