Clinical Prediction Rules
1/57
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
58 Terms
High Ankle Sprain Cluster
TTP
(+) stress test
Presence of hematoma
96% SN
NOTE: squeeze test > specificity than kleiger test
Ottawa Ankle Rules
Valid for patients age 16+ to R/O fracture:
Ankle:
TTP along tip or medial malleolus (6cm proximal from mid-point)
TTP along posterior edge of lateral malleoli (6cm proximal from mid point; NOT anterior malleoli)
Inability to WB immediately and in ED
Foot:
TTP base of 5th metatarsal and navicular area
Inability to WB immediately and in ED
Bernese Ankle Rules
Pain w/ compression of tib and fib approx. 10cm to fib. Tip
Thumb press on medial malleolus
Compression of rearfoot and midfoot
NOTE: more SPECIFIC than Ottawa Ankle Rules
Ottawa Knee Rules
Age >55
TTP hed of fibula
Isolated tenderness of patella during palpation
Inability to flex knee to 90
Inability to WB immediately and upon ER evaluation
Pittsburgh Knee Rules
Blunt trauma or a fall as MOI PLUS one of the following:
- Age >50 or <12
- Inability to walk 4 steps in ED
Carpal Tunnel Syndrome
Shaking hands for symptom relief
Wrist ratio >0.67
Symptom severity scale >1.9
Reduced median sensory field of digit 1
Age >45
3/5 98% SN, 4/5 70%, 5/5 90%
Lumbar Spinal manipulation
Duration LBP <16 days *
FABQ (work) < 19
No symptoms beyond knee *
1 or more hypomobile segment or (+) lumbar spine test for pain
1 or both hips >35 deg IR
3/5 68%, 4/5 95%
Vertebral Compression Fracture (Henscke et all 2009)
Prolonged use of corticosteroids (+LR = 48.5)
Significant trauma (+LR = 10)
Age >70 (+LR = 11)
Female sex
3/4 100% SP +LR 218
NOTE: Vertebral compression fracture "Supine Sign" is pain lying supine and has SN 81% and SP 93%
Vertebral Compression Fracture (Roman et al 2010)
Age >52
No presence of leg pain
BMI <22
Does not exercise regularly
Female gender
NOTE: Vertebral comrpession fracture "Supine Sign" is pain lying supine and has SN 81% and SP 93%
Cervical Radiculopathy
Positive ULTT median (MOST SN)
Cervical AROM <60 to affected side
+ distraction test
+ spurling test
3/4 65%, 4/4 90%
Subacromial Pain / Impingement "HIP"
Hawkins kennedy *
Infraspinatus muscles test/painful/weak ER *
Painful arc (60-120)*
2/3 90%, 3/3 95% and +LR 10.56
others:
Jobe (empty can)
Neers
(+ = rule in)
Full thickness RTC tear
Age >65
Night pain
Weakness ER
3/3: 94% SP PPV 93% +LR 9.8, - LR 0.54
RTC pathology (Park et al)
Painful arc
Drop arm sign
Infraspinatus muscle test
2/3 69%, 3/3 91%
Anterior instability
Anterior apprehension *
Relocation *
Surprise
NOTE: apprehension not pain are more sensitivt and specific for instability
Ankylosing Spondylitis (Berlin Criteria)
Morning stiffness > 30min
Improvement in back pain w/ exercise but not w/o
Awakening because of back pain during second half of night only
Alternating buttock pain
Ankylosing Spondylitis (IBP Criteria)
Age at onset <40 y.o.
Insidious onset
Improvement w/ exercise
No improvement w/ rest
Pain at night w/ improvement on getting up
4/5 SN 77% SP 92%
Cervical Myelopathy
Gait deviation
Positive hoffman's test
Positive inverted supinator sign (MOST SP)
Positive babinski test
Age >45 (MOST SN)
3/5 94%
Cervical Closed Fracture
Age <55
Single (maritial status)
Condition involved trauma
Acute condition
Condition involved ER visit
Wells Criteria
Pulmonary Embolism Criteria
Hip OA
Squatting as aggravating factor
+ scour test w/ adduction for groin or lateral hip pain
Active hip flexion causing lateral hip pain
Passive IR <25 deg
Active hip extension causing pain
3/5 68%, 4/5 91%
Lumbar Spinal Stenosis
B symptoms
Leg pain > back pain
Pain during walking/standing
Pain relief upon sitting
>48 y.o.
MCL Pathology
Trauma by external force to leg
Rotation trauma
Pain w/ valgus stress test @ 30 deg
Laxity w/ valgus stress test @ 30 deg
Meniscal Cluster
History of catching/locking reported
Joint line tenderness
Pain w/ forced hyperextension
Pain w/ maximal passive kne flexion
Pain or audible click w/ McMurray
SIJ pain (Laslett cluster)
SI distraction
SI compression
Thigh thrust
Gaenslen's test
Sacral thrust (laslett) or FABER (van der wuff)
<3 4%, >3 59%
Cervical Manipulation for Neck Pain (Puentedura et al 2012)
Symptom duration <38 days
Positive expectation that manipulation will help
Side to side difference in cervical rotation >10 deg (MOST SP)
Pain w/ PA middle C-spine
3/4 90%, 4/4 10%
Cervical Manipulation for Neck Pain (Tseng et al 2006)
NDI <11.5
B involvement
Not performing sedentary work >5hrs per day
Feeling better while moving neck
Symptoms not worse w/ cervical extension
Diagnosis of spondylosis without radiculopathy
Exercise for Ankylosing Spondylitis
SF-36 physical role >37
SF-36 bodily pain >27
Bath ankylosing spondylitis Disease Activity Index >31
Hip Mobilization for Knee OA
Hip or groin pain or paresthesia
Anterior thigh pain
Passive knee flexion <122 deg
Passive hip IR <17 deg
Pain w/ hip distraction
any 2 +LR 12.9
Manual Therapy and Exercise for Acute Lateral Ankle Sprain
Symptoms worse when standing
Symptoms worse in evening
Navicular drop >5mm
Distal tib-fib joint hypomobility
3/4 95%
Mechanical Traction for LBP
FABQ (work) < 21
No neuro deficit involvement
Age >30
Non manual work job status
4/4 69%
Mechanical Traction for Neck Pain
Peripheralization w/ lower c-spine C4-C7 mobility testing
Positive shoulder abduction test
Age >55
Positive ULTT A
Positive neck distraction test
3/5 80%, 4/5 95%
Mobilization w/ movement from lateral epicondyalgia
Age <49
Affected side pain free grip >112N (25.2lbs)
Unaffected side pain free grip <335N (75.3lbs)
1/3 87%, 2/3 93%, 3/3 100%
Other: Change in pain >25% following MWM
Orthotics for PFPS (Vicenzino et al 2010)
Age >25
Height <165cm
Worst pain <53.25mm (100mm VAS)
Mid-foot difference >10.96cm
Orthotic for PFPS (Barton et al 2010)
Motion controlled properties (weighted mean) >5.0
Usual pain >22.0mm
Ankle DF knee flexed >41.3deg
Reduced pain during SL squat w/ foot orthoses
Patellar Taping for PFPS
Tibial angulation >5 deg
Positive patellar tilt test
Stabilization for LBP
Age <40
SLR >91
Aberrant movement present
+ prone instability test
MODIFIED LBP stabilization CPR
Aberrant movement present
+ prone instability test
other factor: FABQ PA < 8
3+ 67%
Thoracic Manipulation for Cervical Pain "CPR T/S"
Cervical Ext ROM <30
(PA) FABQ <12
Reduced Upper t-spine kyphosis
Thirty days or less symptoms
Symptoms not distal to shoulder
looking up does not aggravate symptoms
3/6 84% 4+ 93%
Canadian C-Spine Rules
Series 1: High risk which mandate X-Ray (yes to any)
- age >65
- dangerous MOI (fall >3ft or 5 stairs, axial load to head, MVA >100km/hr, bike collision)
- paresthesias in extremities
Series 2: low risk factors to allow for safe assessment of ROM (need yes to all)
- simple rear end MVA
- sitting position in ER
- ambulation anytime post injury
- absence of mid cervical tenderness
- delayed onset of neck pain
series 3: AROM c-spine >45 (if no then X-Ray)
NEXUS Criteria X-Ray
No painful distraction injury
Evidence of normal alertness
X-Ray no focal defects
Un-Intoxicated
Sans cervical midline tenderness
NOTE: use Canadian C-spine rules over NEXUS)
NEXUS CT Scan Rule "ABC's"
Altered level of alertness
Behavior change - abnormal
Coagulopathy - clotting disorder
Deficits - neurological
Evidence of skull fracture
Frequent vomiting
Greater than 65 years old
Hematoma skull
Pilates Based Exercise for LBP
Total trunk flexion ROM 70deg or less
Duration of current symptoms 6 months or less
No symptoms in leg for past week
BMI >/= 25 (obese)
Mean hip rotation 25deg or more (either hip)
3/5 93%
AC joint cluster
cross body adduction test or scarf test
AC resisted extension
O'briens test (pain by AC joint)
3/3 80.5%
very SP
Supraspinatus Tendinopathy
age >39
painful arc
self reported popping/clicking
2 +LR 3.82, 3/3 +LR 32.3
Successful short term outcome of C-Spine Manipulation for shoulder pain
Symptomatic < 90 days
Not taking any meds for their shoulder pain
(-) Neer's
Pain-free flexion <127
IR <35 at GH 90 ABD
3/5 85%
SIJ manipulation or PFJ Mobilizations for Knee Pain
Difference in hip IR >14
Ankle DF >16
Navicular drop >3mm
No stiffness with sitting >30min
Squatting is most painful activity
>/= 4 100%
Imaging for hip OA
Painful w/ IR
Hip IR <15 deg
ESR 50
Predictors of Response to PT in hip OA
Unilateral hip pain
Age <58
Pain >6/10
40m self-pased walk test <35.9s
Duration of sx <1yr
>/=3 99%
Hand OA
Hand pain, aching or stiffness AND:
Hard tissue enlargement of 2 or more of 10 selected joints (bilateral DIP, PIP of 2nd/3rd digits and 1st CMC) AND:
- <3 swollen MCP joints and either:
1. hard tissue enlargement of 2 or more DIP joints OR
2. Deformity of 2 or more of 10 selected joints
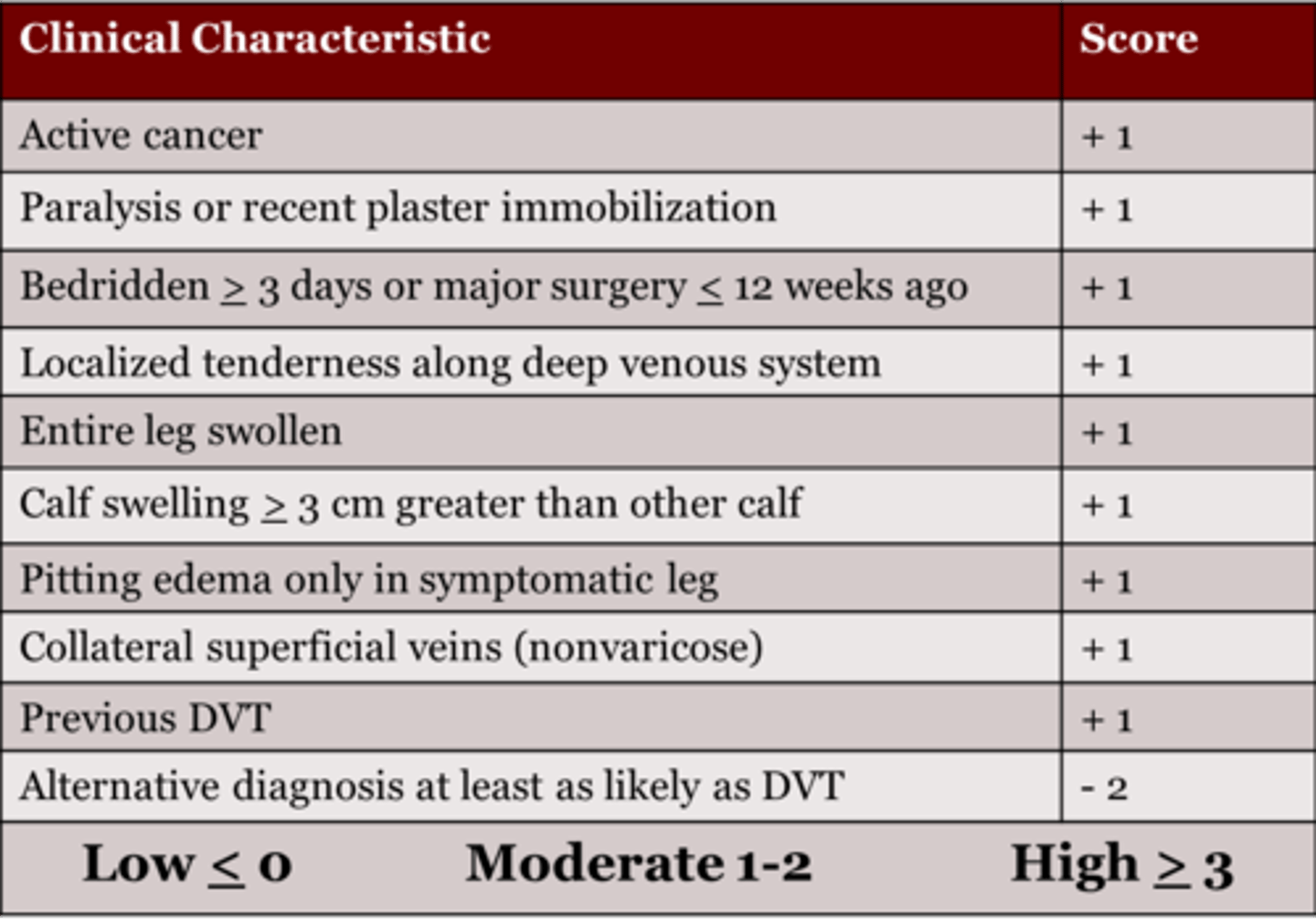
CPR for DVT "ABC's"
Active cancer
recently Bedridden >3 days or major surgery
Calf swelling >3cm
alternative Diagnosis as likely or greater than dvt
pitting Edema
Focal tenderness along deep venous system
Gross LE swelling
Has collateral superficial veins (non-varicose)
paralysis, paresis or recent plaster Immobilization of LE
1-2 17%, 3+ 75%
F/U tests: Dimer (to R/O), if (+) then US
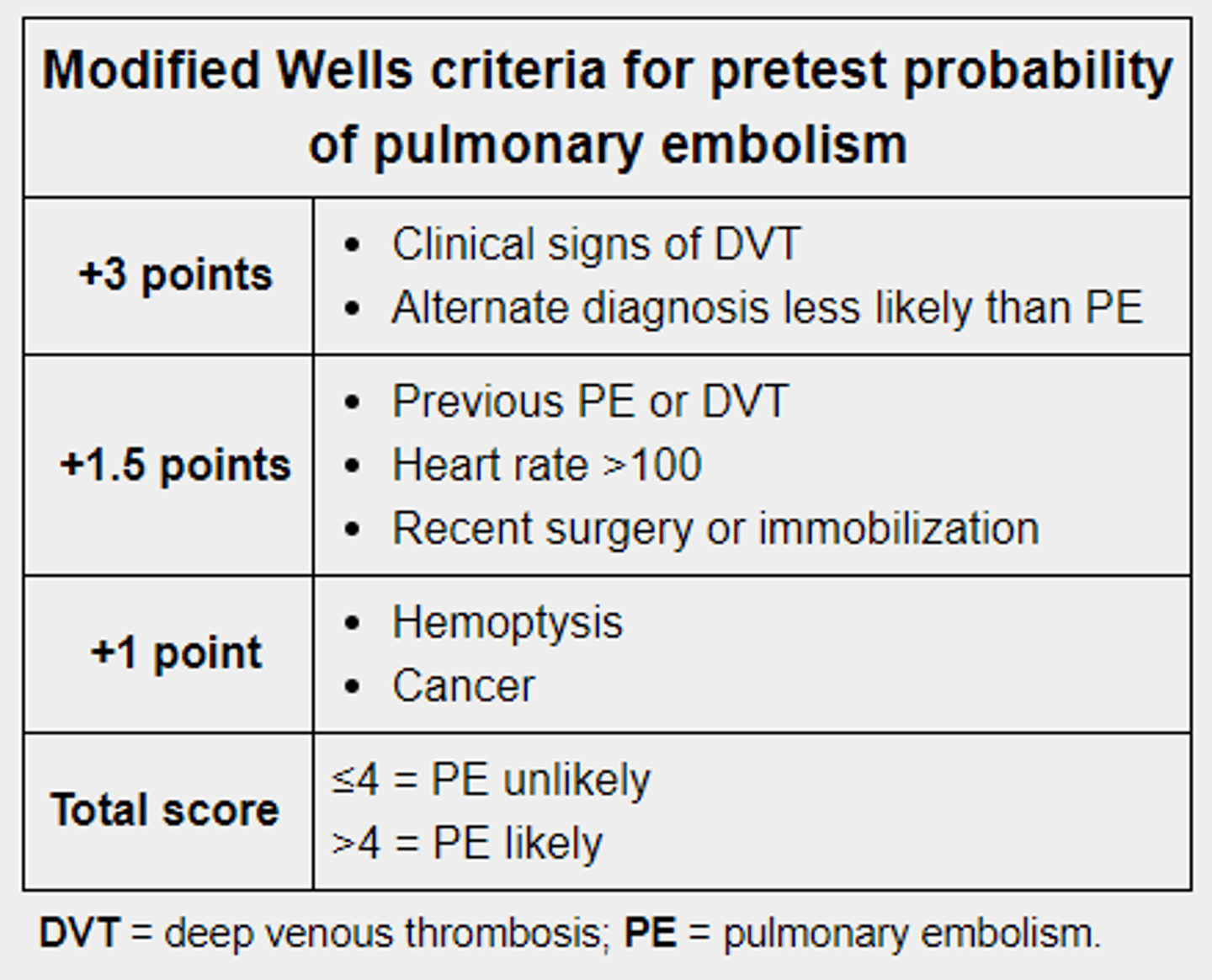
CPR for PE "PULM CPR"
Puke up blood - hemoptysis (1pt)
Unmoved from surgery last 4 weeks (1.5pt)
Lack of alternative diagnosis (3pt)
Malignancy (1pt)
Clinical signs of DVT (3pt)
Previous DVT/PA (1.5pt)
Rate of Heart >100bpm (1.5pt)
<2pts low risk, 2-6pts mod risk, >6 pts high risk
Hip Microinstability
AB-HEER
prone instability (hip)
HEER
3/3 = 95% likelihood
Beighton Score
- passive DF and hyperextension of 5th MCP >90deg (2)
- passive opposition of thumb to flexor aspect of arm (2)
- passive hyperexrtension of elbow >10deg (2)
- passive hyperextension of the knee >10deg (2)
- active forward flexion of trunk with the knees fully extended and palms flat on the floor
Adults 4/9 positive and children 6/9 positive
ACL Coper criteria
- no more than one episode of the knee "giving way"
- at least 80% LSI in timed 6m hop test
- at least 80% on KOS-ADL
- at least 60% on the Global Rating of knee function
Posterior Instability
posterior apprehension test
99% SP and only 19% SN
Inferior Instability
at least 2 directions of postiive testing w/ instability (hyperabduction test>105 SP 89%)
Beighton score >5/9 adolescent 6/9 pre pubescent
NOTE: sulcus sign tests LAXITY, not instability
SLAP/Labral Tear
2 clusters:
1. passive distraction test and active compression (SN 70% SP 90%)
2. h/o popping clicking or catching with a positive anterior slide test (SP 93% and low sensitivity)
Coronary Artery Disease
- sex and age (female >65, male >55)
- known clinical vascular disease (coronary artery, oclusive vascuar idsease, cerebrovascular disease )
- pain worse during exercise
- pain not reproducible by palpation
- patient assumes pain is of cardiac origin
3/5 SN 87%, SP 80% +LR4.52