brain dvpt 2
1/154
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
155 Terms
first trimester (wk 1-12)
development of major body structures & organs
by 4wk: brain & spinal cord starts to form
by end:
heart beating regularly
fingers & toes have formed
nerves & muscles begin 2 work together
eye lids have formed, remain closed until ~28wks
fetus = 1oz
second trimester: wk 13-28
period of growth
by end:
can hear, see, suck
skin, hair, nails formed
lungs formed, but dont work yet
taste buds on tongue
ovaries/testicles formed
lanugo (fine hair) covers body
can feel baby’s movements (flutters)
weight = 1.5lbs
third trimester: wk 29-40
bones hardening
body fat increases
movements more noticable
lung formation complete
lanugo falls away
weight by end: average 6-9lbs
birth weight normality
normal → more than or equal to 2500grams/5.5lbs
low → less than 2500/5.5lbs
very low → less than 1500 grams/3.3lbs
extremely low → less than 1000 grams/2.2lbs
gestational age normality
normal → more than or equal to 37 weeks
preterm → less than 37 weeks
very preterm → less than 32 weeks
extremely preterm → less than 29 weeks
corrected age
chronological age in weeks - weeks premature
(when a child is born preterm their milestones r tracked but not the same way as normal babies so their age is corrected)
disparities between white, native, black, asian, pacific islander moms
Native and Black mothers additionally are 3x more likely to die of child-birth related causes than white
in 2021:
black → 3% increase in preterm births
native → 6% increase in preterm births
asian & pacific islander → largest preterm birth increase at 8%
asian mothers saw decreased birth rate in yr of 2021 and have the lowest preterm birth rate overall
covid → ppl w this r 40% more likely to go into preterm labor
medical factors associated with preterm births
previous preterm birth
family history of infertility
multiple gestation
placental abnormalities
uterine abnormalities/infections
preeclampsia: when pregnant woman dvp high blood pressure & protein in urine after 20th week
demographic differences
men have higher prevalence of neonatal complications and adverse neurodevelopment outcomes
rates of very low birth weight and very preterm birth:
2x as high in nonhispanic blacks as whites
higher in single mothers
higher in family of lower ses
differences hypothesized due to:
effects of stress on neuron-endocrine system
smoking + drug use
underutilization of prenatal care
susceptibilty to genital tract infections
combined effect of low folate intake and GE interactions
medical interventions for preterm births
advances in neonatal intensive care in 1960s resulted in increased survival and reduced morbidity [markedly in VLBW AND ELBW cohorts]
resuscitation
assisted ventilation and high pressure ventilation
drug treatments
IV nutrition
phototherapy for jaundice
surfactant for immature lungs (introduced in 1990s)
antenatal steroids and antibiotics
environmental interventions for pre term interventions
environmental controls over exposure to light, loud noise, sleep interruptions
positioning and handling procedures
parent education and counseling
effects of pre term birth on brain
brain growth is rapid in late fetal period
increases in total brain volume
proliferation of glial cells
formation of myelin
growth of axial and dendritic spines
synaptogenesis
axonal pruning
primary processes responsible for brain damage in neonates with VLBW/VPTB:
hypoxic ischemia (INADEQUATE FLOW OF BLOOD AND OXYGEN TO THE BRAIN)
associated oxygen & glucose deprivation
common brain abnormalities
PVL (periventricular leukomalacia)
involves death of small areas of brain tissue (white matter) around ventricles
death around ventricles can enlarge space in brain and not as much gray and white matter in the brain as we want
creates holes in the brain
hemorrhagic infarctions (IVH=intraventricular hemorrhage)
infarctions are tissue areas in the body that have died because they did not receive proper oxygen - in this case in the brain
major complication of premature birth
cause of CEREBRAL PALSY and HYDROCEPHALUS
ventriculomegaly
lateral ventricles are dilated
brain regions most affected by preterm birth
subcortical structures and circuits connecting these to frontal and parietal regions
diffuse reduction in white matter
cortical atrophy
lesions in basal ganglia, hippo campus, brainstem, cerebellum
larger ventricular volumes
structural abnormalities in school age kids & adults
thinning of corpus callosum
diffuse reductions in white matter
ventricular dilation
porencephaly (very extreme birth weight kids)
cyst or cavity filled with CSF dvps in brain
very rare central nervous system disorder
usually result of damage from stroke or infection after birth
intraparenchymal cysts secondary to IVH & PVL
neuropsychological outcomes of preterm births
risk of cognitive, learning, and behavior problems
persist into school - age and adulthood
lower bw & preterm birth related to poorer outcomes
lower outcomes also related to neonatal complications
ivh, pv, chronic lung disease
performances on tests of executive functions and perceptual-motor abilities more closely related to biological risks
environmental/social risk factors better predict verbal ability, IQ, and behavioral outcomes
VLBW/VPTB vs NBW
mildly reduced global cognitive ability
areas of neuropsychological functioning most affected:
executive functioning (EF)
perceptual-motor skills
memory
high rates of learning disorders (LDs), special education plactice, and grade repetition
weaknesses in math are prominent
behavior difficulties most often involve inattention
late pre term birth vs very preterm birth and normal term birth
lptb vs vptb kids → experience fewer medical complications/lower morbidity risk
neuropsychological deficits are more mild
lptb vs ntb kids → still have more intellectual/neuropsychological deficits
subtle negative effect on intelligence, academic performance, ef, visuospatial/visuomotor functioning, language, and internalizing behavior problems
developmental and neuropsychological group differences have not been found to be universally common
parents health at the time of having child will GREATLY impact the health of the child
current research → NEUROPSYCH OUTCOMES IN PREK KIDS (baron et al. 2011)
aimed to examine the specific neuropsych deficits in pre term and extremely low birth weight kids born btwn 2004-2006 of varying gestational ages
preschool age is an important neuromaturation time neglected by past lit
interested in knowing if deficits expected in premature kids would remain when the corrected age was accounted for
PT and ELBW preschoolers had significant immaturities in their neuropsych dvpt, but most performed within norm limits
some deficits are apparent despite age correction, tho scores vastly improved
research highlihts the importance of early interventions and positive impact on outcomes
neuropsych outcomes for LATE preterm birth
for many years it was thot that ppl born near full term (ie 34-36 6/7 weeks) did not suffer neuropsych consequences of LBW & VLBW kids
current research points out that although these kids are not at risk for the most harmful deficits, significant risks do exist for birth just a few weeks premature
baron et al 2012
near full term birth infants r at risk for problematic medical complications, neurological development, and subtle neuropsychological weakness
outcomes are significantly different for those born near full term when cmopared to those born LBW/VLBW and full term, but more research incorporating this age bracket is needed
auditory system in steps
begins with cochlear nerve to dorsal and ventral cochlea
travels through superior olivary nucleus & trapezoid body (pons)
travels through lateral lemniscus
ascends to the inferior colliculus in midbrain
medial gen nucleus of the thalamus
primary auditory cortex in temporal lobe (heschel’s gyrus)
auditory system areas
ventral cochlea
dorsal cochlea
superior olivary nucleus & trapezoid body
lateral lemniscus
inferior colliculus
medial geniculate nucleus of thalamus
primary auditory cortex
ventral cochlea
encodes intensity info
dorsal cochlea
encodes information and analyzes quality of sounds
superior olivary nucleus & trapezoid body
modulates localization of sound and the intensity of sounds
lateral lemniscus
acoustic startle and likely modulates the amplitude of sounds
inferior colliculus
integrating auditory stimuli and actions
medial geniculate nucleus of thalamus
further processing and integration of auditory stimuli
relays to aud cortx
primary auditory cortex
cortical processing of sounds, noise & auditory info
temporal lobe
primary auditory cortex
TONOTOPIC ORGANIZATION (ie low freq processed ANTERIOR and high freq sounds processed POSTERIOR)
NO strict contralateral rep of auditory world in way that visual and somatosensory cort
types of hearing loss
conductive
sensorineural
mixed
conductive hearing loss
occurs when sound is not conducted properly from the outer ear to the middle ear
results in a reduction of sound level
caused by → foreign body, cold, ear infection, fluid in middle ear, etc
sensorineural hearing loss
occurs when there is damage to the inner ear (cochlea) or neural pathways
often irreversible reduction or loss of sound
caused by → toxins, aging, head trauma, exposure to loud noises, illness, etc
mixed hearing loss
combo of conductive and sensorineural hearing loss
neuroanatomy of langauge
the left hemisphere is dominant in more than 95% of right handers and in more than 60-70% of left handers
two main regions (broca & wernicke) lie adjacent to the sylvian fissure, separating the temporal and frontal lobes and language disorders associated with these associated areas have led to the concept of “perisylvian” aphasias
language areas
initial steps of language processing is the ability to identify sound based sequences (phonological awareness) and comprehend them as words
broca’s area plans and activates the production of sequences of speech sounds
ability to repeat language requires that the phonological representations generated by processing in WA be converted to motor articulatory sequences and utterances in BA
damage to wernicke’s area
fluent aphasia (bc motor articulatory regions in the frontal lobe are intact and the disturbance in convo)
characterized primarily by disturbance in production of sequences of speech sounds
damage to broca’s area
nonfluent aphasia (with intact comprehension)
able 2 comprehend, but when they go to speak it is choppy and disflient like broken language)
broca and wernicke’s areas are connected by
arcuate fasciculus - a large subcortical white matter pathway
damage to this = conduction aphasia
language lateralization
the speech/langauge zones are located in BOTH hemispheres
LEFT = dominant in over 95% of right handers and 60-70% of left handers
RIGHT = some aspects of language like prosody (flavor / intonation/ emotional valence/ intensity of loudness & softness / playfulness)
nondominant hemisphere: recognition and production of affective elements of speech
subcortical structures = THAMALUS + BASAL GANGLIA
the language areas
the speech zones (ie broca, wernicke, sensory/motor areas of face and supplementary speech areas) are located in both hempispheres
stimulation of speech zones resulted in positive (vocalizations but not speech) & negative (inability to vocalize or use words appropriately)
however these studies did not support a strict localization model
[stim outside of speech zones can disrupt speech and stim of speech zones affects more than just speech]
thus, subcortical structures and right hemisphere areas have inputs to lang (ie prosody
DVPTL LANG DSRDRS IE dyslexia/apraxia of speech/dysarthria R NOT APHASIC DSRDRS
aphasia
term reserved for acquired disorder that disturbs language functions
broca’s aphasia
expressive aphasia
nonfluent speech, grammar problems, comprehension GOOD
wernicke’s aphasia
receptive aphasia
fluent speech, grammar okay, but meaningless & comprehension POOR
conduction aphasia
arcuate fasiculus affected - bridge between broca and wernickes
impaired repetition and paraphasic errors
global aphasia
both speech AND comprehension affected
anomia or dysnomia
normal fluency, comprehension & repetition
naming diffuculties (tip of the tongue phenomenon)
NURTURE theories of language development
environmental behaviorism
b.f. skinner
language shaped by reinforcement when child imitates speech
correct words are rewarded
trial and error
child gets the bottle after saying “milk”
learning process
mom says “daddy” every time he walks into room
however, how would one explain a new utterance?
NATURE theories of language development
nativist
noam chomsky
language is innate — etched into the structure of the mind
language acquisition device
proposed this was a neurological system that contained a set of rules
we chunk info and theres a way that we organize it and are naturally able to use it
universal grammar → common to all language
speak in a rule-oriented fashion as soon as enough words are acquired
NATURE + NURTURE theories of language dvpt
interaction btwn inner capacity and environmental influence
lev vygotsky
zone of proximal development
social context and social exchange are the sources of language acquisition
language leads to thought
when kids are around others who are similar and slightly more advanced in dvpt, those kids tend 2 learn at faster rate than kids w diff expce bc they are in proximity of that expsure
overtaxing can be too much tho so u need the right chemistry within group to have right kind of learning
current research about language development
kids transition from BABBLING @6MONTHS to FULL SENTENCES BY 3YRS regardless of culture
young infants exhibit universal capacity to detect diffs btwn phonetic contrasts used in worlds langs
by age 1 → native lang phonetic abilities increase & non native discrimination decreases
parallel structure diffs in brain (pruning)
better discrimination assocaited with faster vocab growth (bidirectional)
social intxns play role in learning language
motherese (high pitch slow + exaggerated) = good for child
language as a system
language is not just communciation but a structured system with a finite set of elements BUT infinite set of possibilities → makes language unique to humans
these elements include words which r composed of phonemes (sounds of language)
words are combined in predictable ways to yeild a potentially infinite number of sentences
structural components of language
phonology (sound system)
syntax (grammar)
semantics (vocab)
functional components of language
discourse processing
pragmatics (social rules)
structure in dvpt of functional
phonology
phonological awareness
phonemic segments
morphology
study of structure and form of words in language
including inflection, derivation, and the formation of compounds
prefixes, suffixes, roots
syntax
word order
sentence patterns
sound element of language development
speech sound (phonological) awareness
ability to segment language into sounds which makes up words
conscious focus on the acoustic signal
language play serves as practice and facilitates the acquisition of form
deficit is dx as speech sound disorder
speech sound disorders
phonological development
incidence 5% of young kids
ca 2-5yrs
deletion of final consonant ca/cat
fronting: t/k, d/g → “mommy, div me tiss”
most kids outgrow or “suppress” phonological processes
for those who don’t, association w later phonological deficits, specific learning disorder, with impairment in reading
amenable to treatment
word element of language development
segmenting sentences into words
seek word meanings
words are tied to communicative functions
awareness that words represent concepts independent of the functions they serve
words r symbols
content in language system development
knowledge of objects
relationship between objects and events
content categories
concept development
temporal
spatial
causal
quantitative
use of functional language system
communicative intent
conversational rules
turn taking
topic control
cohesion
ordering of ideas
inflection
pronoun reference
pragmatics
involve three major communication skills
using language for diff purposes
changing language according to needs of lisstener or situation
following rules for convos and storytelling
language disorders
language deficits → deficiency in set of language skills that develop with exposure
language delays → slowed acquisition in set of language skills that develop with exposure
disorders (impact functioning)
aphasias
communication disorders
specific learning disorder, with impairment in written expression and/or reading
speeded access to verbal codes
access to phonemic or semantic categories and speed of recall
word retrieval or naming difficulties
can also affect reading
verbal fluency
speeded naming
importance of language
verbal deficits tend to have more obvious and widespread cognitive consequences than deficits in other functional systems
task instructions are frequently verbal
self regulating and self critiquing mechanisms are verbal
most of the school day is all verbal
self talk → verbal probs limit us in what we can do to motivate ourselves to do something
communication disorders
most common developmental disorder in kids under age 5
75-80% of early intervention cases involve speech and language issues
disorders:
language disorder
social (pragmatic) communication disorder
speech sound disorder
childhood onset fluency disorder (stuttering)
unspecified communication disorder
childhood disorders
language disorder
speech sound disorder
social (pragmatic) communication disorder
not associated with ID, autism, hearing impairment, or specific social-environmental factors
incidence rates: 7.6% of 5 year olds
heritable
gender diffs → 4boys:1girl
afferent nerve fibers
carry sensory nerve impulses toward the CNS
affects what you feel
approaches the brain
efferent nerve fibers
carry motor nerve impulses away from the CNS to muscles
effect on what you do
exits the brain
spinal cord dorsal/posterior column
ascending sensory fibers
spinal cord ventral/anterior column
descending motor fibers
how does motor info travel from the brain to the body?
primary motor brain regions
primary motor cortex/motor strip
premotor & supplementary motor areas
basal ganglia
cerebellum
descending motor pathways
spinal cord
primary structures involved in motor development
cerebellum
coordination of movement and posture
adaption of movement to changing external and internal conditions
has been implicated in attention and decision making
organized ipsilaterally (on the same side - ie right side of cerebellum manages right side of body)
basal ganglia
subcortical nuclei (cluster of neurons) involved in initiation and control of movement
located deep beneath the cerebral cortex
basal ganglia is comprised of
caudate nucleus
putamen
globus pallidus (pallidum)
associate areas include substantia nigra, subthalamic nucleus, and projections from basal ganglia to thalamic nuclei
cerebellum
“little brain”
recieves sensory input from spinal cord and other parts of brain
functions: smoothly coordinates motor movements and assists with motor planning
integrates inputs to fine tune movement
coordination
precision
accurate timing
damage causes problems with fine movement, equilibrium, posture & motor learning on the side of the body ipsilateral to the lesion
practicing learning motor patterns
circular expereince of practice coupled with novel experience = motor fluency
complex movements are result of “smoothing” out a motor movement in terms of fluidity (timing) and accuracy
ie walking toy thing & playpen with dangling things = practice and opportunities for better motor control
motor transfer and motor memory
transfer = learned motor movements can b adapted and applied to new learning
motor memories are retrieved, modified to adapt to the new skill, and then acquired = new motor learning
cerebellum thought to be a big contributor to motor memory development
the fact that we can ride a bike after not riding it for a long time is because of the motor memory
primary motor cortex
strip of tissue located on the frontal lobe alongside precentral gyrus
generates neural impulses that initiate and control the execution of purposeful movements based on input from sensory cues
(ie sends out signals that cause movement)
somatotopic organization aka body is mapped across motor cortex
classic homunculus but not as clearcut as initially believed
contralateral organization
hemiplegia
loss of voluntary movements on the contralateral side of the body, particularly in the distal effectores (ie fingers)
[aka paralysis of one side of body]
frequently experienced secondary to a hemorrhage of the middle cerebral artery
reflexes are initially absent, but return within a couple of weeks and may become exaggerated
spasticity is evident — muscles that oppose the effects of gravity become extremely rigid
in the absence of cortical inhibition, primitive reflex mechanisms meant to maintain postural stability take hold
hemiplegic patients can no longer generate an action based on internal goals and desires
supplementary motor area
helps with organizing & planning out the steps of complex movements
located in front of primary cortex
has some nerve projections to the spinal cord and brainstem
prefrontal cortex
higher order structure involved in complex thinking and decision making (has subdivisions that play specific roles)
movement + motor aspects of speech
behavior programming
integration of sensory info
integration of arousal, emotion, motivation & behavior/movement
executive functions
prefrontal cortex subdivisions
primary motor cortex + supplementary motor areas
orbital prefrontal cortex → executive control of social and emotional behavior (decisions about social interactions; not automatic)
lateral prefrontal cortex → executive control of cognition (attention, focus, planning, working memory)
medial prefrontal cortex → executive control of motor behavior
multiple sclerosis
affects approximately 400,000 people in the u.s. (200 ppl diagnosed weekly)
multifocial demyelinating disease → causes destruction of myelin sheath of nerve fibers - scar like lesions called sclerotic plaques form in the areas where demyelination has occurred and block or distort the normal transmission of nerve impulses
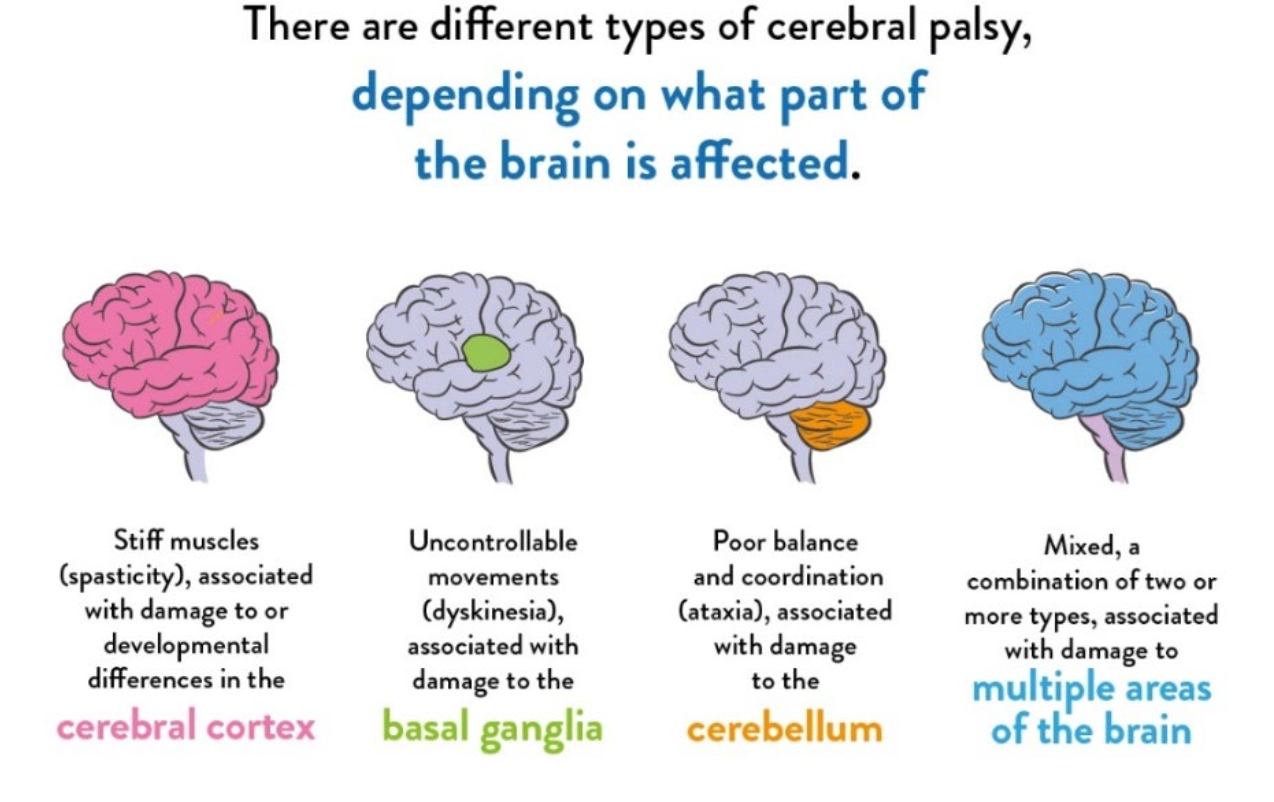
cerebral palsy
10,000 babies diagnosed annually in the u.s.
non progressive heterogeneous group of movement, postural, and muscular disorders
the area of the brain that had the insult wont change / get worse in those regions, but the demands of life will get higher so we may see the skills get weaker over time
this will happen in utero, but wont see the muscles coming online as much as would expect only when we need to use them in dvpt
types of cerebral palsy
muscular dystrophy
progressive muscle weakness and wasting
huntington’s disease
affects ~30k ppl in u.s.
affects striatum/basal ganglia (especially caudate nucleus)
symptoms include motor, cognitive, behavioral
diagnosis relies on emergence of choreoform movements
adult onset, progressively disabling, lethal disease
there is no effective treatment to delay onset or to slow decline
parkinson’s disease
affects ~ 1 million ppl in u.s.
affects production of motor neurotransmitter
symptoms include tremor, rigidity, slowed movement, and instability
no known cure but some treatments can mitigate the effects
dopamine
produced in substantia nigra
decreased dopamine due to damage to substantia nigra leads to parkinson’s
excess dopamine has been implicated in schizophrenia
pathway of visual stimuli
each eye is divided into 2 “visual fields” — a right side and a left side = “hemifields”
via optic chiasm, visual signals from LEFT hemifields of both eyes are sent to the right hemisphere and the signals from the RIGHT hemifields of both eyes are sent to the left hemisphere
optic chiasm
x shaped structure formed by the crossing of optic nerves in the brain (known as the optic commissure)
optic nerves connect eyes to the brain
left primary visual cortex (occipital lobe) receives images from the right visual field of the right and left eyes
right primary visual cortex (occipital lobe) receives images from the left visual field of right and left eye
this is due to the sorting of optic nerves at the optic chiasm so the right side of the brain controls the view of objects in the left side of visual space (+vice versa)
REMEMBER the image is inverted onto the retina when passing through the lens
summary of visual pathways
from retina
through optic nerve
crossing at optic chiasm
travelling to lateral geniculate nucleus
LGN connected to primary visual cortex via optic radiations/tracts
to the primary visual cortex (occipital lobe)
role of superior colliculus
as input “travels” to primary visual cortex, ~10% of tracts target here [aka the optic tectum]
these areas appear central to directing attention and motor functions to points of light within the visual periphery —- aka orient eyes (+other sensory stimuli) to respond to new stimuli in visual fields
van coming toward u while sitting on nyc bench
trying to catch incoming football
role of lateral geniculate nucleus
this is the major target of the two optic tracts, located in the dorsal area of the thalamus (aka relay station btwn subcortical areas of the brain and the cortex)
several of cell layers here r specialized to respond to diff types of cells in the retina, but these layers process incoming info in parallel / simultaneously
thus the unitary nature of our visual perception does not occur bc the info is being processed all at one time by one structure
from the LGN the optic radiations send “visual info” to be processed in the primary visual cortex in the occipital lobe
occipital lobe
topographic/retinotopic map → orderly spatial relationship of info, 2D representation of retinal map of visual world; axons of each retina preserve their orde as they travel back to V1
2V1s in each person (left and right hemispheres)
each has representation of opposite half of the visual field
each V1 does not j receive input from the opposite eye, but from the opposite visual field of each eye
primary visual cortex (v1)
just as image of world is inverted when projected onto retina, retinotopic v1 map is upside down and from the opposite visual field of each eye than the side of the brain
cortical magnification → MORE CORTICAL SPACE DEDICATED TO FOVEA THAN PERIPHERY (higher density of photoreceptors in fovea, thus clearer vision — resp 4 sharp, central vision)
LGN integrates temporal and spatial correlations that contribute to successful vision
recieves feed-forward input from retina AND feed-back input from v1 & other non retinal areas
LGN r not just feed forward areas, but receive 80% of their projections from the primary visual cortex
occipital lobe neuroanatomy
differentiated from parietal lobe via parietal occipital sulcus
on lateral surface of brain, no clear divisions btwn temporal and parietal lobes from the occipital lobe
while specialized for visual material, other lobes also contain visual functions
surface of occipital libe has calcarine fissure which separates upper and lower halves of visual system + fusiform gyrus on ventral surfave
2 streams for processing visual info
ungerleider + mishkin
where? → dorsal pathways projecting to parieto-occipital association cortex
analyze motion and spatial relationships between objects and between body and visual stimuli
what? → ventral pathways projecting to occipito-temporal association cortex
analyze form and specific regions for colors, faces, letters, etc
object perception
involves the ventral stream but distinct areas have been implicated for object perception
process of recognizing images is pre organized
prosopagnosia
cognitive disorder that results in an inability to recognize faces
aka face blindness
occurs when there is damage to the fusiform face area