WRIST POSITIONS
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
CARPAL CANAL
TANGENTIAL PROJECTION:
GAYNOR-HART METHOD
CARPAL BRIDGE
TANGENTIAL PROJECTION
LENTINO
TRAPEZIUM
PA AXIAL OBLIQUE PROJECTION
CLEMENTS-NAKAYAMA METHOD
*alignment WITH ulnar deviation
TRAPEZIUM
PA AXIAL OBLIQUE PROJECTION
CLEMENTS-NAKAYAMA METHOD
*alignment WITHOUT ulnar deviation
SCAPHOID SERIES
PA AND PA AXIAL PROJECTIONS
RAFERT-LONG METHOD- ULNAR DEVIATION
PERPENDICULAR to midcarpal area
STRUCTURE SHOWN
Carpal spaces are better demonstrated compared with PA projection.
Distal radius
Distal ulna
Radiocarpal joint (the scaphoid, lunate, and triquetrum)
Ulnocarpal joint (lunate and triquetrum)
Carpal bones
Bases of the 1st–5th metacarpals
CR & SS
AP PROJECTION
PATIENT POSITION
Seat the patient at the end of the radiographic table.
POSITION OF PART
Arm and hand supinated
Elevate digits to place the carpals in close contact with the IR.
Have the patient lean laterally to prevent rotation of the wrist
CR:
PERPENDICULAR to midcarpal area
STRUCTURES SHOWN
SLIGHT OBLIQUE PROJECTION OF THE ULNA.
SCAPHOID with self-superimposition.
Distal radius
Distal ulna
Radiocarpal joint
Ulnocarpal joint
Eight carpal bones
Bases of the metacarpals
Soft tissue of the wrist
CR & SS
PA PROJECION
PATIENT POSITION
Seat the patient low enough. This position places the shoulder, elbow, and wrist joints in the same plane to permit right-angle rotation of the ulna and radius for the lateral position.
POSITION OF PART
Flex the digits to place the wrist in close contact with the film.
The CR is angled 30° cephalad (toward the elbow), elongating the scaphoid and capitate.
The CR is angled 30° caudad (toward the fingertips), elongating the capitate only.
CR AND SS
PA PROJECION
DAFFNER, EMMERLING, AND BUTERBAUGH METHOD
Purpose: Better demonstrate the scaphoid and capitate.
CR
PERPENDICULAR TO THE WRIST JOINT
STRUCTURES SHOWN
A LATERAL PROJECTION OF THE:
PROXIMAL AND DISTAL CARPALS
PROXIMAL METACARPALS
DISTAL RADIUS AND ULNA
RADIOCARPAL JOINT
LATERAL POSITION (EXTENSION) LATEROMEDIAL PROJECTION
POSITION OF PART
Have the patient flex the elbow 90 degrees to rotate the ulna to the lateral position.
Center the IR to the wrist (radiocarpal) joint.
Adjust the forearm and hand, placing the humeral epicondyles and styloid processes superimposed and perpendicular to the IR, so that the wrist is in a true lateral position
CR
PERPENDICULAR TO THE WRIST JOINT
STRUCTURE SEEN
Specifically demonstrates: Carpal boss (3rd CMC joint).
Distal radius and ulna
Radiocarpal joint
Carpal bones in lateral profile
Proximal metacarpals
CR AND SS
PALMAR FLEXION (LATERAL POSITION)FIOLE METHOD
Position:
Wrist in palmar flexion.
Purpose:
Best demonstrates the carpal boss (carpe bossu).
CR
PERPENDICULAR to wrist joint
STRUCTURE SHOWN
Specifically demonstrates: Scaphoid in lateral profile.
Distal radius and ulna
Radiocarpal joint
Carpal bones in lateral profile
Proximal metacarpals
Scaphoid in lateral profile, achieved by rotating it anteriorly into a dorsovolar position.
PALMAR FLEXION (LATERAL POSITION)
Burman et al. Method
Position:
Wrist in palmar flexion.
Purpose:
Obtains a lateral view of the scaphoid.
Part position:
Palmar flexion rotates the scaphoid anteriorly into a dorsovolar position, producing a lateral profile.
CR
Perpendicular to the midcarpal area (center of the wrist).
STUCTURE SHOWN
*BEST FOR PISIFORM
*Demonstrates the carpals on the MEDIAL SIDE OF THE WRIST
*TRIQUETRIUM, HAMATE and PISIFORM free of superimposition and in profile.
Best demonstrates the pisiform and the medial-sided carpals of the wrist, with the triquetrum, hamate, and pisiform shown in profile and free of superimposition.
AP OBLIQUE PROJECTIONMEDIAL ROTATION
Thumb goes IN = Internal (Medial) Rotation
POSITION
Rotate the wrist medially (internally) until it forms semisupinated position of approx. 45 degrees to the IR.
CR
Perpendicular to the midcarpal area
STRUCTURE SHOWN:
Demonstrates the carpals on the LATERAL SIDE OF THE WRIST, particularly the trapezium and the scaphoid.
PA OBLIQUE PROJECTIONLateral rotation
POSITION
From a pronated position, rotate the wrist laterally (externally) 45 degrees
CR
Perpendicular to the midcarpal area
PA OBLIQUE with Ulnar Deviation
- used when the scaphoid is under examination
CR: PERPENDICULAR to the SCAPHOID.
CR angulation of 10 to 15 degrees proximally or distally is sometimes required for clear delineation.
STRUCTURE SHOWN
CORRECTS FORESHORTENING OF THE SCAPHOID
(foreshortening is a type of shape distortion in which an object appears shorter and thicker.)
opens interspaces between the carpals on the lateral side of the wrist.
PA OBLIQUE with Ulnar Deviation or Flexion
Move the elbow away from the patient’s body.
Turn the hand outward until the wrist is in extreme ulnar deviation.
CR:
PERPENDICULAR to the midcarpal area.
STRUCTURE SHOWN
opens interspaces between the carpals on the medial side of the wrist.
PA OBLIQUE with Radial Deviation
Move the elbow towards the patient’s body.
Turn the hand medially
CR:
PERPENDICULAR to the table and directed to enter the scaphoid
STRUCTURES SHOWN:
Places the scaphoid at right angles to the CR and it is projected without self-superimposition.
PA Axial Projection Stecher Method
POSITION OF PART
Remember: 20 - 20
Finger end elevated 20°.
The horizontal or central ray is directed 20° towards the elbow (cephalad)
Note: reverse if the fracture line angles SUPERIORINFERIORLY.
Hand flat (0° elevation) + 20° cephalad CR
Or
20° hand elevation + CR perpendicular (0°)
CR:
PERPENDICULAR to the table and directed to enter the scaphoid
STRUCTURES SHOWN:
Places the scaphoid at right angles to the CR and it is projected without self-superimposition.
PA Axial Projection Stecher Method
BRIDGMAN METHOD
- Same position as the Stetcher method but with ULNAR DEVIATION.
CR:
PERPENDICULAR and with multiple cephalad angles; with the hand and wrist in the same position for each projection, four separate exposures made at 0, 10, 20, and 30 degrees cephalad
STRUCTURE SHOWN
The scaphoid is shown with minimal superimposition
PA AND PA AXIAL PROJECTIONS
RAFERT-LONG METHOD- ULNAR DEVIATION
PURPOSE:
diagnosing scaphoid fractures using a four-image, multiple-angle CR series
POSITION OF PART:
Position the wrist on the IR for a PA projection.
Without moving the forearm, turn the hand outward until the wrist is in extreme ulnar deviation
CR:
Angled 45 degrees distally to enter the anatomic snuffbox of the wrist and pass through the trapezium
STRUCTURE SHOWN:
The trapezium demonstrated free of superimposition by the other carpal bones except at its articulation with the scaphoid
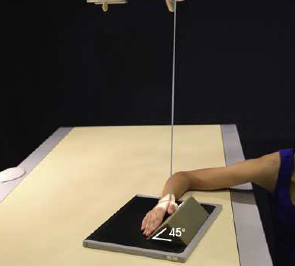
TRAPEZIUM
PA AXIAL OBLIQUE PROJECTION
CLEMENTS-NAKAYAMA METHOD
POSITION OF PART: 45-45
Place the wrist in the lateral position, resting on the ulnar surface over the center of the IR.
Place a 45-degree sponge wedge against the anterior surface, then rotate the hand to come in contact with the sponge.
CR:
1 ½ inches proximal to wrist joint / (superoinferior ) with caudal angle of 45
degrees.
STRUCTURE SHOWN:
The carpal bridge is shown on the image i
Show fractures of the scaphoid, lunate dislocations, calcifications, and forei
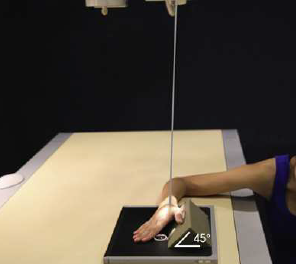
CARPAL BRIDGE
TANGENTIAL PROJECTION
LENTINO.
POSITION OF PART:
Lie palm up, forming a right angle to the forearm.
Central Ray (CR)
Perpendicular to the carpal canal (directed through the carpal tunnel).
Structures Shown (SS)
Carpal canal (carpal tunnel) in tangential profile.
Hook of the hamate.
Pisiform.
Palmar aspects of the trapezium and tubercles of the scaphoid.
Useful for detecting fractures, bony abnormalities, or calcifications within the carpal canal.
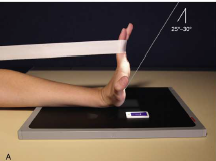
CARPAL CANAL
TANGENTIAL PROJECTIONGAYNOR-HART METHOD
POSITION OF BODY
Wrist hyperextended.
Long axis of the hand is adjusted to vertical as possible
Central Ray (CR)
Perpendicular to the carpal canal (directed through the carpal tunnel).
Structures Shown (SS)
Carpal canal (carpal tunnel) in tangential profile.
Hook of the hamate.
Pisiform.
Palmar aspects of the trapezium and tubercles of the scaphoid.
Useful for detecting fractures, bony abnormalities, or calcifications within the carpal canal.
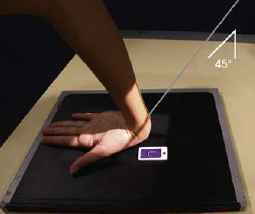
MARSHALL
Suggested placing a 45° angle SPONGE under the palmar surface of the hand to slightly elevate the wrist to place the carpal canal tangent to the central ray.