Ocular Hypotensive Agents - Clinical Ocular Pharmacology Spring 2026
1/281
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
282 Terms
Currently, what is the ONLY universally accepted method of glaucoma treatment?
lowering IOP
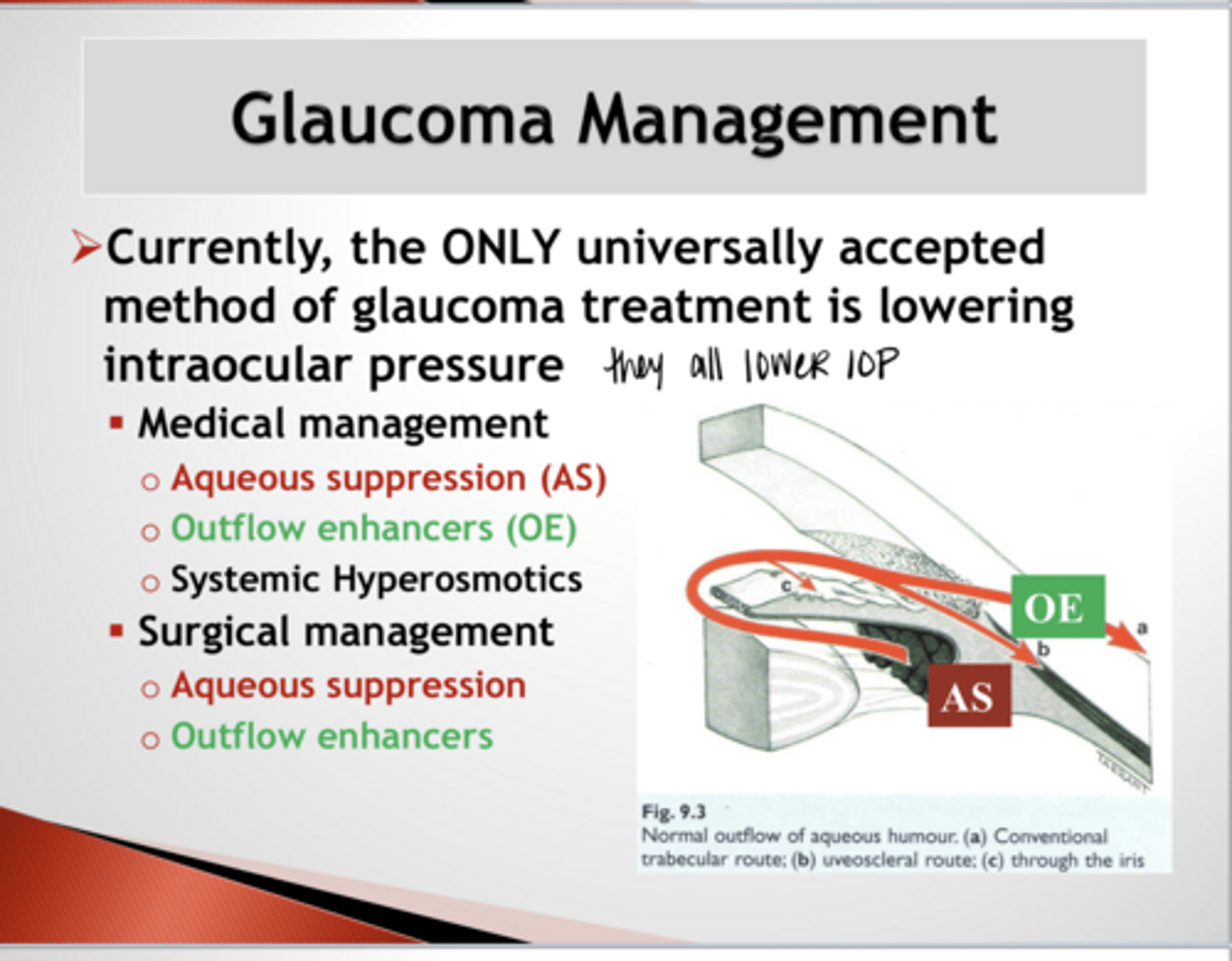
What are the medical management options of glaucoma management?
Aqueous suppression (AS)
Outflow enhancers (OE)
Systemic hyperosmotics
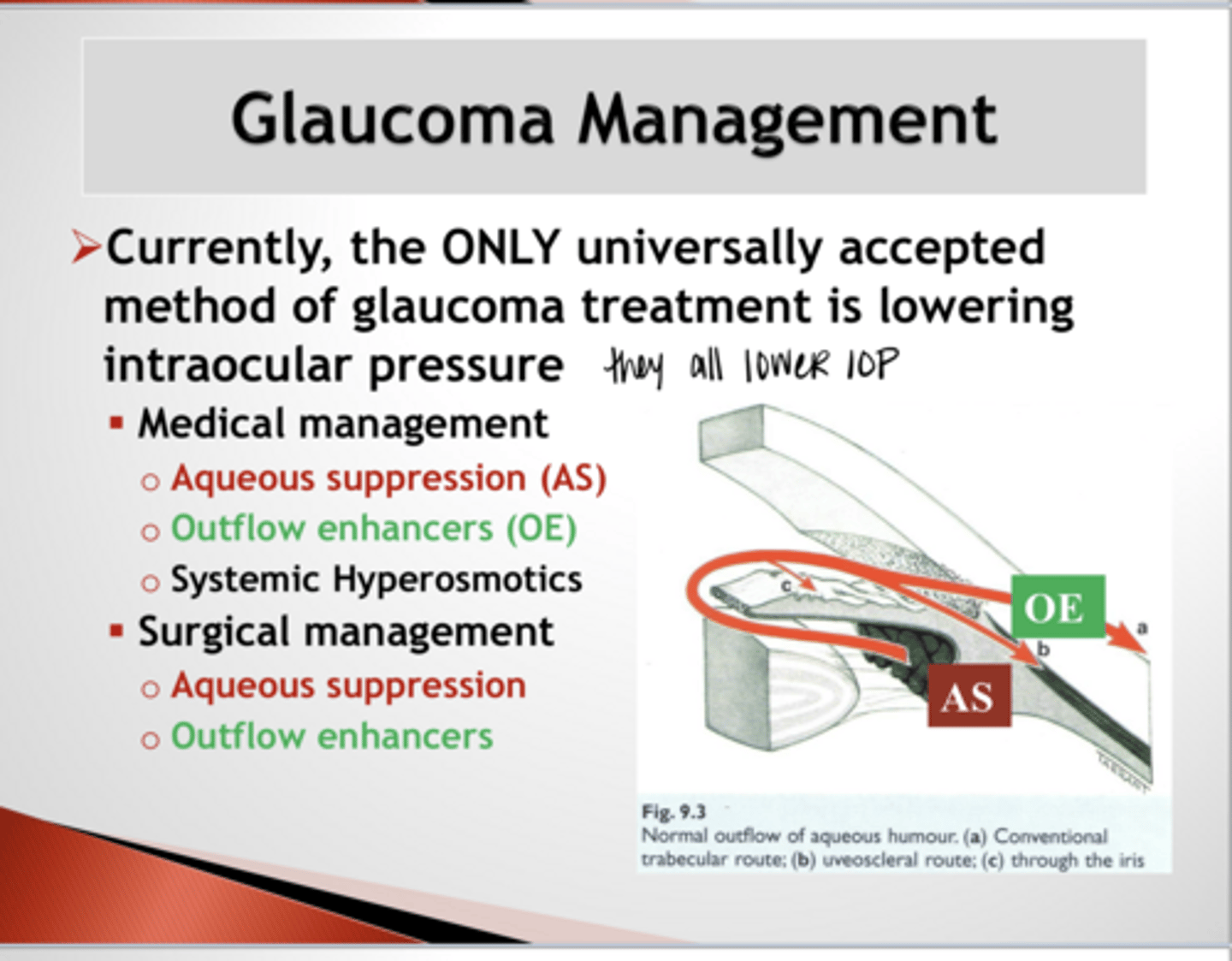
What are the surgical management options of glaucoma management?
Aqueous suppression (AS)
Outflow enhancers (OE)
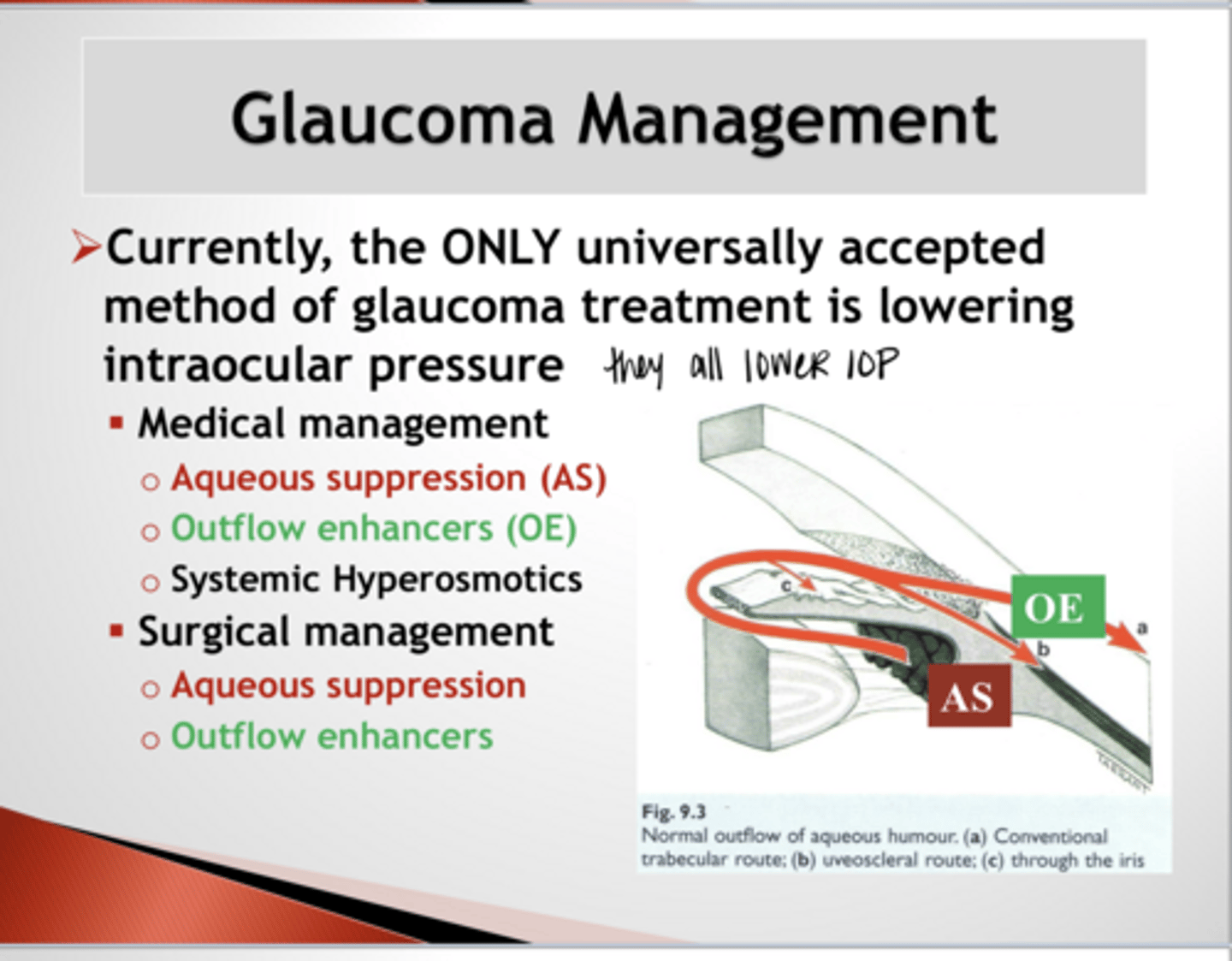
What is the mechanism of aqueous suppression (AS)?
lowers intraocular pressure (IOP) by reducing the production of aqueous humor in the ciliary body
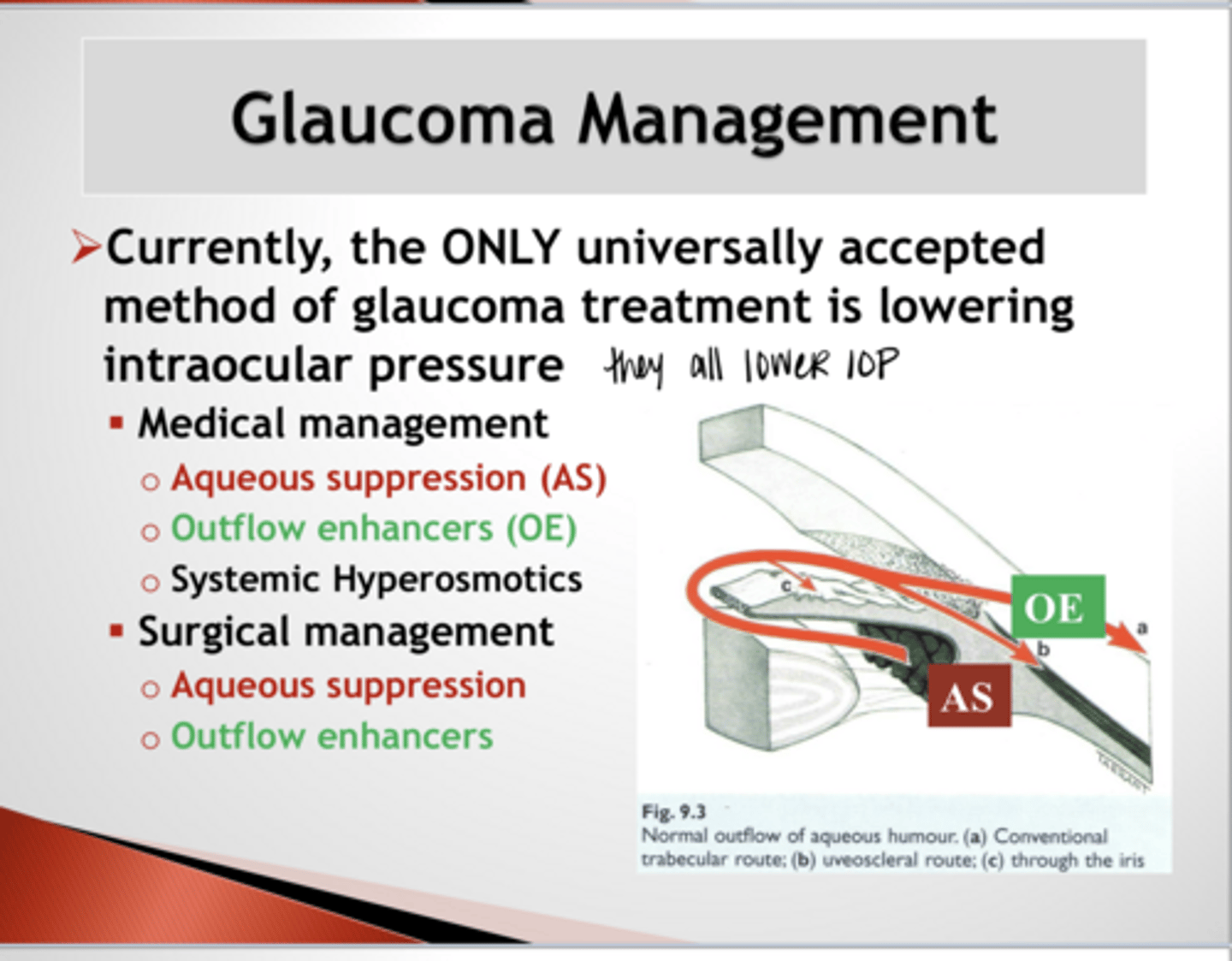
What is the mechanism of aqueous outflow enhancement?
educing resistance in the eye's conventional drainage system (trabecular meshwork and Schlemm's canal) or by increasing flow through the unconventional (uveoscleral) pathway
What are the goals for IOP reduction?
1) Obtain an adequate % decrease in mmHg from the highest measured IOP (Tmax)
2) Maintain a consistent and regular level of acceptable IOP with minimal fluctuations in diurnal IOP
It is critical to document what during the management of glaucoma?
The highest UNTREATED IOP prior to commencing treatment to properly determine a target IOP
What is a critical factor in maintaining consistent IOP control from a topical medication?
Patient compliance
What are 5 factors that contribute to impairment of treatment adherance?
1) Lack of understanding of why they need treatment in the 1st place
2) Medication side effects
3) Cost/lack of access to medications
4) Difficulty with drop instillation/dexterity issues
5) Number of drops/day and bottle confusion if multiple bottles are needed
True or False:
There is a clinically significant drop in adherence to therapy when the prescribing regimen is more than 2 doses per day
true
The addition of a second bottle to glaucoma treatment (increases/decreases) the adherence to the first medication (including refilling of the 1st medication)
decreases
Elements of Proper Glaucoma Medication Selection
Efficacy
Simplified dosing patterns
No/minimal side effects
What makes a glaucoma medication efficacious?
Significant % in IOP decrease
Long duration of action
Effective at maintaining a relatively flat diurnal curve, esp during noctural hours
What makes a "simplified dosing pattern" for glaucoma medications?
Least number of bottles
Least number of drops per day
What is currently the EASIEST DOSING REGIMEN for topical glaucoma medication?
one drug (monotherapy) given once daily
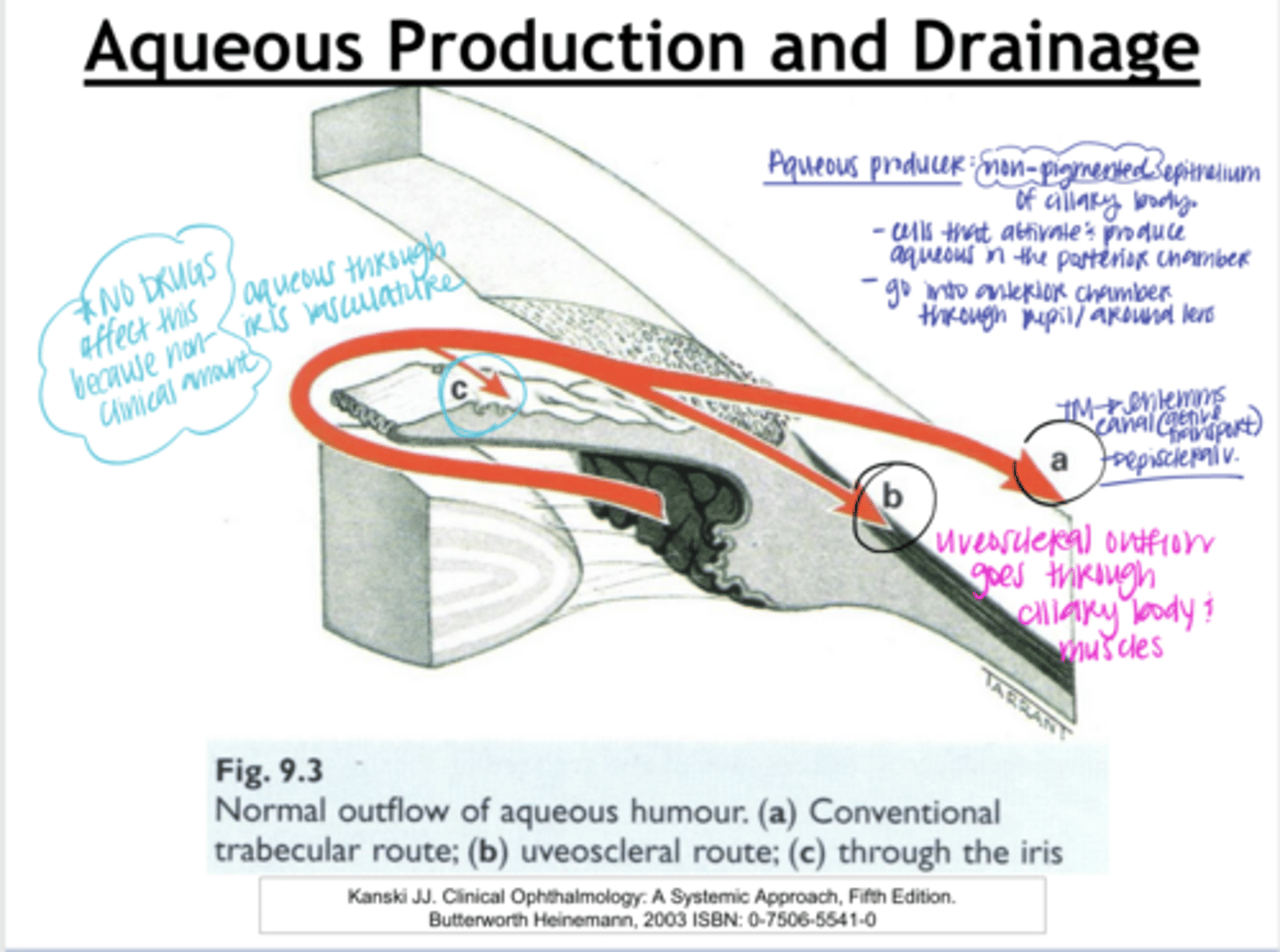
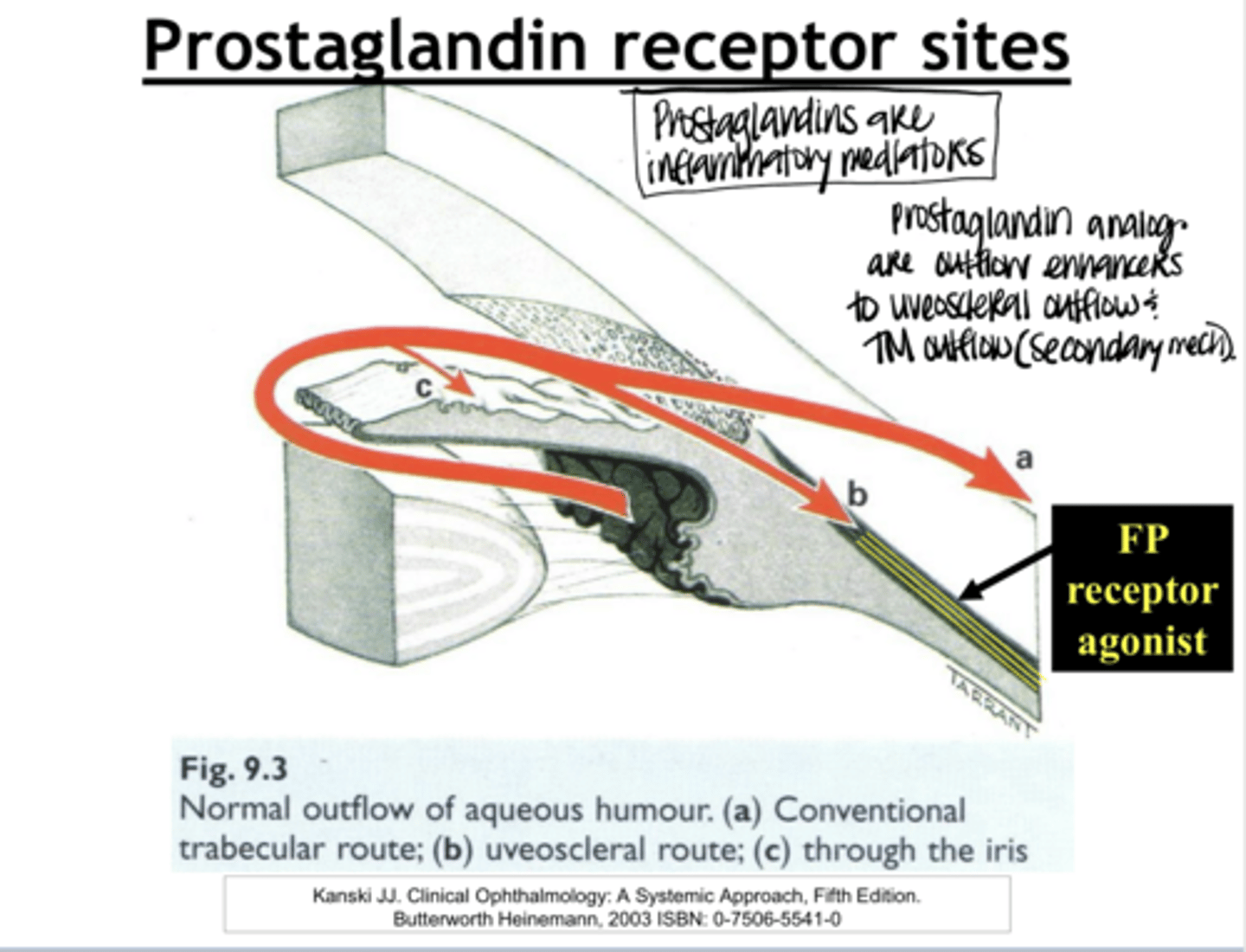
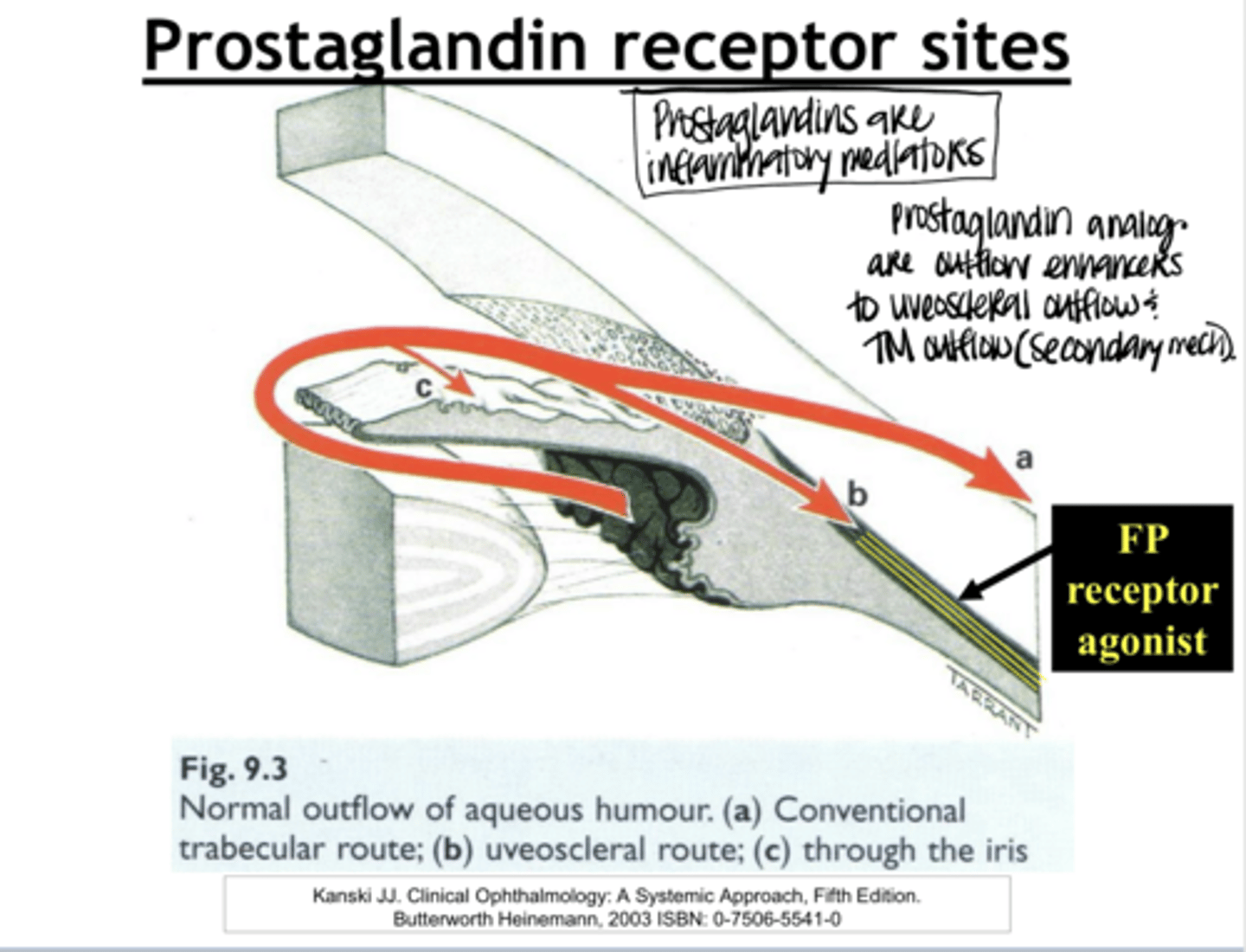
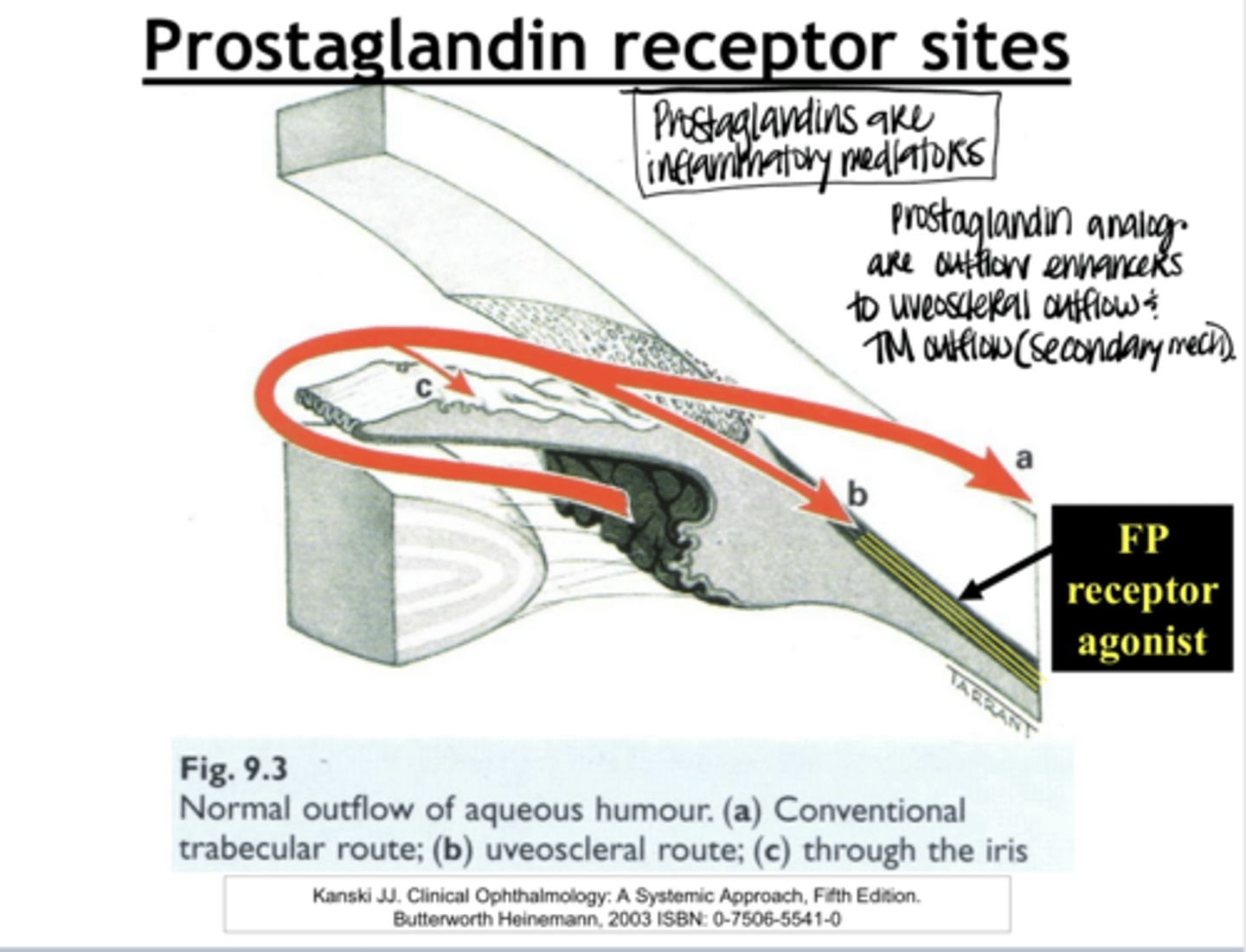
Conventional aqueous outflow method
drives aqueous humor from the anterior chamber through the trabecular meshwork and Schlemm's canal, then into collector channels and the episcleral vein
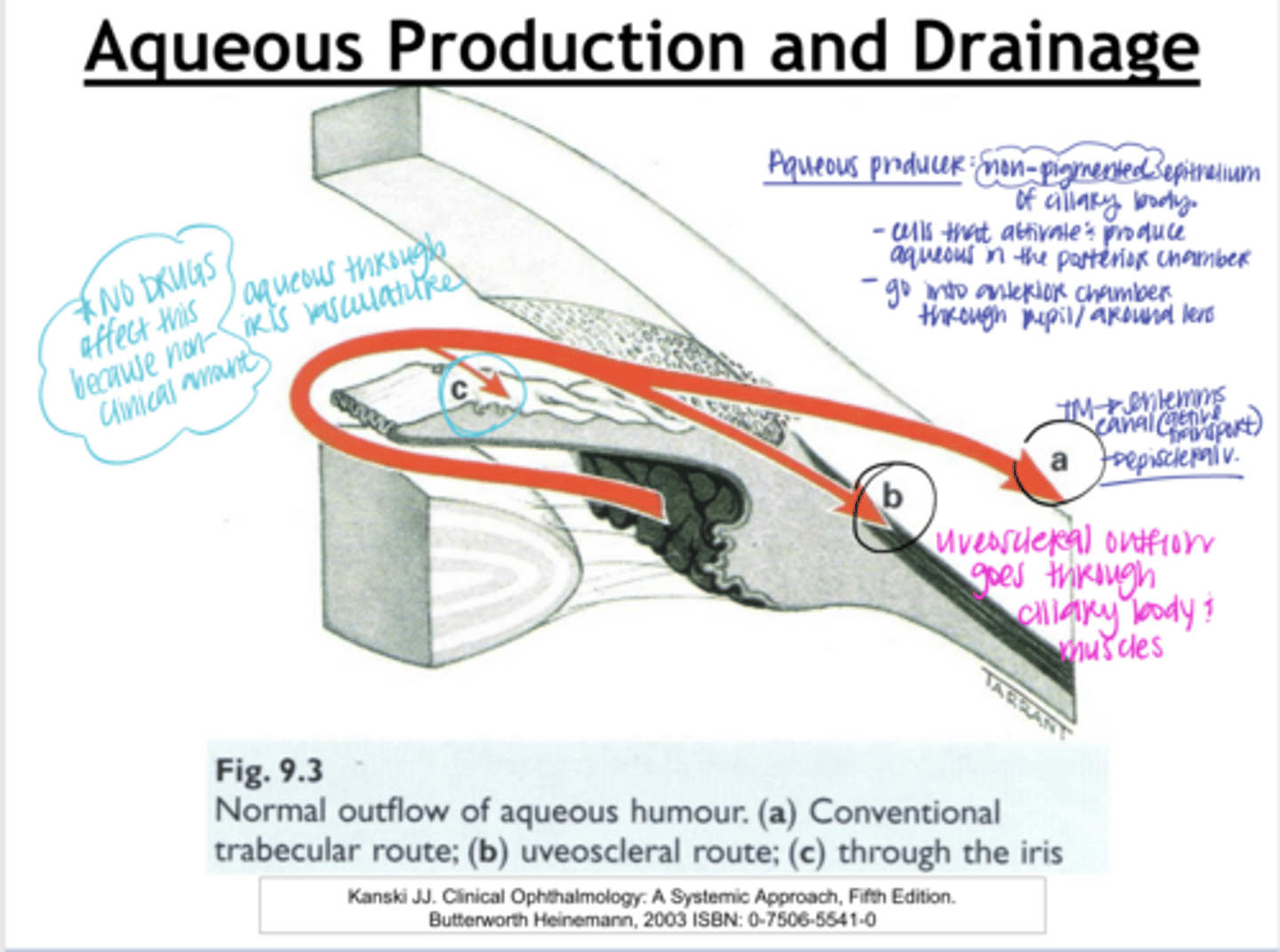
Uveosceral aqueous outflow method
the secondary, non-mechanical drainage pathway of aqueous humor from the eye's anterior chamber, responsible for removing roughly 10%-20% of fluid in humans. It moves fluid through the ciliary muscle and suprachoroidal space rather than the trabecular meshwork, with its flow primarily regulated by resistance in the ciliary body
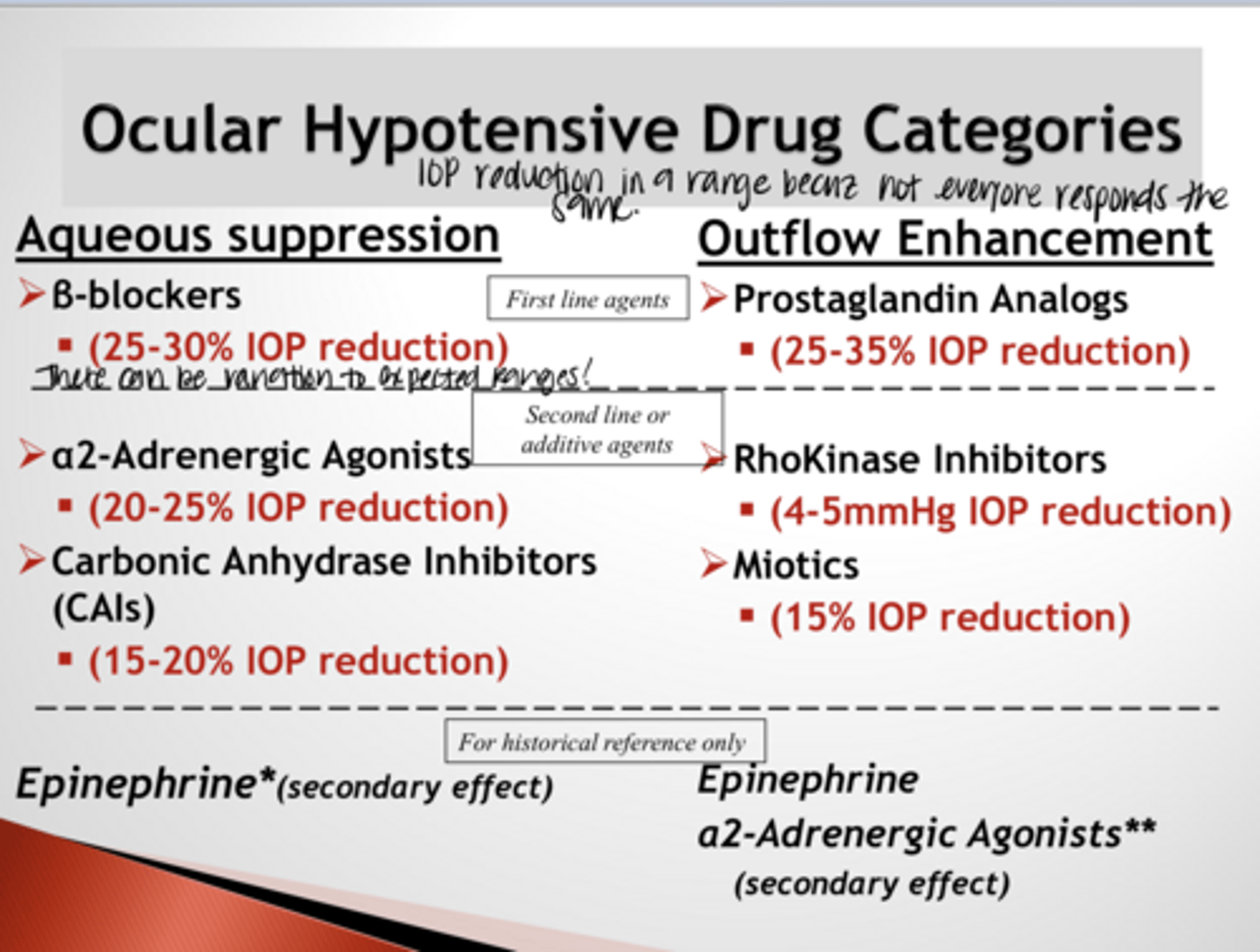
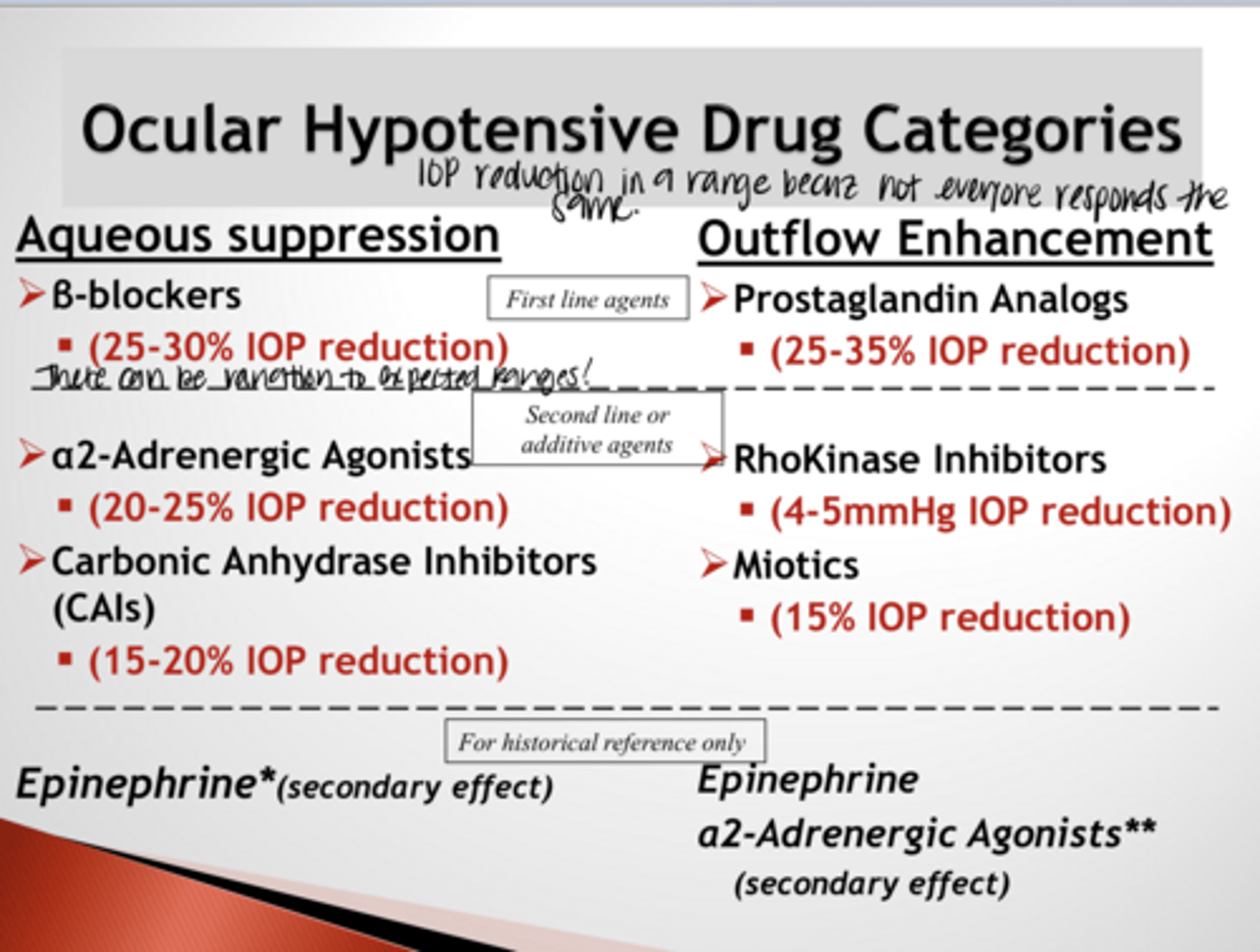
What are the aqueous suppressing ocular hypotensive drugs?
B blockers
a2 adrenergic agonists
Carbonic anhydrase inhibitors (CAIs)
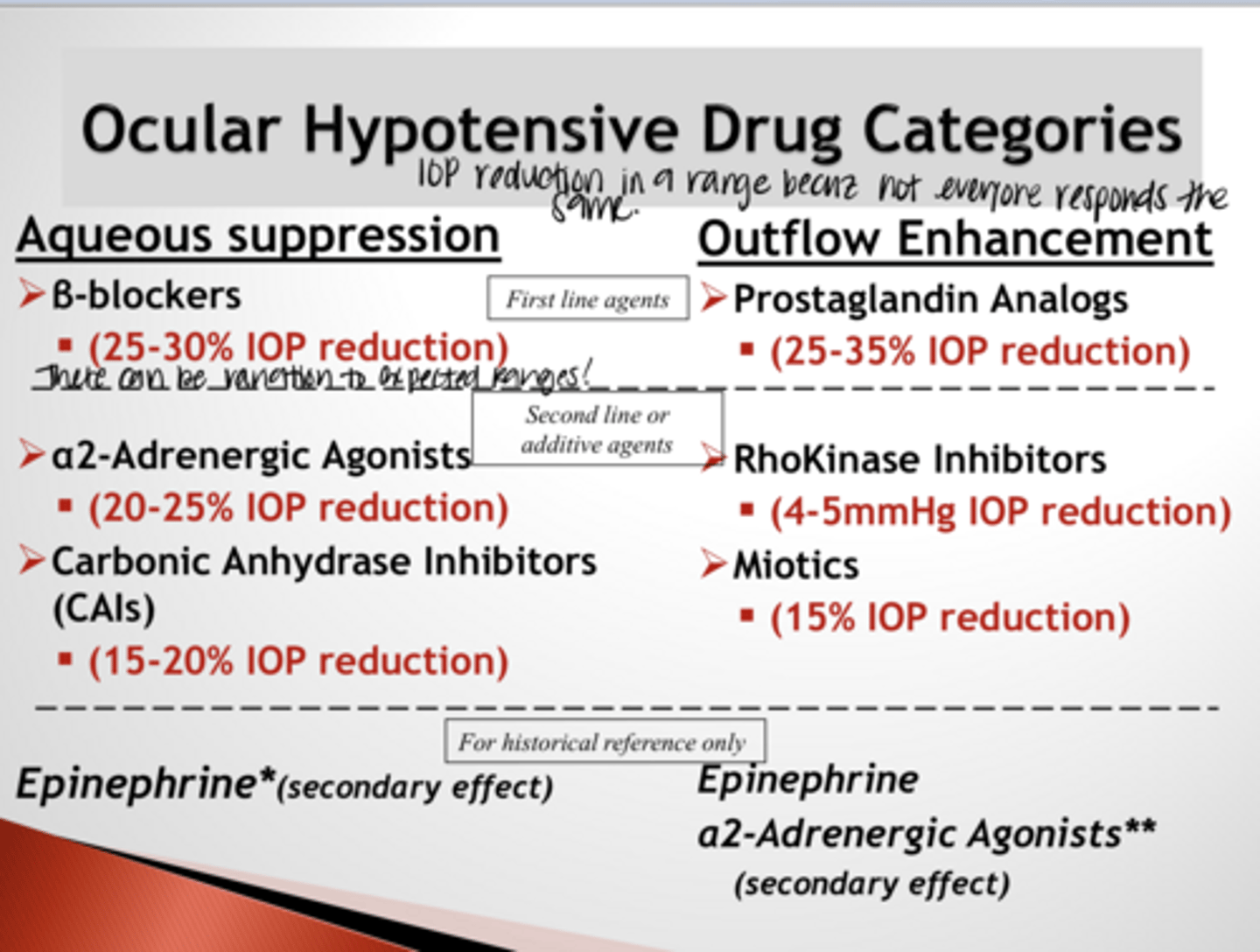
What are the outflow enhancing ocular hypotensive drugs?
Prostaglandin analogs
Rhokinase inhibitors
Miotics
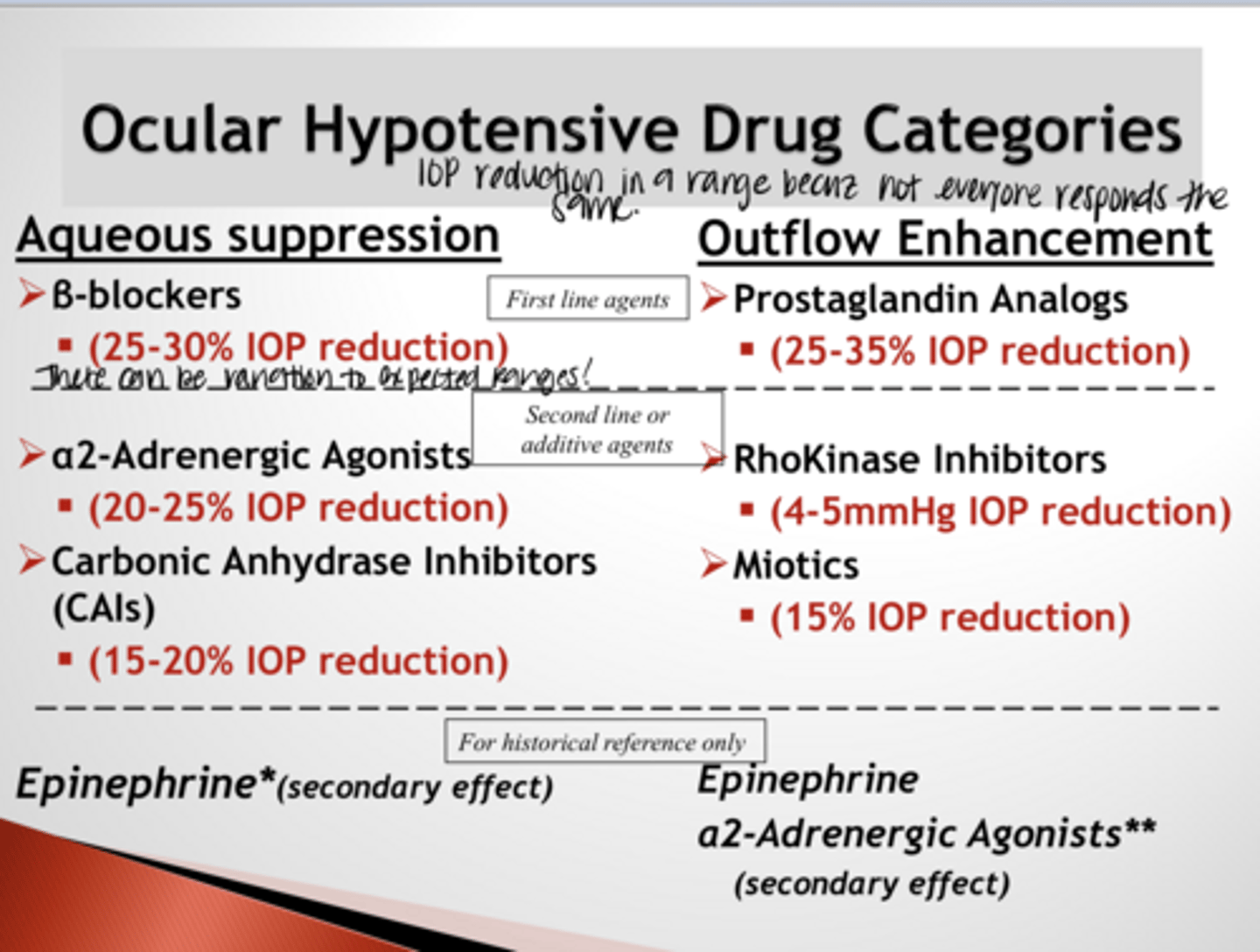
What is the FIRST LINE AQUEOUS SUPPRESSION ocular hypotensive drug?
b blocker
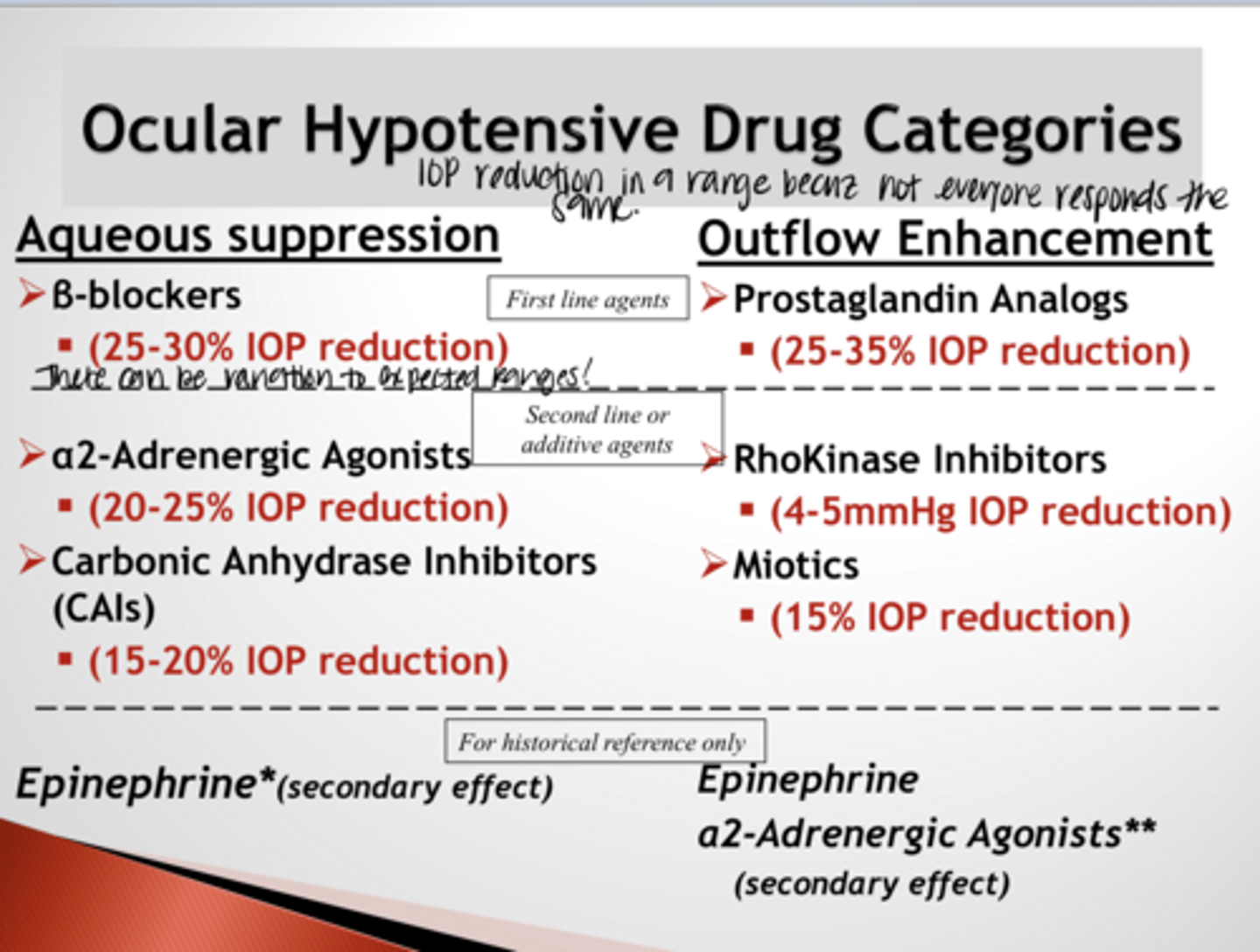
What is the FIRST LINE OUTFLOW ENHANCEMENT ocular hypotensive drug?
prostaglandin analog
What are the 2 situations in which a second line ocular hypotensive drug is used?
1) If all first line drugs are unavailable or ineffective
2) Additive to a first line drug becuz glaucoma is severe
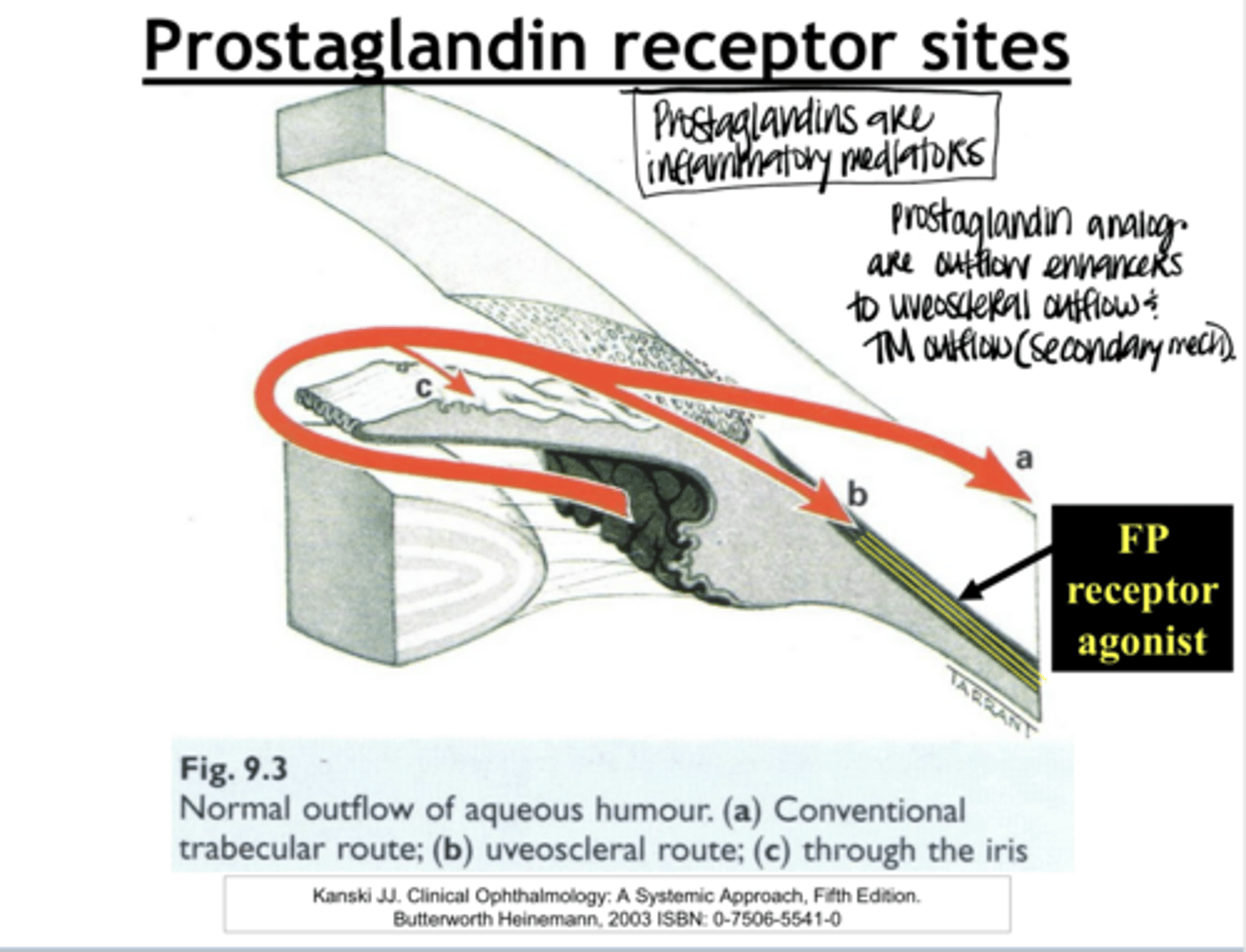
What is the main mechanism of action of the prostaglandins?
Bind to FP receptors on the ciliary muscle that result in a remodeling of collagen in the extracellular matrix surround ciliary muscle fibers resulting in widening space between the longitudinal fibers decreasing resistance to uveoscleral outflow
How many subtype prostaglandin receptors are there?
5
Where do FP receptors exist in the eye?
On the longitudinal ciliary muscles
How do prostaglandins react w/ FP receptors?
They are agonists
What is the effect of prostaglandins binding the FP receptors in the ciliary body?
Bind to FP receptors & cause a remodeling of the collagen in the ciliary muscles that increases the space between the longitudinal fibers & draws aqueous through the uveoscleral pathway
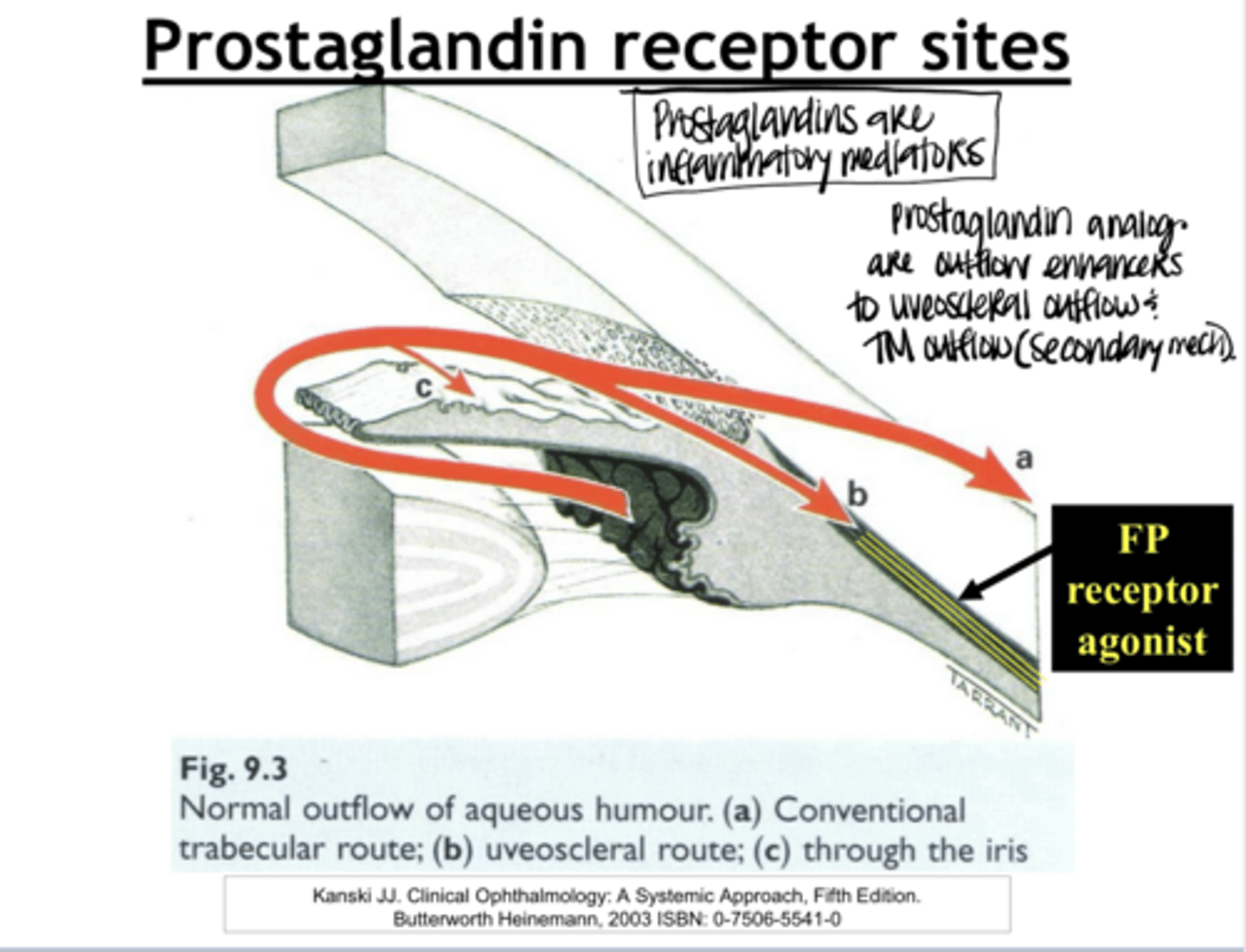
Prostaglandins work predominantly through the _____ pathway
uveoscleral
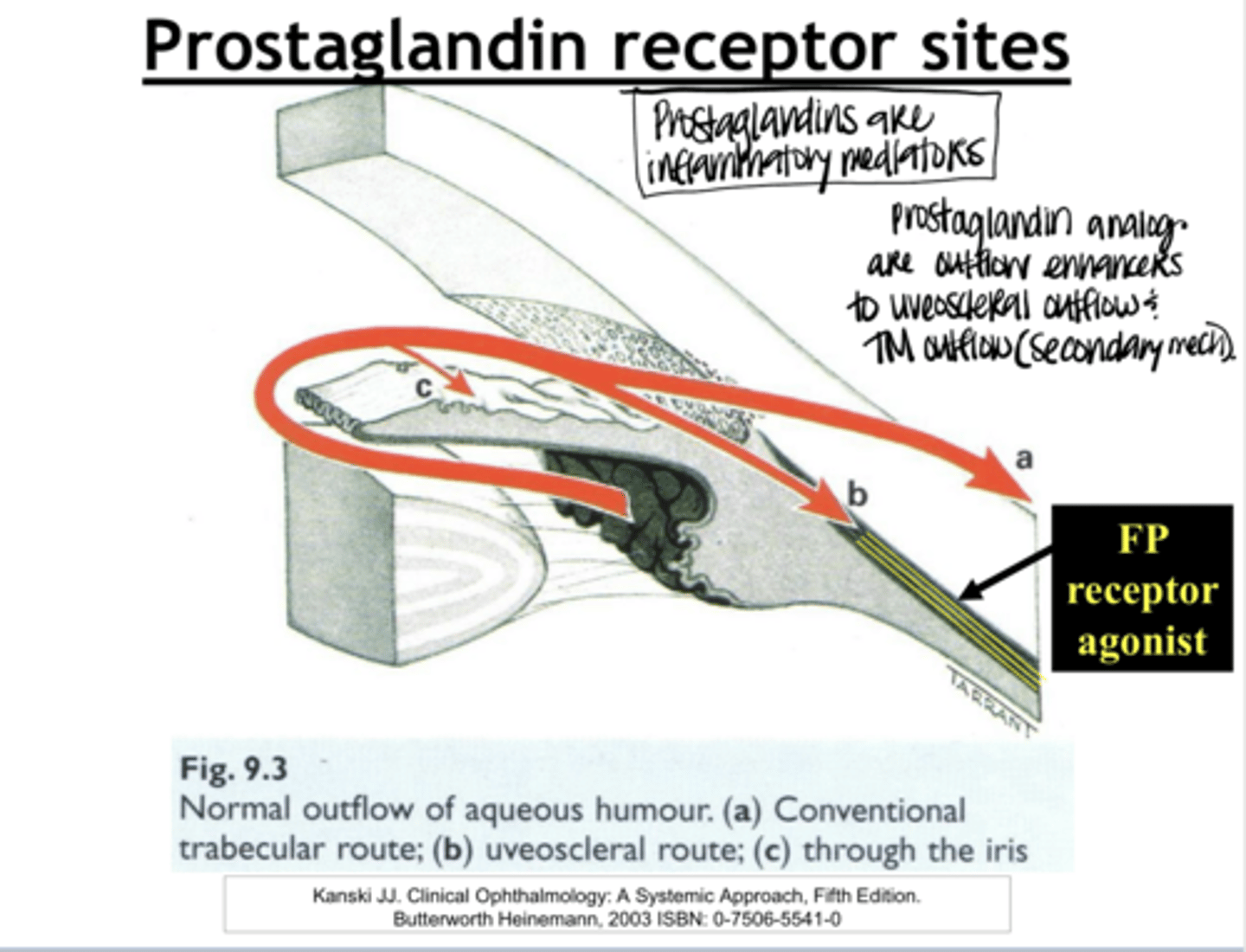
What is the secondary mechanism of prostaglandin use?
enhance TM outflow through the release of inflammatory cytokines within the TM which activate endotheial cells & enhance active transport into Schlemm canal
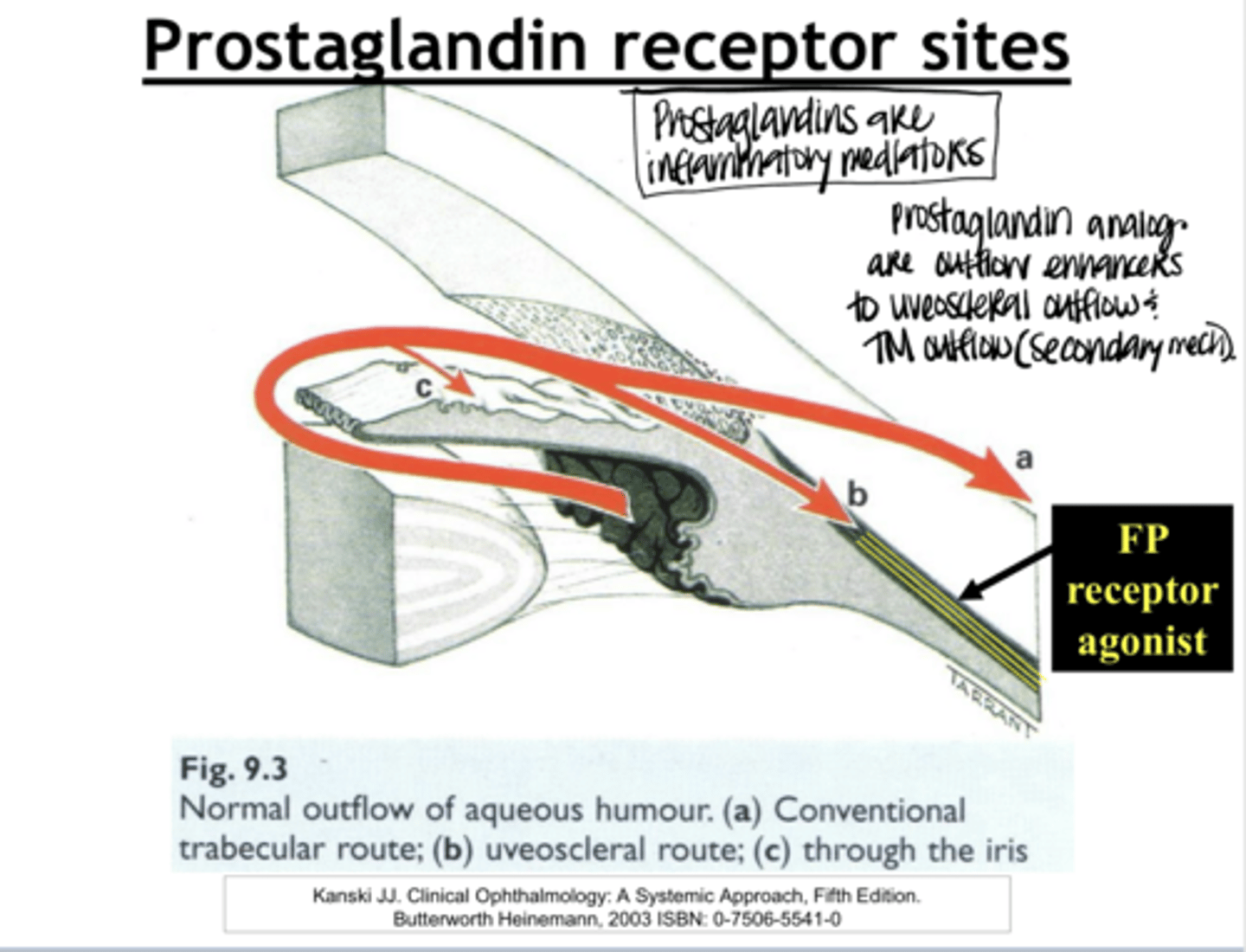
Are prostaglandins inflammatory mediators? Do they invoke inflammation?
Yes -- yes they invoke SMALL amounts of inflammation
What is the theory of how SLT Laser treatments work? (this is related to the secondary mechanism of prostaglandins?
Create inflammation in the TM to enhance active transport into Schlemm canal
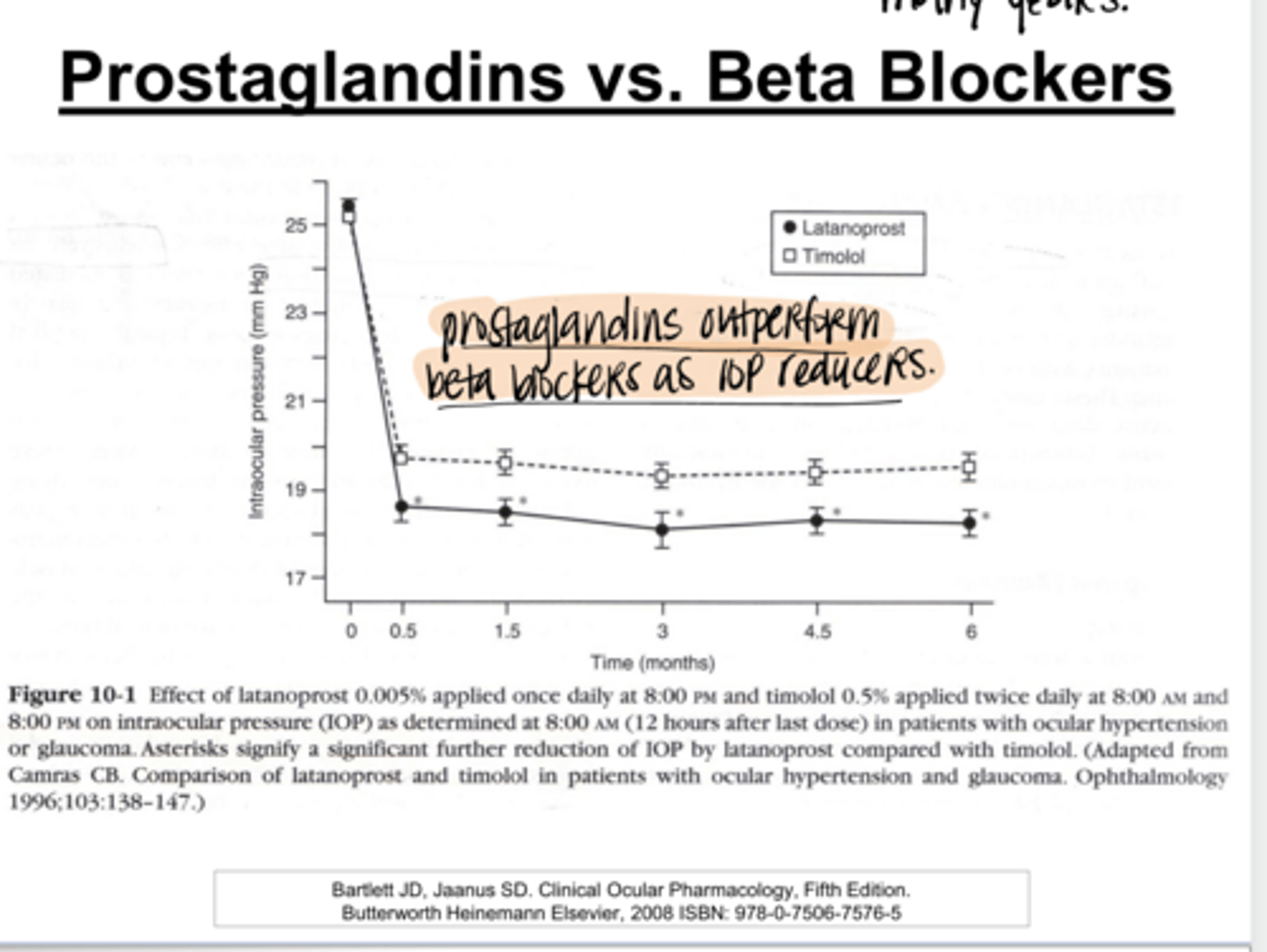
Which is better for consistent IOP reduction?
Prostaglandins or Beta Blockers
Prostaglandins
Prostaglandins decrease IOP by _____%
25-35
Non-responders to prostaglandins are as low as ____%
4
Prostaglandins have a greater effect in which form of glaucoma?
pigmentary glaucoma
Why do prostglandins have a greater effect in pigmentary glaucoma?
Prostaglandin target tissue is ciliary body and TM. Pigment is this form of glaucoma is INTO THE ANGLE AND CB. Pigment attracts more medicine INTO THE TARGET TISSUE. Greater amount of pigment will enhance the effect of the prostaglandin.
What is the peak onset of action time of the prostaglandins?
8 afters after instillation
What is the duration of action of prostaglandins?
24 hours
What is the dosing of prostglandins?
QD -- 24 hour duration of action
Is there any tachyphylaxis or long term drift associated with prostaglandins?
No
What are the ocular side effects of the prostaglandins?
1) Conj hyperemia
2) Increase pigmentation of growth of lashes
3) Periorbital skin tissue pigmentation
4) Iris pigmentation changes are permanent
5) Prostaglandin-Associated Periorbitopathy (Sunkun Sulcus Syndrome)
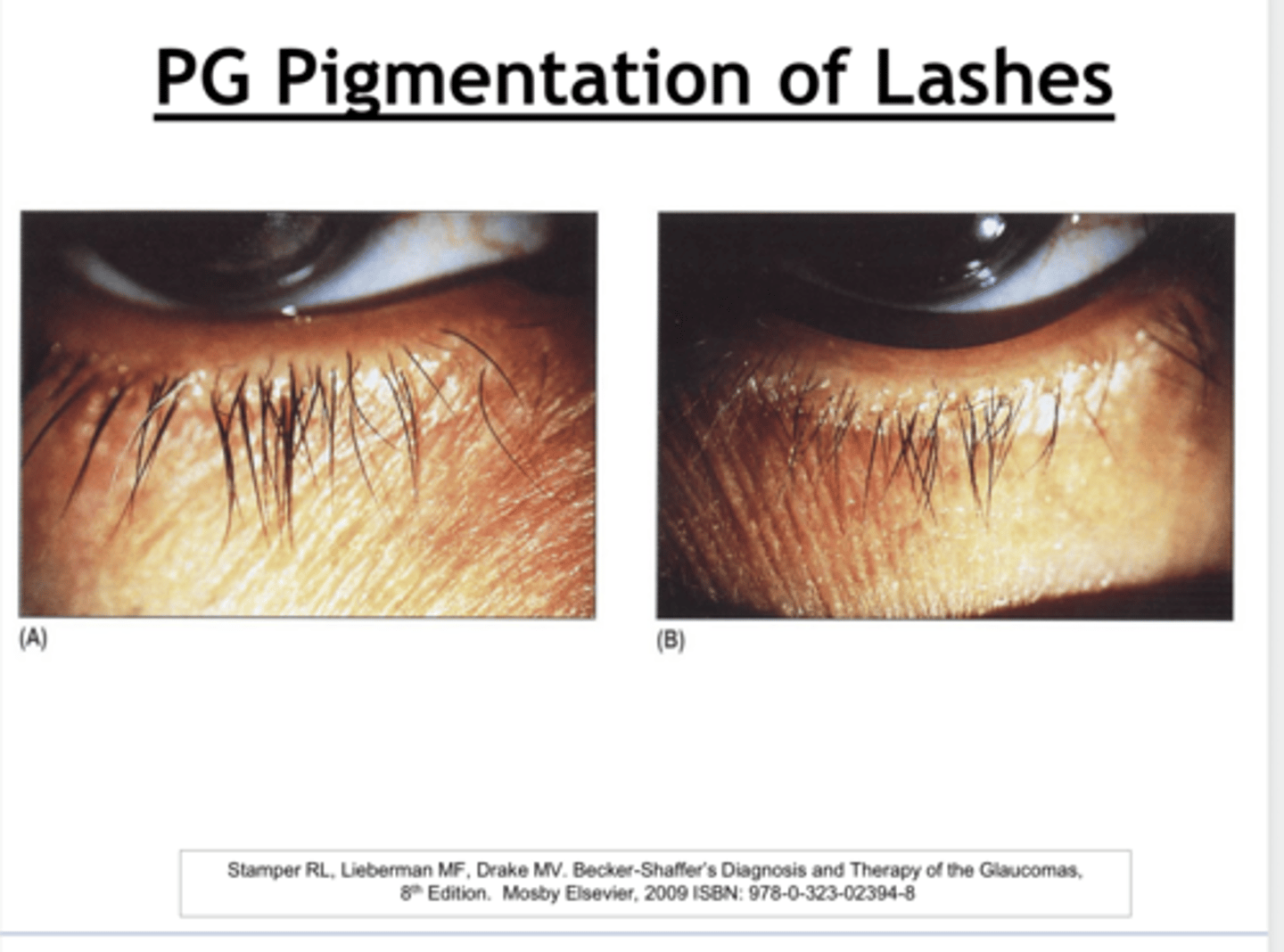
Prostaglandin Pigmentation of Lashes (Pic)
**lashes are thicker, darker and longer
Prostaglandin Pigmentation of Lashes (Pic)
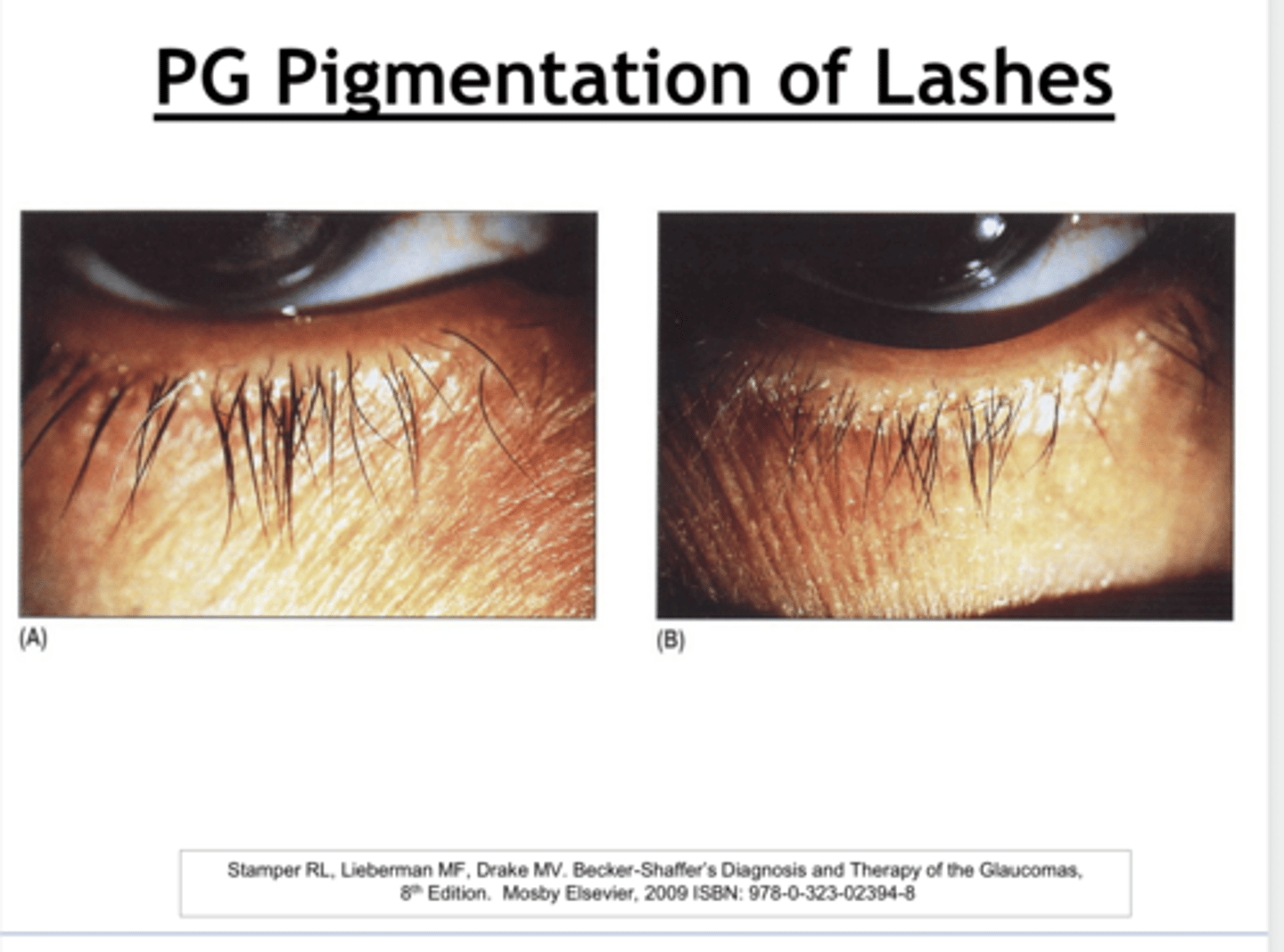
Is the pigmentation and growth of the eyelashes with prostaglandin use permanent or temporary?
Temporary -- lashes have a short life span
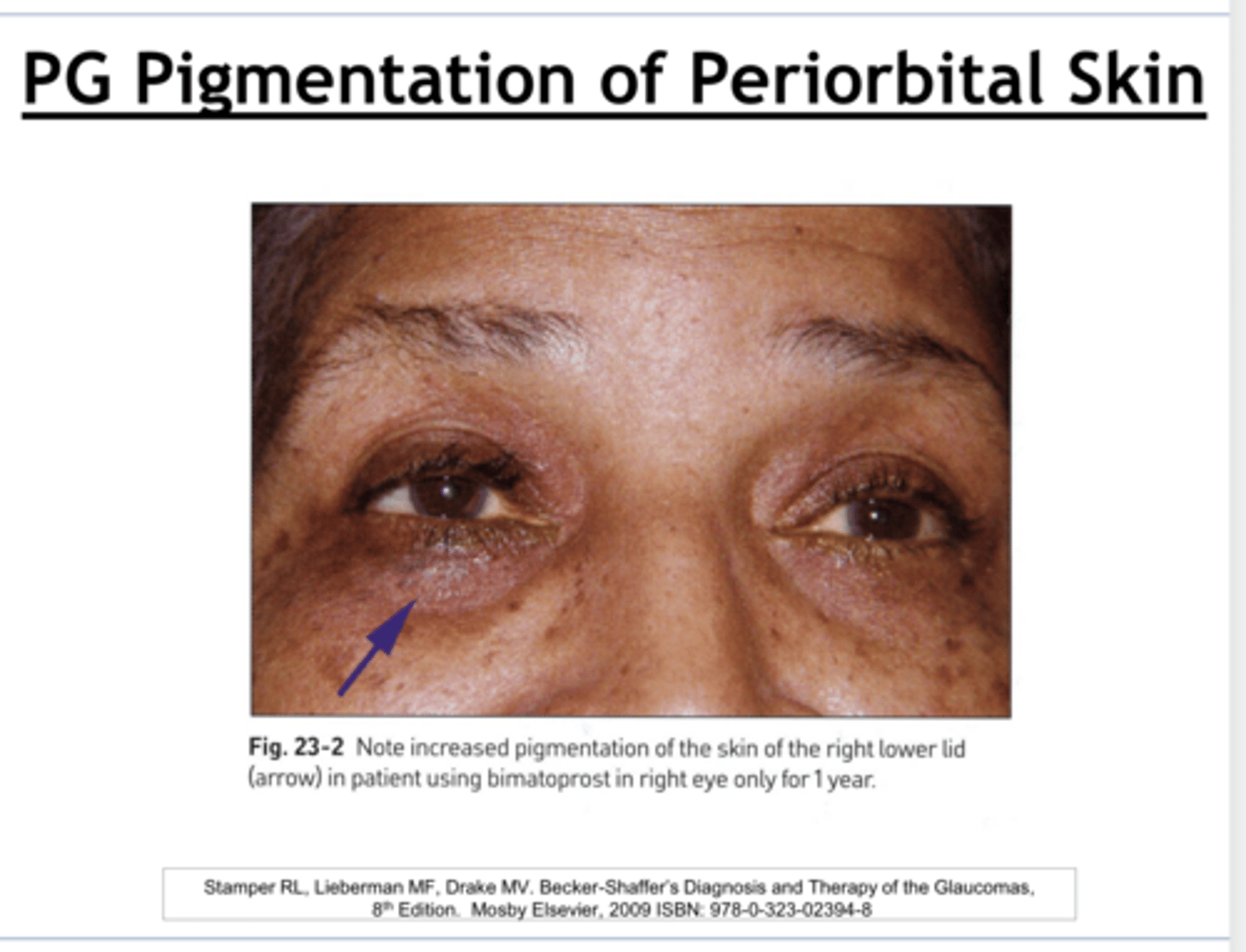
Prostaglandin Pigmentation of Periorbital Skin (Pic)
Prostaglandin Pigmentation of Periorbital Skin (Pic)
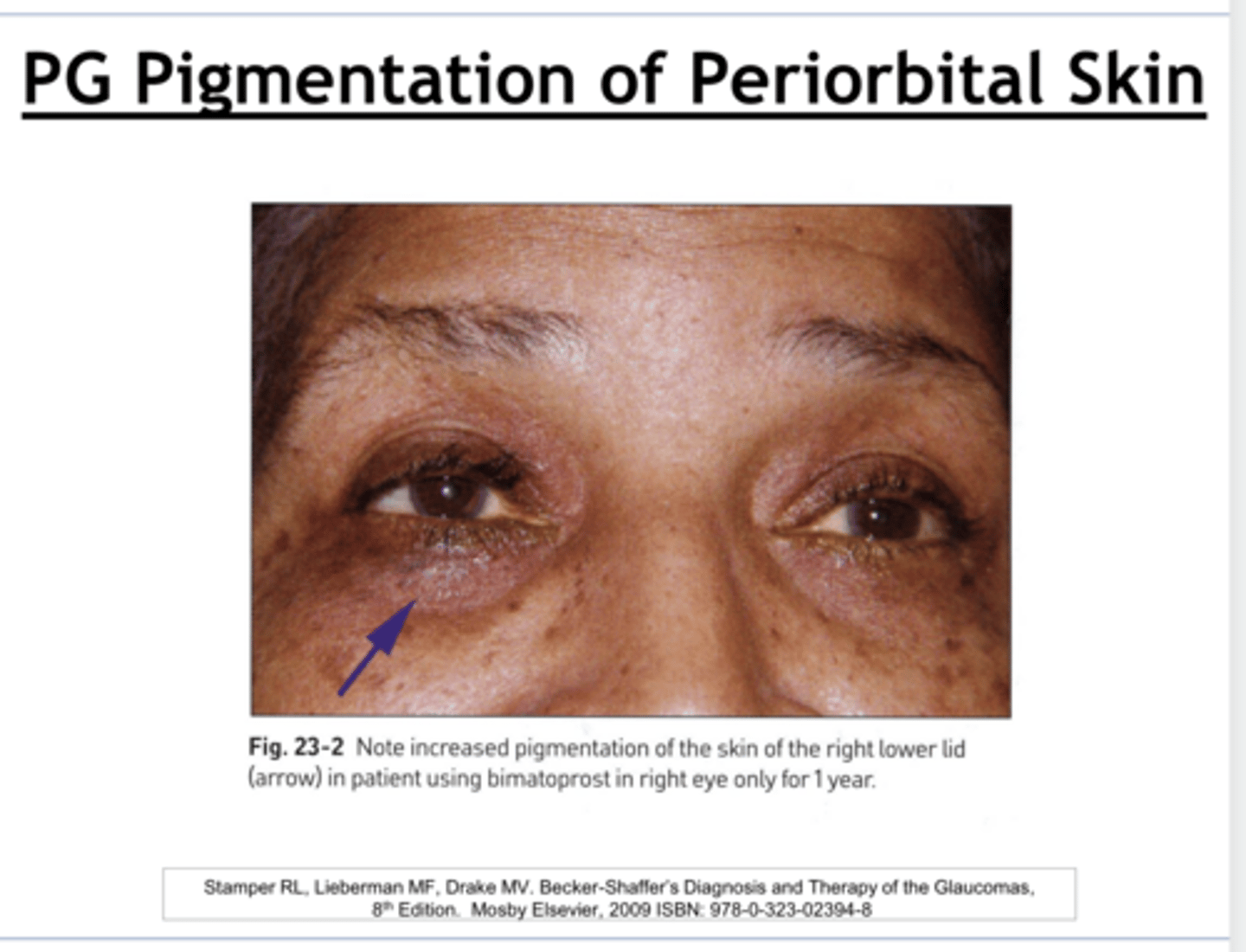
Is the pigmentation of periorbital skin w/ prostaglandin use permanent or temporary?
temporary -- pigment is in the epithelium of the skin
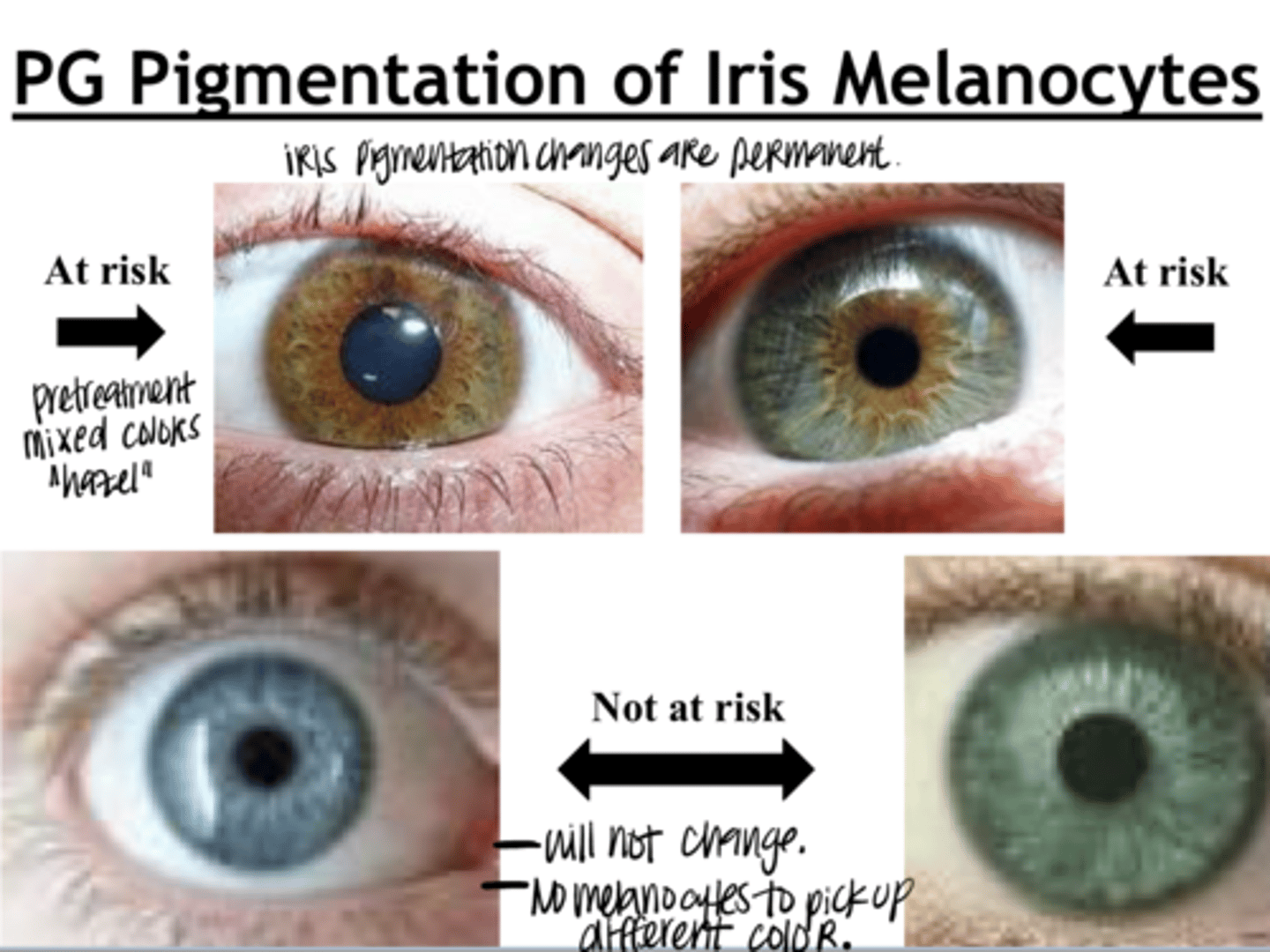
Prostaglandin Pigmentation of Iris Melanocytes (Pic)
Prostaglandin Pigmentation of Iris Melanocytes (Pic)
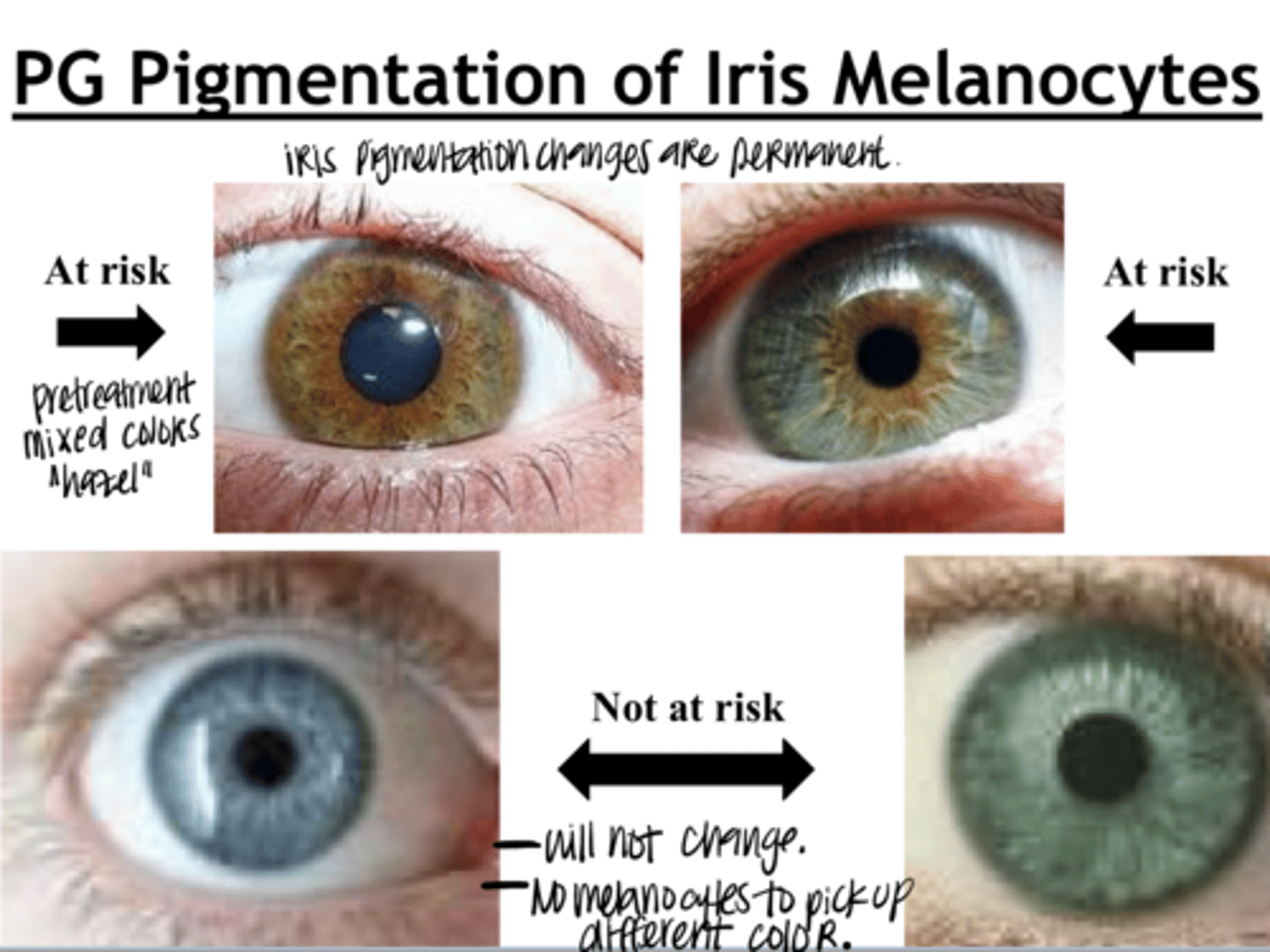
Is the changing pigmentation of iris w/ prostaglandin use permanent or temporary?
permanent
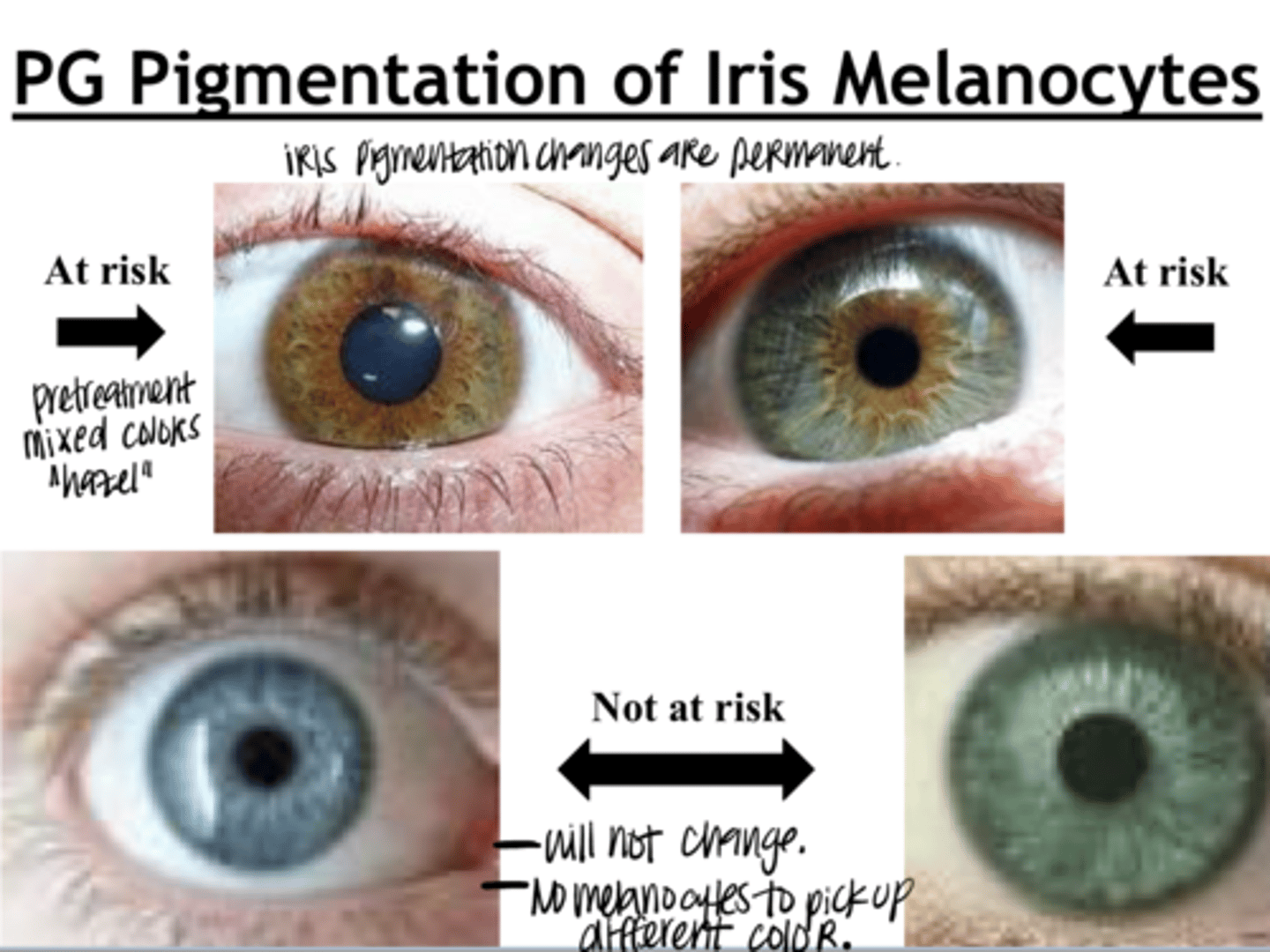
What colored eyes are at risk for iris pigmentation changes w/ prostaglandin use?
Hazel -- mixed color eyes
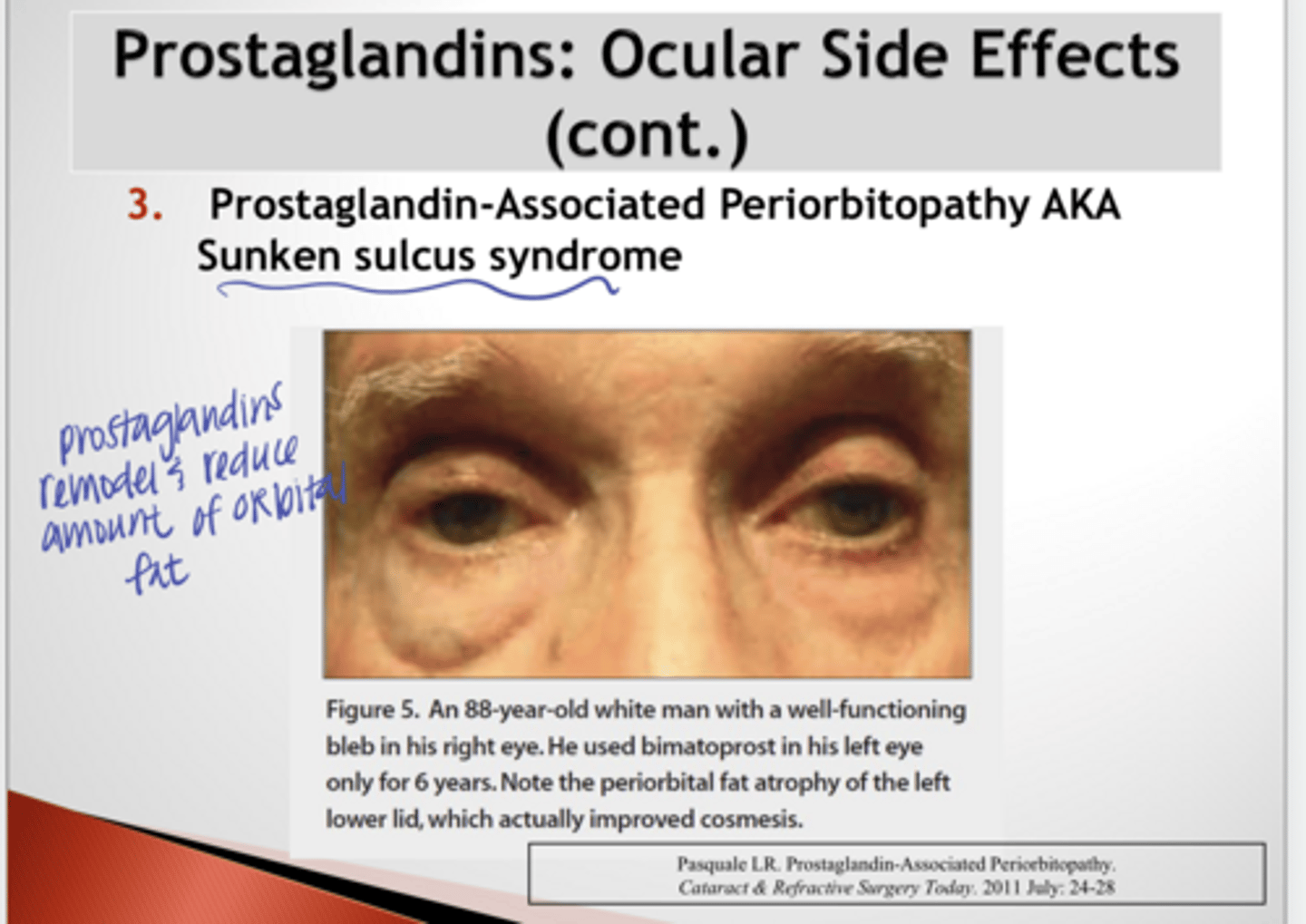
What are the characteristics of Prostaglandin-Associated Periorbitopathy (Sunkun Sulcus Syndrome) secondary to prostaglandin use?
deep upper eyelid sulcus, fat atrophy, ptosis, and eyelid tightening d/t remodeling of the periorbital tissue by the prostaglandins
What are the "potential" ocular side effects of prostaglandin use d/t their inflammatory mediator capability?
Uveitis
CME
Pseudodendrites
Recurrence of Simplex Keratitis ??
What is an absolute contraindication of prostaglandin use?
Uveitic glaucoma
What are the relative contraindications of prostaglandin use?
History of simplex keratitis
Aphakia/pseudophakia d/t risk of CME
Concurrent use with miotics
NOT FOR ANGLE CLOSURE GLAUCOMA or other "rescue" use
Angle recession
Mixed color irides
Unilateral treatment
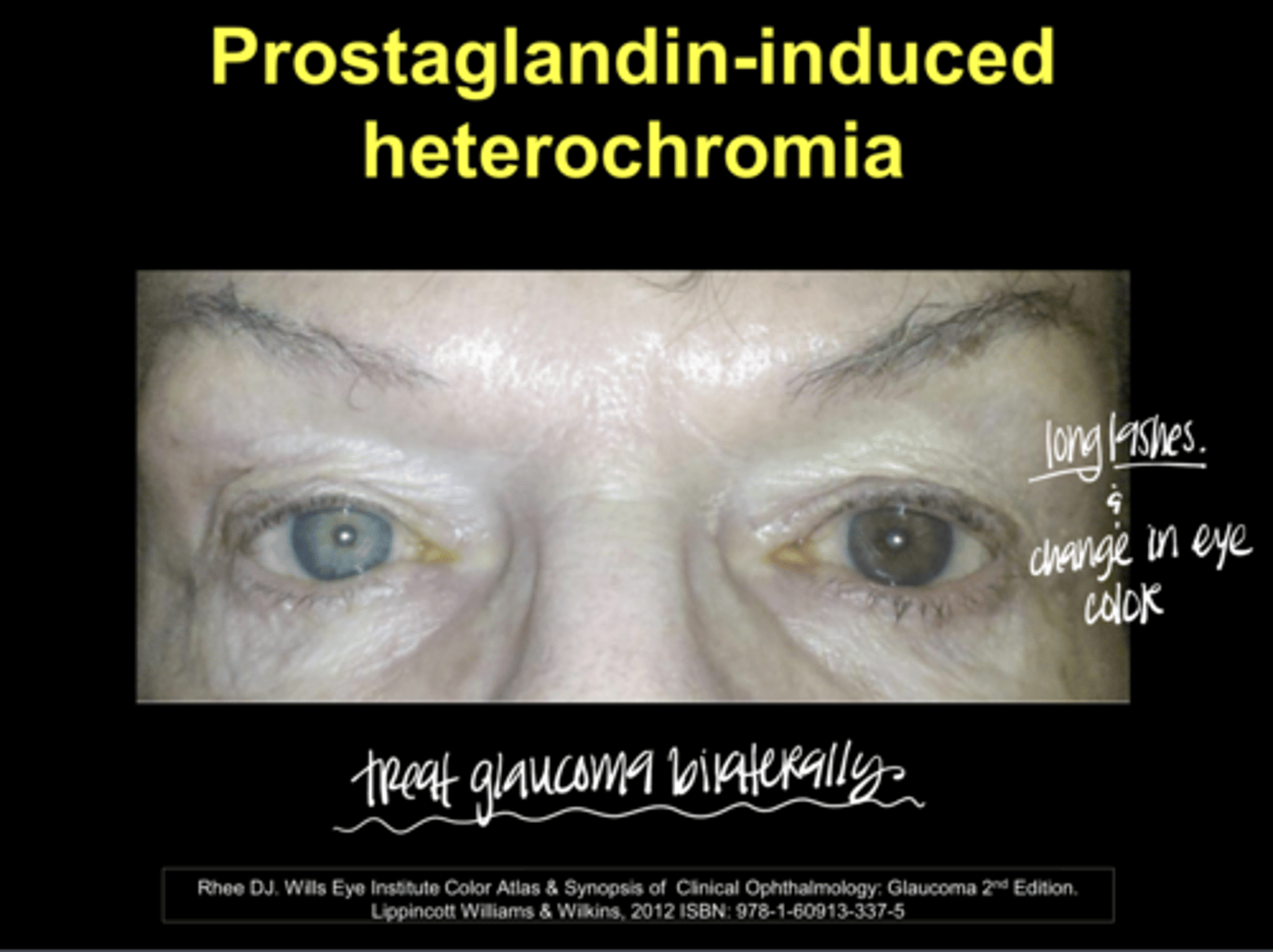
Prostaglandin-Induced Heterochromia (Pic)
**why you treat glaucoma with prostaglandins bilaterally
Prostaglandin-Induced Heterochromia (Pic)
There are RARE associations of prostaglandins with what systemic side effect?
gastric distress
Prostaglandins are the first line drug in treating what conditions?
Ocular hypertension
Primary open angle glaucoma (POAG)
Pigmentary glaucoma
Pseudoexfoliation glaucoma (PXE)
Normal tension glaucoma (NTG)
What is the dosing of prostaglandins?
1 gtt QHS
Why would you want to dose a prostaglandin at nighttime?
Redness side effect will be most prevalent (peaking) while the patient is asleep
24 hour duration of action
Do you HAVE to take a prostaglandin at night for it to be effective? Do you need to consider this on a patient by patient basis?
If a patient cannot maintain consistency with bedtime dosing, it is OK for them to do it at whatever time keeps them taking the drug regularly.
What are the prostaglandin agents that are discussed in this module?
Xalatan (0.005% latanoprost)
Iyuzeh (0.005% latanoprost)
Travatan Z (0.004% travoprost)
Lumigan (0.01% bimatanoprost)
Zioptan (0.0015% tafluprost)
Vyzulta (0.024% latanoprostene bunod)
Omlonti (0.002% omidenepag isopropyl)
Latisse (0.03% bimatanoprost)
What is the generic formulation of Xalatan?
0.005% latanoprost
Why is Xalatan (0.005% latanoprost) special?
first in its class to receive approval as 1st line therapy glaucoma medication
Xalatan (0.005% latanoprost) is a ________
prodrug
Is Xalatan (0.005% latanoprost) preserved? With what?
yes -- with BAK
Xalatan (0.005% latanoprost) is the (most/least) likely to induce redness
least
Is Xalatan (0.005% latanoprost) available generically?
Yes
What is the generic formulation of Iyuzeh?
0.005% latanoprost
Is Iyuzeh (0.005% latanoprost) packed with preservatives?
No -- PF w/ single use vials
Are Xalatan and Iyuzeh the same medication?
Yes 0.005% latanoprost -- only difference is that Iyuzeh does not have preservatives
What is the generic formulation of Travatan?
0.004% latanoprost
Does Travatan (0.004% Travoprost) contain BAK?
No -- but has a preservative SofZia
Is Travatan (0.004% latnoprost) available generically? What is the problem with the generic formulation?
Yes -- the generic is preserved with BAK
What is special about Travatan (0.004% Travoprost)?
Longest duration of action of any prostaglandin
What is beneficial about the dosing of Travatan (0.004% Travoprost)?
Pt is still OK for a few hours with a missed dose
What is the generic formulation of Lumigan?
0.01% bimatanoprost
Lumigan is a ________, possibly providing greater efficacy
prostamide
True or False:
Lumigan has the BEST IOP DECREASE CAPABILITY in the prostaglandin class
true -- can reduce IOP by 1-2mmHg more than other prostaglandins
Is Lumigan preserved with BAK?
Yes
True or False:
Is a 2.5mL bottle of prostaglandin drop a full 1 month (31 day) supply?
True -- specifically titrated for a month supply
What was significant about the original 0.03% Lumigan with 0.005% BAK?
Highest redness risk of all prostaglandins. 30% of patients experienced this.
Current 0.01% Lumigan with only 0.02% BAK has (more/less) redness compared to the original 0.03% formulation
less
Which is more efficacious?
Previous 0.03% Lumigan or 0.01% Lumigan
Equal efficacy
What is a potential glaucoma delivery device?
MediPrint Ophthalmics has completed a Phase 2b study of a weekly drug-eluting CL for glaucoma containing 0.01% bimatanoprost. Initial results show a 30% reduction in IOP with good tolerability/comfort ratings
What is the generic formulation of Zioptan?
0.0015% tafluprost
Is Zioptan (0.0015% tafluprost) preserved?
No -- single use vials
What is the generic formulation of Vyzulta?
0.024% latanoprostene bunod
What is special about Vyzulta (0.024% latanoprostene bunod)?
a nitric oxide donating prostaglandin
What is the dual MOA of Vyzulta (0.024% latanoprostene bunod)?
Once absorbed into the eye, it is metabolized into latanoprost acid and butanediol mononitrate which further metabolizes into nitric oxide (NO). Nitric oxide opens up the TM to provide an enhanced IOP reduction
What is the efficacy of Vyzulta (0.024% latanoprostene bunod)?
-30-35% reduction in IOP
-Vyzulta will reduce IOP by 1.23mmHg more than latanoprost in Voyager Study
-Vyzulta showed effectiveness in Normotension Glaucoma patients in Jupiter Study
Does Vyzulta (0.024% latanoprostene bunod) have the same side effects as other prostaglandins in this class?
Yes
What is the dosage of Vyzulta (0.024% latanoprostene bunod)?
1 gtt QHS
What is the generic formulation of Omlonti?
0.002% omidenepag isopropyl solution
How is Omlonti (0.002% omidenepag isopropyl solution) labelled?
non-PG F analog
What is the dual MOA of Omlonti (0.002% omidenepag isopropyl solution)?
Selective prostaglandin EP2 receptor agonist
Increased uveoscleral outflow
Increased TM outflow
What is the advantage of using Omlonti (0.002% omidenepag isopropyl solution)?
less likelihood of inducing prostaglandin associated orbitopathy
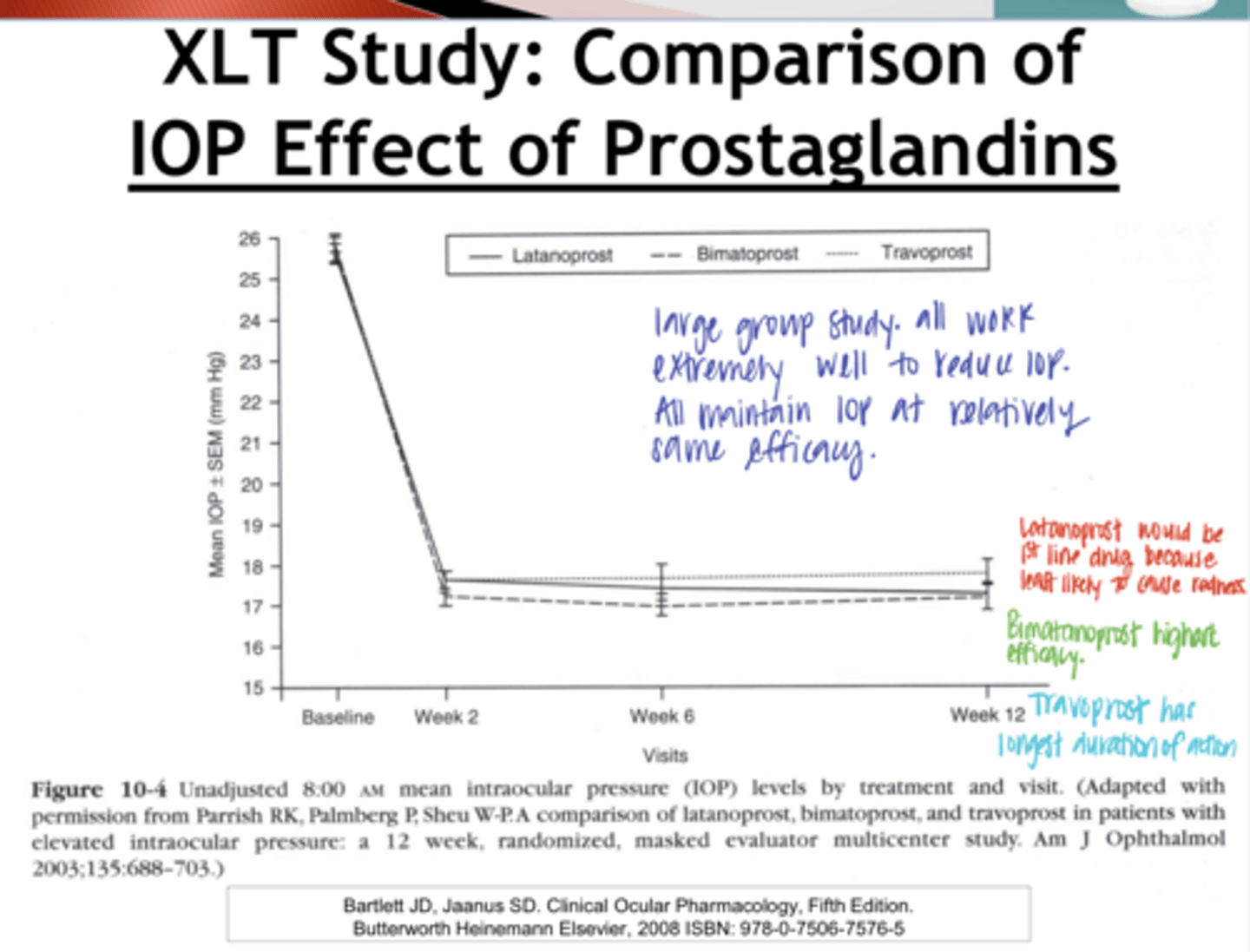
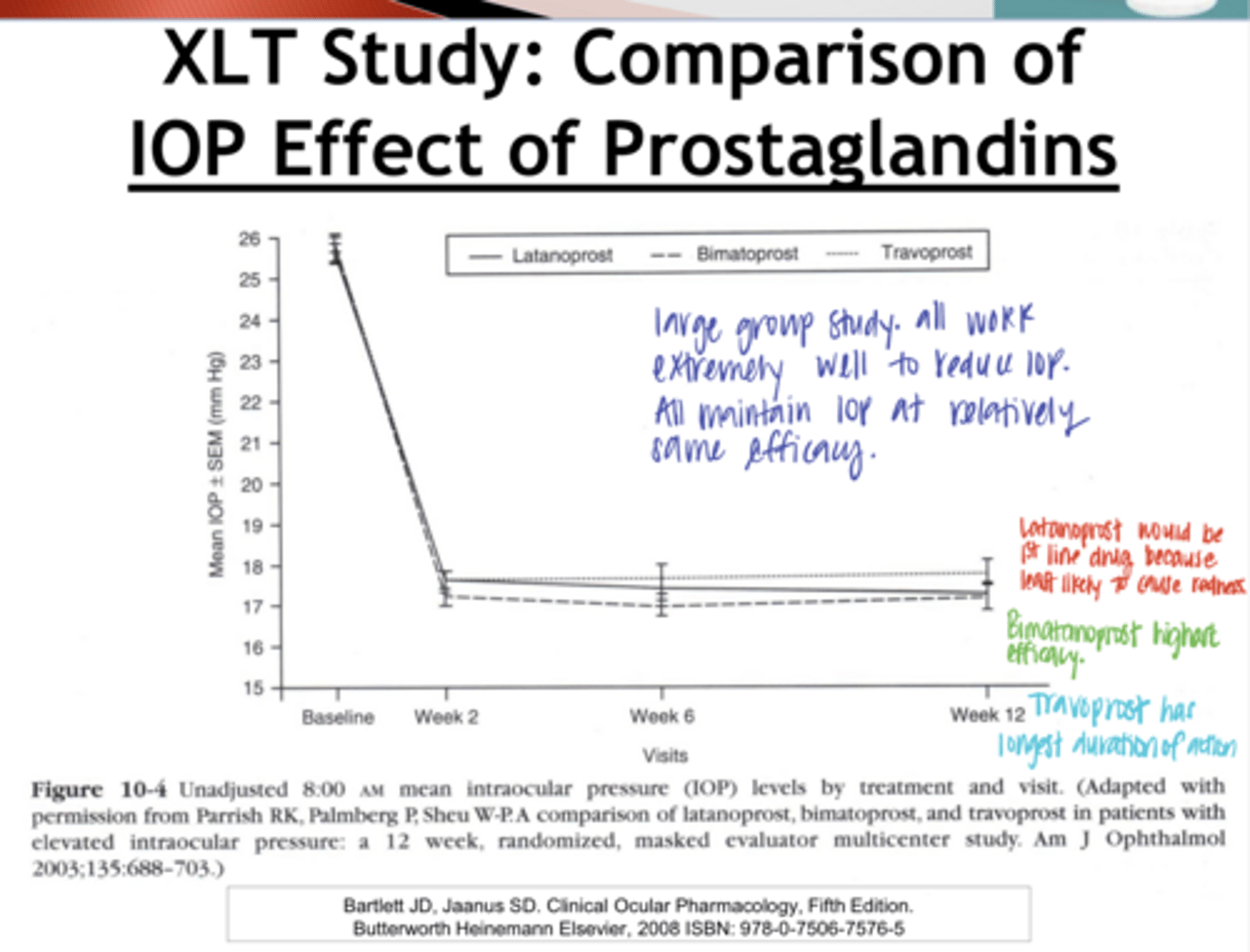
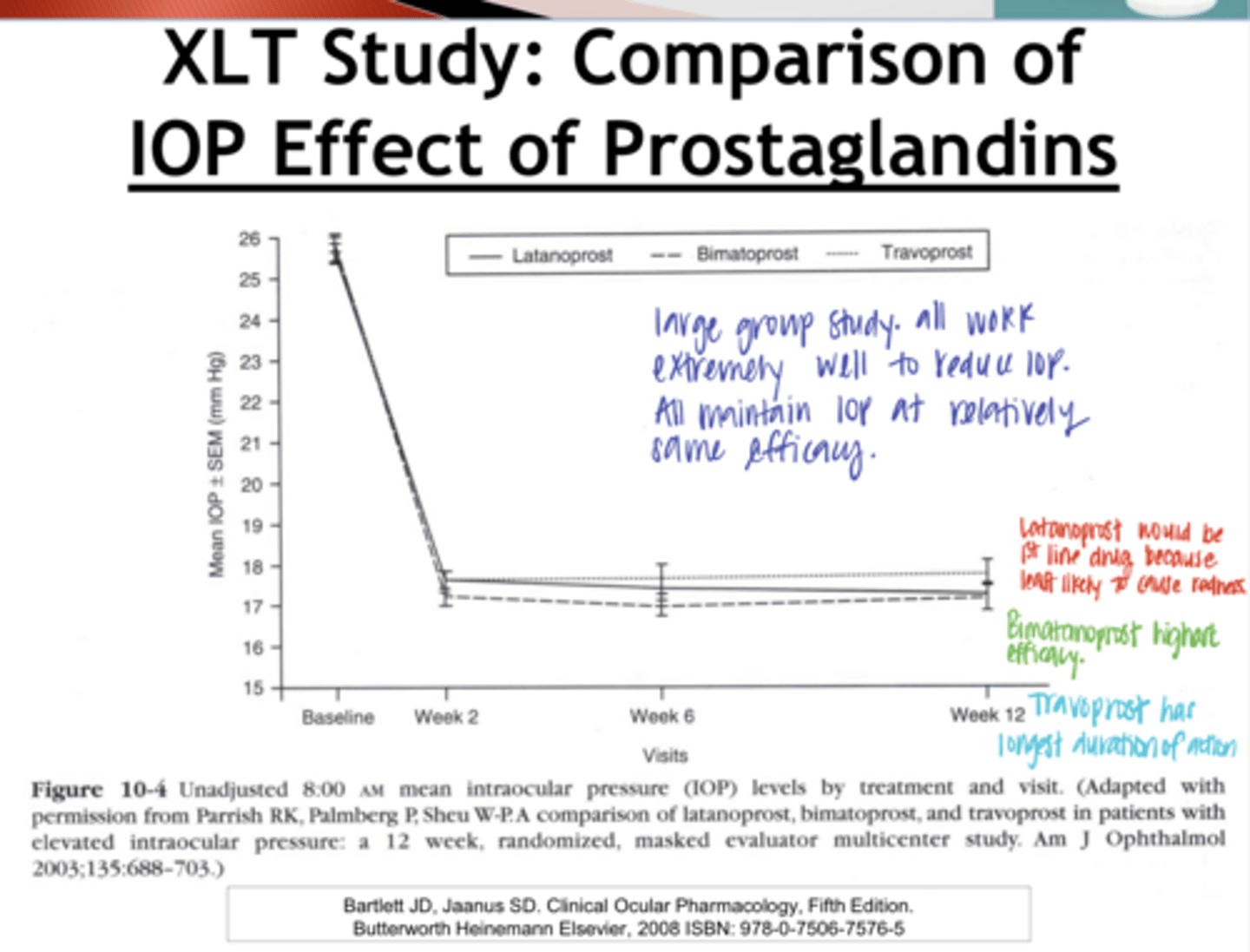
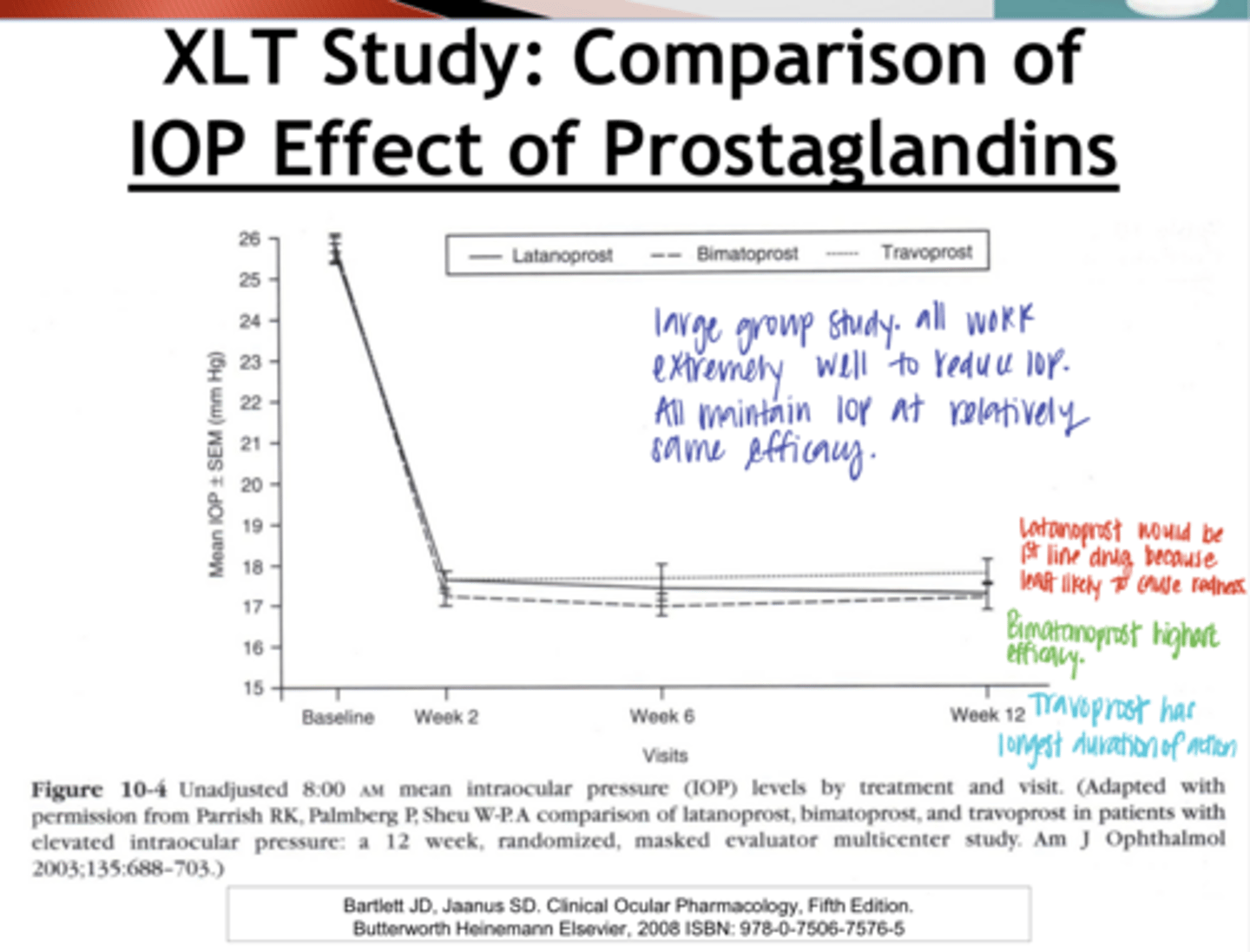
Comparison of IOP Effect of Prostalandins (Pic)
Comparison of IOP Effect of Prostalandins (Pic)
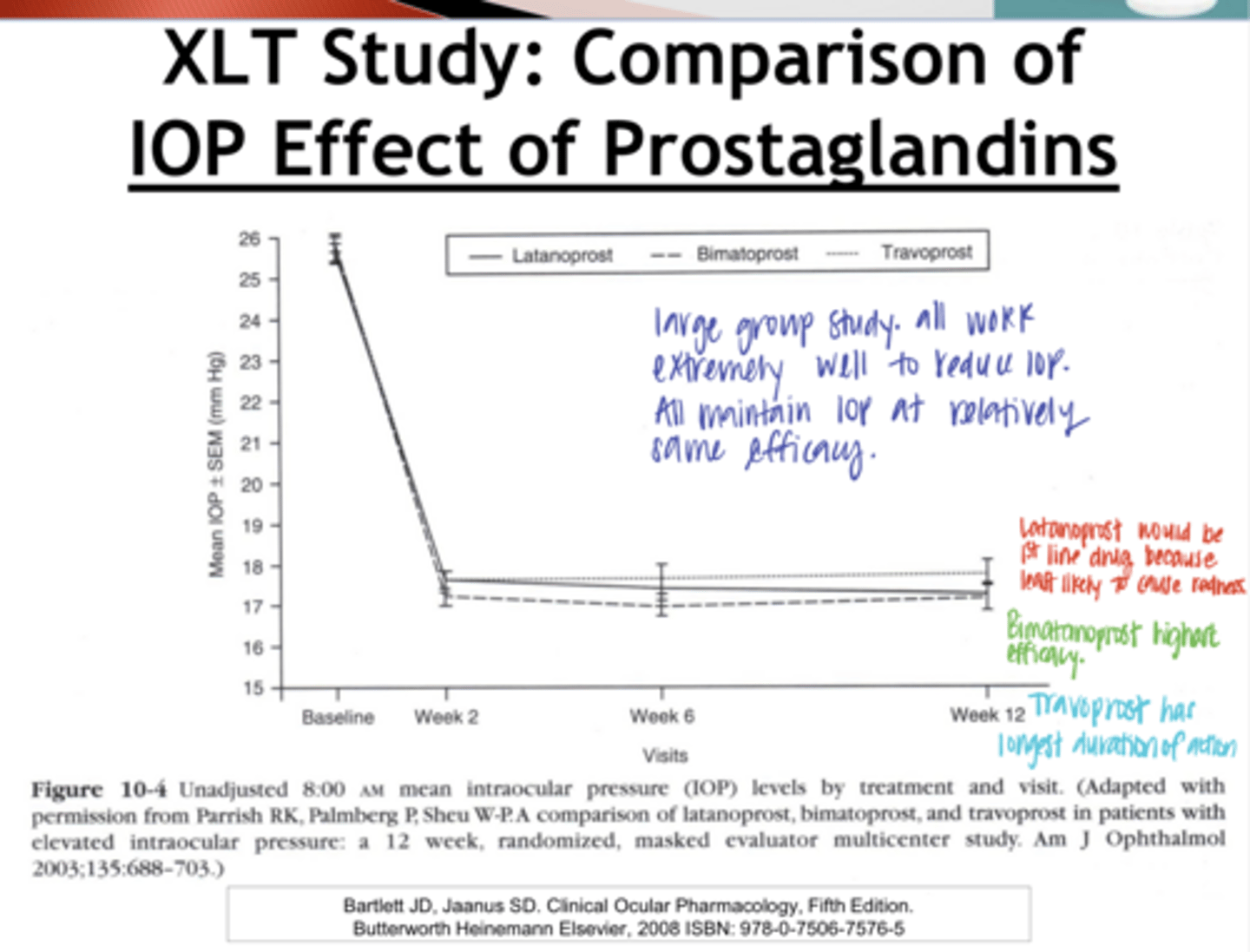
What did the Comparison of IOP Effect of Prostaglandin Study Show?
All meds studied (Latanoprost, Bimatoprost, Travoprost) were extremely effective and were equally efficacious
What are some reasons to switch from one PG to another?
-Formulary/insurance reasons
-To reduce side effects
-To get improved efficacy
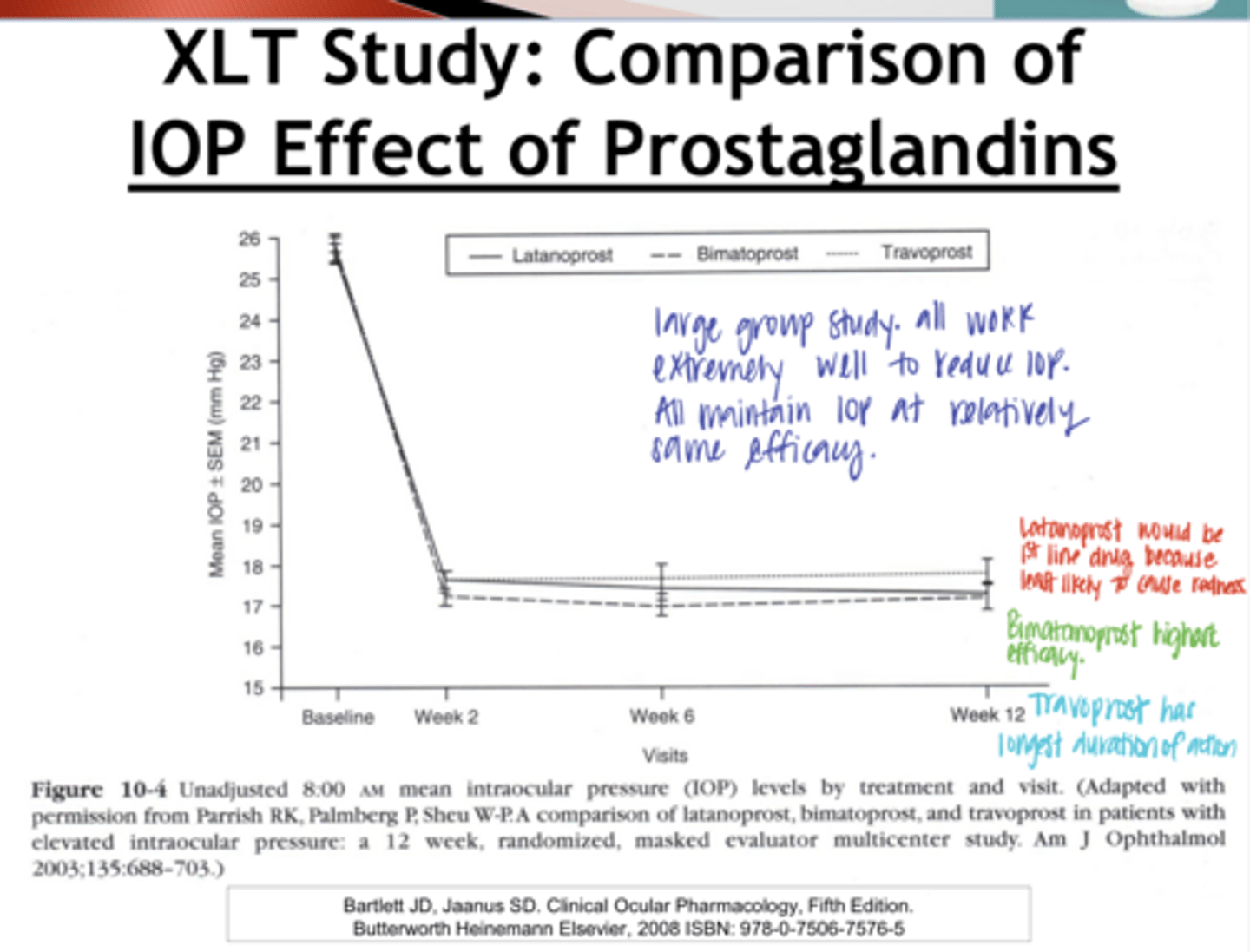
Since the main side effect of Prostaglandin is usually redness, if you want to reduce this, what should you switch to?
-Latanoprost
-Iyuzeh
If you want to Improve efficacy, what should you switch to?
-Lumigan/Bimatanoprost
-Vyzulta
True or False:
If a prostaglandin medication is NOT working, you will get better efficacy NO MATTER what you switch to d/t better patient compliance
true