21-22 Exam 2 Rebecca Effler SUMMERTIME
1/176
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
177 Terms
3 functions of the lymphoid system
1. fluid recovery- fluid continually filters from the blood capillaries into the tissue spaces
2. immune surveillance
3. lipid absorption- lacteals in small intestine absorb dietary lipids that are not absorbed by the blood capillaries for processing in the liver
Describe the sizes of the lymphatic vessels
1. Lymphatic Capillaries: Smallest vessels (microscopic), have thin, overlapping endothelial walls
2. Collecting vessels: larger than capillaries; contain valves similar to veins to prevent back flow
3. Lymphatic trunks and ducts: largest vessel, drain into the venous system
(thoracic duct is the largest)
Drainage of right lymphatic ducts
Receives lymph from right arm, right side of head and thorax; empties into right subclavian vein
Drainage of thoracic duct
Drain the rest of the body; then delivers it into the left subclavian vein; starts at cysterna chyli
What is the recovery rate of interstitial fluid into the lymphatic system?
Lymphatic capillaries collect 15-20% of fluid that was not reabsorbed into the blood capillaries
Which tonsils are usually removed and why?
Pair of palatine tonsils at posterior margin of oral cavity. Tonsillitis occurs here
Forces involved in lymph flow
-Skeletal muscle contractions
-Respiratory pump: changes in thoracic pressure during breathing
-Valves: preventing back flow
-Smooth muscle contractions: in the walls of larger lymphatic vessels
What are perforins? What cells release them? When are they released?
-Are proteins that create pores in the membrane of target (infected or cancerous) cells to kill them
-Released by: cytotoxic cells and natural killer (NK) cells
-When released: Upon recognition of infected, foreign, or abnormal cells
Define pathogen
Agents capable of producing disease, including viruses, bacteria, fungi, and other microbes
What are lacteals? Where are they located? What is the primary function?
-Specialized lymphatic capillaries
-Location: villi of small intestine
-Function: Absorb dietary lipids and fat-soluble vitamins. Especially a fatty molecule called "chylomicrons" which are too large to be collected by blood capillaries. The presence of these lipids causes the lymph draining the small intestine to appear creamy white instead of clear and referred to as "chyle"
Identify the 1st line of defense
-Physical barriers: skin and mucous membranes
-Chemical barriers: tears, saliva, stomach acid, antimicrobial peptides
Identify the 2nd line of defense
-Protections against pathogens that break the skin
-Leukocytes and macrophages
-Antimicrobial proteins
-Natural killer cells
-Fever
-Inflammation
Lymphatic/Immune Functions: Thymus
-Houses developing T cells (T lymphocyte) and secretes hormones regulating their activity
-Help maturing T cells become self-tolerant of the body's own antigens
-Most active in childhood and shrinks with age
-By age 65 unable to make new T cells
-This leaves older people vulnerable to infections, cancer
Lymphatic/Immune Functions: Spleen
-Filters blood, removing old or damaged RBCs and platelets, and acts as a storage site for these cells
-Stabilizes blood volume through plasma transfers to lymphoid system
-Known as "erythrocyte graveyard"
-Red pulp—sinuses filled with erythrocytes
-White pulp—lymphocytes, macrophages surrounding small branches of splenic artery
Lymphatic/Immune Functions: Red bone marrow
-Involved in hematopoiesis (blood formation) and immunity
-B cells mature here
-Produced the formed elements (including all white blood cells)
-As blood cells mature, they push their way through the reticular and endothelial cells to enter the sinus and flow away in the bloodstream
-All immune cells are born here
Lymphatic/Immune Functions: Lymph node
-Filters lymph, house of B and T lymphocytes and macrophages, activate the immune response when pathogens are detected
Fever Regulation: with cells, secretions, structures involved
-Pyrexia
-Triggered by: trauma, infections, drug reactions, Brin tumors, and etc.
-Cells involved: macrophages and other leukocytes
-Target structure: hypothalamus: when the body detects an infection, it releases pyrogens that act on the hypothalamus, the body's temperature control center, to raise the thermostat
Result: vasoconstriction (chills), shivering, elevated body temperature
Cardinal signs of inflammation
redness, swelling, heat, pain, loss of function
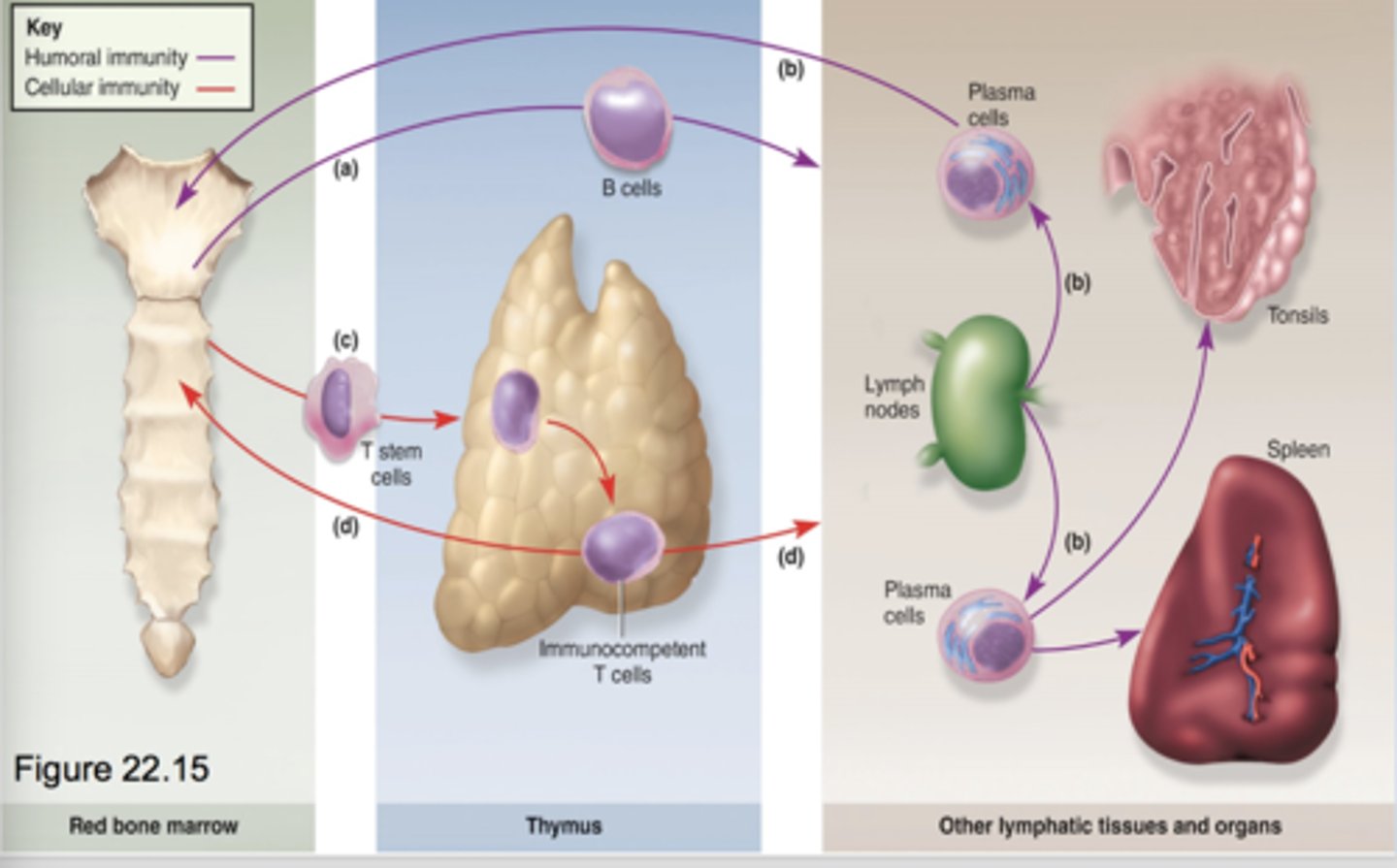
The Life History and Migrations of B and T Cells
-T cells and B cells are born in redbone marrow
-Capable of recognizing antigens presented to them
-Tested and will not attack self-cells
-B CELLS: humoral immunity (antibodies), immunocompetent after leaving bone
-T CELLS: cellular immunity (cells attack), immunocompetent after leaving thymus
What are interferons? What cells secrete interferons? When are interferons secreted?
-Antiviral proteins that inhibit viral replication; recruit and activate macrophages
-Secreted by: virus-infected cells and immune cells (T cells, NK cells, IFN-v)
-When: early in a viral infection
Difference between adaptive and innate immunity
-Innate: immediate (min to hours), non-specific, no memory, 1st and 2nd line of defense
EX: skin, mucous membranes, NK cells, phagocytes, fever
-Adaptive: delayed (days to develop), highly specific to particular antigens, systemic effect, has memory, third line of dense
EX: T cells, B cells, antibodies
Identify the cells capable of making antibodies? How do antibodies assist the immune response?
-B cells, specifically plasma cells
-By binding to and neutralizing pathogens or marking them for destruction by other immune cells
Type 1 allergic reaction
-Triggered by: allergen (pollen, peanuts, dust mites)
-Allergens bind to IgE on the membranes of basophils and mast cells
-Causing a release of histamine and other inflammatory and vasoactive chemicals
-Signs: local edema, mucus hyper secretion and congestion, watery eyes, runny nose, etc.
-Anaphylaxis: immediate, severe case
What is pus?
yellow accumulation of dead neutrophils, bacteria, cellular debris, and tissue fluid
Immune Function of Neutrophils
-Wander in connective tissue killing bacteria
Can ensnare bacteria by releasing a extracellular trap (NET)—web of nuclear chromatin and proteins
-Can kill by phagocytizing and digesting microbe, or by release of bactericidal chemicals to create killing zone
Immune Function of Eosinophils
-Found especially in mucous membranes
-Guard against large parasites: tapeworms, roundworms
-Participate in inflammation
-React to allergens and participate in allergic reactions
Immune Function of Basophils
-Secrete chemicals that aid mobility and action of other leukocytes -Leukotrienes: activate and attract neutrophils and eosinophils
-Histamine: a vasodilator; increases blood flow and speeds delivery of leukocytes to the area
-Heparin: inhibits clot formation that would impede leukocyte mobility
Immune Function of Lymphocytes
-Includes T cells and B cells, which participate in adaptive immunity
-Also includes natural killer (NK) cells, part of innate immunity
-Destroys infectious/cancerous cells
Immune function of Monocytes
-Emigrate from the blood into connective tissues and transform into macrophages
-Macrophage system—all the body’s avidly phagocytic cells, except leukocytes; includes monocytes, macrophages, dendritic cells, and others
-Some macrophages are wandering cells; others are fixed in place (microglia)
How do helper T cells work in cellular and humoral immunity?
Cellular: release cytotoxic T cells and macrophages via cytokines
Humoral: activate B cells to produce antibodies
What are the antigen presenting cells?
B- Lymphocytes cells, macrophages, and dendritic cells
Describe similarities between Cytotoxic T cells and NK cells?
-Both destroy abnormal cells
-Both release perforin and granzymes to kill
-Both found in red bone marrow
-Both have cytokine production
Signs and causes of anaphylaxis
-Causes: food allergens (ex. peanuts, shellfish), insect stings, medication (ex. penicillin), latex or other allergens
-Signs: hives, itching, flushing, swelling of throat, wheezing, difficulty breathing, low blood pressure, rapid/weak pulse
-Severe cases: anaphylactic shock
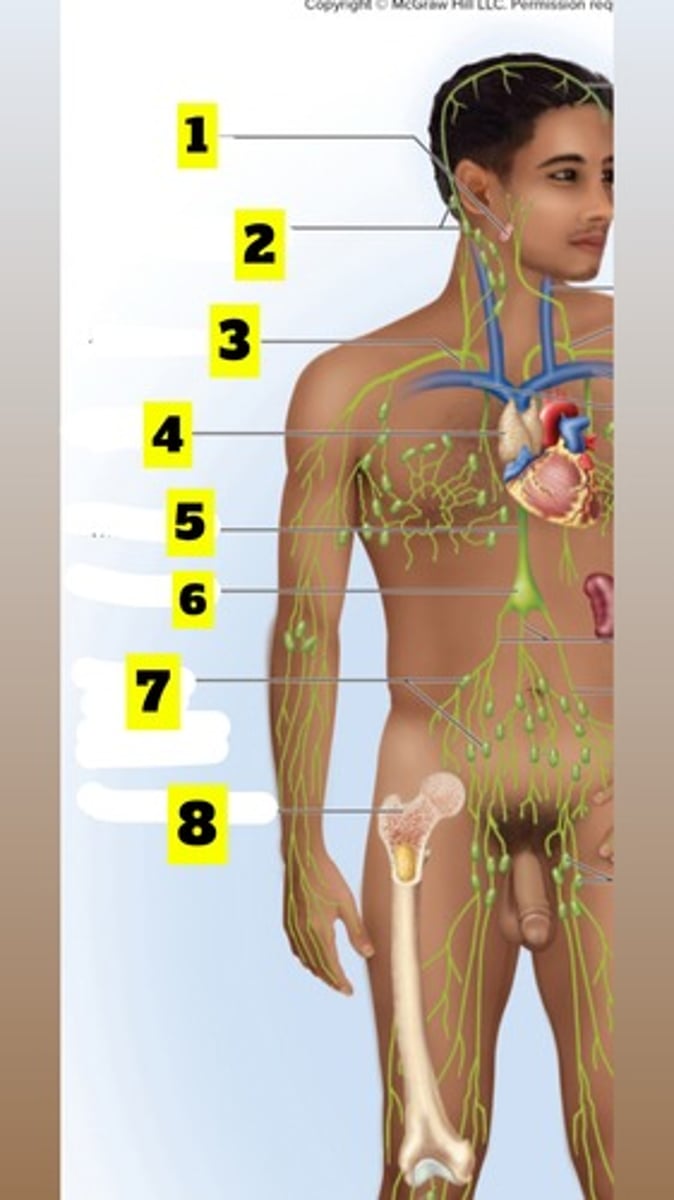
What is number 1? (figure 21.1)
Palatine tonsils
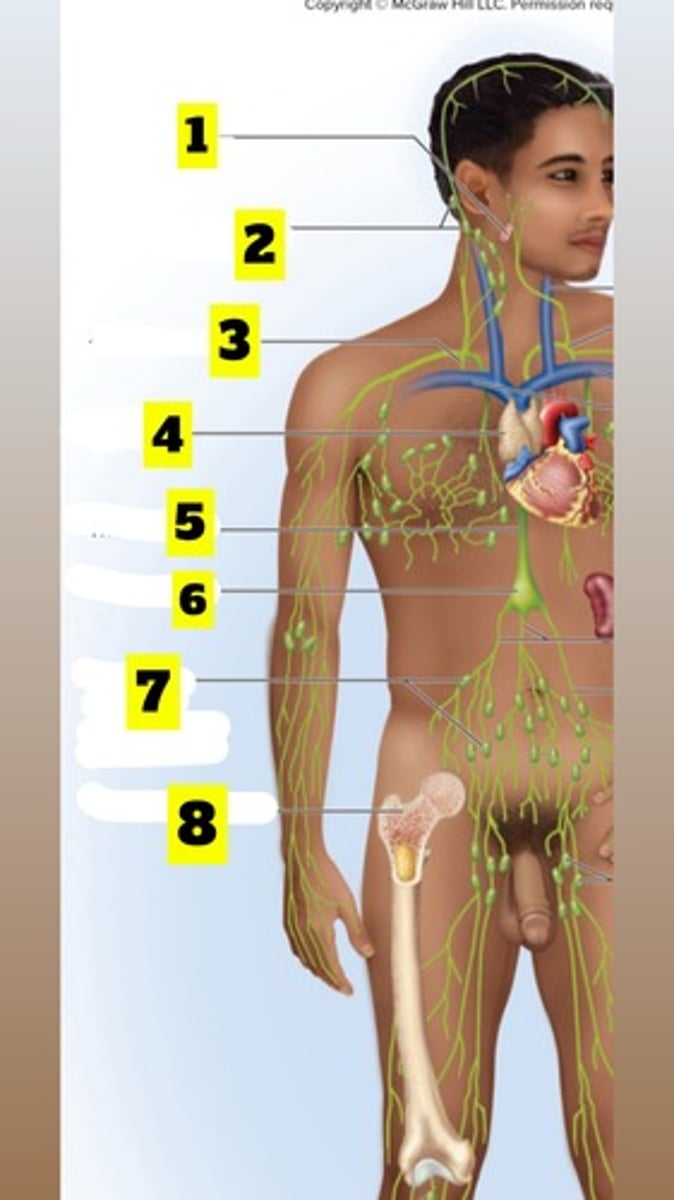
What is number 2? (figure 21.1)
Cervical lymph nodes
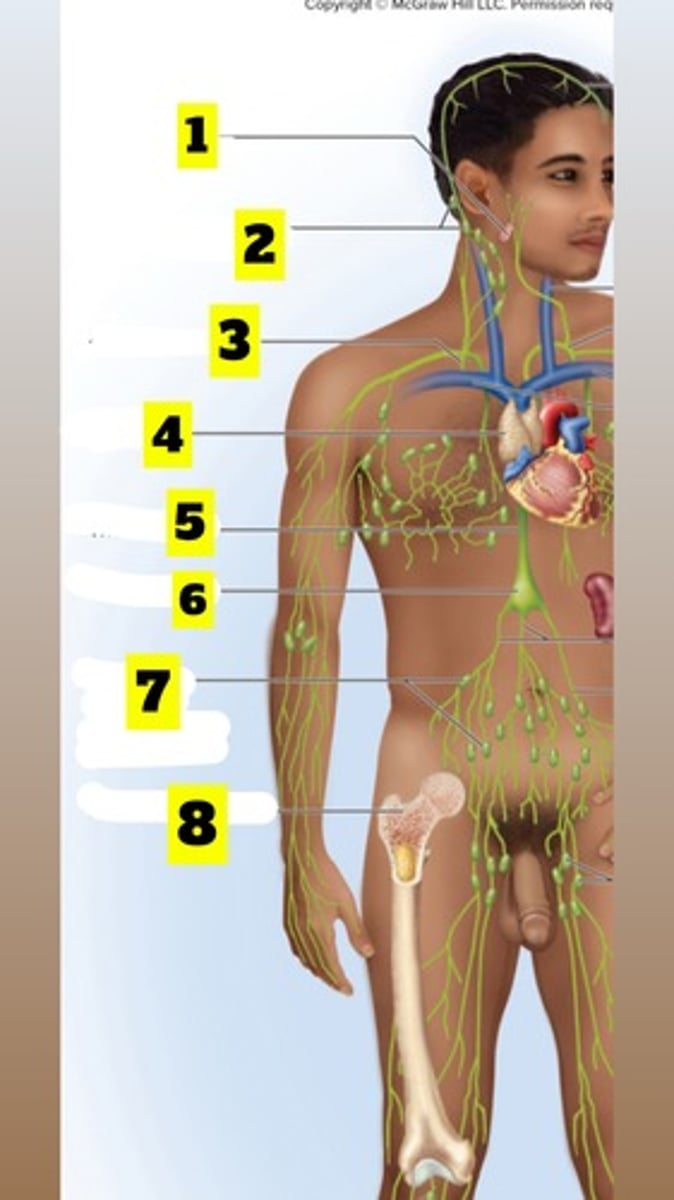
What is number 3? (figure 21.1)
Right lymphatic duct
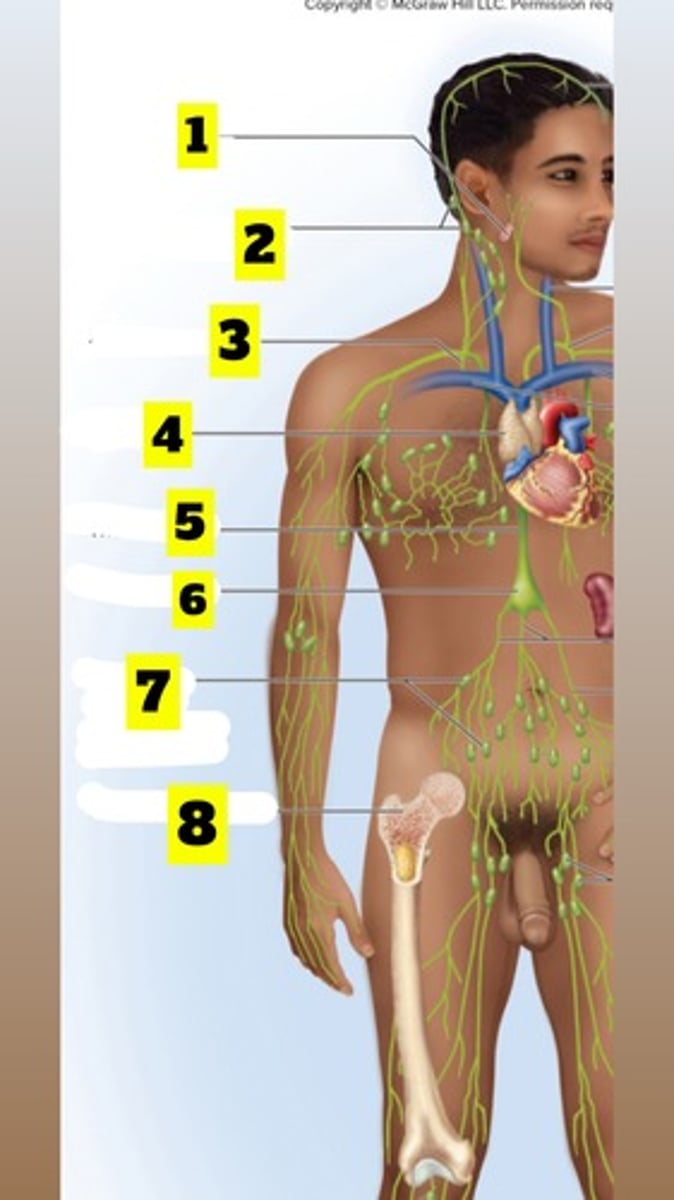
What is number 4? (figure 21.1)
Thymus
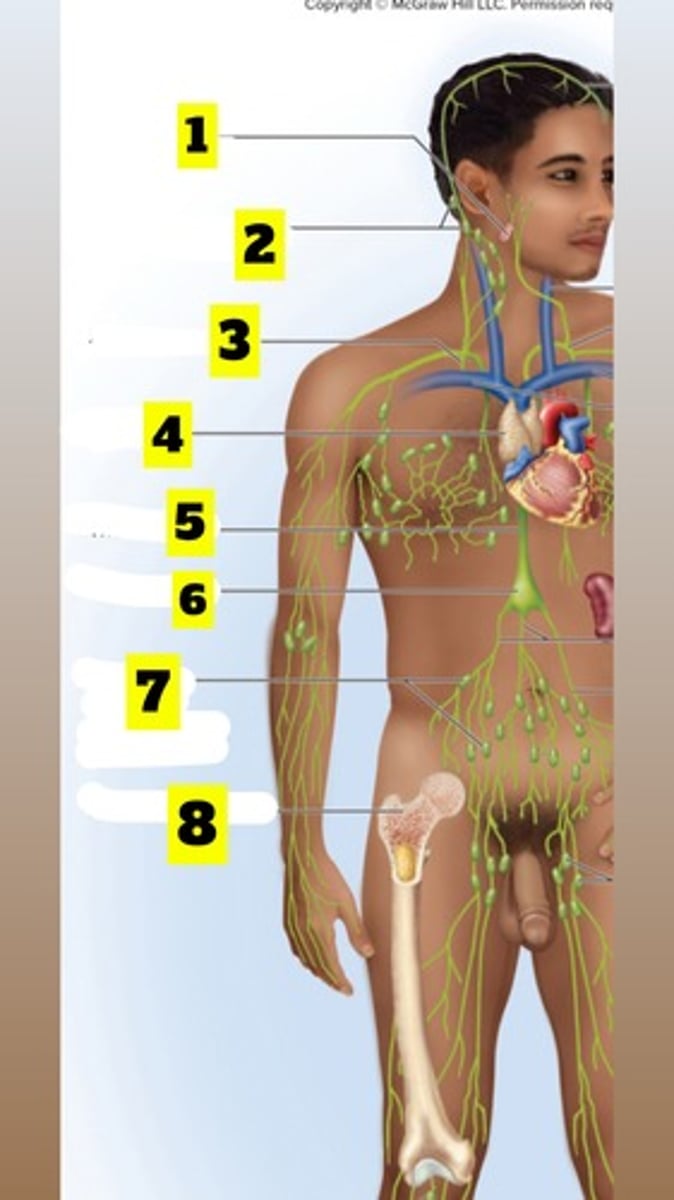
What is number 5? (figure 21.1)
Thoracic duct
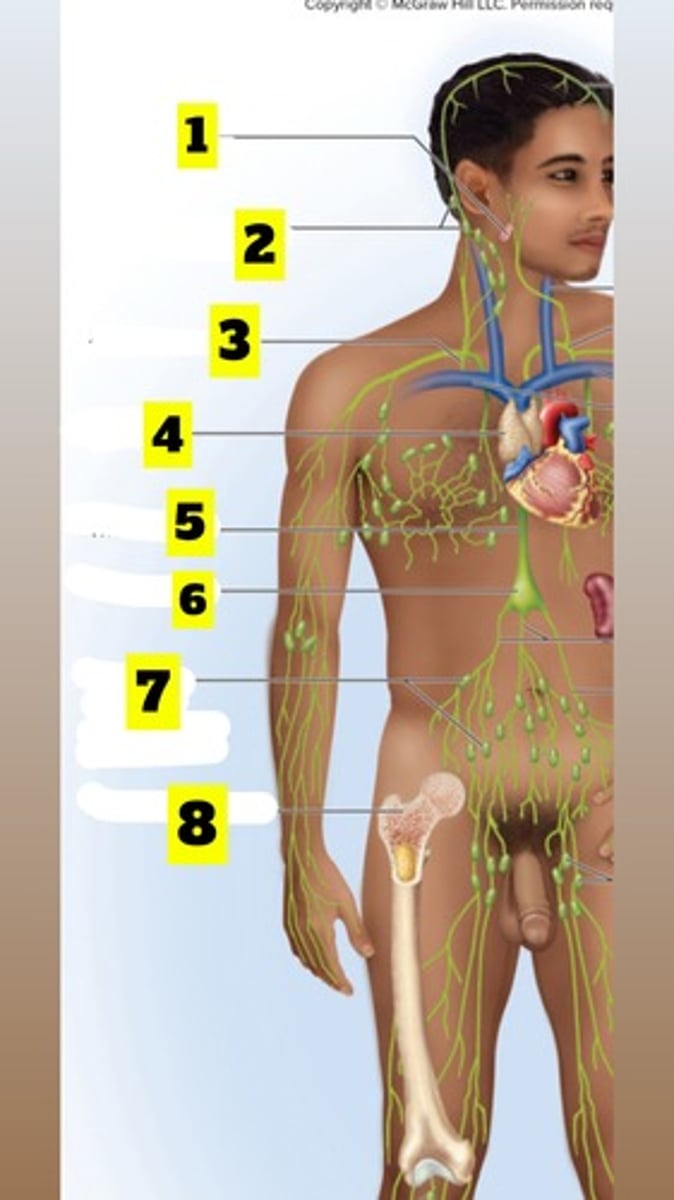
What is number 6? (figure 21.1)
Cisterna chyli
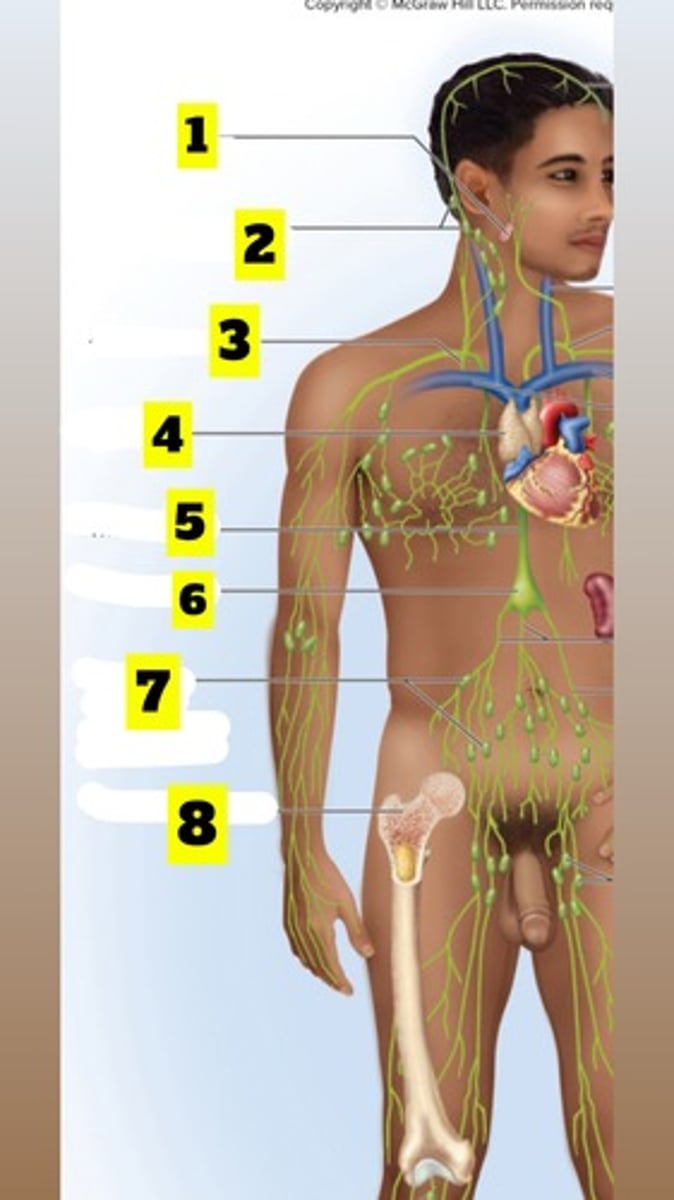
What is number 7? (figure 21.2)
Abdominal, intestinal and mesenteric lymph nodes
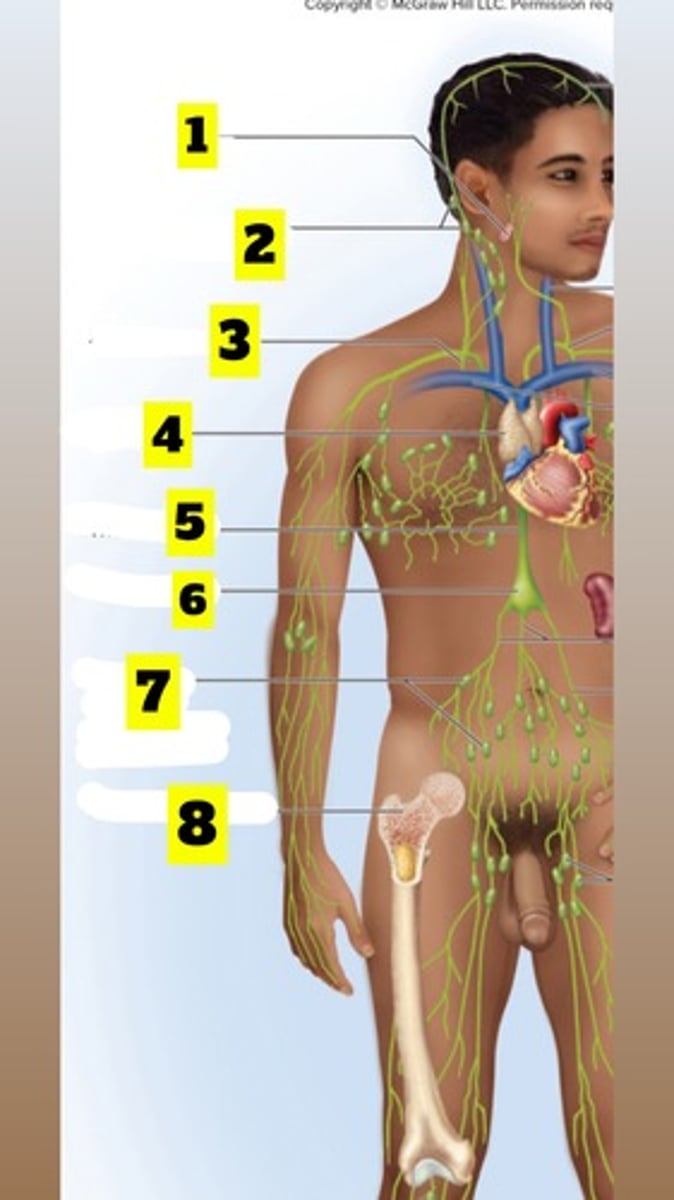
What is number 8? (figure 21.1)
Red bone marrow
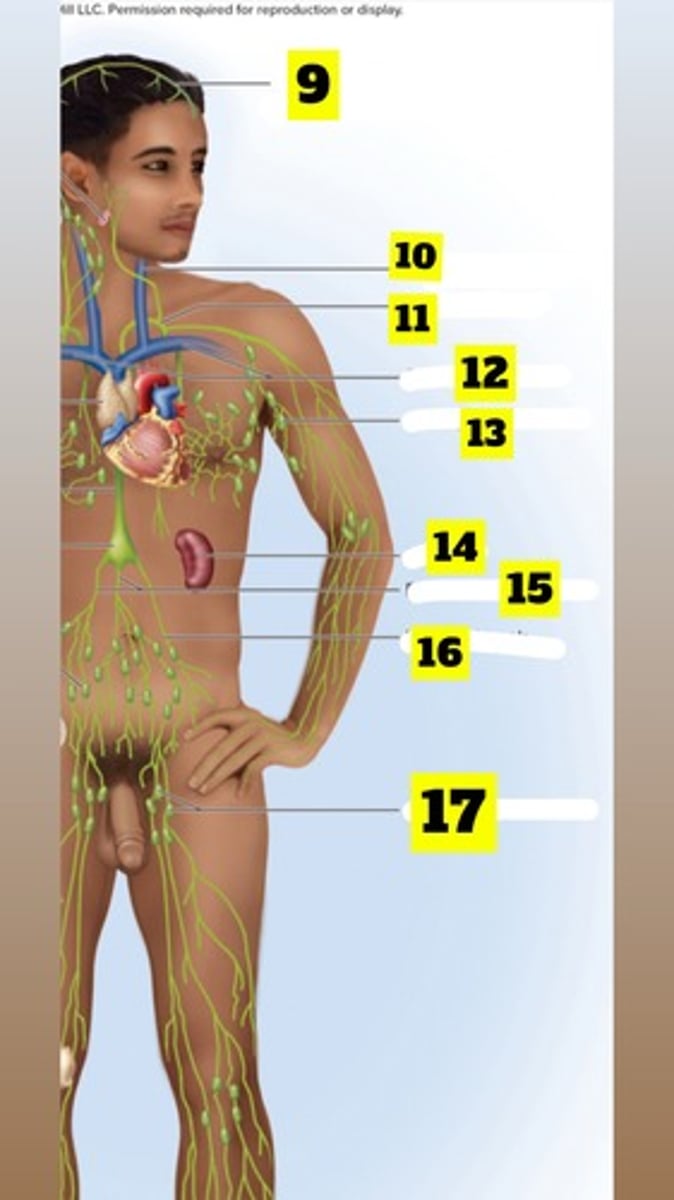
What is number 9? (figure 21.1)
Meningeal lymphatic vessels
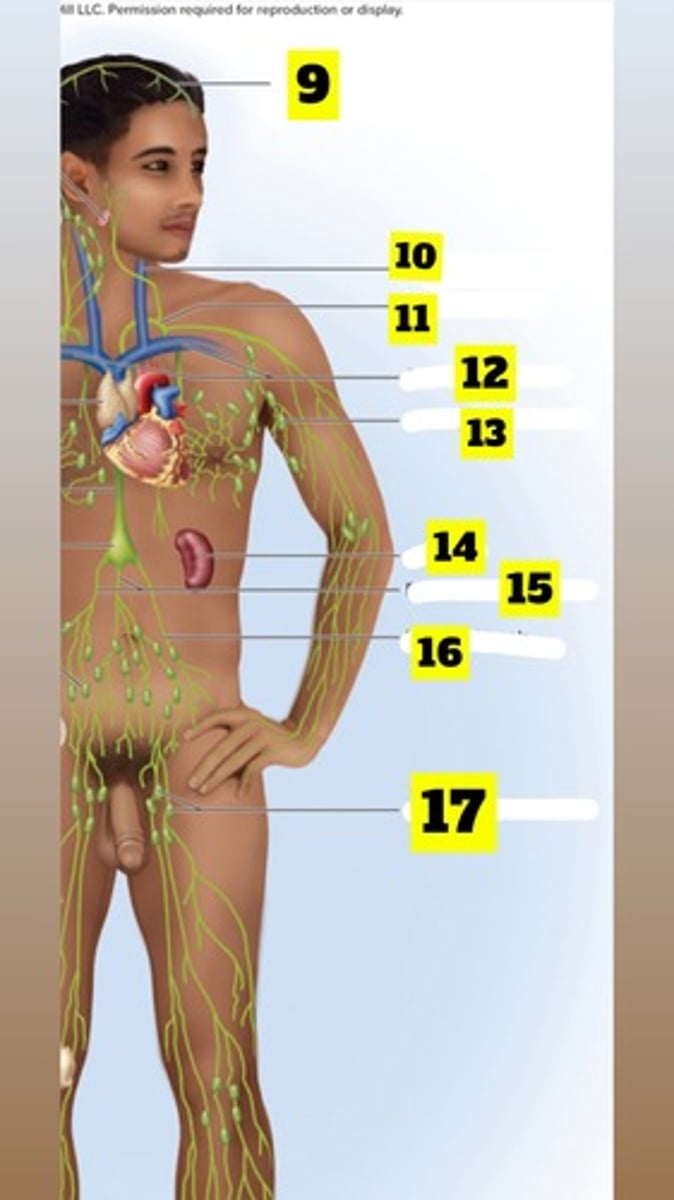
What is number 10? (figure 21.1)
Left internal jugular vein
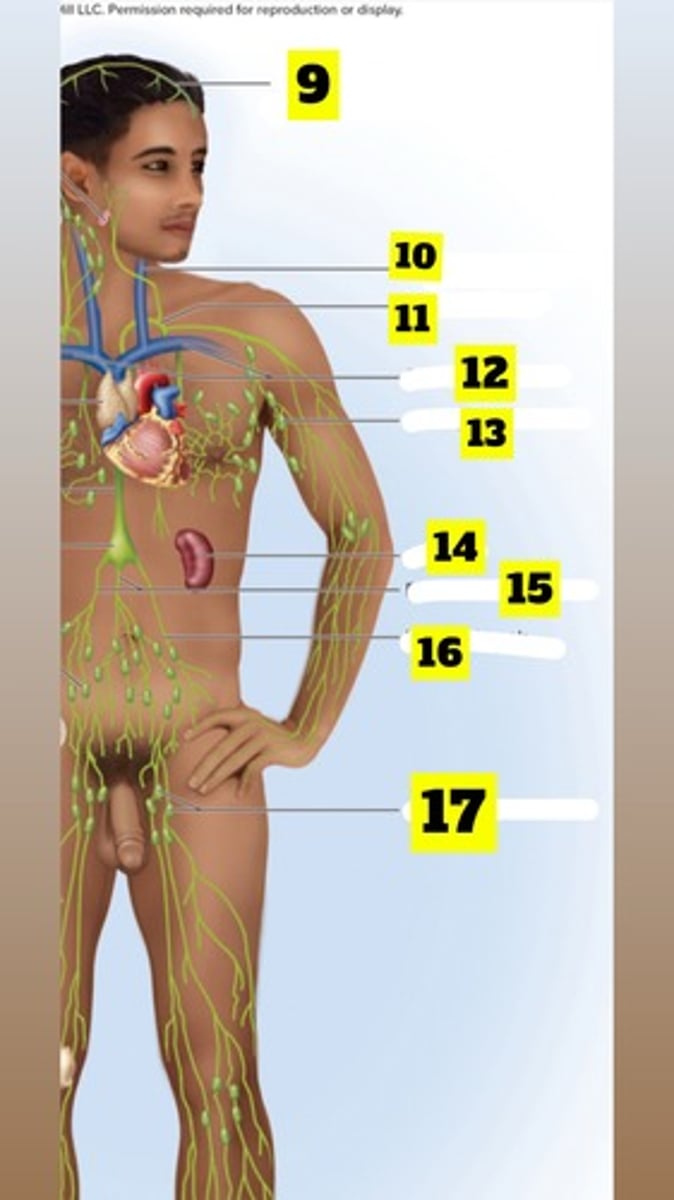
What is number 11? (figure 21.1)
Thoracic duct
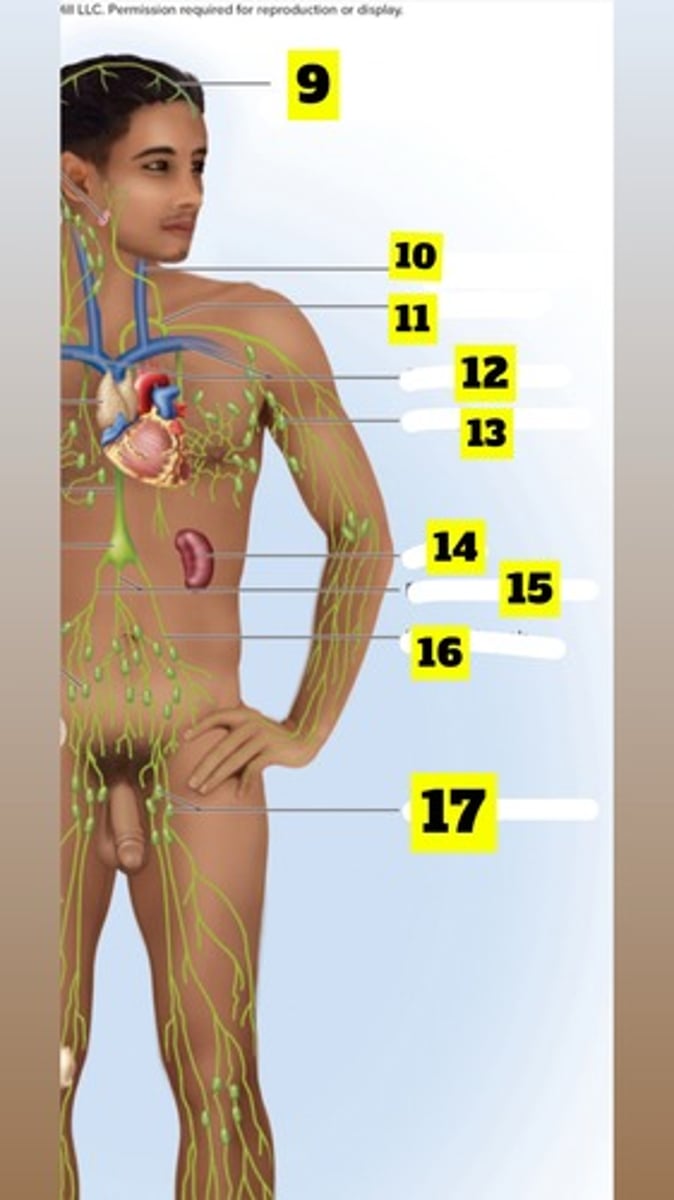
What is number 12? (figure 21.1)
Subclavian veins
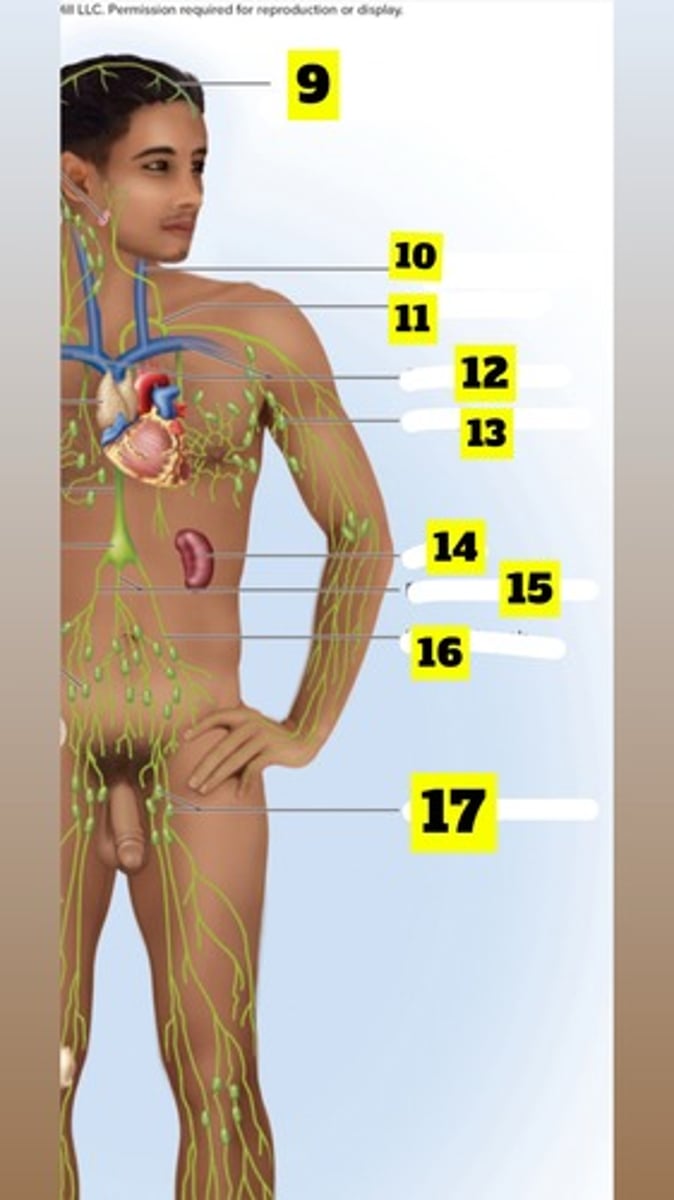
What is number 13? (figure 21.1)
Axillary lymph node
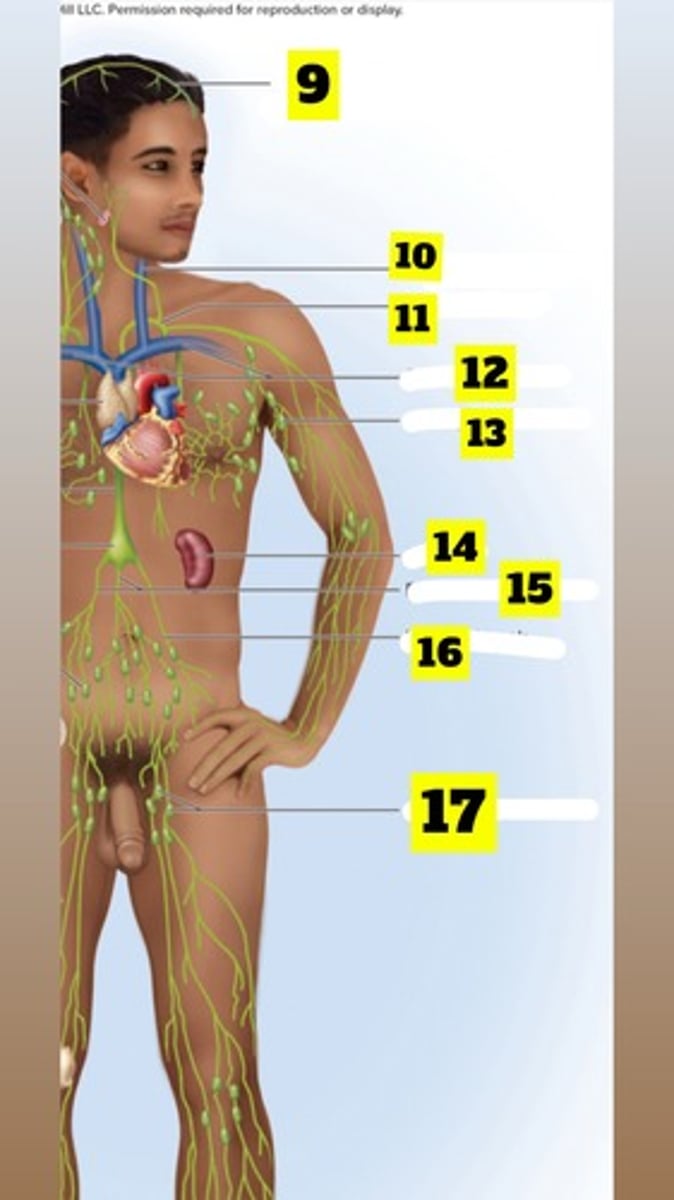
What is number 14? (figure 21.1)
Spleen
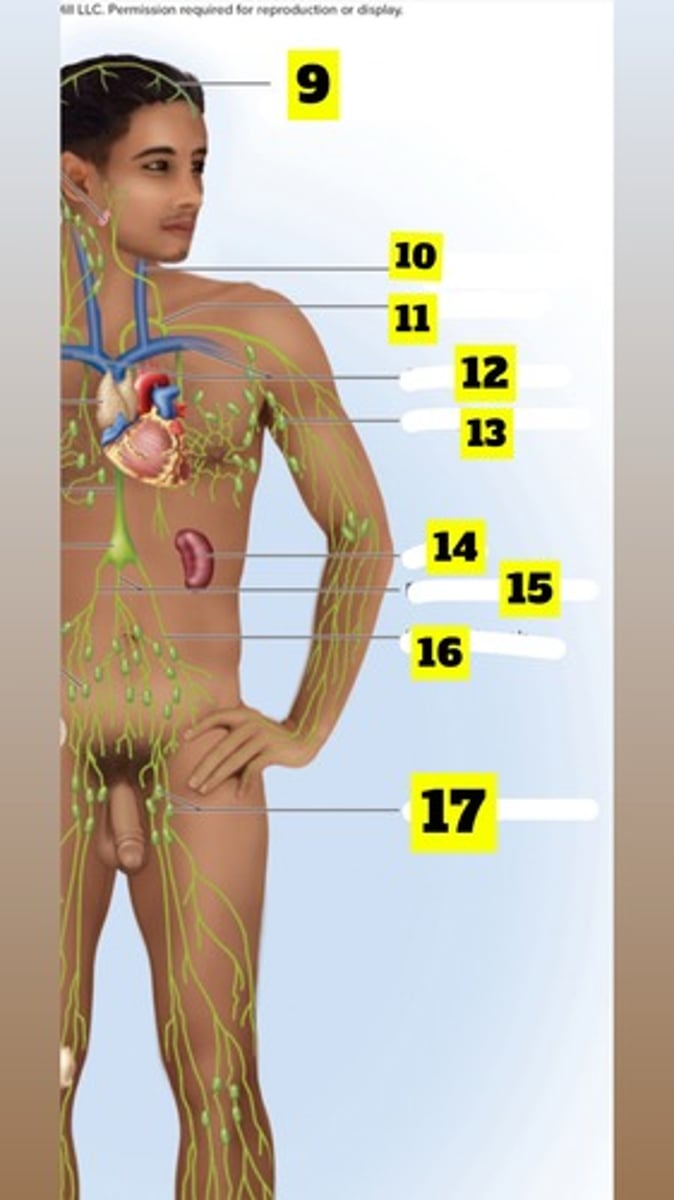
What is number 15? (figure 21.1)
Right and left lumbar trunks
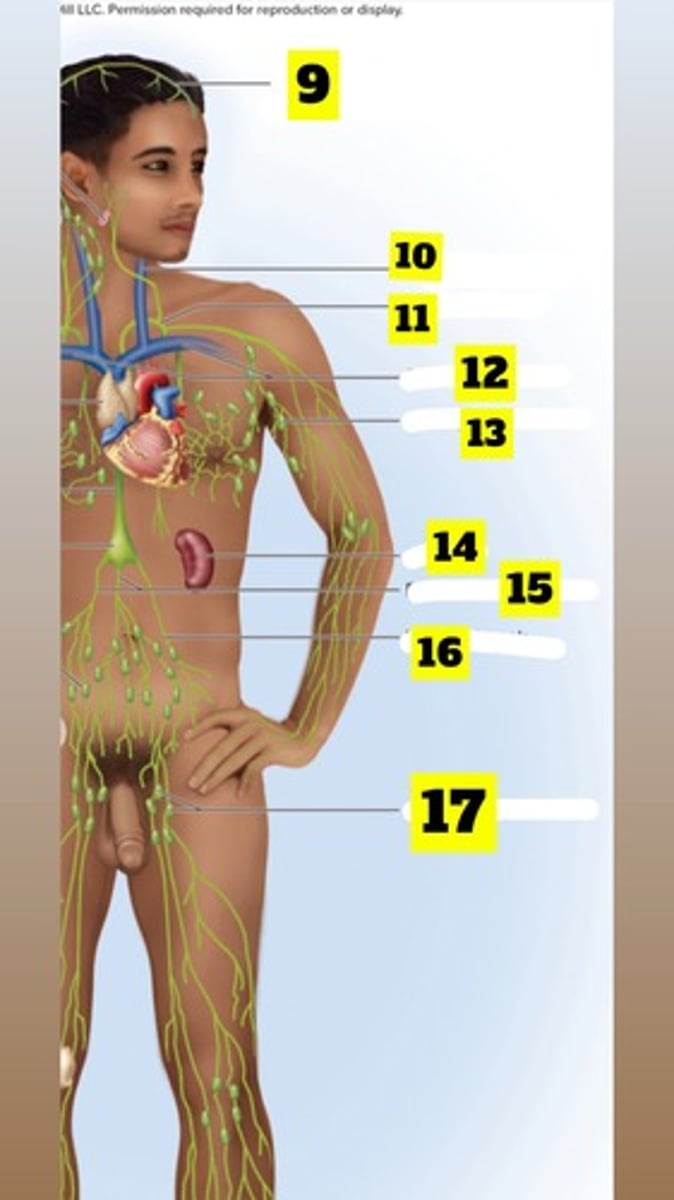
What is number 16? (figure 21.1)
Intestinal trunk
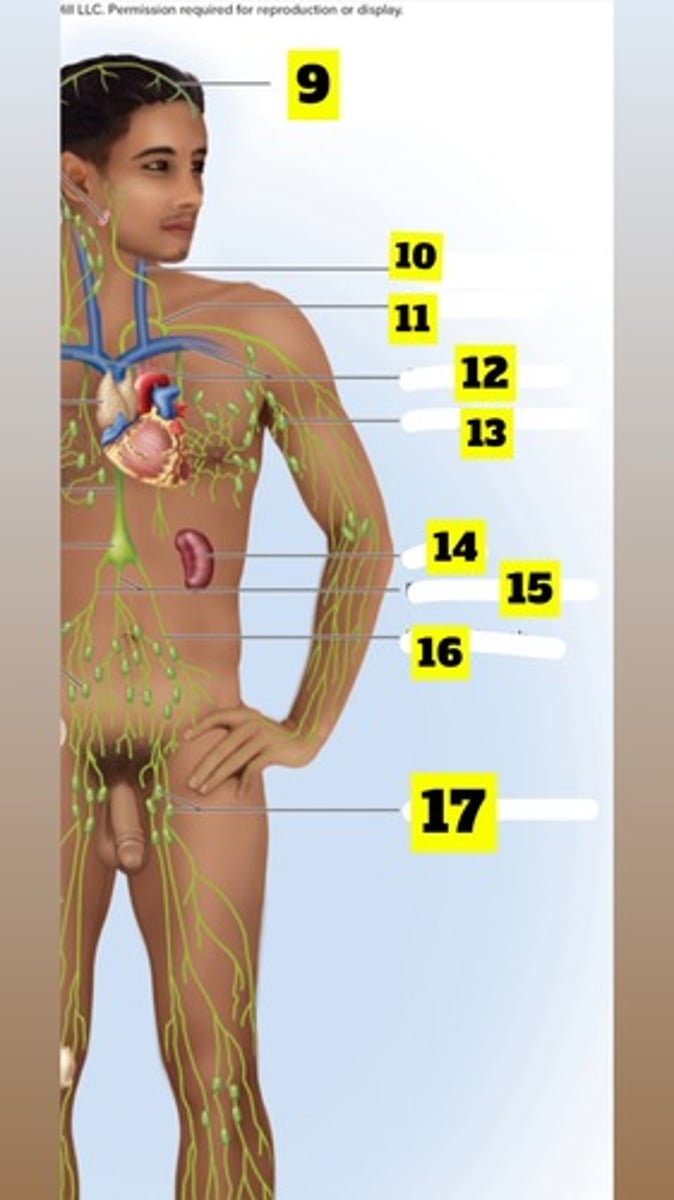
What is number 17? (figure 21.1)
Inguinal lymph nodes
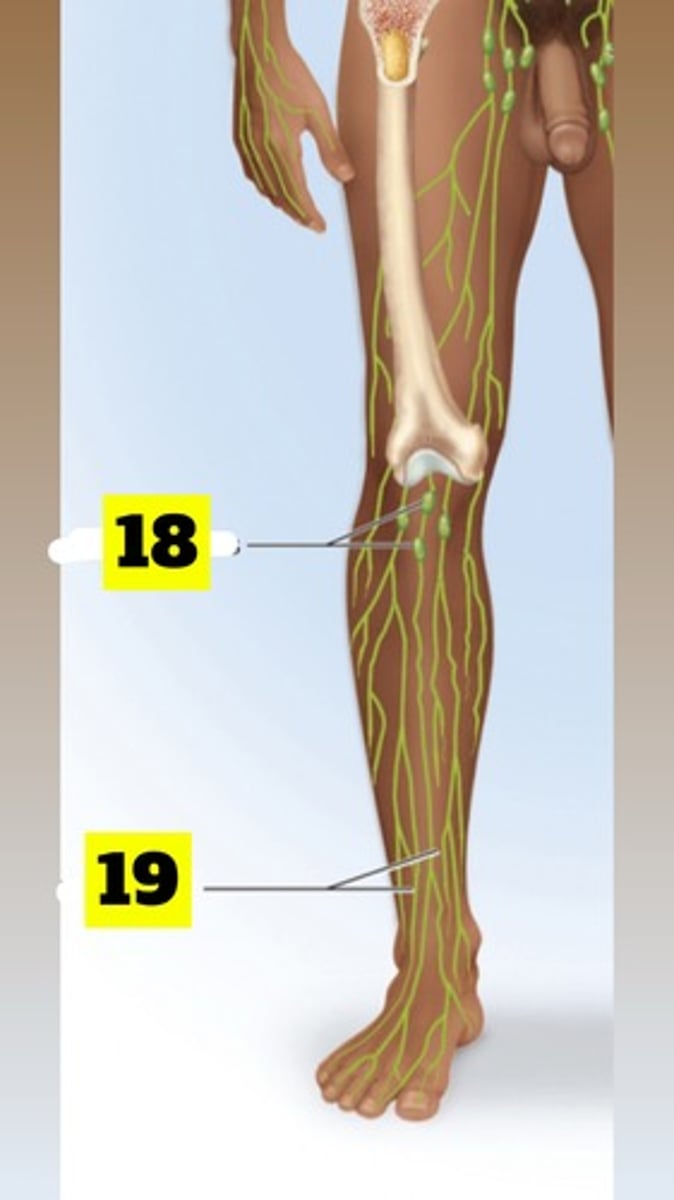
What is number 18? (figure 21.1)
Popliteal lymph nodes
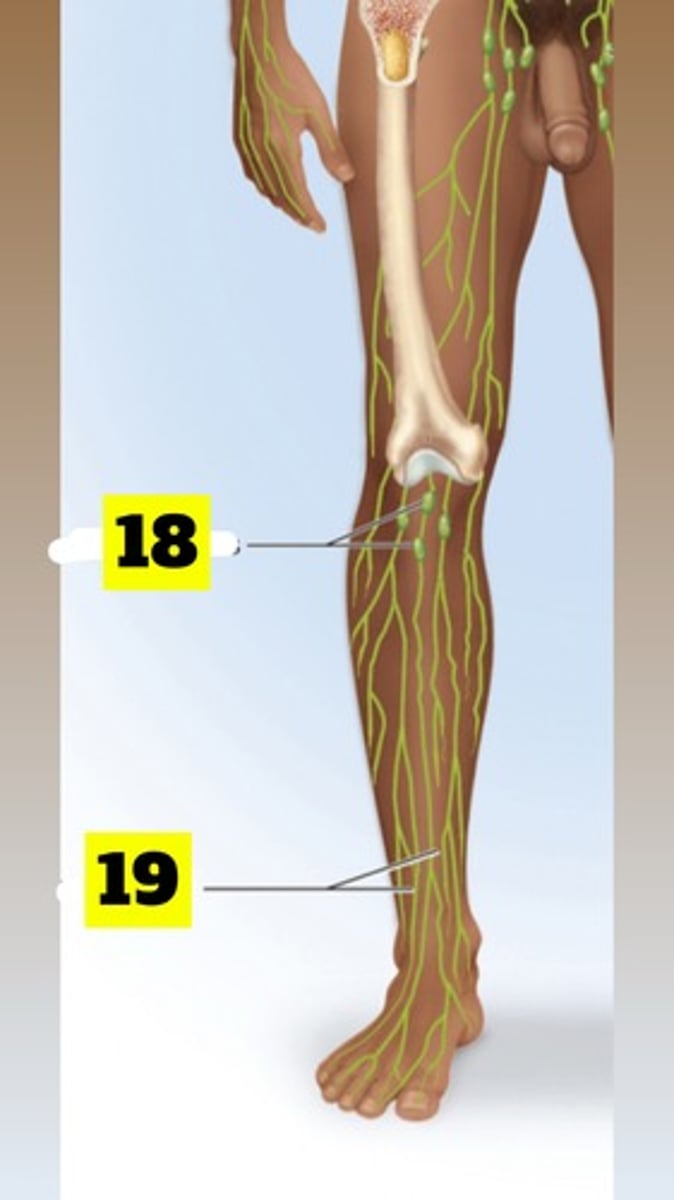
What is number 19? (figure 21.1)
Lymphatic vessels
Principal organs of the respiratory system:
nose, pharynx, larynx, trachea, bronchi, lungs
Respiration
Refers to ventilation of the lungs (breathing)
Gas exchange
-O2 and CO2 exchanged between blood and air
-External (pulmonary) respiration- exchange of gases between air and blood (alveoli)
-Internal (tissue) respiration- blood and tissue fluid (systemic gas exchange)
Charles Law
-The volume of a gas is directly proportional to its absolute temperature
-On a cool day, 16°C (60°F) air will increase its temperature by 21°C(39°F) during inspiration
-Inhaled air is warmed to 37°C (99°F) by the time it reaches the alveoli
-Inhaled volume of 500 mL will expand to 536 mL
Pharynx
(throat) muscular funnel extending from nose to larynx, assist in swallowing and speech
Nasopharynx
-Airflow
-Receives auditory tubes• Mucosa traps airborne pathogensnear pharyngeal tonsil
Oropharynx
-Airflow and digestion
-Space between soft palate and epiglottis
-Contains palatine and lingual tonsils
Laryngopharynx
-Airflow and digestion
-Posterior to larynx, from epiglottis to cricoid cartilage
-Esophagus begins at that point
Larynx
-Keeps food and drink out of airway
-Superior opening is guarded by the epiglottis
-When swallowing the larynx moves up and tonged pushes epiglottis down to meet larynx
-Directs food to esophagus
-"Voice box"
The Larynx is made of 9 cartilages (these are the most important!!!)
1. Epiglottic cartilage—supportive plate in epiglottis (elastic cartilage)
2. Thyroid cartilage—shield-shaped, largest laryngeal cartilage; contains laryngeal prominence (Adam’s apple), testosterone stimulates growth, larger in males
3. Cricoid cartilage—ring-like shape; connects larynx to trachea Thyroid and Cricoid make of the “voice box”
4. Arytenoid cartilages—posterior to thyroid cartilage
5. Corniculate cartilages—attached to arytenoid cartilages like a pair of little horns
Arytenoid and Corniculate areimportant for speech
Trachea (windpipe)
-Rigid tube 4.5 in. long and 1 in. in diameter
-Supported by 16 to 20 C-shaped rings of hyaline cartilage—prevent collapse during inhalation
Carina of Trachea
-Lowermost tracheal cartilage
-Point at which the trachea divides into bronchi
The Trachea Histology
-Lined by ciliated, pseudostratified columnar epithelium
-Contains mucus-secreting cells, ciliated cells
-Mucociliary escalator—mechanism for debris removal
-Mucus traps inhaled particles, upward beating cilia moves mucus to pharynx to be swallowed
Tracheotomy
-To make a temporary opening in the trachea and insert a tube to allow airflow
-Prevents asphyxiation due to upper airway obstruction• --Potential problems include:
1. Inhaled air bypasses the nasal cavity and is hot humidified
2. If left for long, will dry out mucous membranes
3. Become encrusted and interfere with clearance of mucus from tract, there by promoting infection
Intubation
when a patient is on a ventilator, air is introduced directly into trachea (can be mouth or nose)
The Trachea branches into
right and left primary bronchi at the carina
Respiratory zone
-Regions that participate in gas exchange
-Alveoli and nearby structures
The nose and nasal sinus
warms, cleanses, and humidifies inhaled air; detects odors; and serves as a resonating chamber that amplifies voice
Conducting zone
-Passages that serve only for airflow (no gas exchange)
-Nostrils through major bronchioles
Right main bronchus
-Is wider and more vertical than left main bronchus
-Aspirated (inhaled) foreign objects lodge in the right main bronchusmore often than in the left
The primary bronchus divided into a
secondary Bronchus lobe of the lung
Upper respiratory tract
airway from nose through larynx
Lower respiratory tract
regions from trachea through lungs
Right lung has 3 lobes
superior, middle, inferior
Right lung is shorter
Because of the liver
Left lung has 2 lobes
superior and inferior
Left lung is narrower
due to the tilt of the heart
Bronchioles
continuations of airway that lack supportive cartilage and are 1 mm or less in diameter
Pulmonary lobule
-Portion of lung ventilated by one bronchiole
-Each bronchiole divides into terminal bronchioles (80)
-Each terminal gives off two or more smaller respiratory bronchioles
-Each respiratory bronchiole have alveoli
Alveoli
beginning of the respiratory zone (gas exchange)
Simple squamous alveolar cell
layer (rapid gasexchange with blood)
Great alveolar cells
secret phospholipids and proteins to prevent collapse
Henry's Law and Its Relationship to Alveolar Gas Exchange
-Gas exchange across the alveolar membrane is driven by simple diffusion
-Blood arriving has less oxygen thanair in alveoli. Net oxygen input to blood until equilibrium.
-Blood arriving has more CO2 than airin alveoli. Net CO2 output to alveoliuntil equilibrium.
Respiratory cycle
one complete breath, inspiration and expiration
Ventilation
requires a difference between air pressurewithin the lungs and the external air pressure
Diaphragm and intercostal muscles (between ribs) are
-The major muscles involved in creating difference in pressure gradients.
-Diaphragm 2/3 of the airflow
-Intercostal muscles 1/3 of the airflow
Intercostal Muscles
-Primary function -stiffen thoracic cage and prevent collapsing when diaphragm descends•
-1/3 of airflow
-External muscles-contract during inhaling to widen thoracic cavity
-Internal muscles -contract during exhaling to narrow thoracic cavity
Quiet respiration
breathing while at rest; effortless and automatic
Quiet Inhalation
Scalenes of the neck fix ribs 1 and 2 while external intercostals pull the ribs upward and forward
Quiet Expiration
-Energy-saving passive process achieved by the elasticity of the lungs and thoracic cage
-As muscles relax, structures recoil to original shape and original (smaller) size of thoracic cavity
Forced respiration
deep or rapid breathing, such as during exercise or playing an instrument
Forced Inspiration
-Erector spinae arches the back
-Upper ribs are elevated
Forced Expiration
-Accessory muscles: rectus abdominis, internal intercostals, and other lumbar, abdominal, and pelvic muscles
-Increases abdominal pressure pushes viscera up against diaphragm increasing thoracic pressure, forcing air out
Valsalva maneuver
breathing technique used to help expel contents of certain abdominal organs
Atelectasis and Pneumothorax (collapsed lung)
-Atelectasis: caused by obstruction of airway or pressure on the outside of the lung
-Pneumothorax: thoracic wall is punctured, inspiration sucks air into the pleural cavity, and buildup of pressure compresses the lungs
Does your chest expand because your lungs inflate, or do your lungs inflate because your chest expands?
-Your lungs inflate because your chest expands.
-When the diaphragm and intercostal muscles contract, they expand the thoracic cavity, decreasing pressure inside the lungs
When the diaphragm contracts
YOU INHALE
When inferior accessory muscles contract, do you inhale or exhale?
you inhale