Selective Reabsorption (urine formation) T2 W9
1/9
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
10 Terms
Selective reabsorption
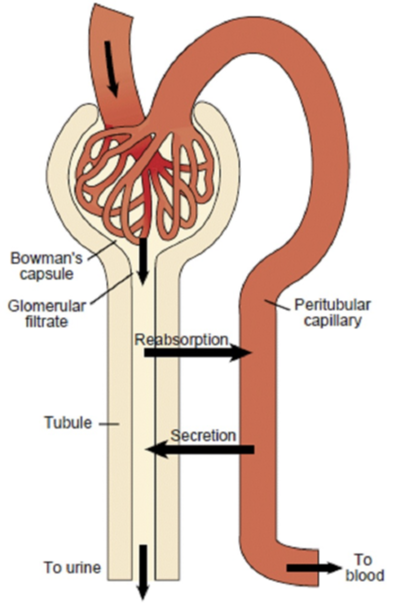
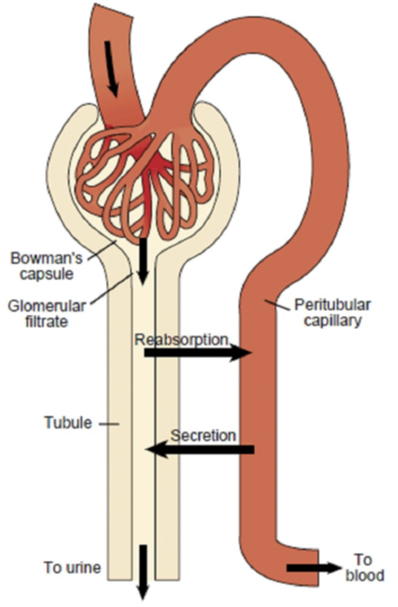
When substances in filtrate are reabsorbed. Not all is reabsorbed into blood the process is “selective“.
Is selective reabsorption active or passive process and where does it occur
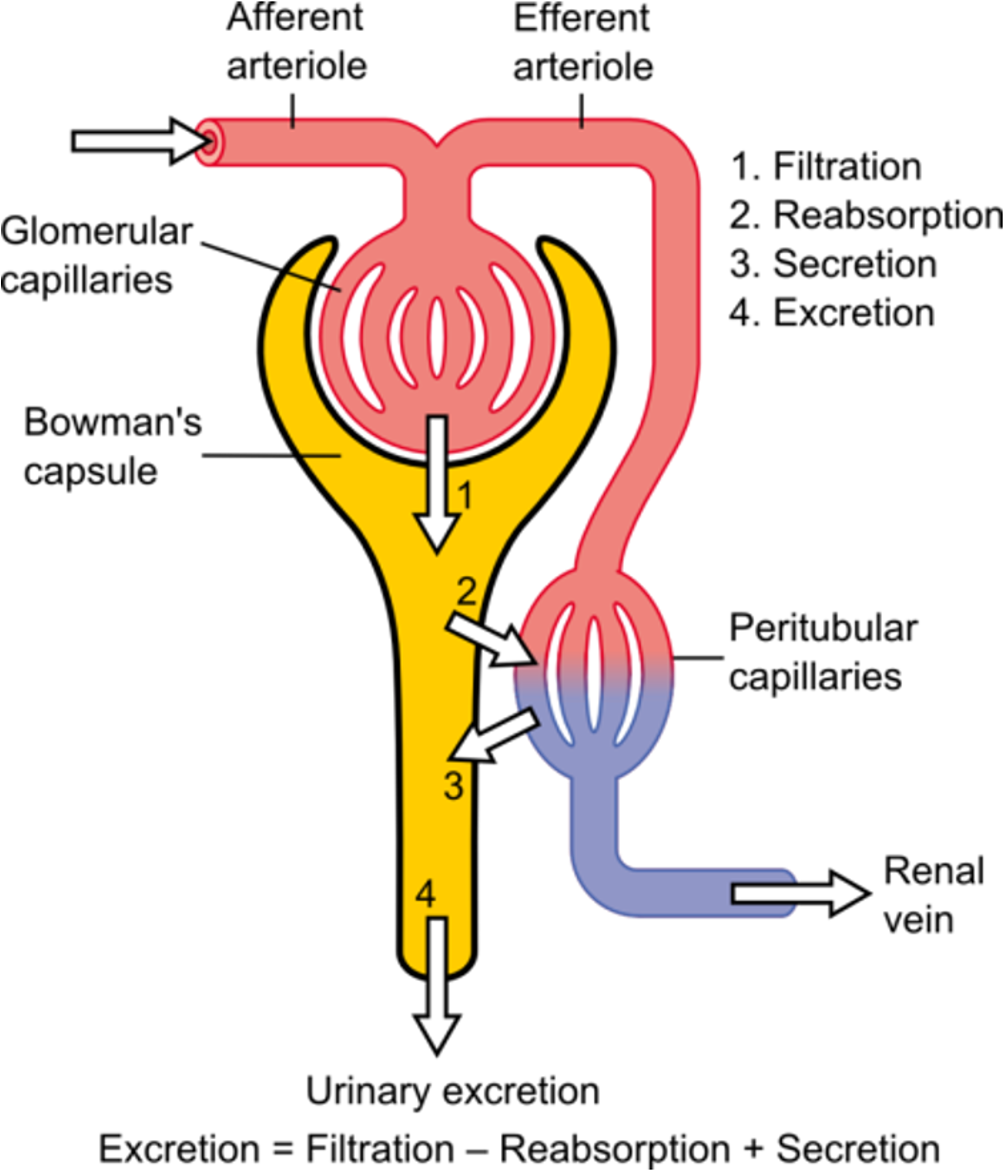
Both a passive or active process in which substances in the filtrate are moved into the blood. Depends on the concentration gradient. Between the renal tubule and peritubular capillaries.
Time taken for total plasma volume to filter into renal tubues
About every 22 minutes. Therefore under 30 minutes all plasma would drain away if not for selective reabsorption which quickly reclaims most of the contents of the filtrate and returns them to the blood.
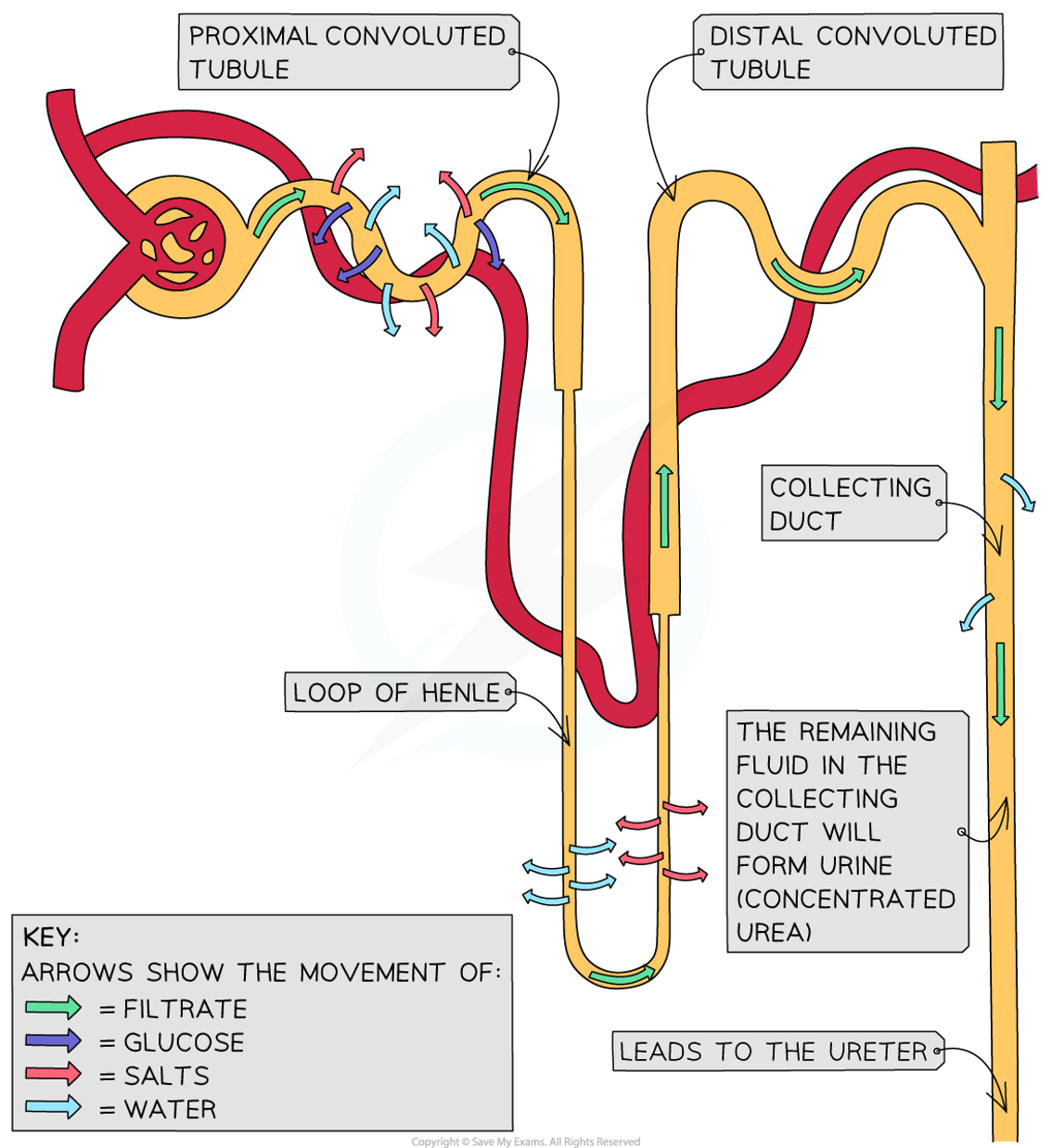
This process begins as soon as the filtrate enters the PCT, where 65% of the filtrate volume is reabsorbed.
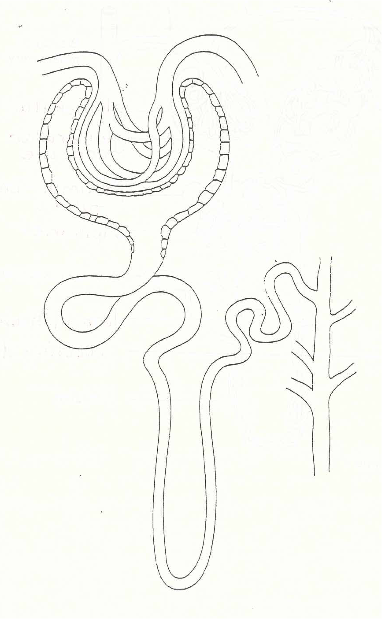
Filtrate path through nephron
Filtrate from the renal corpuscle passes through the PCT first, then the loop of Henle and the DCT.
What are the cells that make up the renal tubule
One cell layer thick – epithelial cells - as are the cells of the peritubular capillaries.
Both the peritubular capillaries and the renal tubule are long, convoluted structures which provides a large surface area.
What is the reabsorption process dependent on
Depending on the substance, the reabsorption process may be either active (active transport) or passive (simple diffusion, facilitated diffusion or osmosis).
What happens in the proximal convoluted tubule (PCT)
•All - 100% - of the glucose and amino acids molecules are also actively transported.
•About 65% of the filtered sodium ions are actively transported.
•Movement of these solutes back into the blood establishes a strong concentration gradient for the passive movement of water via osmosis.
•This flow of water back into the blood is called obligatory water reabsorption.
•About 65% of the filtered water is reclaimed back into the blood.
•As water leaves the filtrate, the concentration of solutes in the filtrate increase.
•There will be some passive transport into the blood of some ions like Cl-, Ca2+, K+.
•Nearly all the uric acid, and about half of the urea is passively reabsorbed into the PCT.
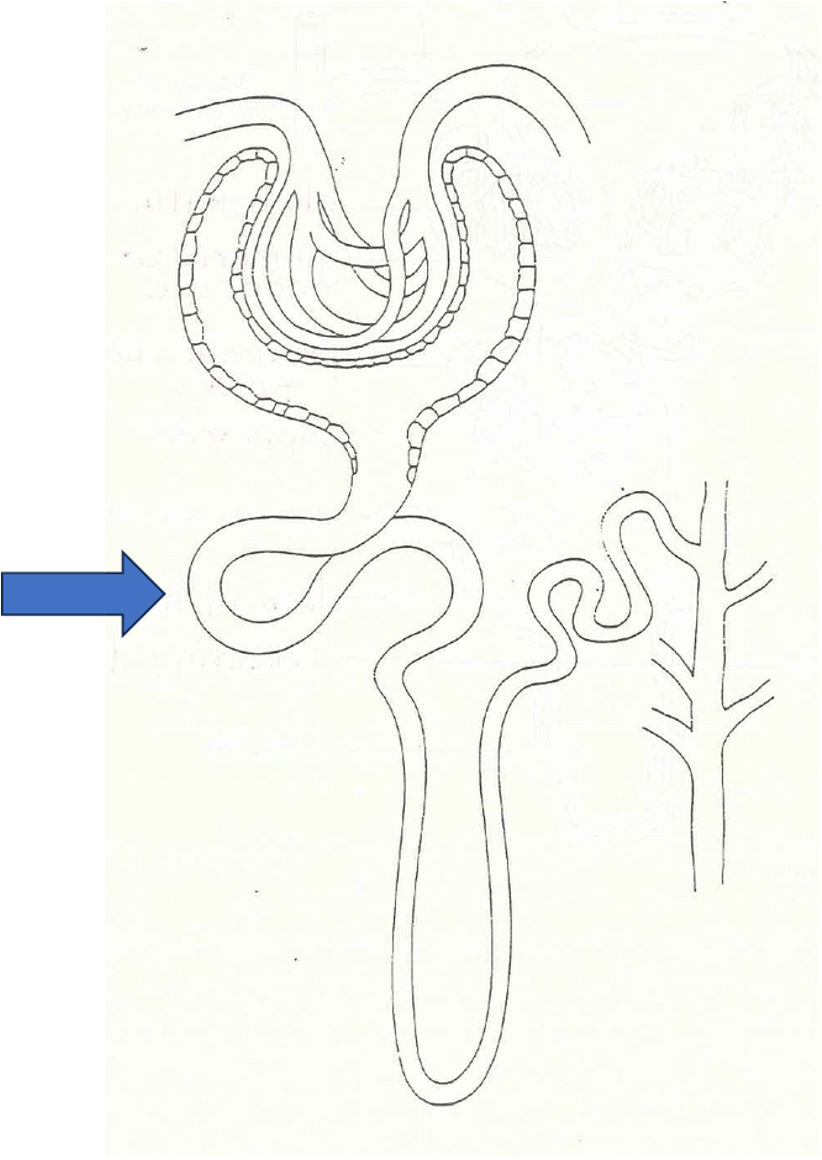
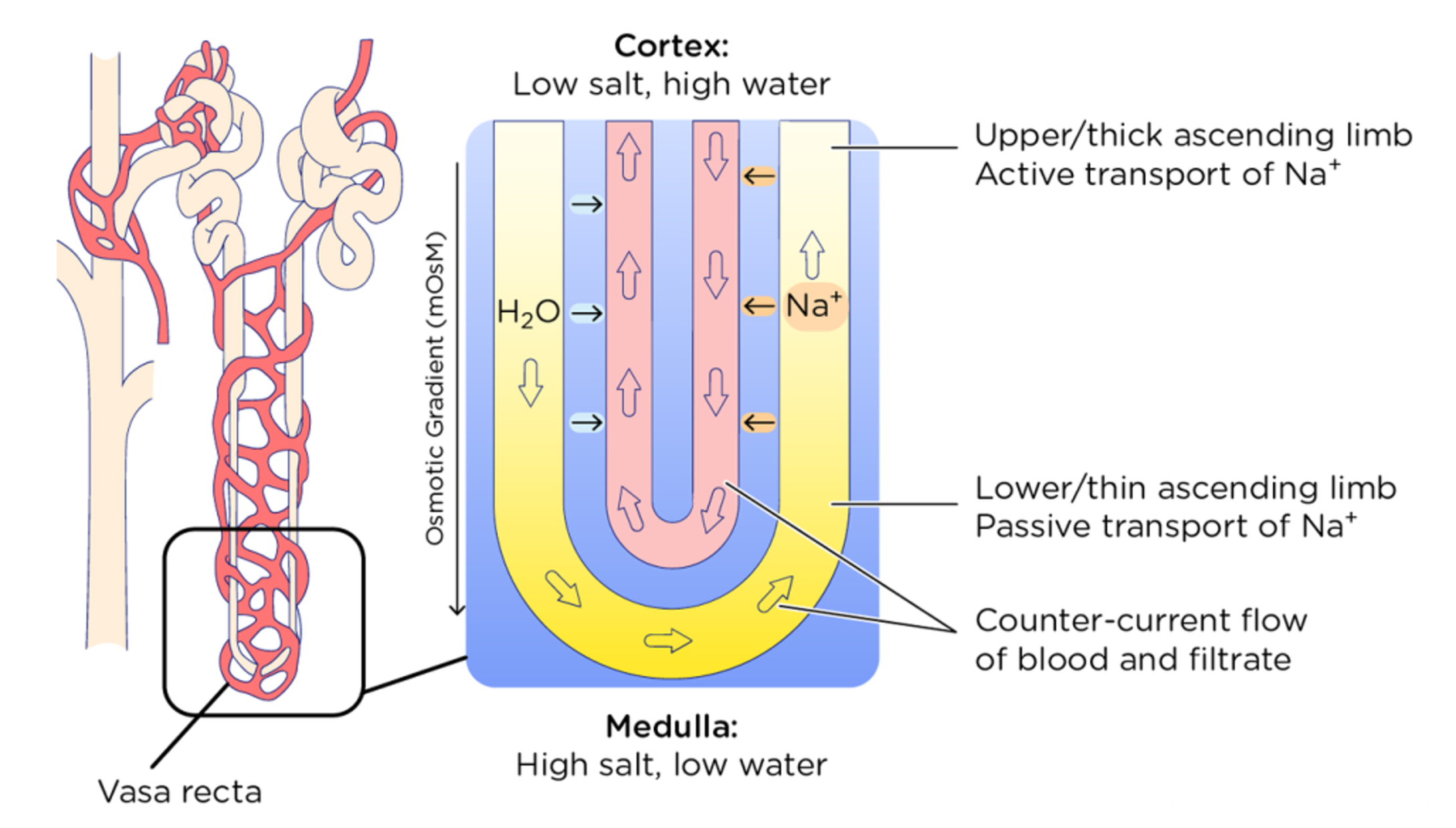
What happens in the loop of Henle (LH)
•Beyond the PCT, the permeability of the renal tubule epithelium changes.
•The descending limb is more permeable to water.
•The ascending limb is more permeable to sodium ions.
•Water can leave the descending limb of the loop of Henle but not the ascending limb as the channel proteins for water (aquaporins) are absent in the cells forming the ascending limb.
•The opposite happens for sodium, potassium and chloride ions which are both actively and passively transported in the ascending limb.
What happens in the distal convoluted tubule (DCT) (is after the HL)
•Most of the filtered water and solutes have been reabsorbed by the time they reach the DCT.
Reabsorption in the PCT and loop of Henle does not vary withthe needs of the body, but in the DCT and CD reabsorption is fine-tuned based on the body’s need by hormones.
What happens at the end of the selective reabsorption process
Absorbed:
•100% of glucose and amino acids
•Water
•Ions: Na+, K+, Ca2+, Cl-, HCO3-
•Some of the wastes are partially reabsorbed, e.g., urea