Chapter 42: Disorders of Upper and Lower GI Systems
1/48
Earn XP
Description and Tags
1,
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
49 Terms
GI Tract
Mouth to Anus

Four cardinal signs and symptoms for GI disorders
Pain
Altered ingestion
Altered motility
Bleeding
Disorders of the Esophagus
Digestive pathway
Food and liquids enter the mouth
Mastication(Mechanical) and addition of salivary enzymes (chemical)
Voluntary transport of food and liquids
Positioned at back of throat for esophageal entry
Pushed into the esophagus
Involuntary transit to the stomach
Common manifestations of esophageal disorders
Pain, alteration in ingestion, and/or bleeding
Dysphagia
Difficulty of swallowing
Causes
Neurological deficit
Muscular disorder
Mechanical obstruction
Results/presentation
Pain with swallowing
Inability to swallow larger pieces of solid material
Difficult swallowing liquids
Causes of Dysphagia
Congenital Atresia- walls of esophagus, food can’t get to stomach
Congenital tracheoesophageal fistula- connection between esophagus and trachea; food gets in lungs
Neurologic damage to cranial nerves V, VII, IX, X, and XII
Achalasia- Walls of the esophagus don’t contract properly; food gets stuck
Esophageal Web and Rings
Thin membranes or folds that narrow the esophagus
Causes: Gastroesophageal reflux, iron deficiency anemia, and autoimmune diseases
Treatment: Dietary restrictions (soft food), Endoscopic dilation therapy
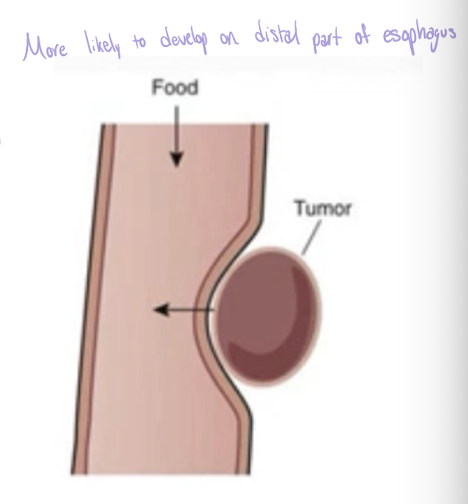
Esophageal Cancer
Primarily squamous cell carcinoma (most common distal esophagus)
Significant dysphagia in later stages
Poor prognosis due to late manifestation
Associated with chronic irritation due to: Chronic esophagitis, Achalasia, Hiatal hernia, Alcohol abuse and smoking
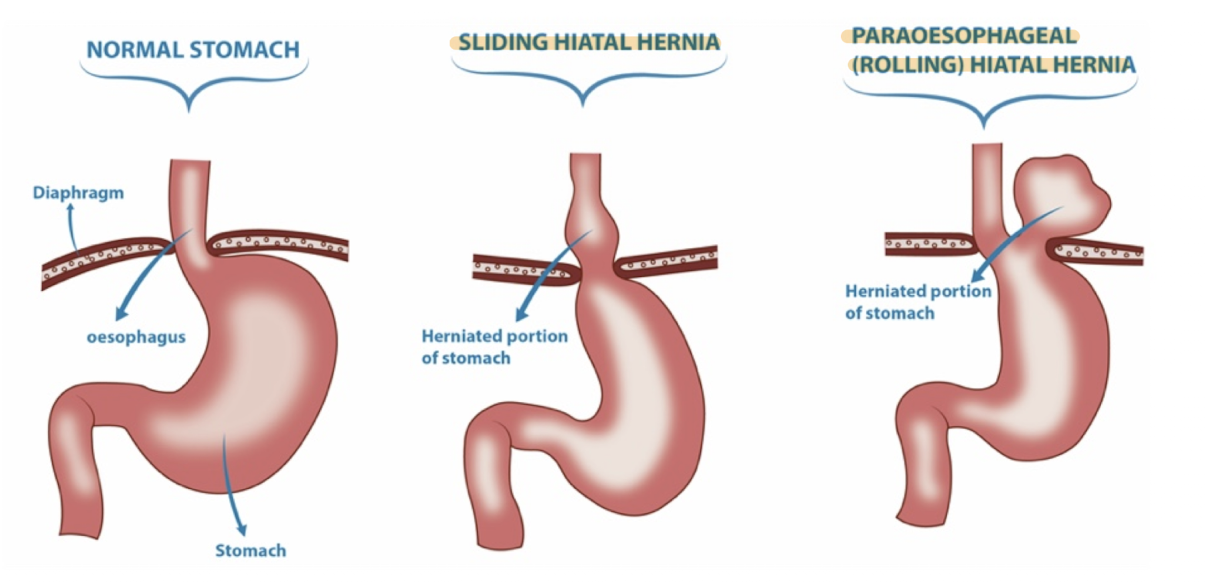
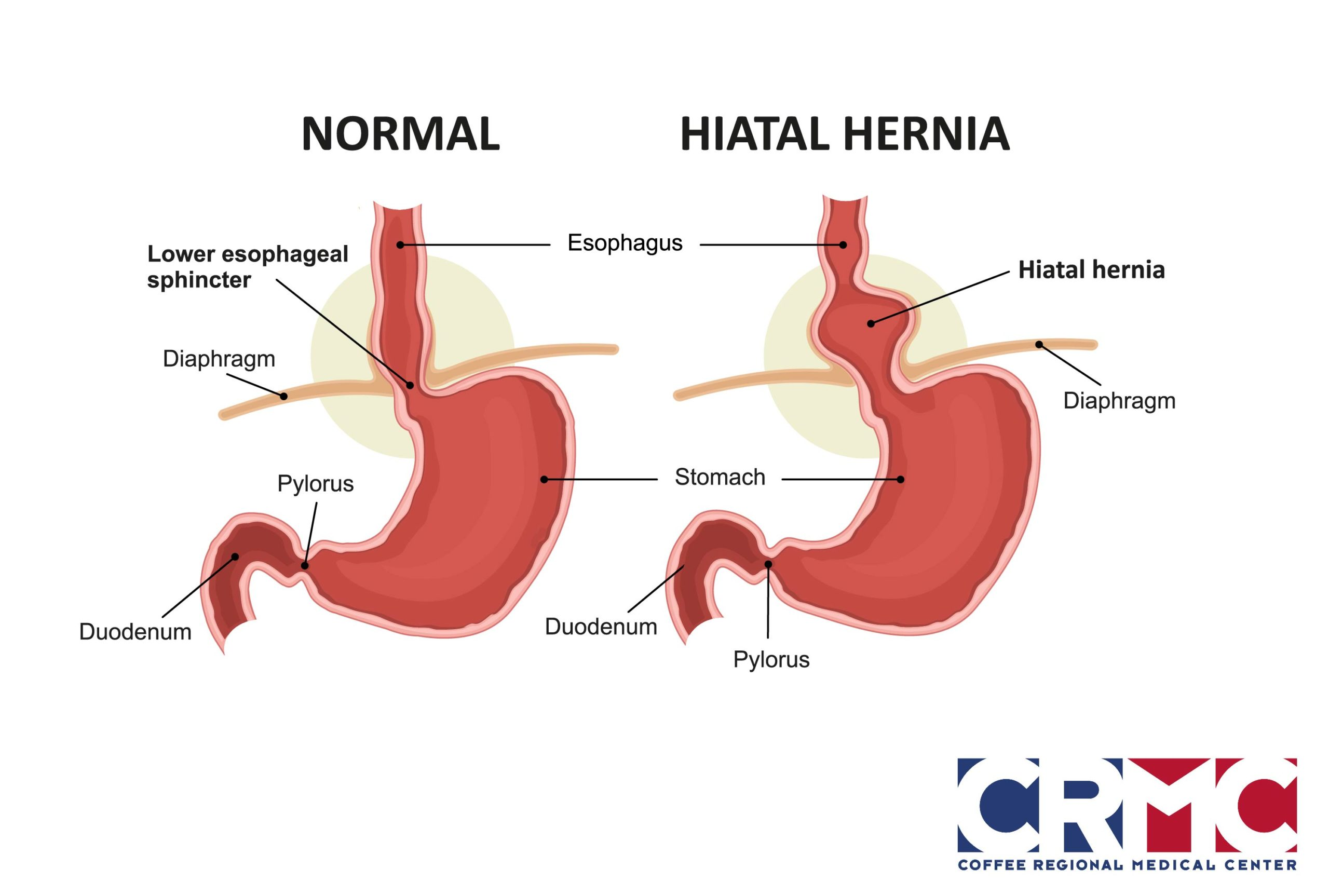
Hiatal Hernia
A hernia is a condition where an organ or tissue protrudes through a weak spot in the muscle or connective tissue that surrounds it
HH: part of the stomach protrudes into the thoracic cavity
Hiatal Hernia- Etiology and pathogenesis
Etiology
Multifactorial
May involve genetic link
Pathogenesis
Herniation of stomach through esophageal hiatus of the diagram
Lower esophageal sphincter (LES) permits reflux of gastric contents
Hiatal Hernia- Manifestations and Signs
Classified by size: I - small, IV - large
Manifestations
May be asymptomatic
Frequently involves symptoms of gastroesophageal reflux
Type IV paraesophageal hernia may produce dyspnea, reduced exercise tolerance, syncope, may cause chronic esophagitis- inflammation on walls of esophagus
Signs
Heartburn or pyrosis, frequent belching, increase discomfort when laying down, substernal pain that may radiate to the shoulder and jaw
Hiatal Hernia- treatment
Medications for symptomatic gastric reflux
Surgery may be indicated
Esophagitis
Etiology
Eosinophilic esophagitis(EoE)- Cause unknown; many associated factors
Radiation esophagitis- treatment of thoracic cancers; exacerbated by chemotherapeutic agents
Corrosive esophagitis- Ingestion of strong alkaline or acid substances
Pill esophagitis- swallowed pill lodges transversely in esophageal lumen and causes inflammation
Pathogenesis
Irritation to and inflammation of esophageal tissues lead to esophageal damage
Manifestations
vary based on etiology
Treatment
vary based on etiology
Thorough history and physical exam is required
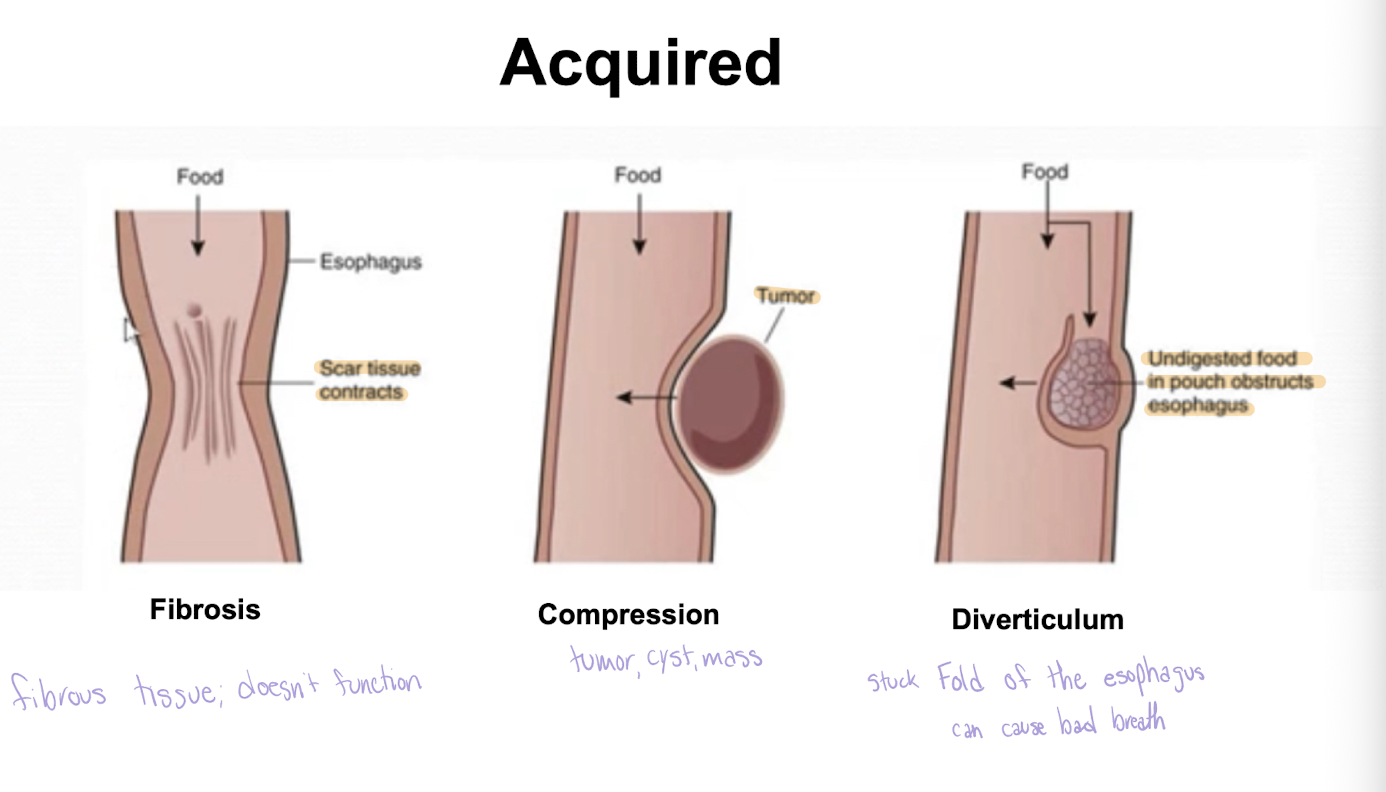
Esophageal Diverticula- Etiology and Pathogenesis
Etiology
Acquired condition
Most common cause: impaired esophageal motility
May be caused by traction on esophagus due to inflammatory disease of mediastinum (e.g., tuberculosis)
Pathogenesis
Pressure increases- esophageal lumen
Esophageal mucosa protrudes through weakened esophageal wall and produces outpouching

Esophageal Diverticula- Manifestations and Treatment
Manifestations
Most often asymptomatic
Manifestations vary based on location of diverticula
May produce dysphagia and heartburn
Treatment
Depends on size and location; surgical intervention may be needed for large diverticula
Disorders of the Stomach
Main categories of stomach disorders
Disorders of secretion
Disorders of motility
Associated cardinal GI symptoms
Pain, Altered ingestion, Altered digestion, Gastrointestinal tract bleeding
Peptic Ulcer Disease- Etiology and Pathogenesis
Etiology
Various causes
Most common: H. pylori infection and NSAID use
Contributing factors include smoking, excessive alcohol use, drug use, emotional stress, and psychosocial components
Pathogenesis
Increased gastric acid secretion or a weakened mucosal barrier leads to mucosal erosion and psychosocial components
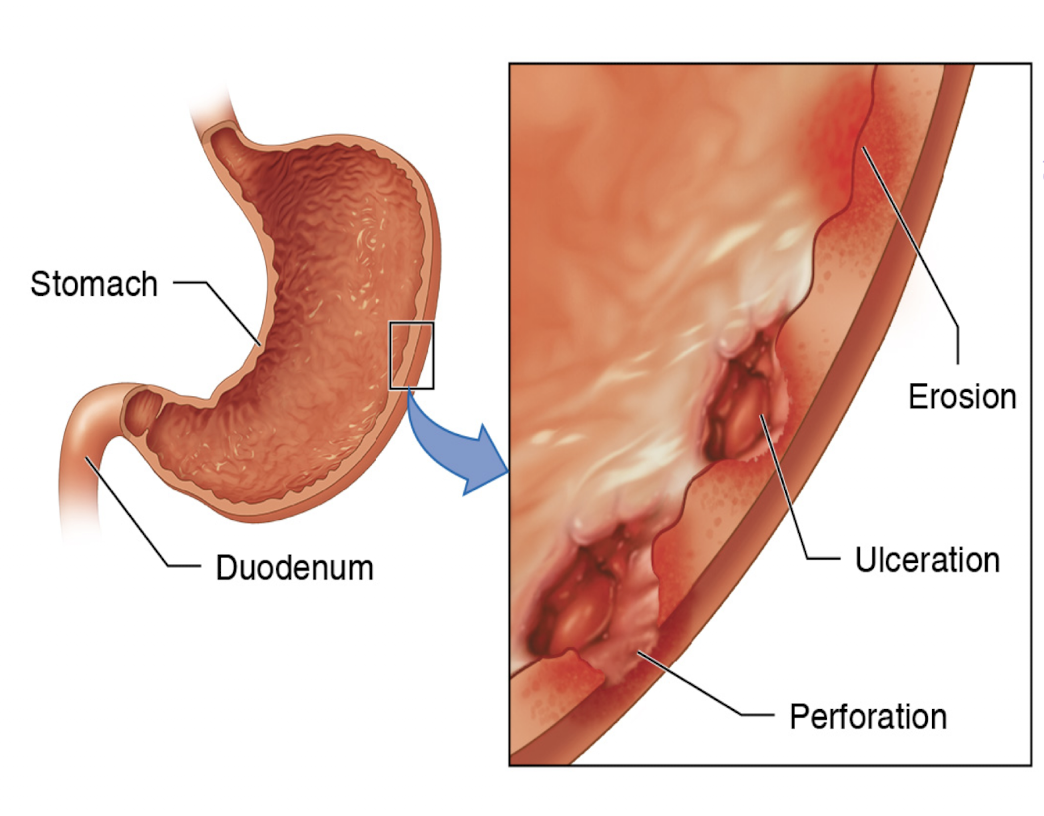
Peptic Ulcer Disease- Manifestations and Treatment
Manifestations
Common manifestations- Epigastric pain and dyspepsia(upset stomach)
Common complications- Bleeding, perforation, obstruction
Treatment
Identify causative factor
H. Pylori- triple or quadruple therapy
NSAID-induced: H2 receptor antagonist and cease NSAID
Acute Gastritis
Etiology
Infection-induced: H. pylori
Drug-induced: NSAIDs, steroids, some chemotherapeutic drugs, alcohol, and iron supplements
Ulcerohemorrhagic: physiologic stress and ischemic changes caused by shock, hypotension
Pathogenesis
Acute imbalance between mucosal injury and erosive changes with histologic presence of inflammation
Treatment
Elimination of causative agent or exacerbating factors
Eradication of H. pylori infection if indicated
Medications to treat dyspepsia
Surgical intervention for GI bleeding
Chronic Gastritis
Etiology
Infection-induced: H. pylori
Chemical and caustic agents including NSAIDs, excessive alcohol ingestion, radiation exposure
Autoimmune disease: Crohn disease, Wegener granulomatosis, and sarcoidosis
Pathogenesis
Begins with superficial gastritis
Progresses to atrophic atrophy
Gastric glandular structures are lost and/or metaplasia
Gastric atrophy is precursor to gastric cancer
Treatment
Elimination of causative agent or exacerbating factors
Eradication of H. pylori infection if indicated
Medications to enhance protection of gastric mucosa
Acupuncture
Surgical intervention for GI bleeding
Acute and Chronic Gastritis Manifestations
Most often asymptomatic or report mild dyspepsia
Potential symptoms may include abdominal pain or upset, burning sensation in chest or upper abdomen, feeling of fullness, bloating, belching, and reflux
More severe symptoms include nausea, vomiting, GI bleeding, fever, and weight loss
Gastric Outlet Obstruction- Etiology and Pathogenesis
Etiology
Includes gastric, duodenal, and/or extraluminal pathology
Malignancies of digestive organs
Surgical and interventional-induced obstruction
Metastatic cancer
Pathogenesis
Mechanical obstruction in the pyloric region
Food can’t move from stomach to duodenum
Gastric Outlet Obstruction- Manifestation and Treatment
Manifestations
Abdominal pain, distention or bloating
Vomiting, dehydration, and weight loss
May include early satiety and nausea
Treatment
Benign cases- Nasogastric tube suction, meds to suppress gastric acid production, IV fluid and electrolyte replacement, nutritional supplementation, trial liquid diet, endoscopic ballon dilation or surgery
Malignant cases- Based on underlying cause; may include stenting, chemotherapy, endoscopic ballon dilation or surgery
Advanced cancers- Palliative procedures may be preferred
Stomach Cancer- Etiology and Pathogenesis
Etiology
Risk factors include H. pylori infection, cigarette smoking, high alcohol ingestion, excessive dietary salt, inadequate fruit and vegetable consumption, and pernicious anemia
High-nitrate diet may also increase risk
Pathogenesis
Tumors or neoplasms in the stomach arise from gastric mucosa (adenocarcinoma- most common 85%)
Stomach Cancer- Manifestations and Treatment
Manifestations
Clinical manifestations are known as alarm features
Most common: Weight loss and abdominal pain
May include dysphagia, nausea, early satiety, occult GI bleeding and palpable abdominal mass
Treatment
Treatment depends on cancer staging
Upper endoscopy may be used for palliative procedures
May require endoscopic resection, radiation, chemotherapy, and/or surgical resection
Inflammatory bowel disease (IBD)
Chronic inflammatory disorder involving the GIT
2 major IBD disorders
Ulcerative colitis (UC)
Crohn disease (CD)
Inflammatory Bowel Disease- Manifestations and Treatment
Manifestations
Active: Fever, loss of appetite, weight loss, fatigue and night sweats
Remission: Symptoms may decrease and even disappear
Treatment
Optimize quality of life by treating acute processes
Induce and maintain remission
Decrease use of corticosteroids
Wholesome nutrition and healthy lifestyles habits
Anti-inflammatory agents, Immunosuppressants, Anti-tumor necrosis factor agents, Antibiotics, Probiotics
Surgery if indicated
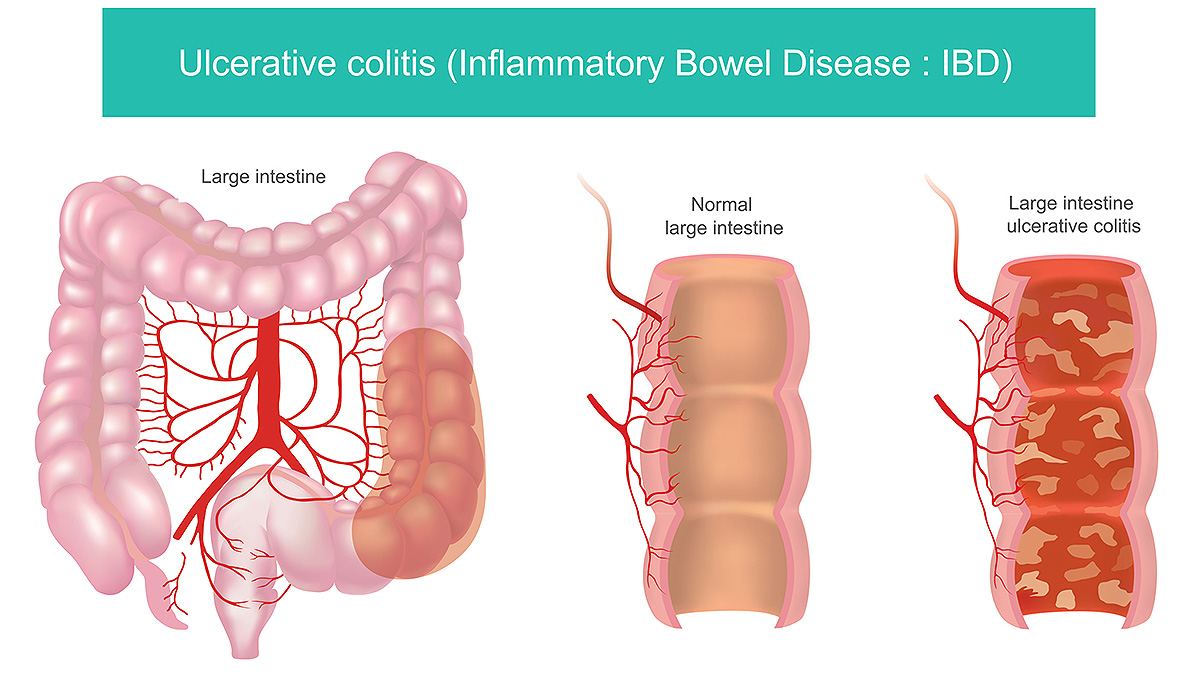
Ulcerative colitis
Chronic inflammatory condition
Limited to mucosal layers of colon
Characterized by relapsing and remitting episodes of inflammation
Develops as a continuous lesion
Ulcerative colitis- Etiology, Pathogenesis, Manifestations
Etiology
Not completely understood
Appears to involve environmental factors, microbial imbalance in the gut, genetic susceptibility, and inappropriate immune response
Pathogenesis
Inflammation of mucosal and submucosal layers of colon
Continuous lesion inflammation may extend into the proximal colon or may affect the whole colon (pancolitis)
Bowel changes include epithelial damage, inflammation, crypt abscesses, and loss of goblet cells
Manifestations
Bloody and/or mucoid, diarrhea, dehydration, and anemia
Crampy abdominal pain, pain with defecation and tenesmus
Involvement of the rectum may also lead to constipation
Crohn disease
Chronic inflammatory condition
May involve any portion of the Gastrointestinal Tract
Characterized by transmural inflammation of the bowel
Most commonly affects ileum and proximal colon
Lesions are not always continuous (skip lesions)
Crohn Disease- Etiology, Pathogenesis, Manifestations
Etiology
Not completely understood
Appears to involve environmental factors, microbial imbalance in the gut, genetic susceptibility, and inappropriate immune response
Pathogenesis
Inflammation and destruction of the bowel
Manifestations
Nausea, vomiting, and diarrhea with or without blood
Abdominal pain and pain with defecation due to anorectal fissures
Complications include bowel strictures, obstructions, perforations in the bowel and intra-abdominal abscesses
Appendicitis- Etiology and Pathogenesis
Etiology
Not fully understood
Believed to be due to appendiceal obstruction
Pathogenesis
Obstruction is thought to lead to bacterial overgrowth and luminal distention
Increased intraluminal pressure and/or excessive inflammation can inhibit blood flow causing vascular compromise to the affected tissue
Appendix may become gangrenous and can rupture
Appendicitis- Manifestations and Treatment
Manifestations
Cramping abdominal pain, tenderness with palpation of the RLQ, nausea or vomiting, increased WBC count, low-grade fever
Treatment
Gold standard- Laparoscopic surgery
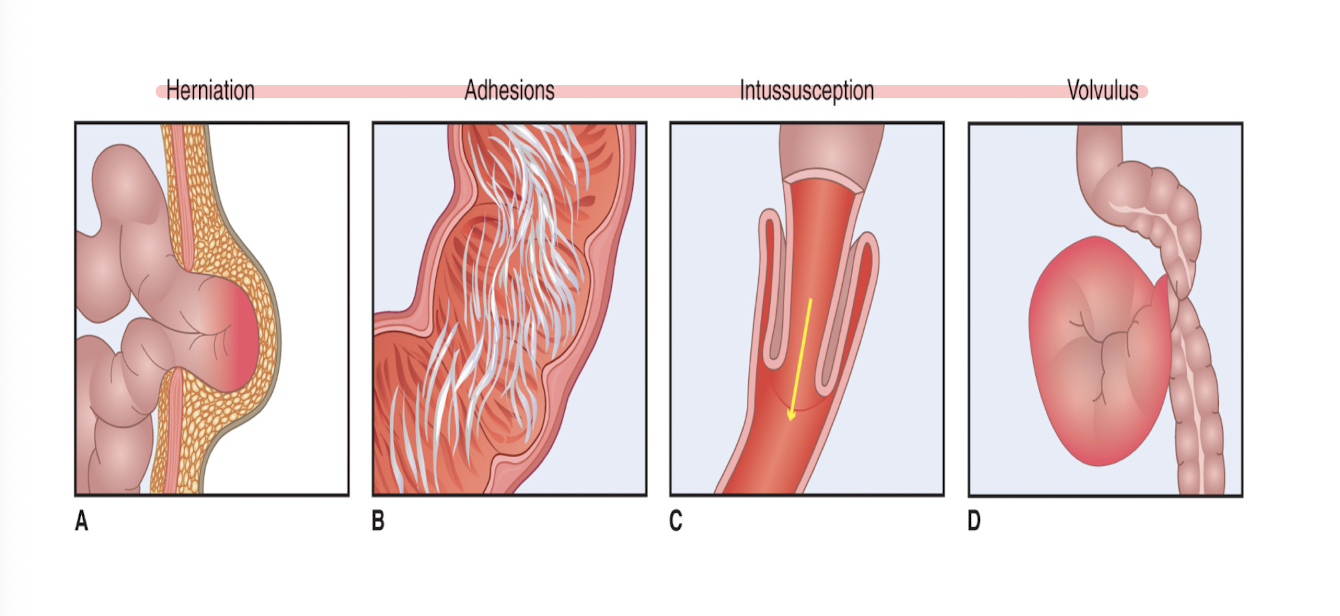
Bowel Obstruction- Etiology and Pathogenesis
Etiology
Most often due to adhesions (75%)
Other causes Hernia, Adhesions Neoplasm/tumor, Gallston ileus, Intussusception, Volvulus
Pathogenesis
Intestinal tract blockage develops due to various etiologies
Up to 80% are small bowel obstructions (SBOs)
Obstruction may be partial or complete
Complications include strangulation and bowel necrosis; may lead to bowel perforation, sepsis, and death
Bowel Obstruction- Manifestations and Treatment
Manifestations
Abdominal pain, nausea, vomiting, abdominal distention, and inability to satisfactorily pass gas or stool
Hyperactive, high-pitched bowel sounds often present
Bowel sounds will be absent if ileus develops
Treatment
Medical management includes gastric decompression, intravenous fluids, and serial physical and serum tests
Surgery may be indicated if medical management fails
If strangulation and bowel ischemia present- emergent surgery needed
Diverticula
Small outpouching (herniations) of colonic mucosa
Protrude through muscle layers of the colon wall
small, bulging pouches that form in the wall of the colon, a condition called diverticulosis
Diverticulosis
Diverticula without evidence of inflammation
Diverticulitis
Enflamed diverticula
Diverticular disease
Etiology
Associated factors include alterations in colonic wall resistance, alterations in colonic motility, low-fiver diets, NSAID use, advanced age, obesity, and lack of exercise
Manifestations
Sudden, constant abdominal pain in LLQ
Abdominal distention and nausea
Diarrhea, constipation and decreased appetite
Fever, tachycardia and hypotension
Treatments
Outpatient management: Clear liquid diet, oral broad spectrum, antibiotics, and follow up care
Inpatient treatment required if suspected peritonitis or complications present
Inpatient treatment: Administration of intravenous fluids and antibiotics, no food or drink by mouth
Surgery may be indicated; depends on size
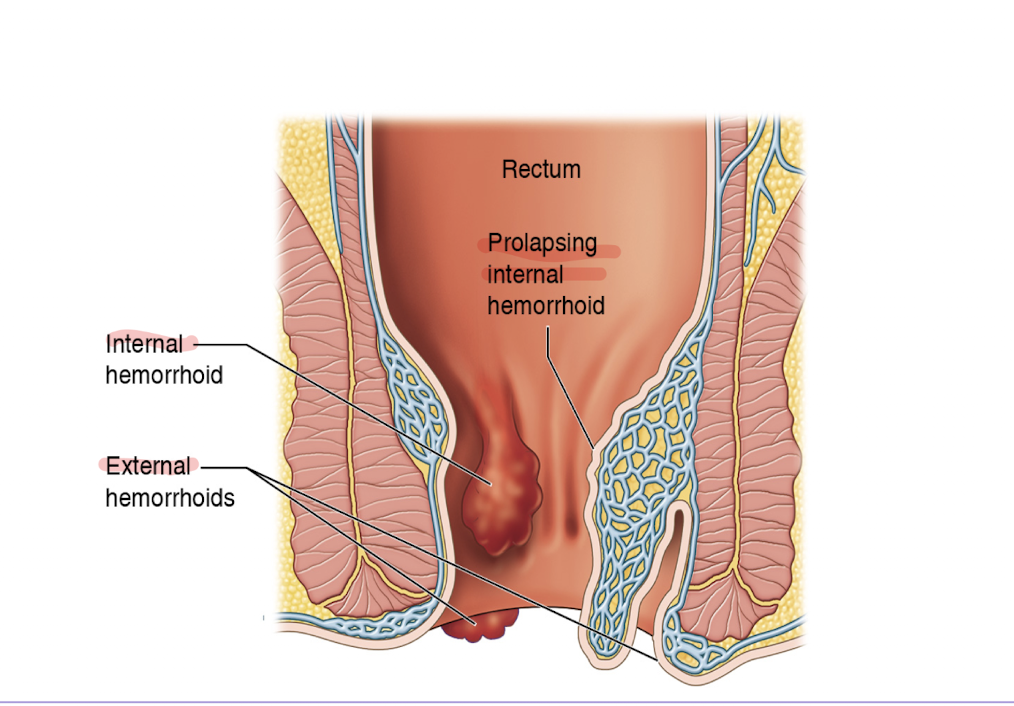
Hemorrhoids
A swollen vein or group of veins in the region of the anus
Hemorrhoidal Disease- Etiology and Pathogenesis
Etiology
Straining during bowel movement
Risk factors- conditions that increase intraabdominal pressure and/or impede venous return (e.g., pregnancy or portal hypertension)
Pathogenesis
Abnormal enlargement of the 3 vascular mucosal cushions (hemorrhoidal cushions) that assist with anal continence; can’t control pooping
Hemorrhoidal Disease- Manifestations and Treatment
Manifestations
Hematochezia, itching, perianal discomfort and soiling
Large hemorrhoid may produce sensation of incomplete evacuation
Treatment
Stage I and II: Diet modification, topical glucocorticoids, vasoconstrictors, analgesics, and sclerotherapy
Stage III and IV: Procedural interventions (e.g., hemorrhoidal banding and surgical hemorrhoidectomy)
Colorectal Masses
Adenomas (polyps) of the colon
Precursors to most most colorectal cancers (CRCs)
Benign tumors
Form in glandular structures in intestinal mucosal epithelium
Colon cancer
Malignant growth or tumor
Results from division of abnormal cells in the colon
Occurs in ascending, transverse, or descending colon
Rectal Cancer
Malignant growth or tumor
Located up to 15cm from the anal opening
Colorectal Cancer (CRC)- Pathogenesis
Genetic abnormalities plus environmental factors
Conventional adenomas and sessile serrated polyps
Commonly developmental pathways
Chromosomal instability pathy
Microsatellite instability pathway
Coloretal Cancer (CRC)- Risk factors and protective factors
Modifiable risk factors
Obesity, Sedentary lifestyle, Smoking, Moderate to heavy alcohol ingestion, Heavy consumption of red and processed meats, Low consumption of fruits and vegetables
Hereditary and medical risk factors
Family history of CRC and/or polyps, Inflammatory bowel disease (UC or CD), Type 2 diabetes, Aging
Protective Factors
Diet rich in whole-grain fiber, Use of NSAIDs (Ex: aspirin)
Colorectal Cancer(CRC)- Manifestations
Typically asymptomatic
Numerous potential manifestations
Hematochezia and symptoms of anemia
Change in bowel habits
Weight loss and fatigue
Generalized or localized abdominal pain
Advanced Colorectal Cancer (CRC)- potential manifestatiosn
Physical assessment
Distended abdomen
Palpable abdominal mass and lymph nodes
Rectal cancer- palpable mass on digital exam
Right-sided cancers (ascending colon)
Usually silent
May become painful
May develop palpable mass in RLQ
Tumors stay to one side of the colon wall
Tumors stay to one side of the colon wall
Unlikely to develop intestinal obstruction
Dark red blood in stool
Left-sided tumors (descending colon)
Tumors grow circumferentially around the colon
Stools may become long and pencil-like
Can lead to intestinal obstruction
Bright red blood in stool
Colorectal Cancer (CRC)- Diagnosis
Screening for CRC
Early detection is essential
Screening methods
Lower GI endoscopy, fecal tests for occult blood and DNA testing for mutant genes
Screening recommendations
Begin screening at age 50
Individuals with predisposing genetic factors
Begin screening earlier than age 50
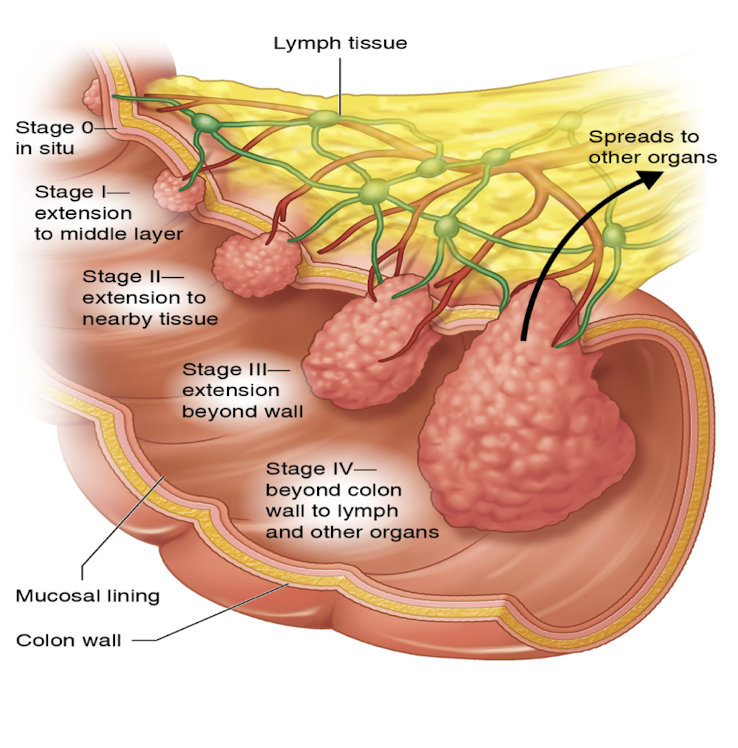
Colorectal Cancer (CRC)- Staging
Used to determine treatment
Usually includes TNM classification
Tumor, lymph nodes, and metastases
Endoscopy may be used for staging
Stage I- extension to middle layer
Stage II- extension to nearby tissue
Stage III- extension beyond wall
Stage IV- beyond colon wall to lymph and other organs
Colorectal Cancer (CRC)- Treatment
Depends on nature and metastasis of CRC
Surgery
Most often used to treat CRC that has not spread
Adenomas may be removed during endoscopy
If cancer extends beyond the bowel wall
Additional interventions may be indicated
Chemotherapy with or without radiation
Organ- or tissue-specific therapy