Vascular abnormalities of scrotum
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
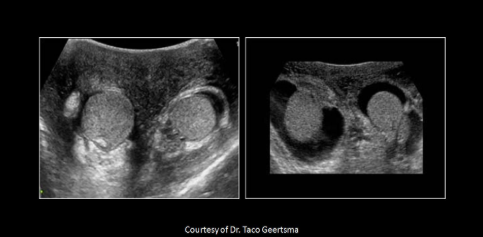
Varicocele
Collection of abnormal dilated serpiginous vein posterior to the testes that extend to the spermatic cord (pampiniform plexus)
Idiopathic - incompetent values in internal spermatic vein
Secondary - increased pressure caused by abdominal mass or hydronephrosis
Can also be related to inguinal hernia or herniorrhapy
Most common cause of male infertility
Varicocele
Normal vein diameter
0.5-1.5mm
______________ more common due to the left gonadal vein emptying into the left renal vein, not IVC
Left varicocele
Nutcracker syndrome
Superior mesenteric artery compresses the left renal vein causing increased pressure and stasis in the venous systems of the left kidney and left testicle
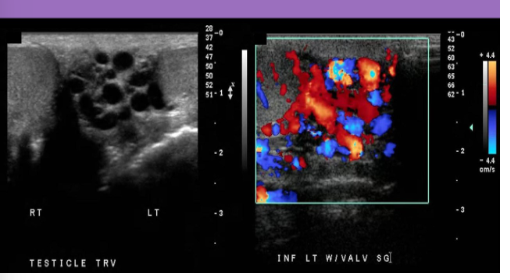
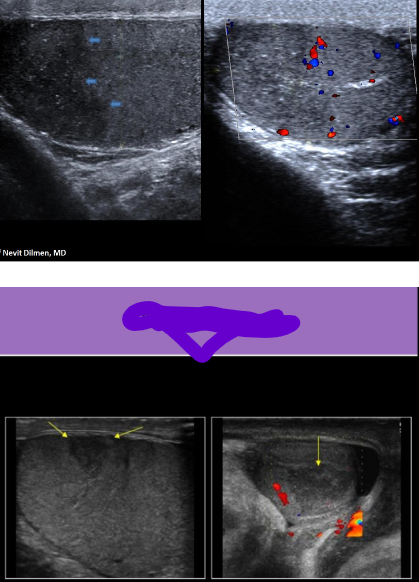
USA varicocele
Extratesticular - Multiple tortuous anechoic structures proximal to upper pole of testis
Intratesticular - multiple cystic structures within the rete testes that fill with color on Doppler eval
Veins dilate with Valsalva
>2mm diameter abnormal with pt supine
If pt stands for exams, hydrostatic pressure causes vessels to dilate
>2.5mm diameter abnormal for standing exam
Upper abdomen should be eval for mass when varicocele is found on right
Varicocele
Infarction
Loss of blood flow to a portion or all of the testicle
Can be focal or diffuse
Related to torsion, trauma, bacterial endocarditis, leukemia and vasculitis
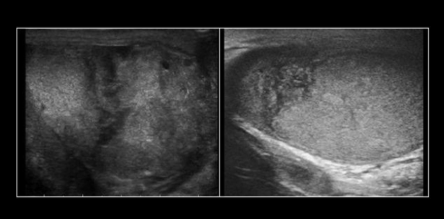
USA Infarction
Varying echogenicity with age of infarct
Acute - hypoechoic area
Chronic - hyperechoic calcs, reduced size of testicle
Use color to help with diagnosis
Testicular infarct
<4 hours torsion
Absent flow in testicle, normal teste
>4 hours testicular torsion
Increased teste size, heterogeneous, hydrocele, absent flow
>24 hours testicular torsion
Scrotal wall thickening, areas of infarct and necrosis within teste
Testicular torsion
Most common before age 30yrs
Larger testicles are those with tumor formation present a greater risk of torsion
Acute testicular pain, swollen scrotum, N/V
CRITICAL
Teste salvage rate
<6hrs = excellent
6-12hrs = declining
>12hrs = poor
Epi and appendix testis can undergo torsion without testicle
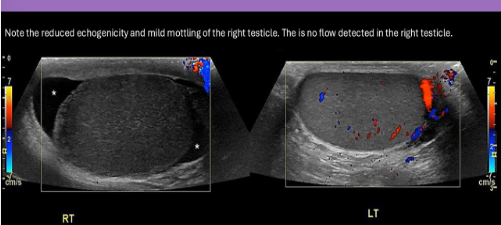
USA Torsion
Blue dot sign: blue dot under skin surface of scrotun
Variable echogenicity
Acute torsion - enlarged testicle, hypoechoic and mottled appearance
Areas of infarct may be seen if progressive
Color AND PW Doppler necessary for diagnosis
Complete torsion
Absence of intratesticular flow
Document color Doppler views of the normal side first, then image the affected side with the same color Doppler setting
Partial torsion
May still demonstrate some high resistance flow with absent or reversed diastolic flow in the affected teste
Comparison of the PW Doppler waveforms from both sides can assist in diagnosis
Asymmetry of the resistive indices can indicate partial torsion
RI value greater than 0.7 = partial torsion
Complete torsion RI value
1.0
Normal RI values in testicle
0.5-0.7
Epididymal torsion
Hypoechoic enlarged epididymis mass with variable echotexture and no vascularity
Normal testicular appearance and vascularity
Torsion of the Appendix testis
Hypoechoic enlarged mass with variable echotexture and no vascularity
Located between a normal teste and a normal epi
Normal testicular and epi appearance and vascularity
Testicular torsion
Testicular rupture
Ruptured testicle
Critical finding, requires immediate intervention
Areas of hemorrhage and infarction can be seen
Hematocele formation
Orchiectomy with possible prosthetic placement
Scrotal hernia
Small intestine, colon and/or omentum falls into scrotal sac through abnormal opening in the inguinal canal
Scrotal hernia USA
Echogenic material within scrotal sac
May see dirty shadowing from air within bowel
Valsalva used to demonstrate peristalsis of herniated abdominal contents
Color Doppler used to evaluate suspected herniated bowel loops for vascularity
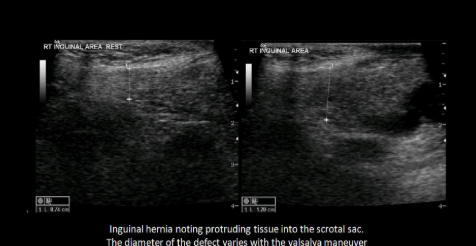
Inguinal hernia
Sperm granulomas
Extravasation of the spermatozoa into tissues around epi
Sperm granulomas USA
Solid hypoechoic or heterogeneous mass
May contain calc
Fibrous pseudotumor
Rare, non-neoplastic mass
Made of fibrous tissue
Fibrous pseudotumor USA
Solid hypoechoic or heterogeneous mass
Scrotal wall thickening
Fluid accumulates in these tissues of the scrotum
Inflammatory causes include cellulitis and Fournier gangrene
Normal vascularity present when there is non-inflammatory cause
Scrotal wall thickening risk factors for inflammatory disease
Obesity, diabetes, or pt is immunocompromised
Inflammatory scrotal wall thickening USA
Wall thickness >8mm
Presence of hypoechoic areas with increased vascularity
Non-inflammatory causes of scrotal wall thickening
CHF, lymphedema, liver failure, and lymphatic and venous obstruction
Non-inflammatory scrotal wall USA
Scrotal wall thickness >8mm
Layers of altering hypoechoic and hyperechogenicity
Scrotal wall thickening
Post-vasectomy changes
Epididymal enlargement and inhomogeneity
Development of sperm granulomas and cysts
Dilated rete testes
Clinical Hx and color Doppler are used to differentiate post-surgical changes from acute epididymitis
NO hypervascularity with post-surgical changes; hypervascularity with acute epi
Most common residual effect of a vasectomy
Spermatic granulomas
When evaluating a pt for a suspected varicocele, the pt should be scanned:
While performing Valsalva strain
While standing
While supine
All of the above
All of the above
How is testicular torsion diagnosed
Comparing the PW Doppler of the centripetal arteries on both sides
If flow is identified in both testicles, but the RI values differ greatly, ________ should be strongly suspected
Partial torsion on the right side with the higher RI value
Which of the following is a risk factor for torsion?
Men over 60yrs
Bell clapper deformity
Small testicles
All of the above
Bell clapper deformity
What describes the appearance of a testicular prosthetic on US
Round structure with reflective borders and an anechoic lumen
What abnormalities can be evaluated by asking the pt to do a Valsalva
Hernia, varicocele, nutcracker syndrome
Which of the following is a non-inflammatory cause for scrotal wall thickening?
Orchitis
Epididymitis
CHF
Systemic HTN
CHF