UNIT 3 Congenitally corrected transposition of great arteries
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
Explain congenitally corrected transposition of the great arteries and why blood still travels in the correct direction.
(what is it categorized by - b/c of this what type of blood flow is maintained?)
What is it also known as? list 4
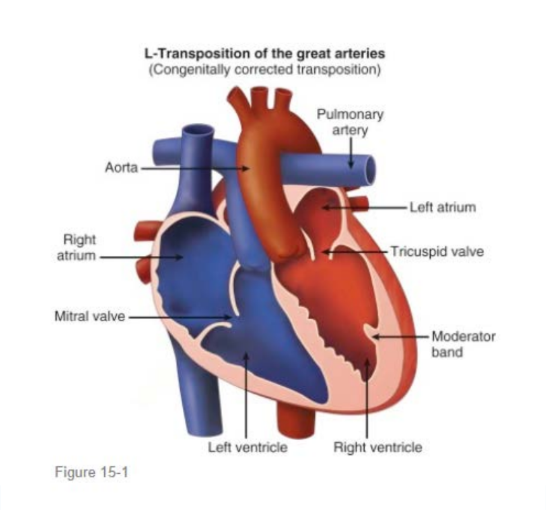
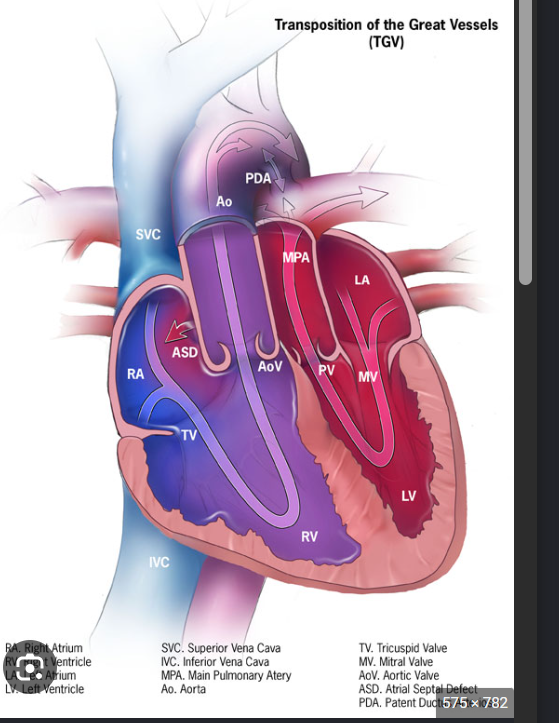
Congenitally corrected transposition of the great arteries, or CCTGA, is a cardiac structural abnormality with double discordance:
Atrioventricular discordance
Ventriculoarterial discordance
Because there are 2 abnormal connections, the blood is redirected back into the correct circulation.
Also known as LTGA, Double discordance, physiologically corrected TGA, and ventricular inversion
Describe the blood-flow pathway in CCTGA.
Systemic venous deoxygenated blood enters the right atrium
The right atrium connects through the mitral valve to the morphologic LV
The morphologic LV pumps deoxygenated blood into the pulmonary artery
Oxygenated blood returns to the left atrium
The left atrium connects through the tricuspid valve to the morphologic RV
The morphologic RV pumps Oxygenated blood into the aorta
Simple reminder:
The ventricles and great arteries are both switched, so circulation is physiologically corrected.
What relationship do the tricuspid and mitral valves have with the ventricles in CCTGA?
Each AV valve remains connected to its corresponding morphologic ventricle:
Tricuspid valve goes with the morphologic RV (The TV is septophillic)
Mitral valve goes with the morphologic LV (MV is septophobic)
What is abnormal about the tricuspid valve in CCTGA?
The tricuspid valve is located on the left side and is almost always abnormal. Because it functions as the systemic AV valve, it is exposed to high systemic pressures and may develop regurgitation.
What happens to the subpulmonary infundibulum in CCTGA?
There is no normal subpulmonary infundibulum. It is replaced by mitral valve–pulmonary valve fibrous continuity.
Subpulmonary = under the pulmonary valve
Infundibulum = funnel/outflow tract
In a normal heart, the pulmonary valve sits above the RV, and there is a muscular outflow portion of the RV leading up to the pulmonary valve. That area is the subpulmonary infundibulum.
In CCTGA, the pulmonary valve is connected to the morphologic LV, not the normal RV outflow area. There is no muscle/funnel separating the mitral valve from the pulmonary valve. Instead, the mitral valve and pulmonary valve are close together and connected by fibrous tissue.
What happens to the membranous septum in CCTGA?
The membranous septum becomes enlarged and may contribute to outflow tract obstruction.
Where are the morphologic ventricles located and what circulation does each one support? - what are the new names for the ventricles
The morphologic LV becomes the subpulmonary ventricle
The morphologic RV becomes the subaortic or systemic ventricle
Normal heart:
RV → pulmonary artery → lungs
LV → aorta → body
But in CCTGA:
Morphologic LV → pulmonary artery → lungs
So the LV is subpulmonary = sitting under/connected to the pulmonary artery.
Morphologic RV → aorta → body
So the RV is subaortic = sitting under/connected to the aorta.
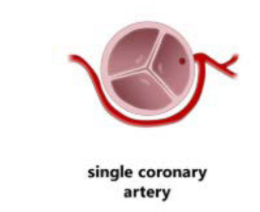
Describe the coronary artery anatomy in CCTGA.
The coronary arteries follow the anatomy of their respective morphologic ventricles, although a single coronary artery is common.
Are the systemic and pulmonic veins are connected normally to the atria?
Yes, The systemic and pulmonic veins are connected normally to the atria
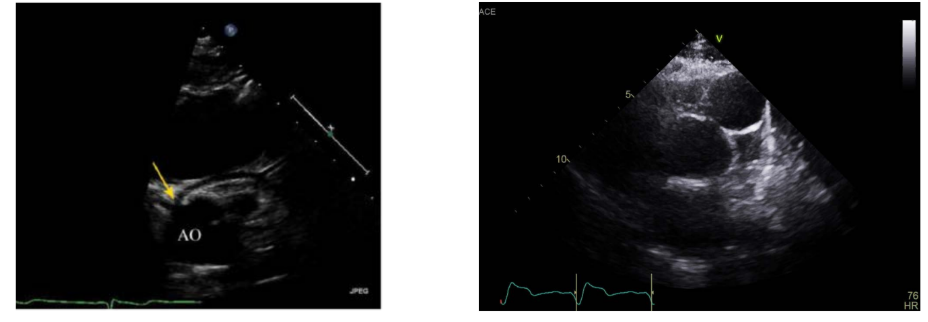
Describe the position of the aorta and pulmonary artery in CCTGA.
Aorta is positioned leftward and anterior to the pulmonary artery
(The normal is aorta is rightward and posterior to the pulmonic valve)
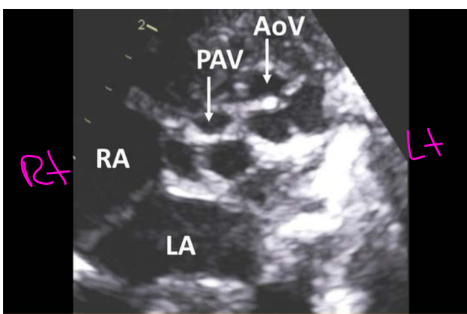
How do the proximal portions of the great arteries course?
They run parallel rather than crossing normally.
Why is the conduction system abnormal in CCTGA?
Leftward looping causes malalignment between the atrial and ventricular septa. This disrupts the normal conduction pathway and changes the position and course of the AV node and bundle of His.
50% Develop what abnormal conduction pathway?
Approximately 50% may develop third-degree AV block.
How common is CCTGA?
CCTGA is uncommon and makes up approximately 0.5% of all congenital heart defects
What is the usual Van Praagh classification for CCTGA?
S, L, L
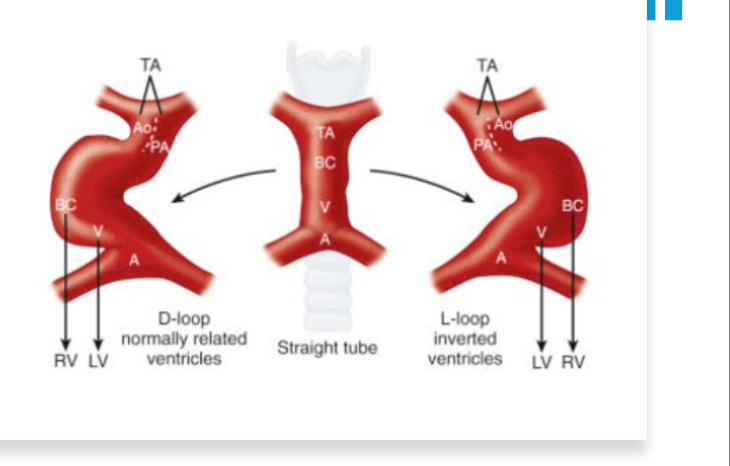
Explain the embryologic cause of CCTGA.
Abnormal leftward looping of the heart tube causes:
Atrioventricular discordance
Ventriculoarterial discordance
(blubs lopping anterior - inferior and to the left - abnormal)
Where does the cardiac apex point in most patients with CCTGA? In 75% of the time
The apex points to the left (in approximately 75% of patients.)
Why can the systemic right ventricle eventually fail in CCTGA?
(talk about the morphologic RV & it features and what its designed to do? & what happens In CCTGA, Over decades, what does the RV struggle to maintain? List 2 things this often leads too?)
The morphological right ventricle is heavily trabeculated and designed for
low-pressure pulmonary circulation
• The RV is acting as the systemic ventricle
• Over decades, it struggles to maintain the high-pressure systemic load, often leading to….
Progressive RV dysfunction (Progressive RV dilation)
Progressive Heart failure
Why does systemic tricuspid regurgitation develop in CCTGA? & List 3 things this may cause?
The left-sided tricuspid valve functions as the systemic inflow valve. It is not designed to tolerate systemic pressure over a lifetime.
This may cause:
Annular dilation
Tricuspid regurgitation
Worsening RV failure
(Progressive systemic RV volume overload)
Why can complete heart block occur in CCTGA?
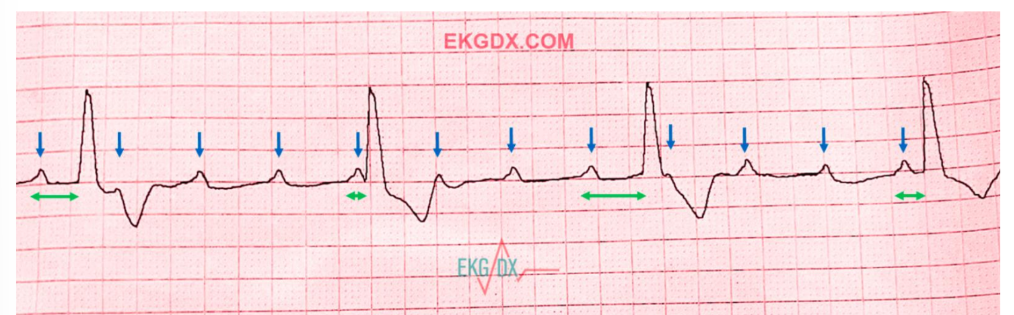
Complete heart block can occur because the AV node and bundle of His have an abnormal location and an elongated conduction pathway.
How may CCTGA present clinically:
When is it detected? Many patients are what? and are diagnosed during routine what evaluation - list 2
CCTGA may remain undetected until adulthood. Many patients are asymptomatic and are diagnosed during routine chest X-ray or ECG evaluation.
List the 2 common presenting symptoms of CCTGA.
Cyanosis
Dyspnea
List the 4 main causes of symptoms in CCTGA.
(Other common presenting symptoms are cyanosis and dyspnea these are a result of…)
These are a result of failing RV or tricuspid valve
• Or from associated anomalies such as LVOTO and a large VSD
If an LVOTO (aka what is it called) is present, it reduces what?
what does it alter list two, and may Contribute to what clinical presentation list 2
If an LVOTO Aka Sub - pulmonary obstruction is present, it reduces pulmonary flow
It can:
Reduce pulmonary blood flow
Alter right-sided pressure
Alter left-sided volume
Contribute to cyanosis & dyspnea
What percentage of patients with CCTGA have associated defects?
More than 90% have associated defects.
List the 5 associated defects of CCTGA.
Ebstein anomaly
VSD
Dextrocardia or mesocardia
Right aortic arch
Aortic coarctation
Describe the VSD commonly associated with CCTGA. list 2 things
The VSD is commonly:
Membranous or perimembranous
Nonrestrictive / Large
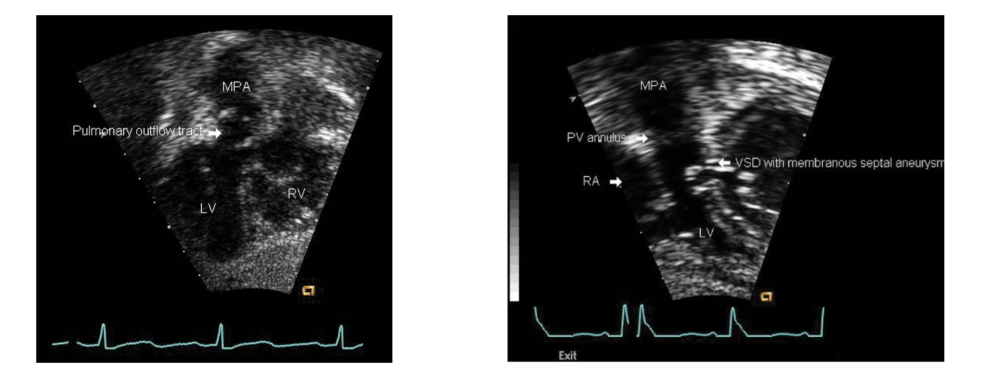
What causes subpulmonary outflow tract obstruction?
It may be caused by:
Caused by a fibrous ridge or aneurysm from the excessive membranous tissue (subpulmonary)
membranous septum, which is the thin/fibrous part of the septum near the AV valves and outflow area.
The word “subpulmonary” just tells you where it is located:
subpulmonary = under the pulmonary valve / under the pulmonary outflow tract
So the slide means:
Extra fibrous membranous septal tissue
→ forms a ridge or bulges like an aneurysm
→ sits under the pulmonary valve
→ can narrow/block flow going to the pulmonary artery/lungs.
Echo findings:
List the beginning steps of the subcostal evaluation for CCTGA.
you should begin by establishing what?
Sweep to determine the what position in the chest
What analysis should you be performing name 3
Begin by establishing visceral situs
Sweep to determine the cardiac position in the chest
Perform segmental analysis of the atria, ventricles, and great arteries
^Identify the morphologic ventricles
^Determine the great-artery connections
What venous connections should be demonstrated?
Both:
Pulmonary venous connections
Systemic venous connections
How should the great-artery connections be determined?
Determine great artery connection through sweeps and color to follow each ventricle into its connected great artery.
List the 6 features used to identify the morphologic RV.
slightly apical displaced of the tricuspid valve septal leaflet hinge point
Trileaflet tricuspid valve
Chordal attachments to the ventricular septum
Moderator band
Irregular, heavily trabeculated endocardial surface
Crescent-shaped ventricular cavity
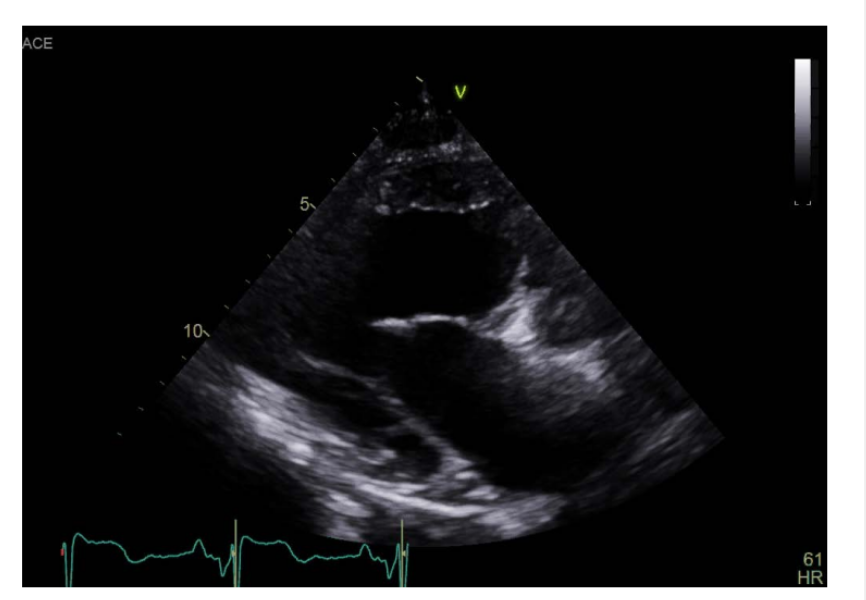
How can the morphologic LV be differentiated from the morphologic RV? List 5
The morphologic LV typically has:
Bullet shaoed
Smooth walls
MV is bileaflet
No attchments to the ventricular septum (septophobic)
Two papillary muscles
Why may obtaining a normal PLAX view be difficult in CCTGA?
What may be visualized by moving the PLAX view more where?
The abnormal ventricular and great-artery positions change the usual heart orientation, so Pulling more laterally will show the parallel great arteries
List the 3 main PLAX assessment goals.
Demonstrate the parallel great arteries
Assess for VSDs - Typically perimembranous due to large membrane
Evaluate the enlarged membranous septum and outflow tracts
Why are VSDs commonly perimembranous in CCTGA?
The abnormal outflow alignment creates a large membranous septal region, making perimembranous VSDs common.
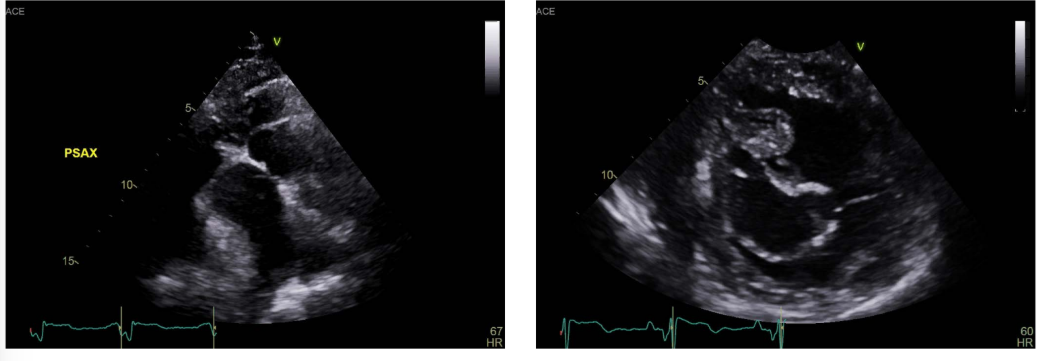
List the 4 assessment goals from PSAX.
Demonstrate the orientation of the what valves
Demonstrate the what arteries
what should you Evaluate for the ventricle? list 2
And Assess for what shunt
Demonstrate the orientation of the semilunar valves
Demonstrate the coronary arteries
Evaluate ventricular morphology and function
Assess for VSDs
What inflow-valve feature should be evaluated to help identify the tricuspid valve and morphologic RV?
Look for inflow valve attachments to the septum
List the 2 assessment goals from the apical views.
And in Ebstein's anomaly List the 2 assessment goals
How do you Evaluate for left sided RV function with what 3 dopplers?
Identify the morphologic ventricles
Evaluate the outflow tracts for location and obstruction using color and spectral Doppler
Ebstein's anomaly:
• Evaluate the amount of TR and TS
• Perform dimensionless index
• Evaluate for left sided RV function
• TAPSE, S’, FAC %
For CCTGA SSN view what 3 things do we look for?
Look for arch sideness, dimensions, and coarctation
List the 2 main differentials for CCTGA.
D-transposition of the great arteries (known to cause cyanosis baby)
Ebstein’s anomaly
How are asymptomatic patients without major associated defects managed
They may require lifelong monitoring by a congenital cardiologist.
List the 3 medication classes used when ventricular weakness or volume/pressure overloads that lead to congestive heart failure
ACE inhibitors
Beta blockers
Diuretics
Approximately 45% may need a what for heart block.
Approximately 45% may need a pacemaker for heart block. (3rd AV block)
When may an ICD be used? list 2
An implantable cardioverter-defibrillator may be used in patients with:
Moderate-to-severe systemic RV dysfunction
Increased risk for dangerous ventricular arrhythmias
What are the 2 general surgical approaches for CCTGA? which Treatment option is #1?
Treatment option #1 Physiologic repair –palliative approach (help control volume inside the heart)
“double” switch operation = anatomic approach
What is repaired during a physiologic repair? List 4
This may include:
PA banding
VSD closure for moderate to large VSDs
Surgically relief of tricuspid valve stenosis or regurgitation with TVR
May require transplantation in RV systemic failure - for a worse case
(Goal is to make the LV the systemic ventricle again and the RV the Pulmonary ventricle again)
TVR usually stands for tricuspid valve replacement.
Associated defects are corrected while the morphologic RV remains the systemic ventricle.The morphologic RV continues pumping against systemic pressure, so systemic RV failure and systemic tricuspid regurgitation may still progress.
Treatment option #1 = physiologic –palliative approach:
What does PA banding, train the LV to become?
Train the LV to become the systemic ventricle with pressure build up
PA banding = makes the LV pump against higher pressure.
That strengthens the LV.
Then the LV may be ready to become the systemic ventricle later.
Treatment option #1 = physiologic –palliative approach:
VSD closure for what VSDS?
list 2 device used? also used for what?
VSD closure for moderate to large VSDs
• Patch or occluder device
• Also used for ventricle switch
VSD used for ventricle switch = use that hole as a doorway to redirect LV blood to the aorta/body. The VSD is not always just “closed.” Sometimes the surgeon uses the VSD as part of the new pathway to connect the LV to the aorta, then patches around it to direct flow correctly.
What is the goal of a double-switch repair?
The goal is to make the morphologic LV the systemic ventricle and the morphologic RV the pulmonary ventricle.
What are the 2 stages or components of a double-switch repair?
Part 1 Atrial switch / Atrial redirection
Part 2 ventricular redirection or Great artery switch
Part 1 Atrial switch:
what are baffled to the mitral valve and what are baffled to tricuspid valve
What is the purpose of the atrial switch? ^
Pulmonary veins → mitral valve/LV → aorta
SVC/IVC → tricuspid valve/RV → pulmonary artery
The atrial switch redirects systemic and pulmonary venous blood to the opposite ventricles.
Part 2 ventricular redirection or arterial switch
Explain the Rastelli component of CCTGA repair. & What is the goal of the Rastelli procedure?
The Rastelli procedure includes:
An LV-to-aorta baffle routed through the VSD
with an RV-to-pulmonary artery conduit
What is the goal of the Rastelli procedure? It redirects the morphologic LV to the aorta so the LV becomes the systemic ventricle
What is done during an arterial switch or ____procedure - whats the name? What does this establishes?
The aorta and pulmonary artery are transected and reconnected to the appropriate ventricles.
This establishes the morphologic LV as the systemic ventricle.
Transected = cut apart so they can be moved and reattached.
Post surgical Imaging in CC-TGA list 5 things we assess?
WHAT IS THE NUMBER 1 THING WE EVALUATE !!!!!!!!
• Look for baffle leaks and obstructions
• Assess the amount of inflow regurgitation
• Evaluate for outflow tract obstruction
• NUMBER 1 ***Evaluate ventricle function****
• If present, look at RV to PA conduit for stenosis or regurgitation