CAM part 2 exam 1
1/109
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
110 Terms
3 cardinal features of asthma
intermittent airflow caused by obstruction
bronchial hyperresponsiveness
airway inflammation
muscles tighten causing lining to get inflamed and mucus to build up
allergen/irritant exposure in asthma
allergen causes airway inflammation
IgE antibodies are made against the trigger and when exposed the antibodies bind mast cells that cause histamine to be released which causes an increase in eosinophiles, mucus hypersecretion and airway hyperresponsiveness
how can airway obstruction in asthma occur?
smooth muscle contractions
mucosal edema
and mucus hypersecretion
airways remodeling
chronic inflammation, mucus production, bronchospasm, protease activity cause goblet cell hypertrophy, SM hypertrophy, and scarring of bronchial endothelium- means a stiff thick bronchi
the increase in eosinophiles (eosinophiles release protease) - that causes scarring and thickening
histamine and leukotrienes cause constriction and increase mucus production
asthma changes in lumen cause what
as the lumen narrows there is turbulent air flow (expiration) = wheezing
and air trapping cause hypercapnia and hyperinflation
extrinsic triggers of asthma
means allergic IgE mediated
animals: cats, dogs, cockroaches, and mice
mold
dust mites
pollen - trees and grass
Intrinsic triggers of asthma
non allergic
exercise
cold/ dry air
pollutant like tobacco and smoke
respiratory infections
medications: aspirin, NSAID, beta blocker
asthma worse with what kind of living
urban
asthma development
interplay between:
genetic susceptibility
environmental exposure
developmental risk factors
asthma phenotypes
there is heterogeneity (state in being diverse) in pathogenesis and response to treatment
allergic (atopic)
associated with triad of eczema and rhinitis
non allergic
more often adult onset, neutrophils predominance and variable response to tx
eosinophilic asthma
needs corticosteroids early
sx of asthma
often worse at night or early morning
episodic wheezing
SOB
chest tightness
cough
vary by degreeas
asthma on PE
acute
tachycardia
could be using accessory muscle use, tripoding
wheezing
tachypnea
silent
chronic ( in between attacks)
often normal
allergic rhinitis, eczema, mild wheezing
what is required for asthma diagnosis
asthma sx plus variable expiratory airflow obstruction the gold standard is spirometry
others are bronchoprovocation testing, peak expiratory flow (helpful in management)
all three test are PTFs pulmonary function testing
spirometry
measure of volume inhaled and exhaled over time
help differentiate obstructive and restrictive lung disease
FEVI
is the max volume of air exhaled in the first sec
FCV (forced vital capacity)
total amount of air exhaled
normal results from spirometry
what would restrictive and obstructive disease look like
FEV1/FVC= 80%
restrictive disease normal or increase ration
obstructive less than 70% (issue with exhalation)
spirometry asthma vs COPD
get baseline PTF then do the bronchodilator test where albuterol is administer and if FEVI or FVC increase by 10% then asthma cause it is showing airflow limitation that is reversible with bronchodilator
testing for asthma if pt is asymptomatic during spirometry
establish baseline FEVA/FVC then administer bronchoconstrictive agent such as histamine or methacholine and if FEV1 drops by 20 % or more than asthma
TEST CONTRAINDICATED in pt with baseline FEV1 less than 65% predicated
peak flow meter
measures the peak expiratory flow
use in the morning before bronchodilator and then again after using it and above 20% means inadequately controlled asthma
helpful tool in managing but involves adherent pt
green good
yellow not good control getting worse
red asthma is severe
goal of asthma tx
decrease sx that interfere with normal activity
reduce future risk like ED visits
prevent permanent airway remodeling
non pharm tx of asthma
aviod triggers/ irritants
increase physical activity
breathing exercises
pharm tx of asthma focus on what two issues
bronchospasm aka relievers
bronchial inflammation aka controllers
types of bronchodilators
anticholinergics
beta 2 agonist
theophylline
beta agonis
SABA- albuterol
LABA0 salmeterol and formoterol
anticholinergics
SAMA- ipratropium
LAMA- tiotropium
medications for bronchial inflammation
corticosteroids
leukotrienes modifiers
mast cell stabilizers
biologics
corticosteroids
systemic= prednisone, prednisolone, and methylprednisolone
ICS= budesonide, fluticasone, momentasone
leukotrienes modifiers
Montelukast
mast cell stabilizer
cromolyn
biologics
omalizumab
mepolizumab
relizumb
combination medications
ICS/ SAB= albuterol and budesonide
ICS/ LABA= budesonide/ formoterol and fluticasone/ salmeterol
low dose ICS
can be used as manteance and reliever
max 12 a day
medium dose
daily maintenance
can not be used as reliever too
go back to chart on slide 36
what can be done to reduce risk of exacerbations
using the ICS-formoterol as the reliver according to GINA but in NAEPP they rec only using SABA PRN for step 1
cycle of asthma tx
assessment of asthma control- eval based on sx of the last 4 weeks
treatment adjustment
periodic review
classifications for asthma control
one point for each of the following:
daytime sx more than 2x a week
nighttime awaken
interference with norm activity
reliver medication needed more than 2 a week
0 points= well controlled
1=2 partly controlled
3-4 not controlled
step up/ step down
when uncontrolled despite adherence and good inhaler technique
step down to find the minimum effective dose
monitor for 2-3 months prior to change
asthma severity
is classified retroactively
mild: step 1 or 2
mod: step 3
severe 4 or 5 - can not be diagnosed until inhaler technique, comorbidities, ongoing exposure to allergens looked at and med adherence confirmed all severe cases need referral to pulm
acute exacerbation of asthma
sudden worsening of asthma sx
bronchial SM contraction
step to take:
R/O other possible causes- make sure asthma
severity
O2'
give rapid acting inhaled bronchodilators via nebulizer or IV magnesium if severe
start systemic glucocorticoids
asthma exacerbation severity catagorization
mild/moderate:
mild= pulse less 100 & PEF/ FEV1 less than 70%
mod= pulse 100-120& PEF/ FEV1 40-69%
severe- pulse over 120 and less than 40%
respiratory arrest imminent bradycardia and less than 25% of PEF FEV1, wheezing absent
mild moderate tx
inhaled SABA via nebulizer ot meter dose inhaler with holder chamber
systemic corticosteriods if peak flow less than 70 % or did not respond to SABA
severe tx
goal to maintain SPO2 above 90%
use inhaled SABA + SAMA- albuterol +ipratropium every 20 minutes or continuous for an hour and repeat assessment after 3 doses
inhaled bronchodilators
act on the SM by enhancing or blocking the affects of the autonomic NS
beta agonist bind to enhance relax
anticholinergics block the activity of Ach to suppress PNS and block SM contraction
admit/ transfer if
pt does not feel better
O2 below 94%
PEF less than 60%
fails the road test
boderline okay but no follow up plane
when to discharge
O2 above 94
pt feels better
PEF above 70
passes road test
make sure to have close follow up
asthma prevention and pt education
asthma action plan is written document with instruction with what medication to take, when each medication is appropriate and when to seek help
sleep apnea
apnea mean breath cessation for over 10 sec
hypopnea is decrease airflow with decrease in O2 greater than 4 %
types of sleep apena
obstructive - physical blockage of the airway despite respiration effort
central sleep - decrease or absent respiration drive
mixed
obstructive sleep apnea OSA
collapse of the pharynx during inspiration due to loos of normal muscle tone
upper airway obstruction during sleep
more common in men and obesity
increase in neck circumference strongest correlation of OSA
signs: excessive daytime somnolence and fatigue
ask partner if they have loud cyclical snoring or breath cessation
on PE: bull neck and may see narrowed oropharynx
OSA complications
cardiac arrthmias, HTN, and pulm hypertension
screening of OSA
STOP=BANG survey
use when pt has sx or pre op
score 0-2 no work up
3+ testing recommended
OSA labs
CBC can have erythrocytosis, increase hemoglobin/ hemocrit due to hypoxia
exclude hypothyroidism
OSA definitive diagnostics
polysomnography - sleep study and will show apneic episode with hypoxemia
OSA tx
weight loss
CPAP
aviod sedatives like alcohol
MRD mandibular repositioning
obesity hypoventilation syndrome OHS
development of daytime hypercapnia triad of:
obesity above 30
awake daytime hypercapnia above 45 paCO
sleep disordered breathing
diagnosis of exclusion
compilications: HTN, CHF, coronary artery disease
patho of obesity hypoventilation syndrome OHS
respiratory mechanical impairment: increase adipose tissue along the chest wall and abdomen reduces function residual capacity, lung compliance, and expiratory reserve increase the total work of breathing
blunted central respiratory drive: the neural stimulation to remain eucapnic fails and this starts as REM sleep but extends to daytime hypercapnia
same tx plan
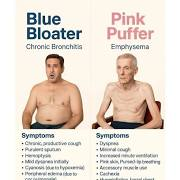
what is COPD chacterized by
it is an obstructive disease
chronic bronchitis - a mucus problem blue bloaters
emphysema - a structural prob pink puffers
with persistent respiratory sx and airflow obstruction with history of significant noxious exposure and largely irreversible and progressive
main noxious stimuli for COPD
tobacco smoke
biomass fuel for cooking and heating
chronic bronchitis patho
repeated noxious stimuli
chronic inflammation and irritation
hyperplasia increase in gland size and destruction of cillia
bronchial thickening with excessive mucus production and retention
airway obstruction
chronic cough and phlegm
chronic bronchitis consequences
airway obstruction leads to decrease tidal volume and will cause air trapping and hyperinflation
damage to the mucociliary defense and increase risk of infection due to reduced clearance
emphysema patho
chronic irritant exposure cause an increase in protease and a decrease in anti means there is more alveolar destruction of the capillaries and alveolar wall with air space enlargement (dilation)
alpha 1 antitrypsin deficiency
increase risk of emphysema even with limited air pollutant exposure
emphysema consequences
aveolar wall and capillary destruction means the the SA is decreased and there is an increase in dead space and due to the elastin destruction it impairs ability to recoil which leads to air trapping and decrease tidal volume
clinical presentation of COPD
SOB
septum production
cough
productive cough is the bronchitis and the SOB is emphysema
acute exacerbation is worsening of any of these sx and is precipited by infection often times
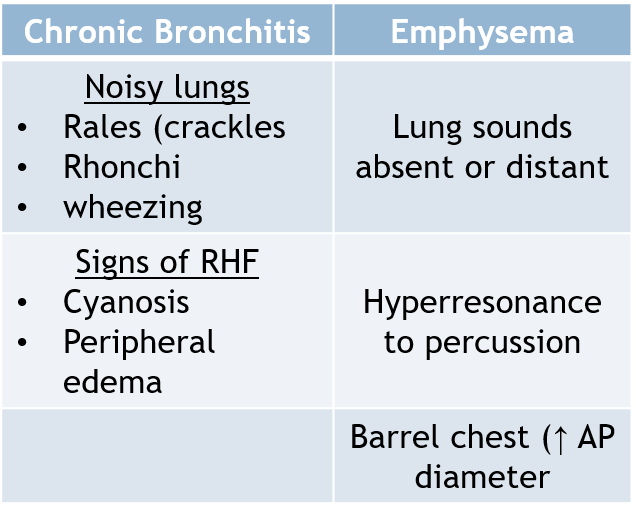
COPD on PE
chachexia (wasting)
hypoxic or tachypnea
increase AP diameter, decrease breath sounds, hyperresonant to percussion, wheezing, rhonchi, crackles
diagnosis critera for COPD
COPD sx
persistent airflow limitation soj post bronchdilator FEVA/FVC<70%
no alternative explanation of sx
COPD initial assessment
spirometry (needed for diagnosis)
asses severity via GOLD which is spirometry, questionnaire (CAT or Mmrc) AND EXACERBATION HX
CBC with diff
CXR
test for alpha def
spirometry of obstructive pattern
FEV1/FVC less than 70%
what can you use to asses severity of COPD on spirometry
FEV1 the degree of airflow obstruction is a prognostic factor
1- above than 80%
2- between 50-80
3-severe between 30 and 50
4- very severe less than 30 %
GOLD ABE assessment tool
if one or more exacerbation in the last year = E
if no exacerbation and mMRC0-1 or CAT less than 10=A
if no and mMRC equal or above 2 and CAT equal or greater than 10=B
CBC with diff in COPD
polycythemia
anemia (of chronic disease)
eosinphil count used to guide tx iICS if above 300
CXR findings in COPD
most reliable: hyperinflation and flattening of the diaphragms
others: hyperlucency of lungs, prominent pulm arteries, and bullae
chronic bronchitis cause increase in pulm vascular and right heart enlargement
emphysema cause decrease in vascular, hyperinflation, flatten diaphragms, hyperlucent, bullae/blebs, and both cause an increase in AP diameter
bullea increase risk of pneumothorax
stable COPD management
stop smoking, make sure they get vaccinations, aviod envirnmental triggers. pulm rehab, physical activity, good sleep and diet
oxygen th via nasal cannula 1-3 L /min if less than 88%, ABG above 55mmHg, cor pulmonale (RH failure). titrate o2 92% to not decrease respiration drive
everyone gets rescue inhaler -= SABA+ SAMA and th is dependent of group
bronchodilators for COPD
anticholinergics: block Ach from muscarinic receptor means less bronchoconstriction and decrease secretions. SE: dry everything, blurred vision, hard time swallowing
SAMA- ipratropium
LAMA- tiotropium, aclidinium, umeclidinium, glycopyrrolate
beta agonist for COPD
se: tremor, tachycardia, restlessness, hypokalemia, CNS stimulation
SAMA- albuteral
LAMA- formoterol and salmeterol
oral corticosteroids for COPD
ICS= budesonide, fluticasone, momentasone
helps reduce exacerbation use when EOS above 300
oral- tx for exacerbations long term affects: osteoporosis, weight gain, cataracts, glucose intolerance, increase risk of infection
COPD tx based on groups
all get rescue inhaler that is SAMA, SABA
group A= LAMA
group B- LAMA+LABA+ICS
COPD exacerbation management
o2 th to 88-93%
nebulize SABA/SAMA (albuterol and ipratropium)
systemic corticosteroids for airway inflammation'
empiric antibiotics for five days if they are hospitalized or if two of the cardinal sx are present
no risk factor: azithro and cefpodoxime
risk factor: amox-calvulanate, levofloxacin
smoke inhalation
slide 60
acute bronchitis
self limiting respiratory tract infection causing bronchial inflammation (of the large airways) when there is no evidence of pneumonia or chronic obstructive pulm disease. highest occurrence in late fall and winter along with viral peak.
virus caused thickening, increase mucus production (blockage), and airway hyperresponsivity (like asthma)
chronic cough is the cardinal sx is 18 days to 8 wks can be purulent or not, +/- hemoptysis but should bot be febrile
clinical dx
tx: supportive can use dextromorphan and guaifenesin as need for cough
indications for cxr for chronic bronchitis
abnormal vital
pulse above 100
RR above 24
temp above 100.4
o2 sat below 95 %
or if there is mental confusion with a patient above 75 y
respiratory syncytial virus
paramyxovirus outbreak in october-jan
aka RSV
can affect adult older than 60, severe immunodef
prodrome=1-3 days (URI sx like nasal congestion and cough) then progress to lower resp infection 2-3 days later with sx like wheezing, tachypnea, and worsening cough, peaks on 3-5 days
clincal dx: winter season less than 24 months, RSV PCR is gold standard only test if tx changes
RSV tx
supportive
hydrate, humidification of inspired air, nasal suction…
admit if they are hypoxic, respiratory distress, unable to tolerate PO
Ribavirin is antiviral when hospitalized
RSV prevention
Nirsevimab: all for infants less than 8 months entering first RSV season. Children 8-19 months at increase risk entering 2 season (prematurity. CF)
clesroviman: also first line for infant less than 8 months before RSV season no approved for second season
palivizumab- alt tx
arexvy- adults over 60
arbyso pregno pt 35-39 wks antibodies are transmitted to fetus.
pneumonia transmission
aerosol inhalation
colonizes in the nasopharynx and then reaches the alveoli and infection leads to inflammation and damage
legionella disease
through infected water such as AC units, ventilation systems (planes)
CM: extrapulmonary like watery diarrhea with neurological sx headache, confuson
PCR testing labs will show hyponatremia, increase ALT/AST & LDH, CK
tx: macrolides
different site of acquisition for pneumonia
community acquired - outside the hospital (or within 48 hrs of admission)
nosocomial (hospital acquired) after 48 hrs also includes VAP
aspiration pneumonia - aspiration of oropharyngeal or upper GI contents
Etiology of pneumonia
typical
atypical
fungi
virus
mycobacterium
CM of typical pneumonia
fever, productive cough, chest pain, dyspnea, rigors (chills and violent shaking)
atypical pneumonia
extrapulmonary symptoms
low grade fever
dry non-productive cough
physical exam for pneumonia findings
signs of consolidation:
inspiration crackles
bronchial breath sounds
dullness to percussion
increase tactile fremitus
egophony
atypical is often normal
bacteria that cause typical
kleb
strep pneumonia
staph pneumonia
h. influenza
Moraxella catarrhalis
atypical organism
mycoplasma pneumonia
legionella
chlamydia pneumonia
CAP
MC- strep pneumoniae gram + cocci in pairs (pairs strep down)
2nd MC h influenza gram - rod, often older adults
sudden onset chills and rigors with rusty blood-tinged sputum
staph aureus influenza
post influenza infection
gram + cocci in cluster
cxr: bilateral infiltrates multoloblar and can cause cavitary lesionsl
klebsiella pneumoniae
CAP in DM, alcoholics and impaired host defenses
gram - rods
has currant jelly sputum due to marked inflammation and necrosis cause the thick mucus that is blood tinged
cxr: can be cavity will be upper lobar consolidation with bulding
mycoplasma pneumoniae
walking pneumoniae
in young health collage students
URI prodrome followed by persistent cough
DX: CXR shows reticulonodular pattern or interstitial infiltrates and cold agglutinin titers will not be able to PCR
tx: macrolide or doxy
2 levofloxacin
CAP viruses
influenza
PCR testing or respiratory pathogen panel
tx: supportive care
influenza - oseltamivir
COVID- nirmatrelvir-ritonavir