Looks like no one added any tags here yet for you.
Hyperparathyroidism
overproduction by the parathyroid glands
Paget's disease
- bone disease of unknown cause characterised by the excessive breakdown of bone tissue, followed by abnormal bone formation
- incidence ~3% 40+
- some clustering in families
Osteoporosis
a condition in which the bones become fragile & break easily
Osteomalacia
abnormal softening of bones in adults
- Bone weakness due to defective mineralisation of osteoid matrix
– On biopsy see increased surface osteoid plus decreased mineralisation
– Can get increased osteoid w/ normal mineralisation during rapid bone turnover eg.Pagets, HPT, near fracture site
Normal bone remodelling - Bone Remodelling Unit
- coordinated sequence of events (3-4 months)
- bone removal
- bone formation
Bone removal:
- osteoclast activation (via osteoblasts)
– resorption of bone matrix & mineral
Bone formation:
- activation of osteoblasts
– formation of new bone matrix (osteoid)
– mineralisation of bone matrix (delay of 6-12 days)
– reversal (cement) lines mark the limits of each BRU
What controls bone formation?
- local physical factors act as the trigger for remodelling
– parathormone receptors found on osteoblasts
– vitamin D
Control of bone formation: Local physical factors
- sensed by osteocytes within bone lacunae
- release cytokines or other substances
Control of bone formation: Parathormone receptors
net effect of actions is to increase blood calcium
Control of bone formation: Vitamin D
- needed for the resorbing action of PTH in bone
- 1,25 diOH vitD
> increases intestinal calcium absorption
> promotes bone mineralisation
What is parathormone?
- Hormone secreted by parathyroid glands
- Controls imbalanced levels of calcium & phosphate in the blood & tf
- Influences levels of excitability
What is the action of parathormone: Bone?
– increases numbers of osteoblasts & osteoclasts
– activates osteoblasts which, in turn, activate osteoclasts (probably via PGE)
– inhibits matrix production by osteoblasts
– stimulates production of proteases by osteoblasts
What is the action of parathormone: Kidney?
- increased calcium resorption by tubules
- increased phosphate excretion
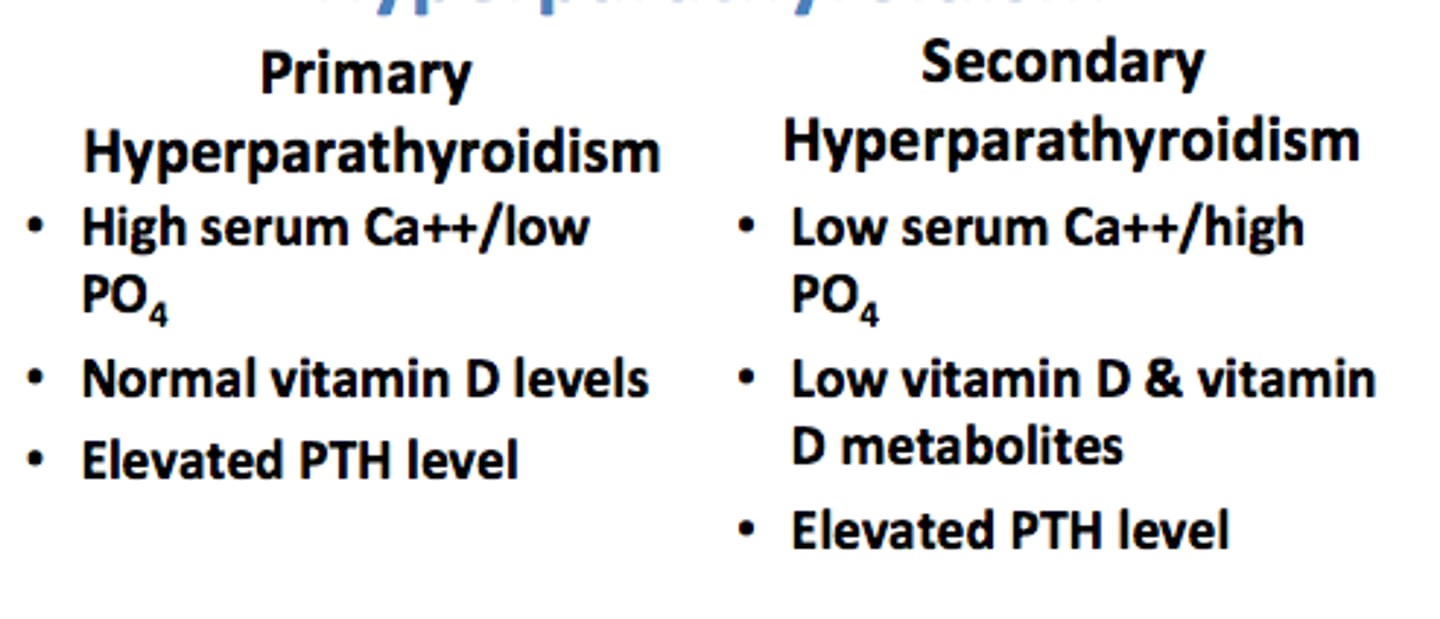
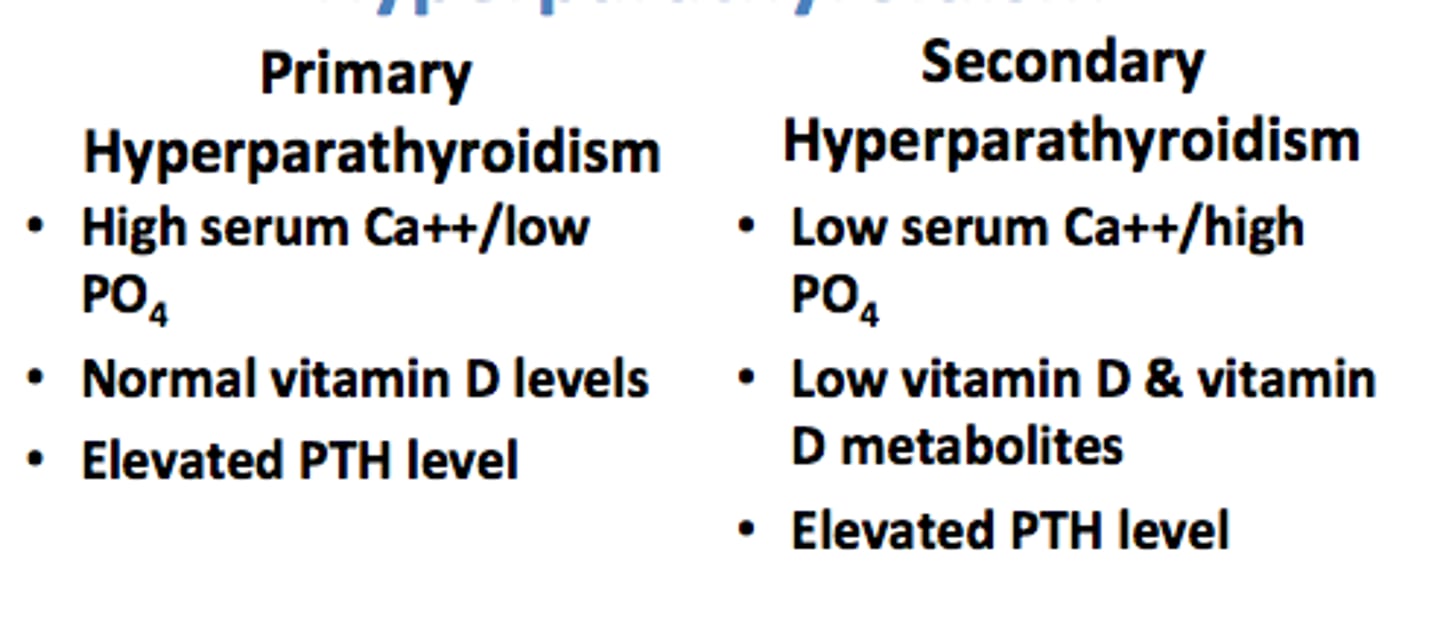
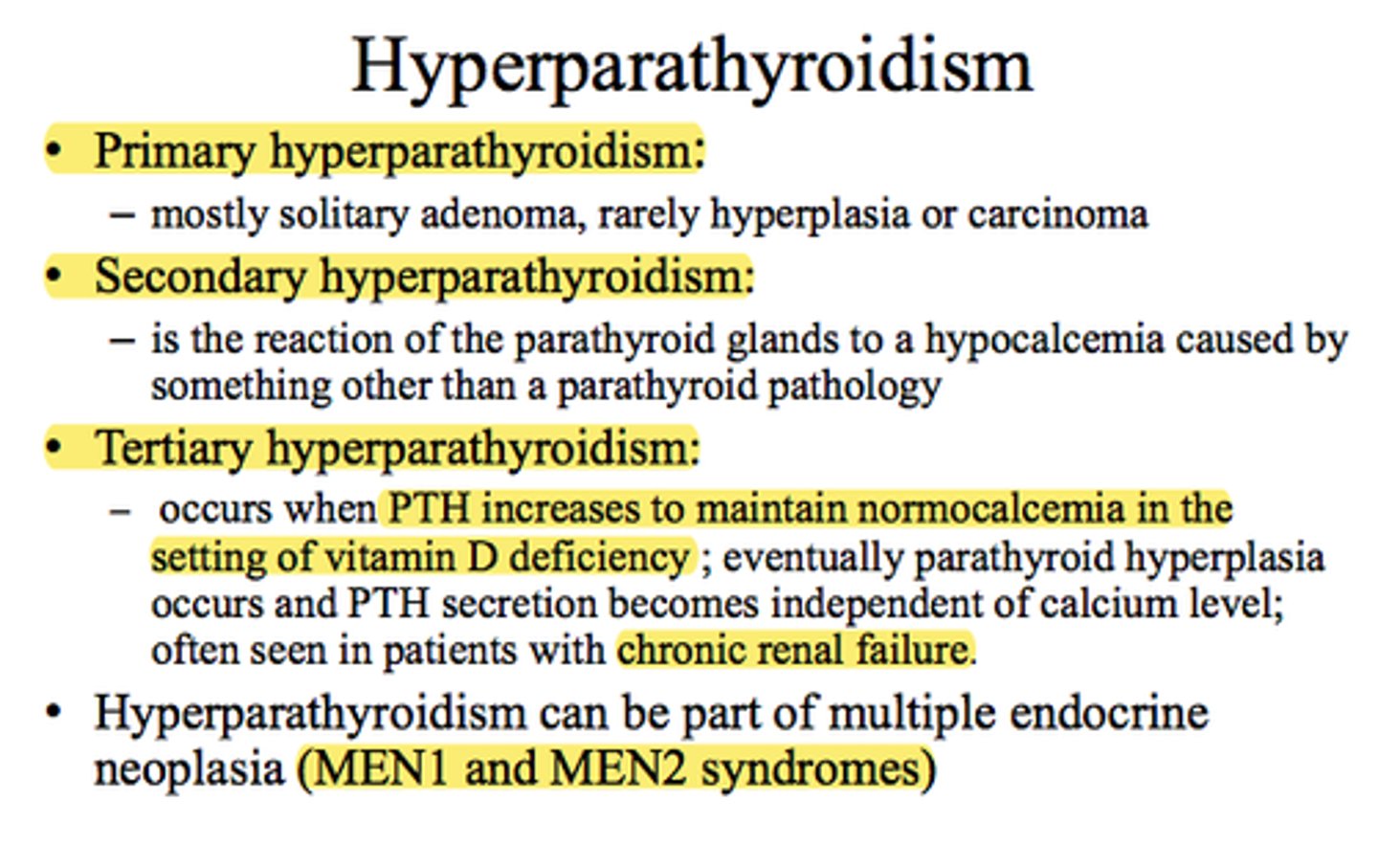
Primary hyperparathyroidism:
raised hyperparathyroid hormone
- 80% due to solitary adenoma
– typically F, peak age 45y
– usually asymptomatic
– detected on biochemical screening (raised Ca & low PO4 raised ALP)
– if severe: bone pain & fractures muscle weakness & renal calculi
Where are the two places in the body alkaline phosphatase is found?
- liver
- osteoblasts
Secondary hyperparathyroidism:
– raised PTH in response to persistent hypocalcaemia (renal failure, vit.D deficiency, hypophosphataemia)
– all glands enlarged & hyperplastic
Tertiary hyperparathyroidism:
- secondary HPT plus autonomous nodules
- tx of cause does not reverse parathyroid changes
What are bone changes which can be seen through radiology in hyperparathyroidism?
Hands:
- resorption of tufts of terminal phalanges
– subperiosteal erosions of sides of phalanges
- localised lytic areas in shafts of long bone, ribs, jaw & skull (brown tumours)
Bone pathology of hyperparathyroidism: Bone (oesteitis fibrosa)
- excessive osteoclastic activity, lacunae & tunnelling resorption
- excessive osteoblastic activity
- marrow fibrosis
- lytic lesions
Bone pathology of hyperparathyroidism: Soft tissue
metastatic calcification: vessel walls, alveoli, skin, renal tubules, renal calculi
What is the aetiology of Paget's?
– unknown, but may be related to virus infection of bone cells
– paramyxovirus-like inclusion found in osteoclasts
– viral antigens shown by IHC
– measles virus & RSV possibilities
? canine distemper virus implicated (unproven)
How does Paget's disease present radiographically?
– Mainly sacrum & pelvis, spine, skull & femur
– In long bones starts at end of bone & spreads towards diaphysis
Spectrum of changes:
– initially osteolytic (flame defect)
– osteoblastic phase: increased endosteal & periosteal new bone (bone scans useful)
– inactive phase: residual increased bone
Pathology of Paget's disease:
– increased osteoclastic resorption plus fibrosis affecting cortical & trabecular bone
– increased osteoblastic activity produces woven bone
– random replacement causes mosaic appearance of cement lines
- late phase: thickened, mosaic bone, little activity
What are the general clinical presentations of Paget's?
– Usually no symptoms, signs or biochemical abnormalities
Focal manifestations:
– bone expanded (skull enlargement)
– bone softened: deformities – spine curves forward, femur & tibia bow anteriorly & laterally, pelvic deformities
– nerve compression: cranial nerves in foramina, sc (thoracic) causes lower limb signs
What are the clinical presentations of Paget's? Local complications
- fracture (particularly femur & tibia)
- tumours (osteosarcoma - pelvis, skull, femur, humerus)
What are the systemic manifestations of Paget's disease?
- cardiovascular: increased CO if extensive dx
- biochemical:
> raised ALP due to osteoblastic activity
> raised urinary hydroxyproline due to bone breakdown
> occasionally get hypercalcaemia & hypercalciuria, hyperuricaemia & gout
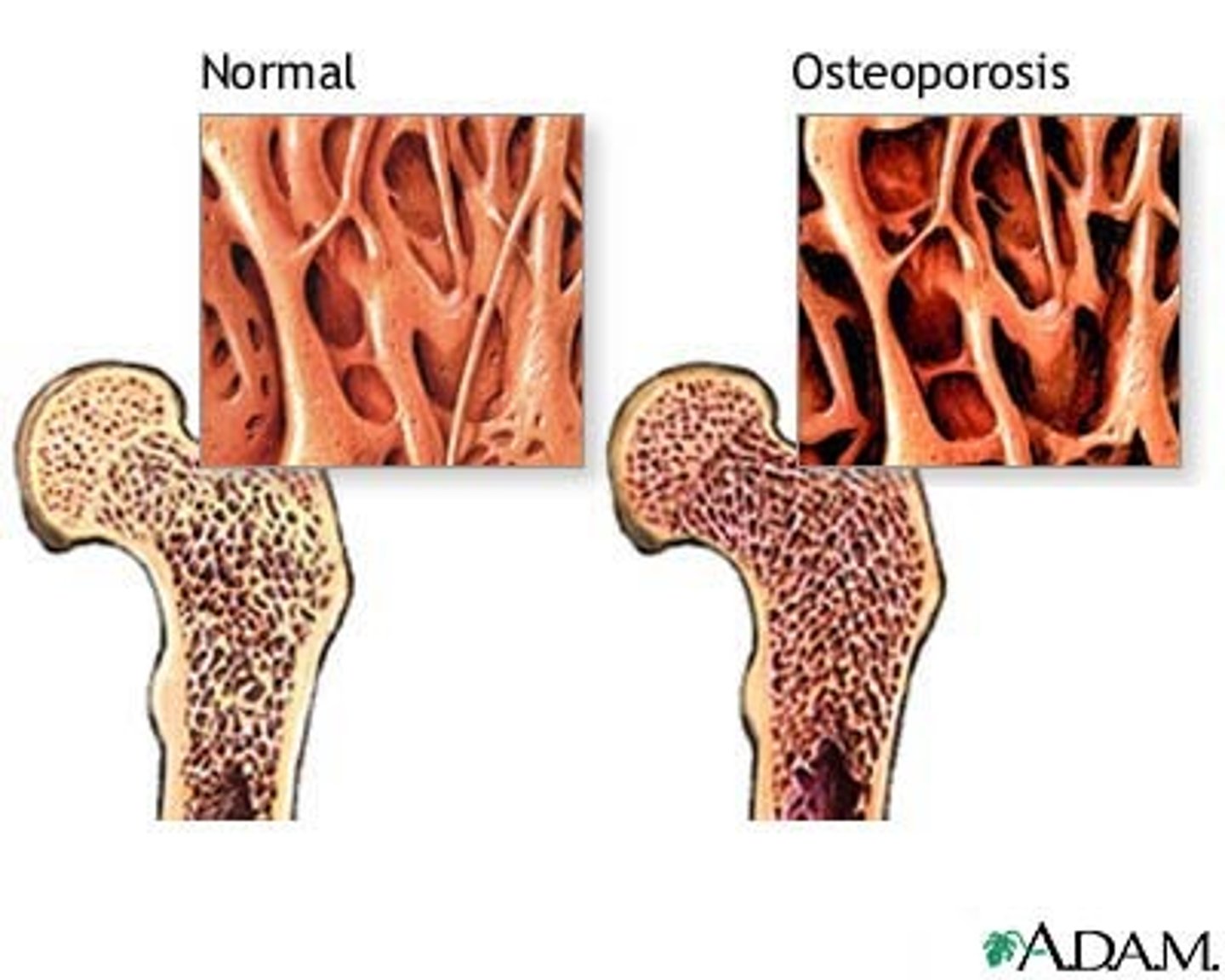
What are the effects of osteoporosis on bone?
– Reduction in trabecular bone mass (i.e. trabecular thickness & number)
– Bone remains qualitatively normal (i.e. proportions of mineralised & unmineralised bone remain normal)
When does bone mass peak in adults with osteoporosis?
30-40y, then decreases particularly in F
> Osteoporosis = 1SD or 2SD below normal for age & sex
> Trabecular bone volume (TBV) <11% then likely to get vertebral fractures
What are possible causes of decreased bone mass?
– decreased bone formation
– increased bone resorption
– any combination of (a) & (b)
N.B. different cellular mechanisms may be important when considering tx
What is an idiopathic aetiological cause of osteoporosis?
idiopathic/involutional
– postmenopausal loss of oestrogens
– decreases Ca absorption
– increases Ca excretion
– accompanied by increased bone remodelling activity (net BL)
What are some other aetiological causes of osteoporosis?
– Immobilisation: increases osteoclastic activity
– Malabsorption of calcium
– Collagen disturbances: scurvy, OI
– Homocystinuria
– Endocrine: Cushing's, steroid therapy (increased resorption)
– Hyperthyroidism, acromegaly
– Hypogonadism
– Cellular proliferation: mast cells, haemopoietic cells, neoplasia
What is a clinical manifestation for osteoporosis?
- predominantly a dx of postmenopausal, elderly F
– fractures
> in <70 mainly trabecular loss (vertebral # (L thoracic & U lumbar spine. Loss of height))
> in >70 (cortical & trabecular loss – femoral # (37500 hip # per year))
> also proximal humerus & distal radius often after trivial trauma
How is a diagnosis of osteoporosis formed?
– bone biopsy of iliac crest
– correlates well w/ vertebral loss
– needs good standardisation
– single photon or dual photon absorptiometry (Dexascan)
How is osteoporosis treated?
- Oestrogen replacement
– Exercise to increase preMP bone mass (?postMP)
– Ca, vitamin D – probably little effect
– Fluoride: increases trabecular bone mass but decreases cortical mass (only used for severe vertebral OP - 1/3 don't respond)
– Etidronate (blocks osteoclasts to decrease resorption)
What is the aetiology of osteomalacia?
vitamin D related
- Vitamin D deficiency: diet, sunlight
– Vitamin D malabsorption: ileal/pancreatic disease
– Impaired vitamin D metabolism: liver/renal disease
– Increased vitamin D catabolism: enzyme induction
– Phosphate depletion & hypophosphataemia: increased PTH, congenital, metabolic acidosis, Fanconi syndrome
– Inhibition of mineralisation: diphosphonates, F-, aluminium (dialysis pts)
– Hypophosphatasia
What are general clinical manifestations of osteomalacia in adults?
– bone pain & tenderness
– deformities - bowing of limbs, pigeon chest, spinal
– muscle weakness (type 2 fibre atrophy)
– X-ray: density of bone may be increased or decreased (osteoid is denser than marrow)
– pseudofractures (Looser's zones)
– cortical microfractures w/ poorly-formed callus
What are general clinical manifestations of osteomalacia in children?
rickets
- failure of calcification of epiphysial cartilage
– disordered, continued cartilage proliferation
– widened & irregular growth plate
– flaring of the metaphysis.