Session 1: Joint Pathology
1/40
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
41 Terms
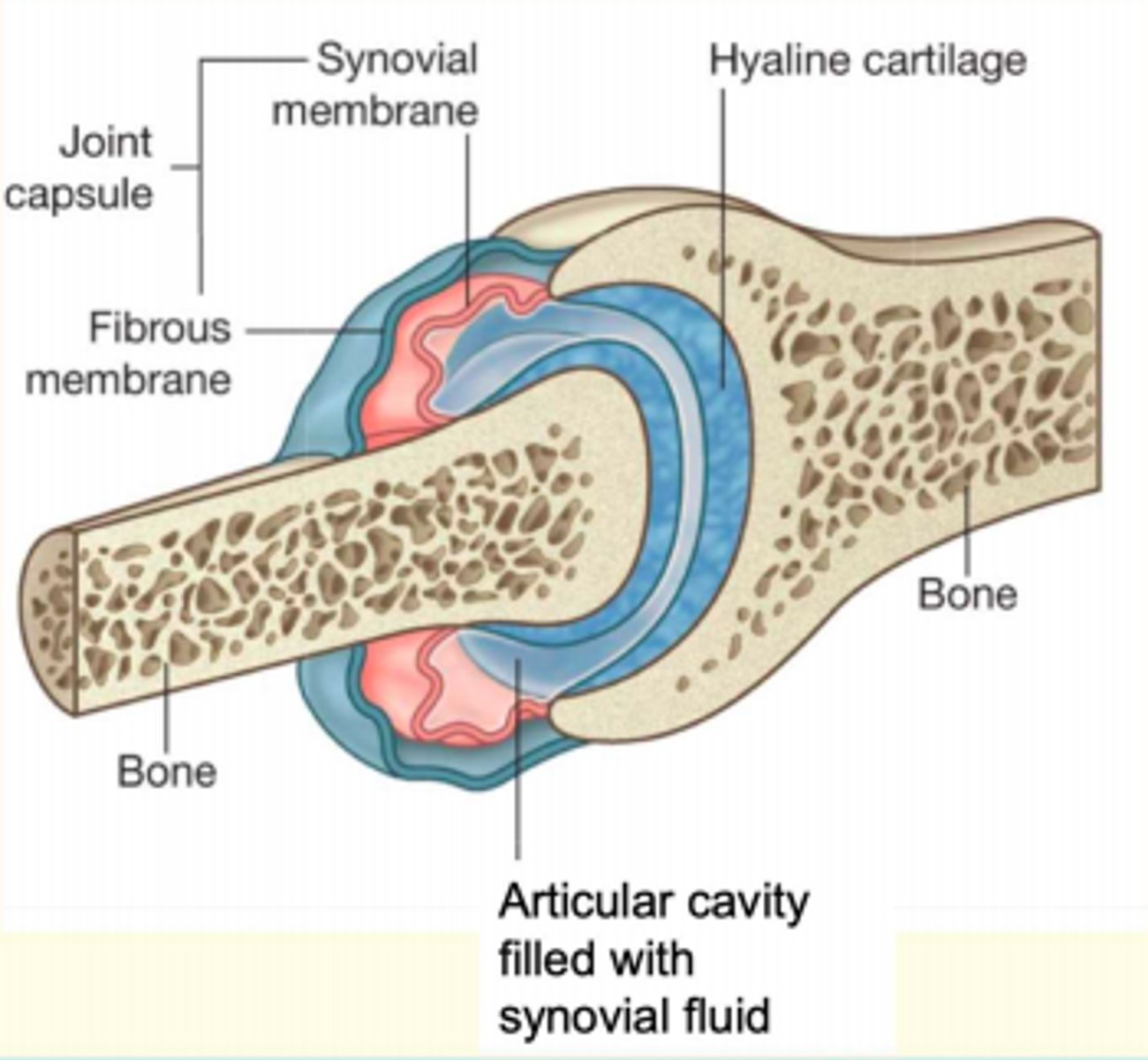
Synovial joint features
1) Capsule
Fibrous Outer Membrane
Inner Synovial Membrane
2) Synovial Fluid
3) Hyaline cartilage
4) Other Structures
Ligaments
Menisci
Bursae
Tendons
Osteoarthritis
Degenerative disorder of synovial joints
Primary OA
Idiopathic
Secondary OA
Related to trauma, congenital abnormalities, infection, or necrosis
Risk factors for OA
Non-modifiable
Age
Female
Genetics
Joint misalignment
Modifiable
Obesity
Exercise/occupational stress
Muscular weakness
Presentation of OA
- Pain at end of day
- Older people
- Crepitus
- ↓ ROM
- Morning stiffness only lasts <30 min
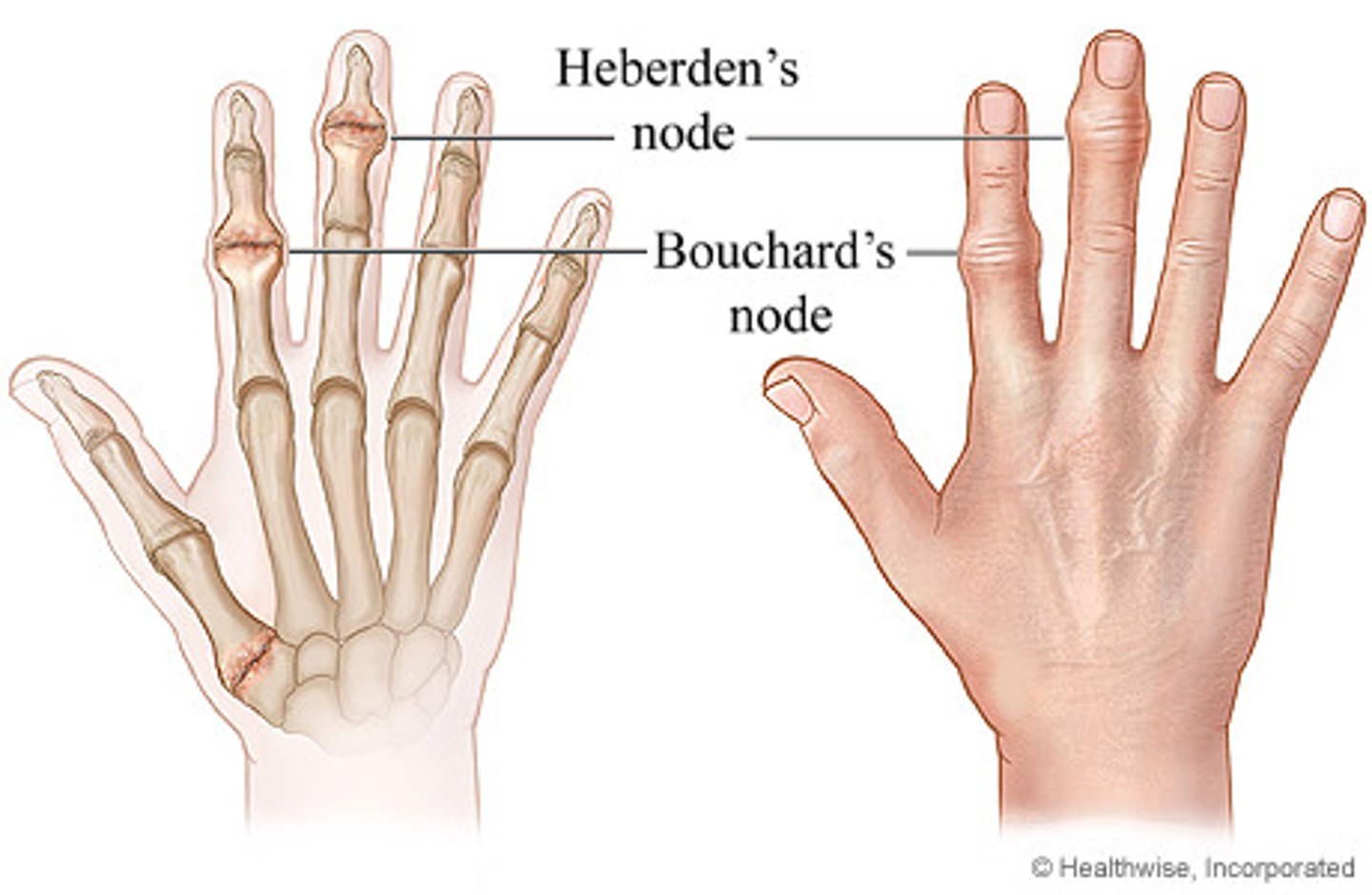
- Bouchard and Heberden nodes
Investigations OA
Routine x-ray of the affected joints is not usually needed to confirm diagnosis
Consider arranging x-ray (depending on clinical judgement)
X-ray (weight bearing)
Loss of joint space
Osteophytes
Subchondral cysts
Subchondral sclerosis

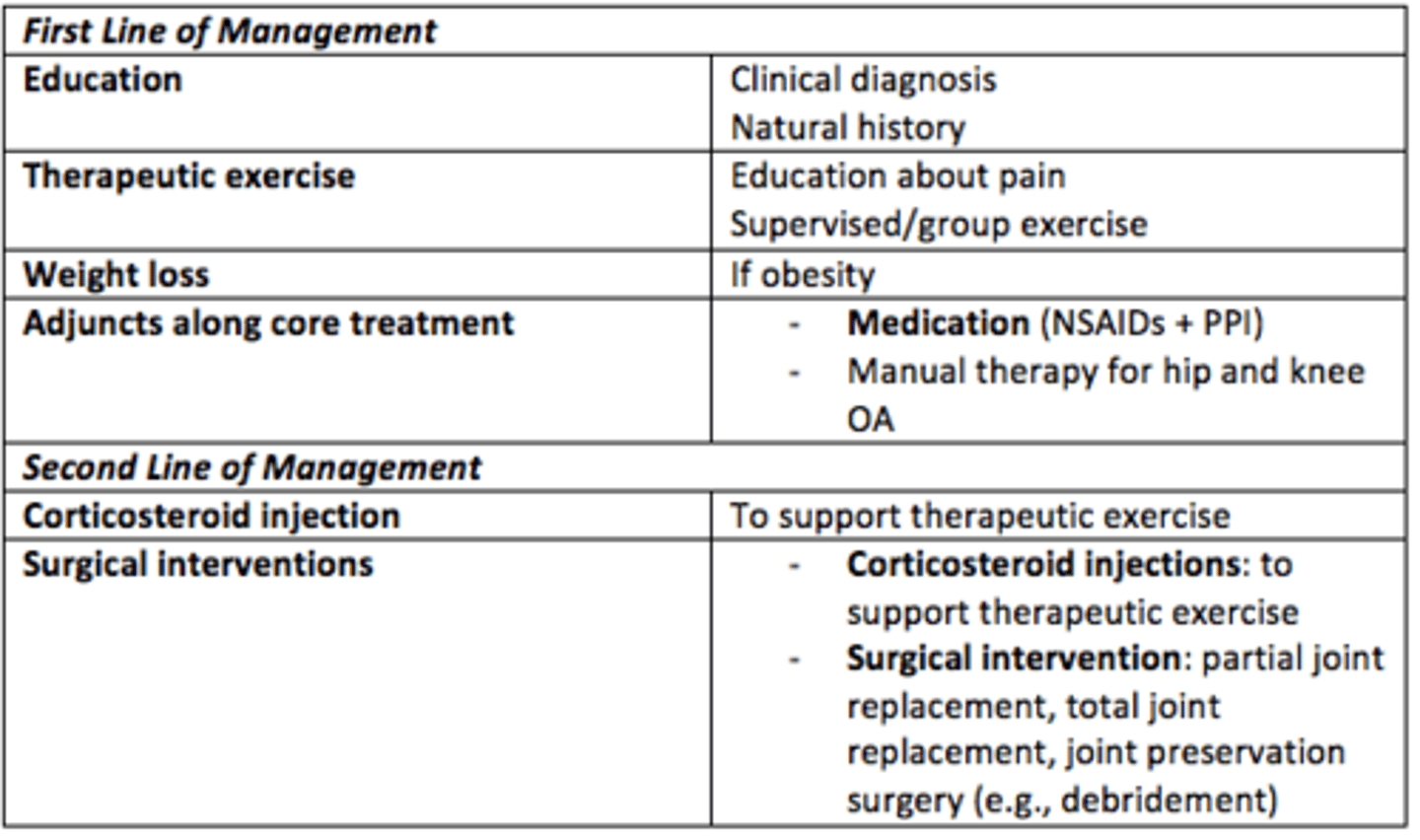
First and second line of management for OA (according to NICE guidelines)
First Line
- Education
- Therapeutic exercise
- Weight loss
- Adjuncts: medication (NSAIDs, PPIs), manual therapy for hip/knee OA
Second Line
- Corticosteroid injection
- Surgical interventions: partial/total joint replacement, joint preservation surgery (e.g., debridement)
Which joints are commonly affected in OA
Proximal interphalangeal joints (PIP)
Distal interphalangeal joints (DIP)
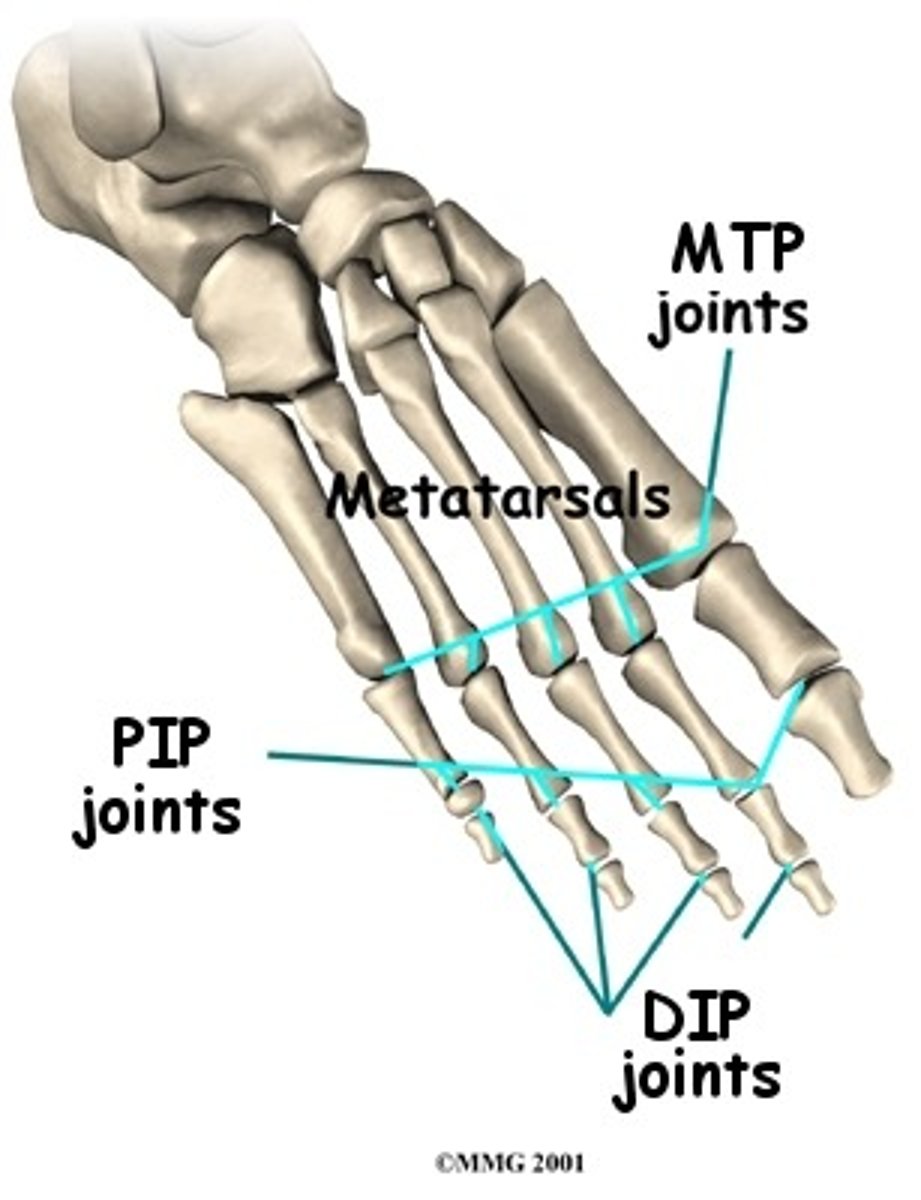
Deformities of OA
Heberden's at DIPs
Bouchard's nodes at PIPs
Rheumatoid Arthritis (RA)
Chronic, systemic, inflammatory disease affecting the synovial membranes (inflammation) of multiple joints, eventually resulting in crippling deformities
Production of autoantibodies, pathogenesis not fully elucidated. Autoimmune disease.
Risk factors RA
FHx
Female
Obesity
Heavy smoker
Presentation RA
Symmetrical pain
Swelling
Warm joints (erythema)
Stiffness
Symptoms better with activity
Stiffness is worst in morning (>1hr waking)
Poor function
Which joints are most commonly affected in RA
Metacarpophalangeal joints
Carpometacarpal joints

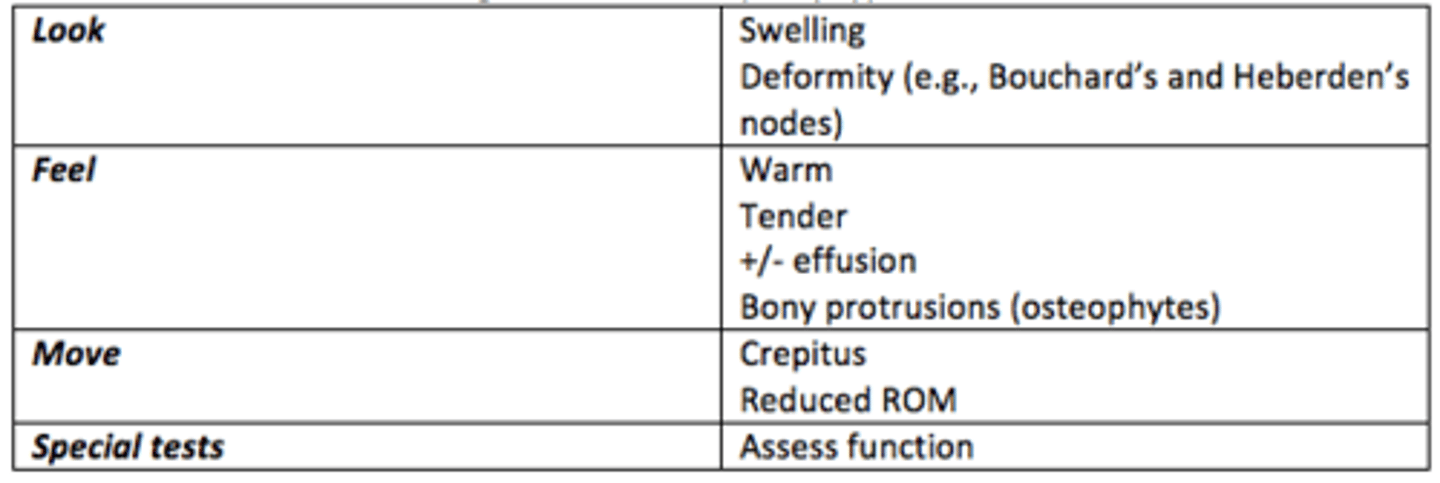
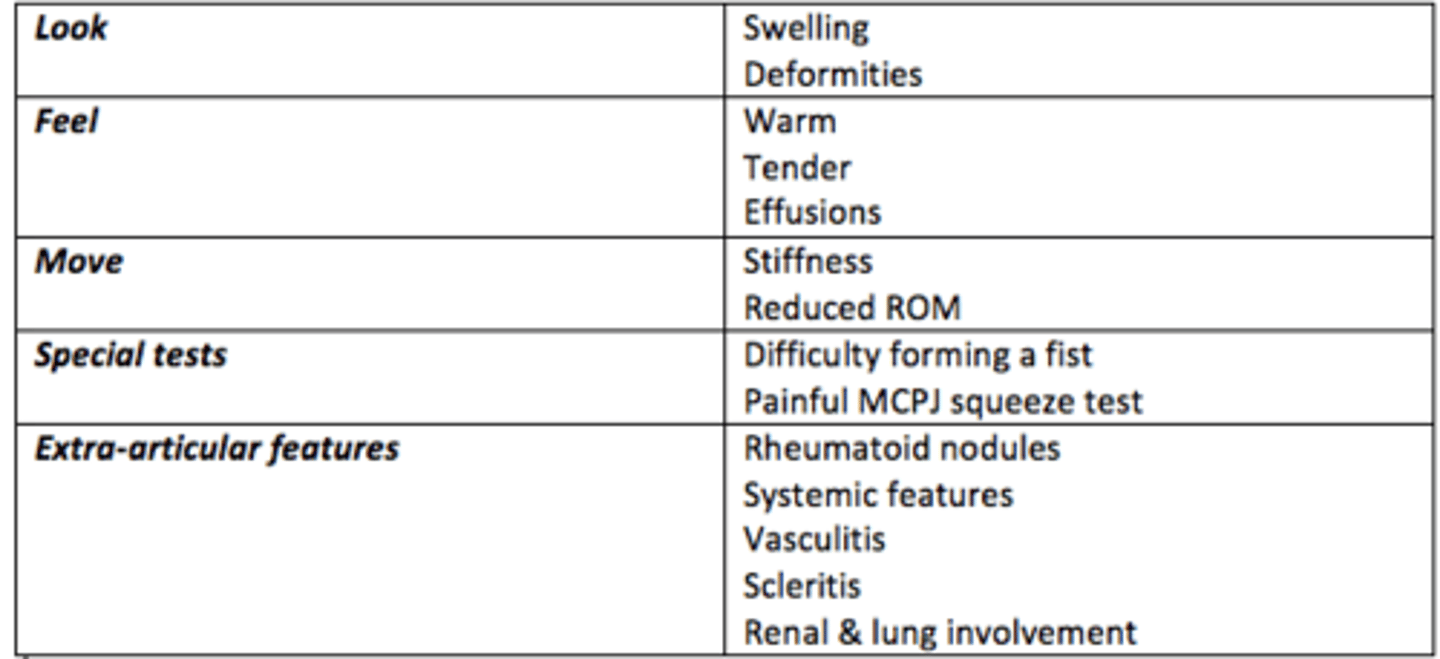
Signs of RA
SWELLING / DEFORMITITES = LOOK WARM / TENDER / EFFUSIONS = FEEL
STIFFNESS / REDUCED ROM = MOVE
DIFFICULT FIST FORMING / PAINFUL MCPJ SQUEEZE = SPECIAL TESTS
RHEUMATOID NODULES / SYSTEMIC FEATURES / VASCULITIS / SCLERITIS = EXTRA-ARTICULAR FEATURES
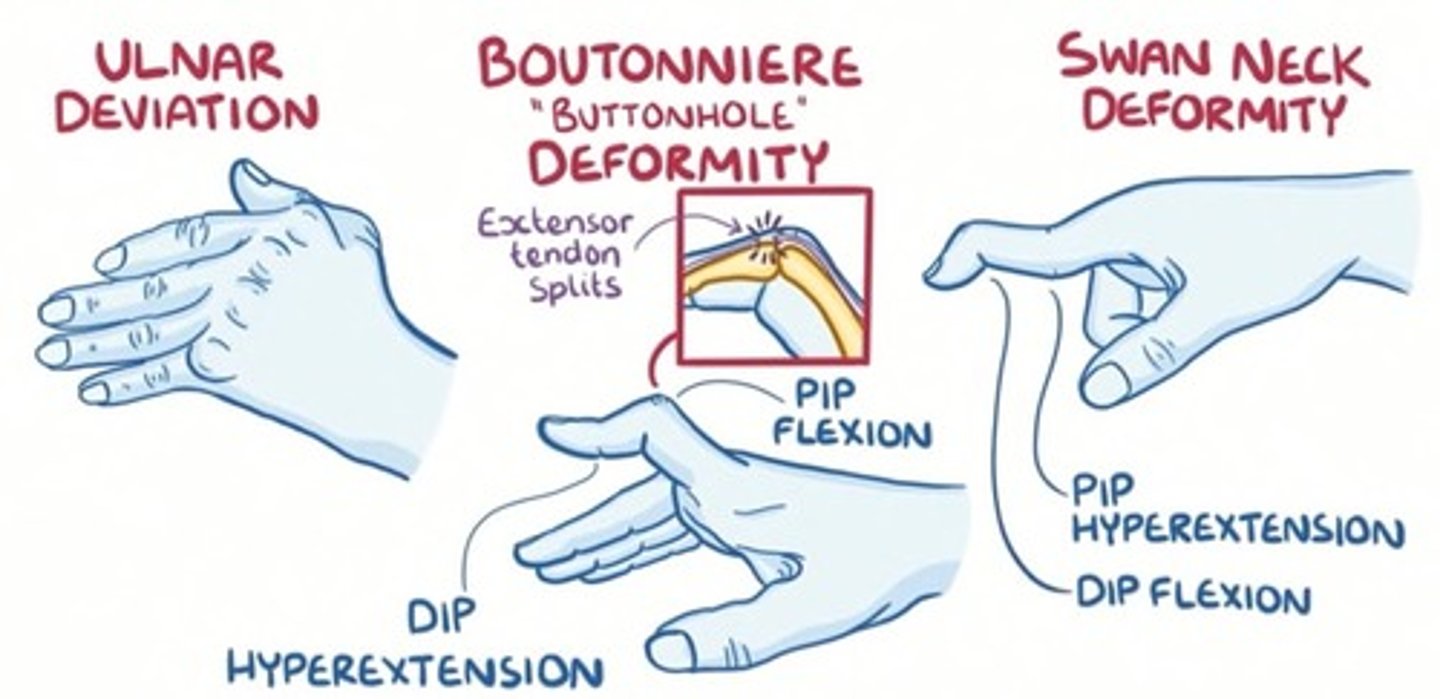
Specific deformities of RA
Special test for RA
Positive (painful) metacarpophalangeal joint squeeze (MCPJ) test

Clinically suspected arthralgia score of >4 in any of the following is considered high-specificity for RA...
1) Joint symptoms with onset in last year
2) Symptoms involving MCP joints
3) Morning stiffness (>1hr)
4) Positive squeeze test on MCP joints
5) Difficulty forming fist
6) First-degree relative with RA (FHx)
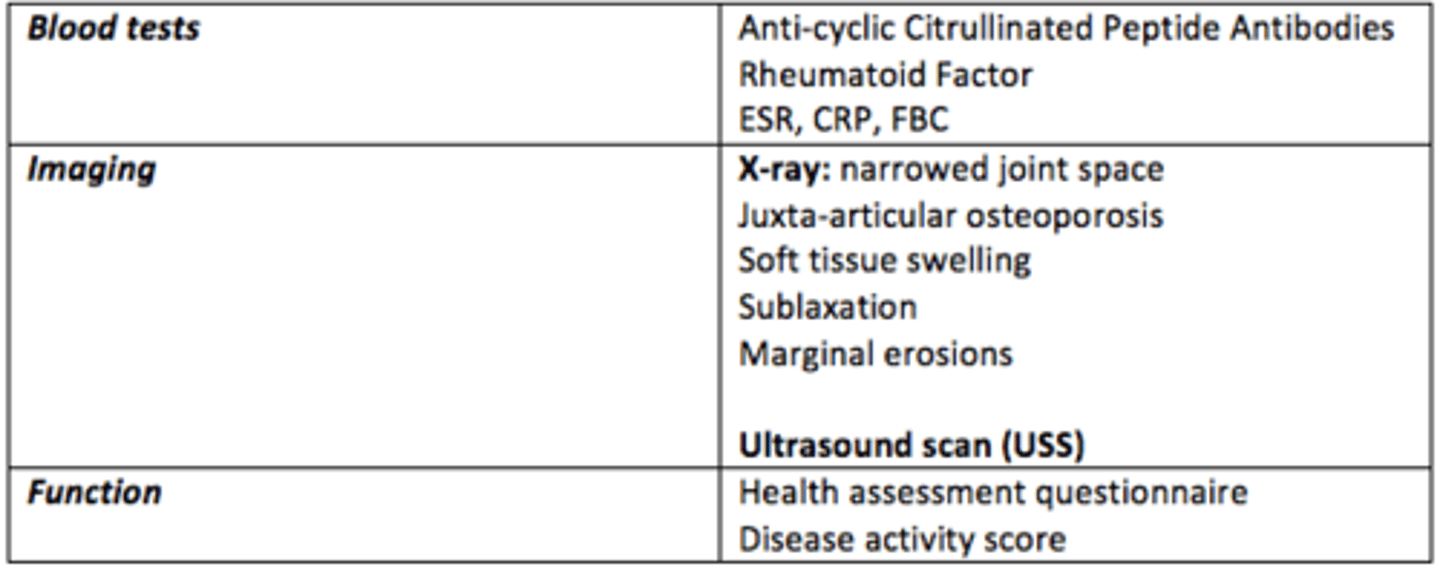
Investigations for RA
Blood tests
Anti-cyclic citrullinated peptide antibodies
Rheumatoid factor
ESR, CRP, FBC
Imaging
X-ray: narrowed joint space
Soft tissue swelling
Subluxation
Marginal erosions
Function
Health assessment questionnaire
Disease activity score
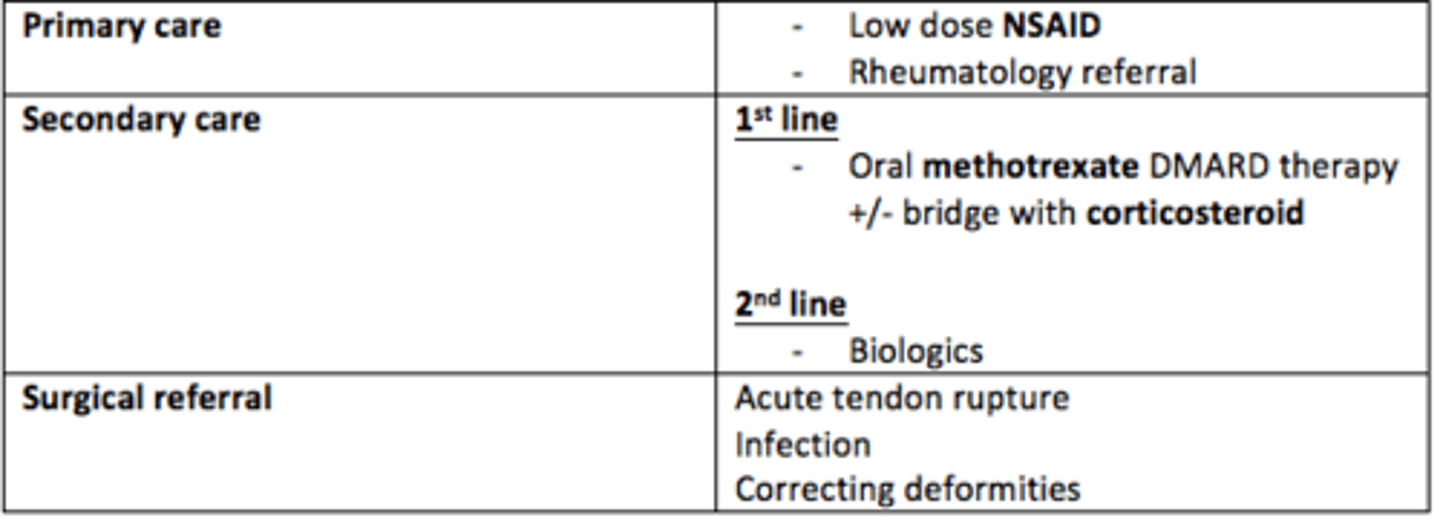
Management of RA
The aim of management of RA is to manage pain, improve functioning & prevent deformities
Primary care
- Low dose NSAIDs
- Rheumatology referral
Secondary care
- 1st line = oral methotrexate DMARDs & bridge with corticosteroids
- 2nd line = biologics
Surgical referral
- Acute tendon rupture
- Infection
- Correcting deformities
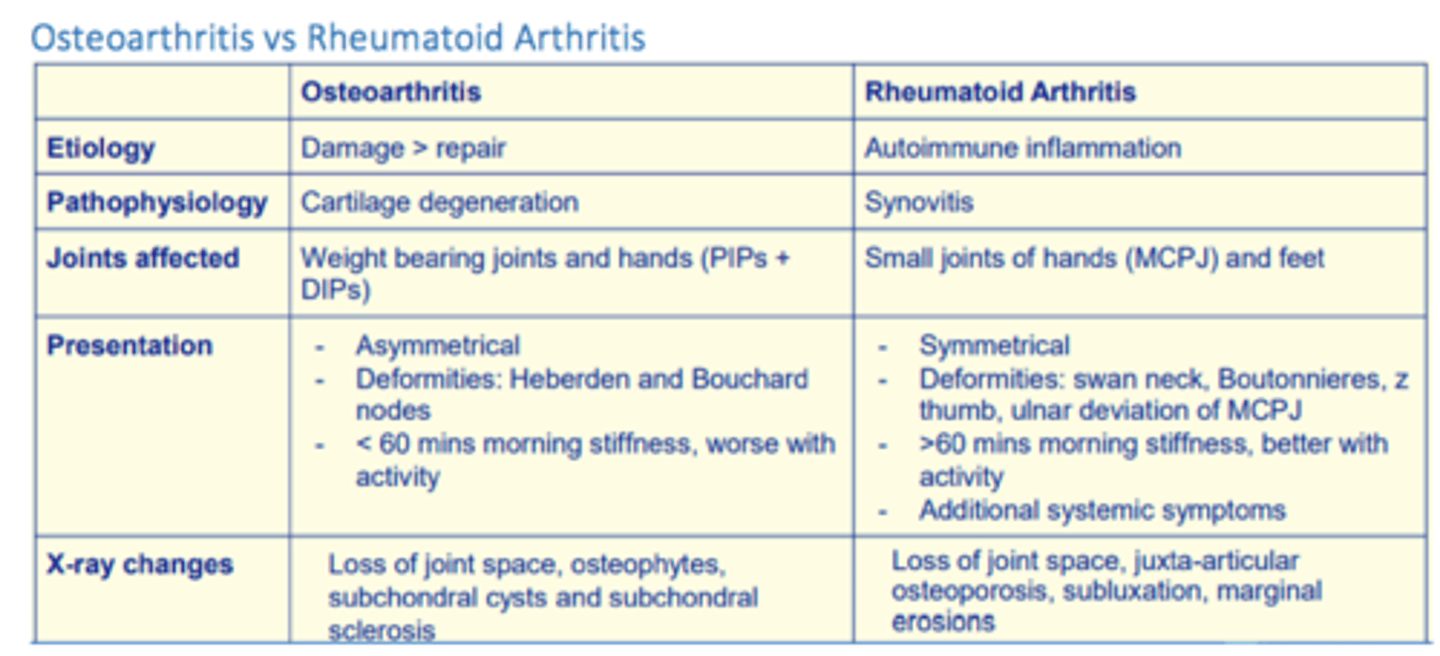
Osteoarthritis vs Rheumatoid Arthritis
Gout
Acute inflammation as result of monosodium urate crystals accumulating in the joint. Urate is a purine metabolite excreted by renal and GI systems.
Risk factors for gout
- FHx
- CKD
- Diabetes
- Hypertension
- Diet (alcohol, meat, seafood)
- Obesity
- Age
- Male > female
Presentation of gout
Acute onset (overnight usually)
Severe pain, red, hot, swollen joint
Usually monoarticular
Often affecting metatarsal phalangeal joint
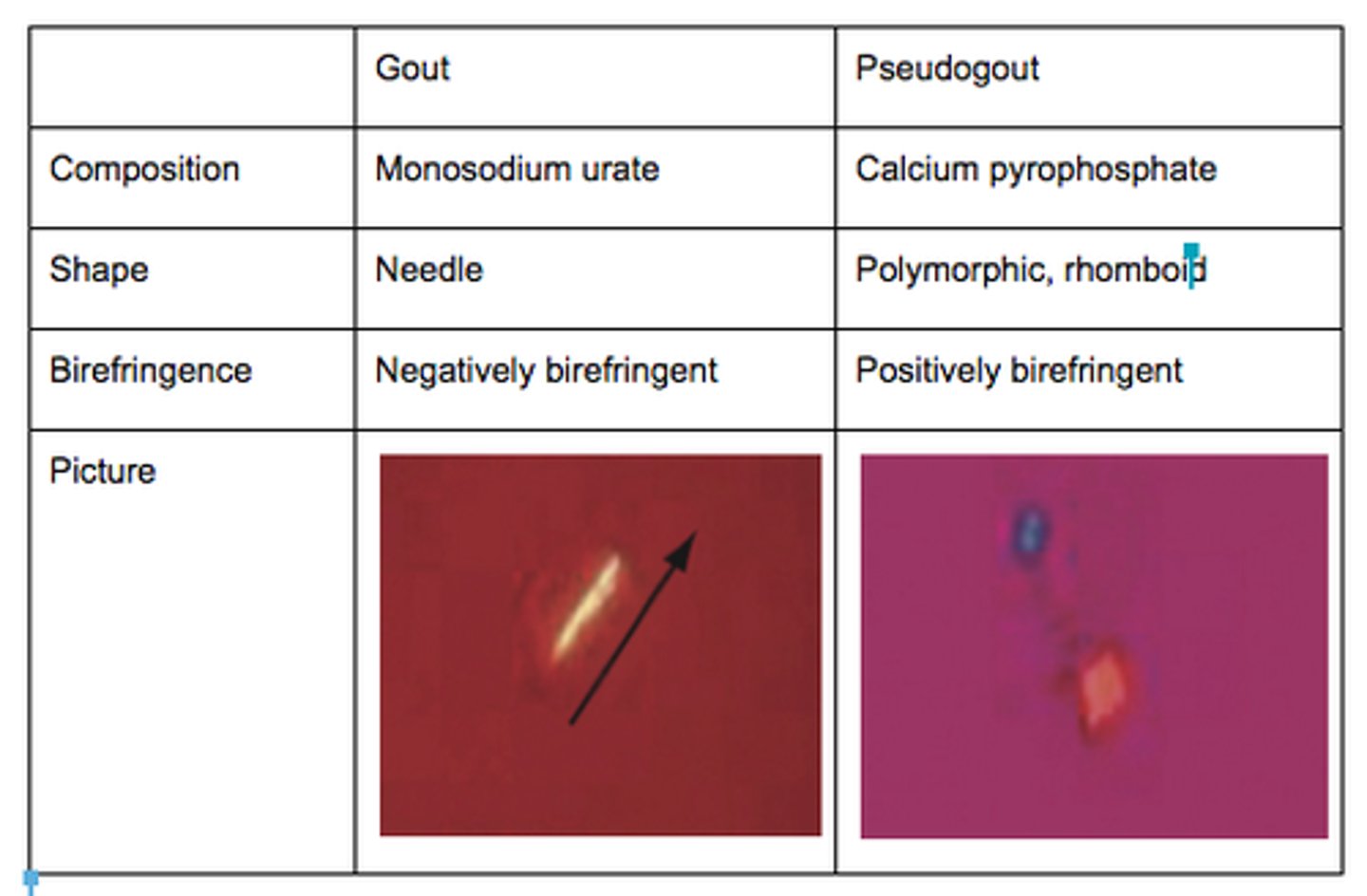
Differential diagnosis of gout
Pseudogout: deposit of calcium pyrophosphate crystals
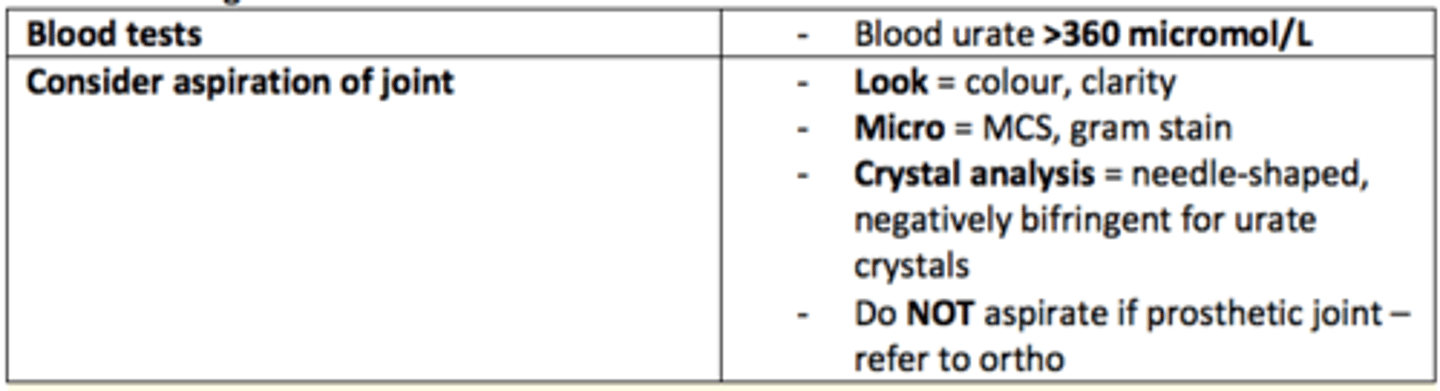
Investigations for gout
Blood tests
- Blood urate >360 micromol/L
Joint aspiration
- MCS, gram-stain
- Crystal analysis = needle-shaped, negatively bifringent for urate crystals
- Do not aspirate if joint is prosthetic (refer to ortho)
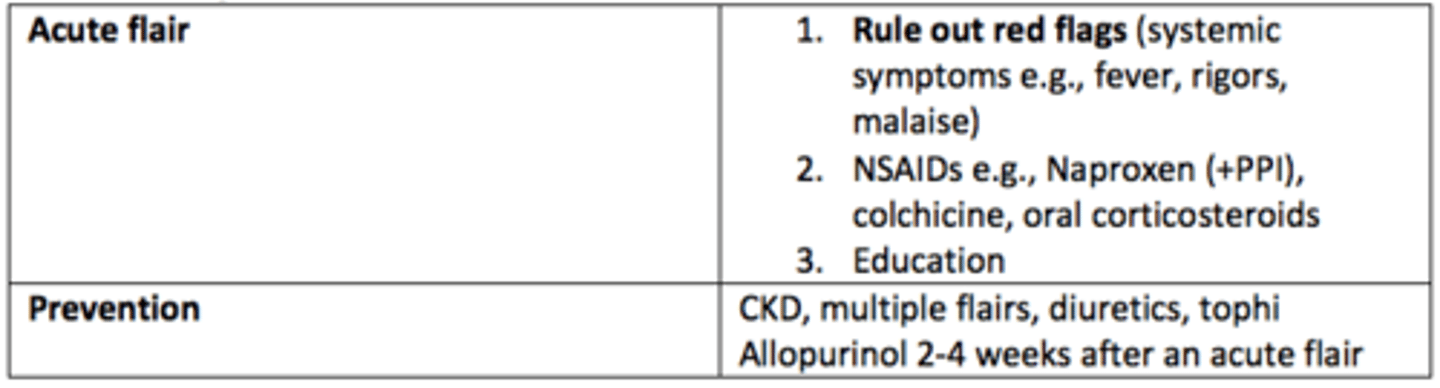
Management of gout
- Medications to help excrete uric acid
- Ice on area
- No weight bearing
- NSAIDs e.g., Naproxen (+PPI) colchicine, oral corticosteroids
- Education
- Low purine (protein) diet and increased fluids
Septic arthritis
Inflammation of the joint caused by infection
Name some causes of septic arthritis in neonates
S. aureus
N. Gonorrhoea
Group B Strep
Name some causes of septic arthritis in children
S. aureus
Name some causes of septic arthritis in adults
S. aureus
N. Gonorrhoeae
S. Pneumoniae
Pseudomonas (trauma/puncture wounds)
Salmonella in sickle cell
Pathophysiology of septic arthritis
Irreversible joint damage within 6 hours
Organism releases chondrocyte proteases
Host inflammatory response
Medical emergency
Risk factors of septic arthritis
Abnormal joint: OA, RA, prosthetic joint, Gout
Age > 80
DM
IV drug abuse, alcoholism
Intra-articular glucocorticoid injections
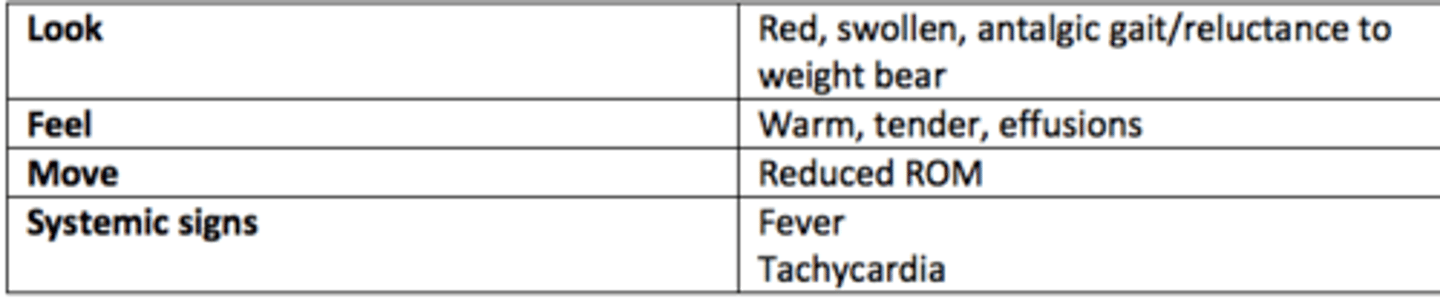
Presentation (Hx) of septic arthritis
Acute onset
Monoarticular (knee = adults, hip in children)
Pain, swollen, red, warm joint
Systemic symptoms = fever, rigors, myalgia and malaise
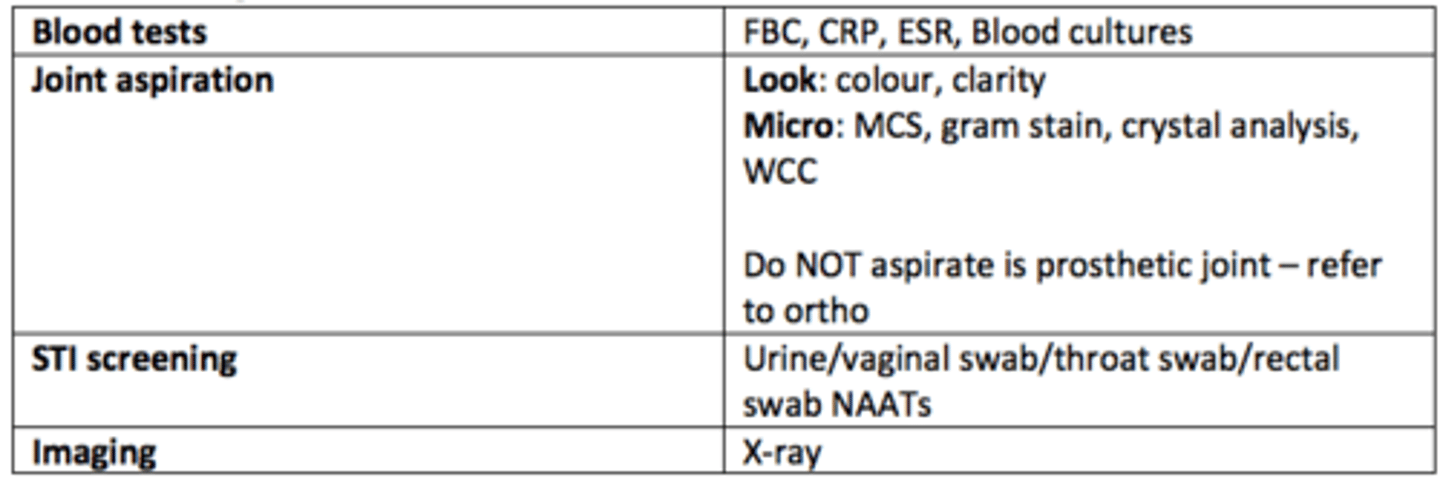
Investigations for septic arthritis
Blood tests
FBC, CRP, ESR, blood cultures
Micro: MCS, gram stain, crystal analysis, WCC
STI screening
Urine/vaginal swab/throat swab/rectal swab NAATs
Imaging
X-ray
Kocher criteria
Used to distinguish septic arthritis (SA) from transient synovitis in children with hip pain
Each positive increases the likelihood of septic arthritis
- Non-weight bearing
- Temperature >38.5
- ESR >40
- WCC >12
Management of septic arthritis
Flucloxacillin + Gentamicin
Review antibiotics with culture results
4-6 weeks in total

Other differentials for arthralgia (joint pain)
Psoriatic arthritis
- Psoriasis
- Nail changes
- Enthesitis
- Dactylitis
Reactive arthritis
- Previous GI/GU infection
- Urethritis
- Conjunctivitis
Autoimmune connective tissue disorders
- SLE
- Sjogren's
Tendonitis
Inflammation of tendon
Bursitis
Inflammation of bursa from trauma, infection, crystalopathy, inflammatory arthropathies
Labral tear
Tear of the fibrocartilage glenoid labrum or the acetabular labrum from the bone