Clinical psychology
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
68 Terms
What is clinical psychology
Identifying abnormal behaviour that is problematic to the individual.
Name the 4 Ds
Deviance, distress, dysfunction, danger
Deviance
The extent to which behaviour is rare in society which may suggest a clinical problem, behaviour in the minority eg. 2 different eye colours/ left hands
Dysfunction
behaviour that interferes with the quality of a persons life and prevents “a normal lifestyle” eg. OCD, severe anxiety that stops you going out
Distress
Extent to which behaviour is upsetting for the individual eg. Hypochondriasis consisting of the severe fear of having a serious disease
Danger
Danger to themselves/others to the extent intervention is required eg. Self harm/ smoking nicotine -second hand smoke is dangerous to others
The 5th D
Duration -if some behavioir is short term it can’t really be considered a psychological disorder eg. Getting into a bar fight once and then never again
What is psychosis
Where you experience a different reality eg. Schizophrenia
Affective disorders
Mood affecters eg. Depression
Classification
The act of classing things into groups
Diagnosis
The recognition and identification of a disease/conditions by its signs or symptoms
The two classification systems
The DSM-V (5) - stands for the diagnostic and statistical manual of mental disorders published by the American psychiatric association
ICD- Internstional classification system of diseases used globally covering all disorders and psychological illnesses
What is abnormal?
Behaviours and psychological functions considered different from the normal behaviour in any given society. This is relative to culture
Features of schizophrenia
Global prevalence is 1%
Immigrants are more likely to suffer
Onset is earlier in males (early 20s) than females (late 20s)
Positive symptoms tend to improve over time but negative symptoms often remain
Females make up more late onset cases (40+ years)
Schizophrenia symptoms (positive)
Those which add something non schizophrenic people don’t have eg. Hallucinations/delusions/disordered thoughts
Schizophrenia symptoms (negative)
Not being able to do things that normal people can do often appearing in the pro from al period (years before diagnosis) eg. Showing apathy, lack of energy, socially withdrawn, not responding appropriately in social situations
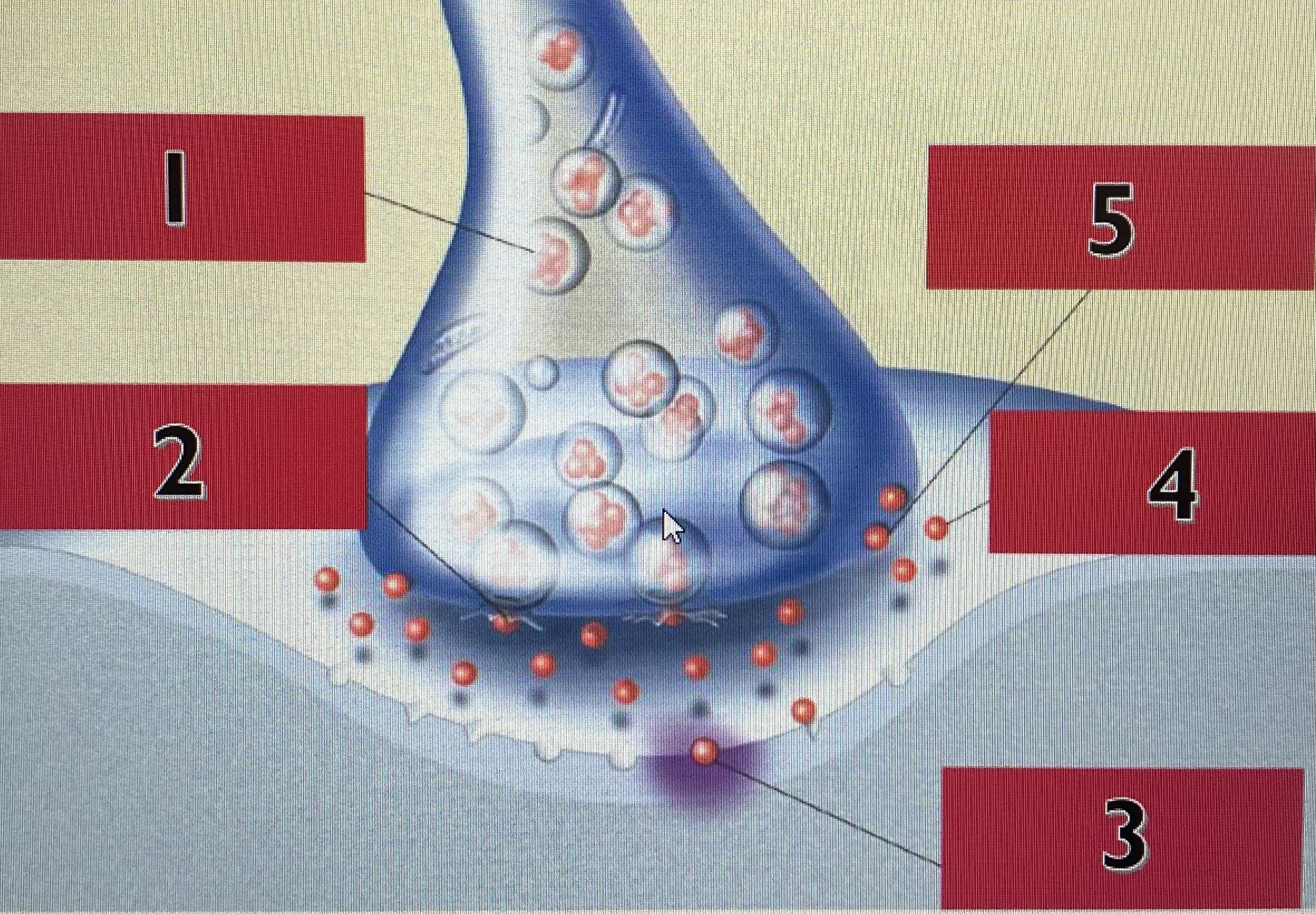
1- Synthesis and storage of neurotransmitter molecules in synaptic vesicles
2- release of neurotransmitter molecules into synaptic cleft
3- binding of neurotransmitters at receptor sites on post synaptic membrane
4- inactivation (by enzymes) or removal (drifting away) of neurotransmitters
5- reuptake of neurotransmitters sponged uo by the presynaptic neuron
The dopamine hypothesis/explanation A01
The dopamine hypothesis theorises that too much dopamine known as hyperdopaminergia or too little known as hypodominergia in the brain can cause development of schizophrenia. Too much is associated with positive symptoms eg hallucinations and has been linked to the mesolimbic pathway. Too little is related to negative symptoms like social withdrawal associated with the mesocortical pathway. Dopamine dysregulation may also be observed in the striatum.
The dopamine hypothesis A03
S- Tenn et al 2003 showed amphetamine induced rats show schizophrenic like symptoms such as erratic movement and social withdrawal, and found dopamine antagonists were shown to reverse these behaviours in the rats
C- Dépatie and Lal 2001 found that apomorphine (a dopamine agonist which stimulates D2 receptors) doesnt induce psychosis symptoms in non psychotic patients and doesn’t worsen symptoms in those with schizophrenia
O- Genetic hypothesis/ social causation
U- biological explanations have lead to the development of modern anti-psychotics which have fewer unpleasant side effects and allow people with schizophrenia to live fairly normal lives in the community rather than being institutionalised.
T-yes brsin scanning with advanced medical equipment that produce biological data that’s objective and accurate.
COMPT gene
Codes for the COMPT enzyme involved in metabolizing various catecholamine neurotransmitters including dopamine and epinephrine, a mutation or absence would result in neurotransmitter dysregulation
DISC1 gene
Stands for Disrupted in schizophrenia 1 - those with an abnormality in this gene are 1.4 times more likely to develop schizophrenia than the rest of the population. DISC1 codes for GABA which regulates glutamate and dopamine in the limbic system
NRGI gene
(Stands for neuregulin) and ErbB4 defects have also been associated with increased risk of schizophrenia both of these genes code for protein and if mutated are disruptive to both developing and mature individuals
The Genetic hypothesis A01
This explanation assumes that patients have inherited an increased inclination to a disorder, researched by utilising twins and adopted children to establish a concordance rate to signify genetic influence. Monozygotic twins are at increased risk compared to dizygotic twins to develop the disorder if the other twin has received a diagnosis m suggesting genetic inheritance is a primary factor triggered by environmental factors. Other genes such as COMT, DISC1 and Neuregulin have been associated with risk of developing symptoms eg those with a mutation of DISC1 are 1.4 times more likely to develop schizophrenia.
The genetic hypothesis A03
S- Tienari et al 1994
C- Veling et al 2008 who theorised that an environmental affect on immigrants specifically was a main influence for schizophrenia
O- Dopamine hypothesis, Glutamate hypothesis
U- through genetic testing you could find out how likely offspring could have schizophrenia and decide not to have children
T- genetic testing much more accessible
The diathesis stress model A01
Proposes that schizophrenia is caused by a genetic vulnerability oaired with environmental and psychosocial stresses. Family studies suggest that people have varying levels of inherited genetic vulnerability from very low to very high to schizophrenia
Environmental stressors included in the diathesis stress model
Prenatal trauma, childhood sexual/physical abuse, family conflict, significant life changes
Evidence for the diathesis stress model
Tienari et al 1994 used a sample of 172 Finnish women diagnosed with schizophrenia with a child adopted before the age of 4, adoptive families were rated as healthy, mildly disturbed or severely disturbed, children in healthy adoptive homes didnt develop schizophrenia, 9% did in mildly disturbed and 11% did in severely disturbed suggesting a well adjusted family environment protects children who would otherwise be predisposed and at risk of the illness.
Social causation
The opposite of biological ideas referring to social factors including using cannabis, gender, stress, malnutrition
What is social adversity
Challenging or unfavourable social conditions tho at negatively impact individuals eg poverty, discrimination, social exclusion
Social drift
People with schizophrenia find it hard stay in education/hold down a job which leads them to drift into a lower social class than their parents and as a result they migrate to deprived inner-city areas
Evidence: Goldberg and Morrison 1963 found that schizophrenic sons were found to be much more likely to be lower class than their fathers
Social causation theory
This theory suggests environmental factors are a reason why some people are at an increased risk of psychosis. Factors including social adversity (being deprived of basic needs like nutrition/shelter) have been shown to make people more vulnerable to all kinds of mental health disorders including schizophrenia. Urbanisation has been linked to much higher vulnerability to psychosis as it increases stressors like noise/overcrowding in urbanised environments. Migration status as well has implications due to perceived discrimination
Social causation A03
S- Veling et al 2008
C- Goldberg and Morrison 1963 where they showed social drift is the consequence not the cause of schizophrenia
O- dopamine, genetic, glutamate
U- highlights factors that people can change in their life such as housing projects to reduce overcrowding and inclusivity with regard to immigration
T- social research is correlational so cannot directly manipulate these variables
The glutamate hypothesis A01
Developed by Carlson followed a meta-analysis of studies investigating neurotransmitter function in a psychosis context. He suggested that the dopamine hypothesis was over simplistic and instead highlighted the role of glutamate in the presence of psychotic symptoms. PCP or angel dust has been found to deplete glutamate while increasing dopamine and psycho stimulation yet receptors of glutamate were able to override the psychostimulant effects of PCP even with dopamine excess suggesting dopamine can’t be the sole cause of psychotic behaviour.
The glutamate hypothesis A03
S- is more holistic view as it works with the dopamine hypothesis and expands rather than replacing it. Lots of evidence from neuroimaging and animal studies showing that blocking glutamate relates to psychotic symptoms
C
O
U- research came from animal studies where psychostimulation may not be equal to humans
T- use of brain scanning techniques such as PET scans is invalid because the human brain may behave differently to in an everyday situation so the glutamate activity measured may not reflect what the schizophrenic brain characteristically does
Typical antipsychotics example
Clorpomazine- not effective for negative symptoms and unpleasant side effects such as facial and body tics,
Effect at the synaptic level- blocks postsynaptic dopamine receptors without activating them which reduces positive symptoms of schizophrenia
Atypical antipsychotics example
Clozapine- a dopamine serotonin and glutamate antagonist that reduces positive and negative symptoms, side effects include agranulocytosis (fatal blood condition)
A03 evaluation of antipsychotics
S- Emsley 2008 found 84% of patients on antipsychotics had at least 50% reduction in symptoms if they were given it early enough
C- Rosa et al 2005 found only 50% of patients complied with taking their antipsychotics
O- CBT
U- allow patients to stay in society rather than become institutionalised
U- anti-psychotics have serious side effects such as decreasing motivation so schizophrenics may not be bothered to take them
A01 description of antipsychotics
They are a biological treatment that aim to change brsin chemistry. They block dopamine receptors and therefore minimise the effect of dopamine, there are multiple forms that a person can take the antipsychotics in such as tablets vs injections. Injections can be used to combat the main issue of antipsychotics which that people don’t take their meds
What is a biological treatment for schizophrenia?
Antipsychotics
What is a psychological treatment for schizophrenia
A cognitive behavioural therapy (CBT)
A01 of cognitive behavioural therapy for schizophrenia
This is a talking therapy that aims to assist people with schizophrenia by managing their symptoms and improve the patients quality of life. This relies on a good relationship of trust between the patient and therapist in order for treatments such as psycho education to be effective. Cognitive restricting techniques used include identifying automatic thoughts, identifying cognitive distortions, disputing thoughts, and replacing thoughts which teaches the patient how to handle and recognise their symptoms instead of correcting them.
A03 of cognitive behavioural therapy for schizophrenia
S- NICE 2014 study where it was found to be effective in reducing hospital readmissions and reduced time spent in hospital
C- McKenna and Kingdon 2014 disputed the efficiency after observing it was only superior to biological treatments in 2/9 trials suggesting it’s not effective for everyone
O-Drug treatments
U- useful for drug resistant clients
Features of depression
Women’s are twice as likely to experience it than men
15% of women receive treatment compared to 9% of men
Global prevalence is approximately 5%
Neuroticism is positively correlated
Classification differences in depression
DSM-V - 5+ symptoms during the same two week period, one of those must be a depressed mood/loss of interest or pleasure, must clinically cause significant distress or social impairment
ICD-10 -Symptoms should be present for a month or more with every symptom being present for most of every day, degree of depression established by how many and their severity
Symptoms of Depression
Depressed mood
Loss of pleasure/interest in activities
Changes in appetite/weight
Low energy
The monoamine hypothesis A01
Monoamines are a group of neurotransmitters that regulate mood, including serotonin, noradrenaline and dopamine. The monoamine hypothesis theorises that the disregulation of these can lead to underlying symptoms of unipolar depression particularly when serotonin levels are low. This is because these neurotransmitters have a key function in regulating the activity of the limbic system most significantly the amygdala, hypothalamus and hippocampus which are connected to the frontal areas of the brain. Low levels of noradrenaline are linked to a lack of pleasure as it regulates attention, reward, concentration and arousal.
The monoamine hypothesis A03
S
C- the monoamine hypothesis can’t explain therapeutic delay where it can take up to 6 weeks for symptoms to be alleviated
O
U- biological explanations are based on observations that antidepressants alleviate symptoms so it’s an ussumption that if a biochemical treatment improves symptoms, then the cause is biochemical
T
The BDNF hypothesis A01
Brsin derived neurotrophic factor is a chemical that “feeds” neurons and plays a role in neuroplasticity (formation of new synapses). In depressed people low levels of BDNF are low in the PFC and hippocampus correlating with severity, the lower the level the more severe the symptoms. It’s suspected the gene for BDNF may be switched off under stress which results in the neurons affected becoming atrophic (shrinking) or the cells die off altogether which both occur in depression.
The BDNF hypothesis A03
S- Martinowich et al 2007 found abnormally low levels of BDNF in the hippocampus and PFC in post-mortem examinations of depressed patients
C
O
U
T- reductionist
Cognitive distortions examples
Arbitrary inference- drawing conclusions on irrelevant evidence
Selective abstraction- focusing on small negative aspects of a situation
All or nothing thinking- ignoring any middle ground of a situation
Name biological treatments for depression
Drug therapy
ECT- electro convulsive therapy
Trans cranial magnetic stimulation
SSRIs and SNRIs
SSRIs (selective serotonin uptake inhibitors) and SNRIs (serotonin and norepinephrine inhibitors) prevent reuptake of serotonin and noradrenaline alleviating symptoms of depression after around 4 weeks
Example of SSRIs- citalopram
Example of SNRIs- atomoxetine
Evaluation of biological treatments for depression in general
Strengths- act more quickly than psychological therapies, can be used globally
Weaknesses- not everyone improves after taking drugs, common unpleasant side effects, CBT is shown to be just as effective over a course of 6 months
CBT A03 (depression)
S- no side effects and non invasive
C- not effective for severe depression and people have to be commuted which is a challenge for depressed people who lack motivación
O
U- empowers rather than pacified people aiming to change a persons thinking by giving them tools
T
Hankin et al 1998 A03
Methodology- longitudinal research
Description-same people are studied over time to look for developmental issues and patterns, can be retrospective or prospective, similar to repeated measures
Strengths- can show the side effect of time on a particular variable, eliminates participant variables
Weaknesses- sample attrition, research can become outdated quickly
Wijesundera et al 2014 A03
Methodology- Cross-sectional design
Description- used to gather information on a population at a particular point in time similar to independent groups
Strengths- obtain immediate results cost-effective
Weaknesses- participant variables -the cohort effect
Tsung et al 2013 A03
Methodology- cross cultural design
Description- taking samples of different cultures to draw comparisons about the similarities and differences between them
Strengths- can establish whether a behaviour or phenomenon is a global nature
Weaknesses- language barriers
Stafford et al 2015 A03
Methodology- meta analysis
Description- researchers examine the results of several previous studies
Strengths-lots of data can examined no direct dealings with participants -no ethical concerns, cheap and relatively easy to do
Weaknesses- secondary data
Lavarenne et al 2013 A03
Methodology- case study
Description- an individual or small group is studies as they have a particularly unique or experience
Strengths- yields lots of ecologically valid data, illuminates areas where they may be little previous research
Weaknesses- qualitative -not as easy to interpret, cant generalise or replicate so less scientific
Valentine et al 2010 A03
Methodology- interviews
Description- self report where participant is directly questioned, may be structured unstructured or semi structured
Strengths- if structured= reliable if unstructured= rich data
Weaknesses- structured = low in ecological validity
Unstructured- leading questions
Classic study -Rosenhan 1973 A01
A- to answer the question “can the insane be distinguished from the sane?” By using 8 pseudo patients including Rosenhan 3 female 5 male all with no history of mental health problems
P- a mixture if old/new mental institutions -a total of 12 which were phoned up to make an appointment due to hearing voices. They all used the words empty, thud, hollow as it had no previous connection to any mental disorder. They were all truthful about their life events and all got diagnosed with schizophrenia or psychosis. Once admitted they acted “normally” and tried to convince the staff of their sanity.
F- the average stay in the hospital was 19 days, none of the patients were detected by staff due to their normal behaviour being pathologised yet were detected by other patients. Out of 1283 attempts to approach staff 80% were ignored, 10% made eye contact and 2% stopped to chat.
C- It is not possible to distinguish the same from the insane in psychiatric hospitals
Classic study -Rosenhan 1973 A03
G- lots of data collected over 12 hospitals rated as old/new and good/bad which gives the target population -the psychiatrists an inside so yes good generalisability
R- it was a covert observation which lacks control, but is naturalistic. Standardised by the same 3 words of thud hollow and empty
A- lead to widespread critisism of the system and practice was changed as a result
V- lacks internal because it was covert but has good external because it was naturalistic
E- The participants (the hospital staff) were observed without consent, were deceived and didn’t have a right to withdraw.
SPECT scan
single photon emission computed tomography
Contemporary study for schizophrenia A01 -Carlsson et al 2000
A- to provide up to date review on the dopamine hypothesis while exploring the role of glutamate in relation to psychosis to provide suggestions for future drug treatments
P- a review of studies using PET scans. These are an imaging technique produced by using a radioactive tracer that dissolves in the blood stream and concentrates around particularly active brain structures, until recently the dopamine hypothesis was only supported by indirect evidence such as metabolite levels in cerebrospinal fluid.
F- low levels of glutamate were linked to both positive and negative schizophrenic symptoms where carlsson located this activity in the striatum and in the cerebral cortex. The striatum is the brains reward center so abnormal activity there leads to positive symptoms and low glutamate activity in NMDA receptors in the cerebral cortex explains negative symptoms.
C- lack of glutamate might cause patients to have an exaggerated response to dopamine at the post-synapse, even though only normal levels of dopamine are being produced, the dopamine receptors have an extreme reaction.
Contemporary study for schizophrenia A03 -Carlsson et al 2000
G-
R-
A-
V-
E-
Contemporary study for depression A01 Kroenke et al 2008
A- To investigate whether the PHQ 8 accurately predicts the items on the quality of life measures, and the algorithm calculation and scores agreed with each other
P- A telephone survey of 198,678 people living in America with the sample being 61.6 women with over half being white, college educated, currently married and currently employed
F- Depressed respondents were more likely female, non white, less educated, unemployed or unable to work. They were more likely to report lifetime diagnoses of both depression and anxiety, characteristics of the depressed grouos were quite similar between the two methods of defining depressions as well as the non depressed groups.
Using the 10 and above cut off was as successful in measuring depression and those scoring below 10 had no diagnosis of depression
C- compared to other measures the PHQ yields similar prevalence rates and depression is a highly prevalent disorder in the US population
Contemporary study for depression A03 Kroenke et al 2008
G- Huge sample carried out in 38/50 US states including big cities and rural areas which is representative, yet was only conducted in the US and could have only included people who were in a phone book and was an opportunity sample as they had to have picked up the phone at the right time
R- Questionnaires with closed questions are reliable because every participant gets same questions in same order and they’re marked in the same way, but there could have been researcher effects as people may not want to reveal health problems to a stranger rather than fill in the PHQ themselves
A- Shows that the PHQ can be used to initially diagnose depression through a telephone interview/online diagnosis and helps identify people who should go to a doctor for more thorough diagnosis using DSM-5 leading to people getting earlier diagnosis and more effective treatment for depression
V- the similarity in results between the DSM based PHQ algorithm and the PHQ cut point suggests it’s a valid tool for measuring depression
E- the researchers were specially trained in their job to avoid causing offence or distress with their questions and the 9th question on suicide was dropped from the survey as if a respondent had admitted to being suicidal the researcher couldn’t have helped
Clinical practical
A- To investigate how different sources represent mental health by using written media such as the sun, the guardian and the mirror
H1- There will be more negative portrayals if mental health than positive
H0- There will be no significant difference in how positively mental health is portrayed
P- we used summative content analysis looking at key words relating to attitudes of mental health between the 20-21st august 2015. Key words were listed and counted in each newspaper as well as a separate list containing the concept of the words
F- 4 negative keywords found compared to 6 positive keywords, this could’ve been because there were only 6 articles coving the subject, yet there were 2 incidents in a mental health hospital not reported so the validity is compromised as it could be more focused on how often it’s portrayed rather than just how
Evaluation
S-interprets qualitative into quantitative so it’s easier to analyse, good reliability because there was no social desirability due to no one knowing the experiment took place.
W- only 3 newspapers chosen so less generalisable and the sample was done leading up to a general election meaning most news stories would be focused on that.